Introduction
Currently, there are no reliable biomarkers for
predicting the prognosis of patients who undergo radical cystectomy
for bladder cancer. Previous studies have shown that several
inflammatory markers, including the neutrophil-to-lymphocyte ratio
(NLR), monocyte-to-lymphocyte ratio (MLR), lymphocyte-to-platelet
ratio (LPR), De Retis and prognostic nutritional index (PNI), are
raised as new prognostic factors for number of cancers (1-3).
The NLR, MLR, and LPR represent the ratios of
lymphocytes to neutrophils, monocytes, and platelets (4). High values of these markers indicate a
poor prognosis in the NLR. To the best of our knowledge, no other
markers have been reported in bladder cancer (5). The detailed mechanisms underlying how
these inflammatory cytokines are correlated with cancer progression
remain unclear. A candidate mechanism involves malignant disease
enhancing inflammation, thereby affecting regulatory T cells
(4,6). Cancer progression decreases the number
of lymphocytes, which increases the NLR and MLR and decreases the
LPR (4,6).
Studies have shown that the PNI was correlated with
the prognosis in several malignancies including lung and
gastrointestinal cancers (2,7).
Systemic inflammation increased tumorigenesis and cancer
progression, resulting in low albumin levels and immunosuppression
(3). This phenomenon has been
reported in colon, gastric, lung, and pancreatic cancers (8).
De Ritis is calculated as the aspartate transaminase
(AST) levels divided by alanine transaminase (ALT) levels, as first
reported by Fernando De Ritis in 1957(8). This marker does not evaluate liver
function but rather indicates the severity of liver dysfunction
(8). In genitourinary cancer, a
high De Ritis ratio was reported to be a poor prognostic marker in
prostate, renal, and urothelial carcinoma. In other solid
malignancies including breast and lung cancer, a high De Ritis
ratio was also reported to be a poor prognostic marker (8).
The present study aimed to assess the most reliable
inflammatory tumor marker in bladder cancer patients who have
undergone radical cystectomy.
Patients and methods
A total of 161 cases underwent radical cystectomy
between April 1994 and April 2014 at Yokohama City University
Medical Center (Yokohama, Japan). The median and mean follow-up
periods were 29.2 and 39.4±31.4 months and all patients were >18
years. Of these patients, the 107 who had data for the NLR, MLR,
LPR, De Ritis and PNI were enrolled in the present study (Table I). The PNI is calculated using the
albumin and lymphocyte count with the following formula: PNI=(10 x
albumin) + (0.005 x total lymphocyte count) (7). A total of 31 (29.2%) cases received
cisplatin-based neo-adjuvant systemic chemotherapy. Laboratory
data, including complete blood cell count (CBCs) and albumin, AST
and ALT levels, were obtained a few days before surgery. CBCs
included the number of blood cells, platelets and white blood cells
with differentiation. None of the patients showed systemic
inflammation or blood disease at the time of the blood test. The
criteria of systemic inflammation were determined as fever and
elevation of serum C-reactive protein (CRP) levels. In the present
cohort, none of the patients had fever and CRP elevation. The
median value was used as the cut-off value of each factor as
follows: NLR, 1.00; MLR, 0.24: LPR, 73.9; PNI, 44.0 and De Ritis,
1.1. Receiver operator characteristic (ROC) curves were plotted to
show candidate cutoff points. The candidate cutoff points and the
area under the ROC (AUROC) are shown in Table II. Postoperative complications were
assessed using the Clavien-Dindo Grading System and the existence
of surgical complications was defined by the presence of
complications classified as Clavien-Dindo Grade I or higher
(9). The Institutional Review Board
of Yokohama City University Medical Center (Yokohama, Japan)
approved the present study (approval no. D1507018) and written
informed consent was waivered due to the nature of the
retrospective observational study without patient
identification.
 | Table IPatient characteristics. |
Table I
Patient characteristics.
| Characteristics | No. of subjects
(%) |
|---|
| Age, years | |
|
<65 | 42 (39.3) |
|
≥65 | 65 (60.7) |
| Prognosis | |
|
Alive | 79 (73.8) |
|
Death | 28 (26.2) |
| Neo-adjuvant
chemotherapy | |
|
Yes | 31 (29.2) |
|
No | 76 (71.0) |
|
Recurrence | 33 (30.8) |
| Pathological T
stage | |
|
≤2 | 53 (49.5) |
|
≥3 | 54 (50.5) |
| Pathological N
stage | |
|
Positive | 17 (15.9) |
|
Postoperative
complications | 21 (19.6) |
| Table IICandidate cutoff points determined
using ROC analyses. |
Table II
Candidate cutoff points determined
using ROC analyses.
| A, Overall
survival |
|---|
| Marker | AUROC | Cutoff value |
|---|
| NLR | 0.6044 | 2.38 |
| MLR | 0.5136 | 0.18 |
| LPR | 0.5927 | 71.60 |
| PNI | 0.6731 | 47.90 |
| De Ritis | 0.6022 | 1.30 |
| B, Recurrence free
survival |
| Marker | AUROC | Cutoff value |
| NLR | 0.5123 | 2.38 |
| MLR | 0.5381 | 0.25 |
| LPR | 0.5135 | 71.60 |
| PNI | 0.6605 | 47.90 |
| De Ritis | 0.5561 | 1.08 |
The preoperative NLR, MLR LPR, De Ritis and PNI were
examined as prognostic factors for recurrence-free survival (RFS)
and overall survival (OS). A Kaplan-Meier product limit estimate
was used to estimate the OS and RFS. The log-rank test was
performed to compare each risk factor. Values between neoadjyuvant
chemotherapy (NAC) and non-NAC groups were compared. P<0.05 was
considered to indicate a statistically significant difference.
Statistical analyses were performed using the GraphPad Prism 7.0
(GraphPad Software, Inc.).
Results
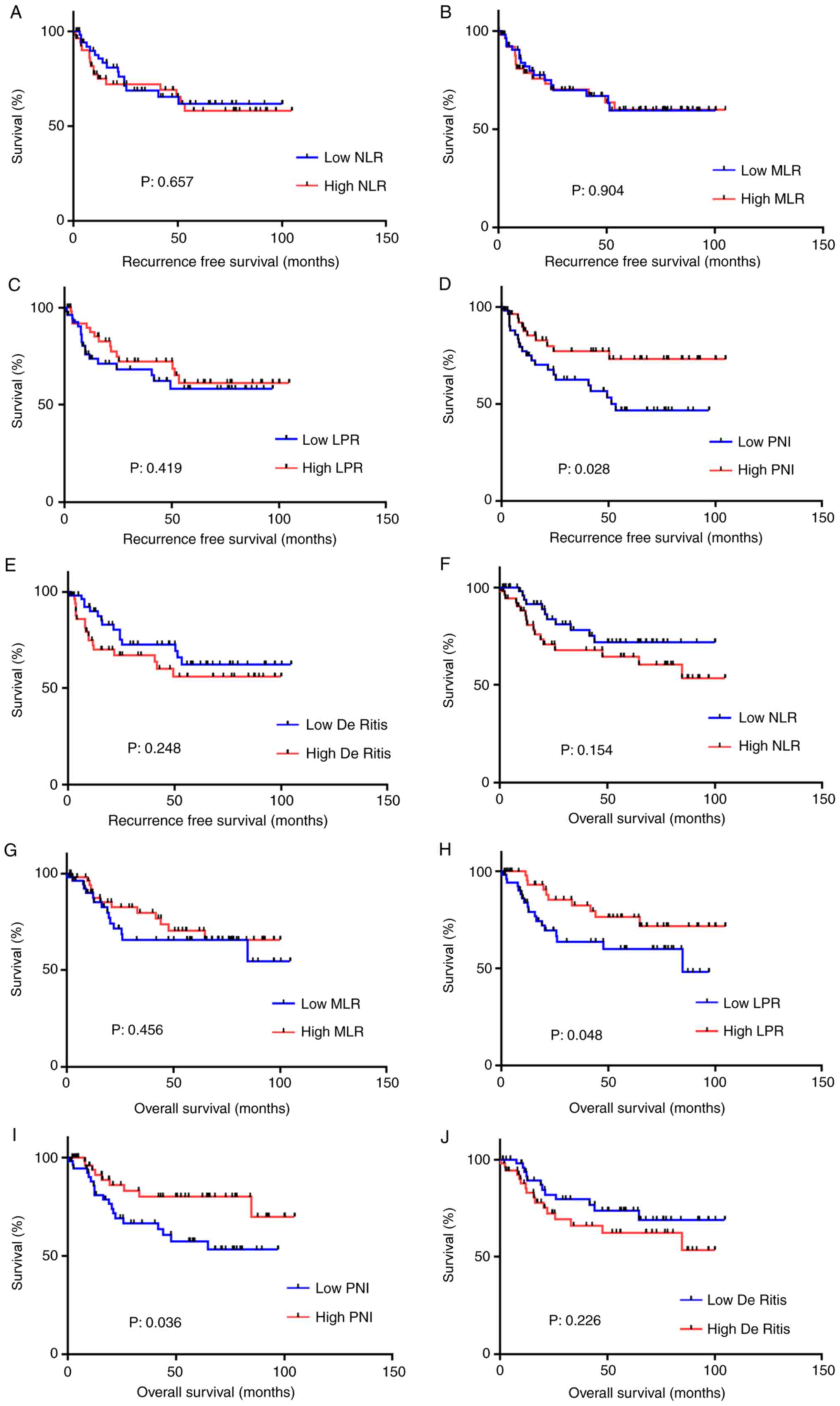
Regarding the RFS, the only noteworthy finding was
that a lower PNI was associated with a significantly lower RFS
compared with higher PNI (P=0.028). Regarding the OS, lower LPR and
PNI were associated with significantly lower OS compared with
higher values (more than median value) (P=0.048 and P=0.036,
respectively). When the cutoff point was set as the median value,
the other inflammatory markers showed no significant association
with either the RFS or OS (Fig. 1).
When the cutoff point was set using the ROC curve, a lower PNI was
associated with significantly lower RFS and OS (P=0.0143 and
P=0.0216, respectively; Fig. 2).
Based on these findings, De Ritis was evaluated as a prognostic
risk factor after radical cystectomy. No differences were observed
between these systemic inflammatory markers and the pT stage, lymph
node metastasis, age, neo-adjuvant systemic chemotherapy or sex
(Table SI).
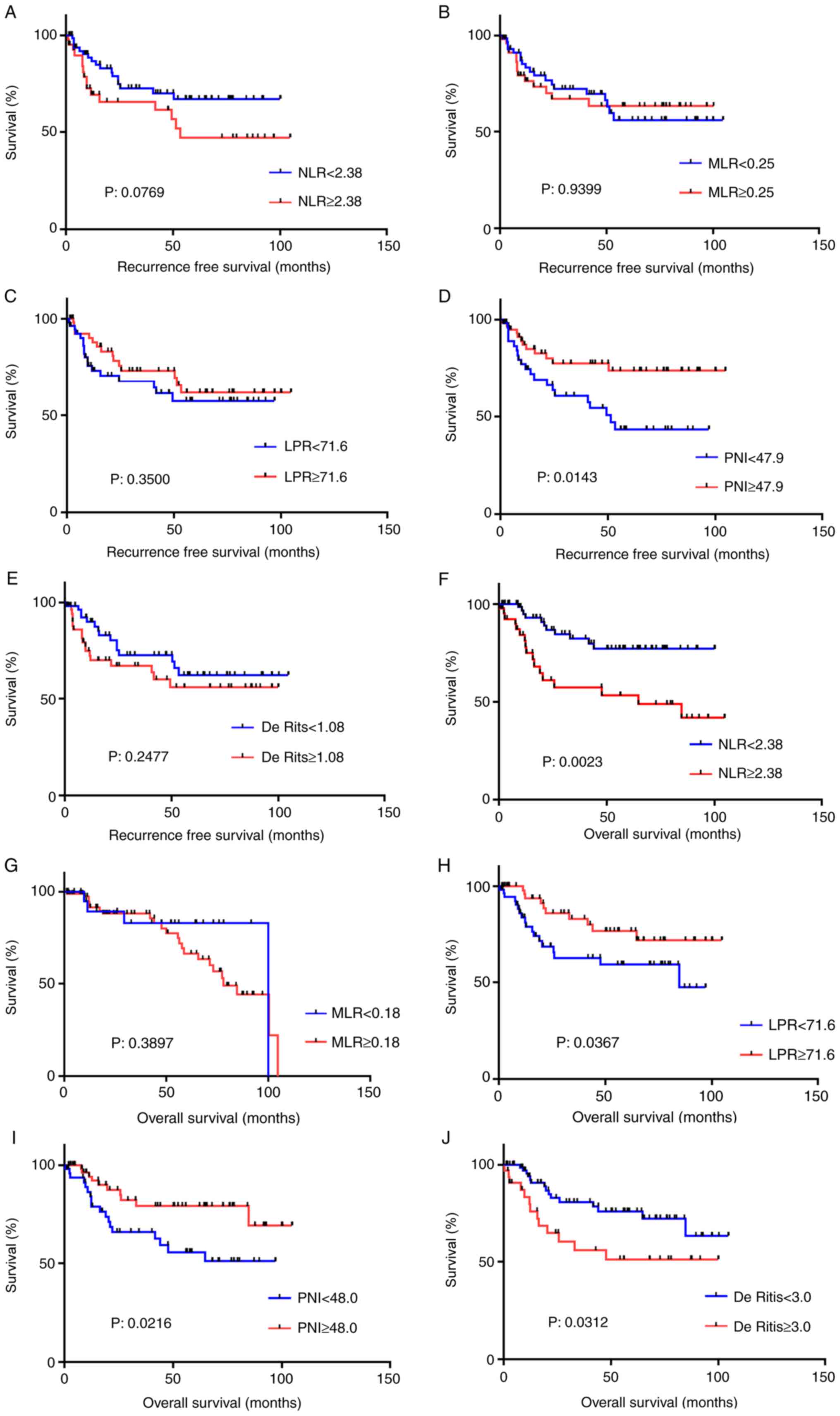 | Figure 2Recurrence-free survival in each
prognostic factor. The recurrence-free survival according to (A)
NLR, (B) MLR, (C) LPR, (D) PNI, and (E) De Ritis. Overall survival
according to (F) NLR, (G) MLR, (H) LPR, (I) PNI and (J) De Ritis,
as determined using candidate cutoff points identified in a
receiver operator characteristic curve analysis. NLR,
neutrophil-to-lymphocyte ratio; MLR, monocyte-to-lymphocyte ratio;
LPR, lymphocyte-to-platelet ratio; PNI, prognostic nutritional
index. |
Discussion
The current strategy for the treatment
muscle-invasive bladder cancer is based on staging using imaging
modalities (3). For non-metastatic
muscle-invasive bladder cancer, radical cystectomy is the gold
standard treatment (3). While
radical cystectomy has proven effective, the recurrence rate is
still not entirely sufficient (4).
Thus, preoperative risk management is necessary. Previous studies
have revealed the usefulness of inflammatory markers in several
solid malignancies, including bladder cancer (2).
The present study examined the effectiveness of
systemic inflammatory markers, including NLR, PNI, MLR, and LPR for
predicting prognosis of bladder cancer. In addition, the utility of
De Ritis was evaluated as a prognostic risk factor after radical
cystectomy. A lower PNI was found to be associated with a
significantly poorer prognosis in both the RFS and OS. This
suggested that albumin may play a role in bladder cancer
progression, in addition to lymphocytes. Therefore, a lower
preoperative PNI predicted an increased risk of recurrence, which
suggested that several adjuvant or neo-adjuvant therapies should be
performed in combination with radical cystectomy.
Onodera et al revealed that a PNI of >45
denoted a low risk of surgical complications, a PNI of 40-45
denoted a high risk of surgical complications and a PNI of <40
suggested that surgery should be avoided (10). A recent study showed that the PNI
was correlated with the prognosis of several malignancies including
lymphoma and pancreas cancer (11,12).
Systemic inflammation increases tumorigenesis and cancer
progression, resulting in low albumin levels and immunosuppression
(7). This phenomenon has been
reported in colon, gastric, lung, and pancreatic cancers (7). Although nutrition plays an important
role in patients undergoing radical cystectomy, no studies have
reported a correlation between the PNI and survival and recurrence
(13).
Several limitations associated with the present
study warrant mention. First, the present study initially used
median values and values determined based on ROC curves as
candidate cutoff points. Until now, no established cut-off point
has been determined. Although median value might have included some
good cutoff points, the median value cutoff points determined from
ROC curves were ultimately used for analysis. The PNI demonstrated
significance using both sets of cutoff points. Second, the number
of patients was relatively small. Therefore, further studies are
needed in order to validate the superiority of the PNI to other
markers. Third, patients from 1994 to 2014 were included. Although
there have been improvements in muscle invasive bladder cancer
treatment such as development of gemcitabine and cisplatin
treatment, there have been no dramatic changes until 2018. Until
2018, immune-checkpoint inhibitors were not permitted for daily
clinical use. Furthermore, none of the patients in the present
cohort received pembrolizumab.
In conclusion, the present study revealed that a low
PNI more accurately predicted lower RFS and OS compared with other
systemic inflammatory risk factors.
Supplementary Material
Marker values in non-NAC and NAC
groups.
Acknowledgements
Not applicable.
Funding
This study was supported by KAKENHI grants (grant
no. 16K20152) from the Ministry of Education, Culture, Sports,
Science and Technology of Japan and grant for 2016-017 Research
Development Fund (grant no. WJ2810) of Yokohama City
University.
Availability of data and materials
The datasets generated and/or analyzed during the
current study are not publicly available due to ethical
restrictions but are available from the corresponding author on
reasonable request.
Authors' contributions
SN and TK drafed the manuscript and performed
stastical analysis and interpretation of data. SN, TK, YM, MY and
HU acquired the data. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Review Board (IRB) of Yokohama City University Medical Center. This
study is a retrospective observational study and the IRB did not
require written informed consent blinded to patients'
identification.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Potretzke A, Hillman L, Wong K, Shi F,
Brower R, Mai S, Cetnar JP, Abel EJ and Downs TM: NLR is predictive
of upstaging at the time of radical cystectomy for patients with
urothelial carcinoma of the bladder. Urol Oncol. 32:631–636.
2014.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Tokunaga R, Sakamoto Y, Nakagawa S,
Miyamoto Y, Yoshida N, Oki E, Watanabe M and Baba H: Prognostic
nutritional index predicts severe complications, recurrence, and
poor prognosis in patients with colorectal cancer undergoing
primary tumor resection. Dis Colon Rectum. 58:1048–1057.
2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ohno Y: Role of systemic inflammatory
response markers in urological malignancy. Int J Urol. 26:31–47.
2019.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Sarraf KM, Belcher E, Raevsky E, Nicholson
AG, Goldstraw P and Lim E: Neutrophil/lymphocyte ratio and its
association with survival after complete resection in non-small
cell lung cancer. J Thorac Cardiovasc Surg. 137:425–428.
2009.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Kawahara T, Furuya K, Nakamura M, Sakamaki
K, Osaka K, Ito H, Ito Y, Izumi K, Ohtake S, Miyoshi Y, et al:
Neutrophil-to-lymphocyte ratio is a prognostic marker in bladder
cancer patients after radical cystectomy. BMC Cancer.
16(185)2016.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Ohtake S, Kawahara T, Kasahara R, Ito H,
Osaka H, Hattori Y, Teranishi JI, Makiyama K, Mizuno N, Umemoto S,
et al: Pretreatment neutrophil-to-lymphocyte ratio can predict the
prognosis in bladder cancer patients who receive gemcitabine and
nedaplatin therapy. Biomed Res Int. 2016(9846823)2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Feng JF, Huang Y and Chen QX: Preoperative
platelet lymphocyte ratio (PLR) is superior to neutrophil
lymphocyte ratio (NLR) as a predictive factor in patients with
esophageal squamous cell carcinoma. World J Surg Oncol.
12(58)2014.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Botros M and Sikaris KA: The de ritis
ratio: The test of time. Clin Biochem Rev. 34:117–130.
2013.PubMed/NCBI
|
|
9
|
Dindo D, Demartines N and Clavien PA:
Classification of surgical complications: A new proposal with
evaluation in a cohort of 6336 patients and results of a survey.
Ann Surg. 240:205–213. 2004.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Onodera T, Goseki N and Kosaki G:
Prognostic nutritional index in gastrointestinal surgery of
malnourished cancer patients. Nihon Geka Gakkai Zasshi.
85:1001–1005. 1984.PubMed/NCBI(In Japanese).
|
|
11
|
Go SI, Park S, Kang MH, Kim HG, Kim HR and
Lee GW: Clinical impact of prognostic nutritional index in diffuse
large B cell lymphoma. Ann Hematol. 98:401–411. 2019.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Nakagawa S, Yamashita YI, Umezaki N, Yamao
T, Okabe H, Imai K, Nitta H, Hashimoto D, Chikamoto A and Baba H:
Serum marker score based on prognostic nutrition index,
carcinoembryonic antigen, and carbohydrate antigen 19-9 is
associated with recurrence for patients undergoing surgery for
pancreatic ductal adenocarcinoma. Pancreas. 47:1130–1134.
2018.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Miyake M, Morizawa Y, Hori S, Marugami N,
Iida K, Ohnishi K, Gotoh D, Tatsumi Y, Nakai Y, Inoue T, et al:
Integrative assessment of pretreatment inflammation-, nutrition-,
and muscle-based prognostic markers in patients with
muscle-invasive bladder cancer undergoing radical cystectomy.
Oncology. 93:259–269. 2017.PubMed/NCBI View Article : Google Scholar
|