Introduction
Dendritic fibromyxolipoma (DFML) is a rare benign
tumor that was first reported by Suster et al in
1998(1). It consists of a mixture
of small spindles to stellate cells and several mature fat cells.
The stellate cells were embedded in an abundant myxoid stroma with
strands of ropey collagen bundles. It shares similar morphologic
features to other myxoid mesenchymal tumors, such as myxoid
liposarcoma (MLS) and solitary fibrous tumor (SFT). In most
reports, it is considered as a special variant of spindle cell
lipoma (2). It is typically present
in the older age population with a male preponderance. Most of
these tumors occurred in head and neck, chest wall, shoulder and
back, and a few were located in limbs, including toes. They are
often located in superficial fascia and occasionally in muscle
(2). To the best of our knowledge,
only 59 cases of DFML were reported and cited in PubMed and Chinese
journals. In this study, we have described three DFML cases that
were located in the limbs and thoracic cavity. Written informed
consents have been obtained from these three patients.
Case presentation
Case 1
The patient was a 50-year-old male who presented
with a painless right upper arm tumor mass for six years. In August
2012, he was admitted to Qingdao Municipal Hospital for the first
time. Recently, the tumor was gradually growing. No other mass was
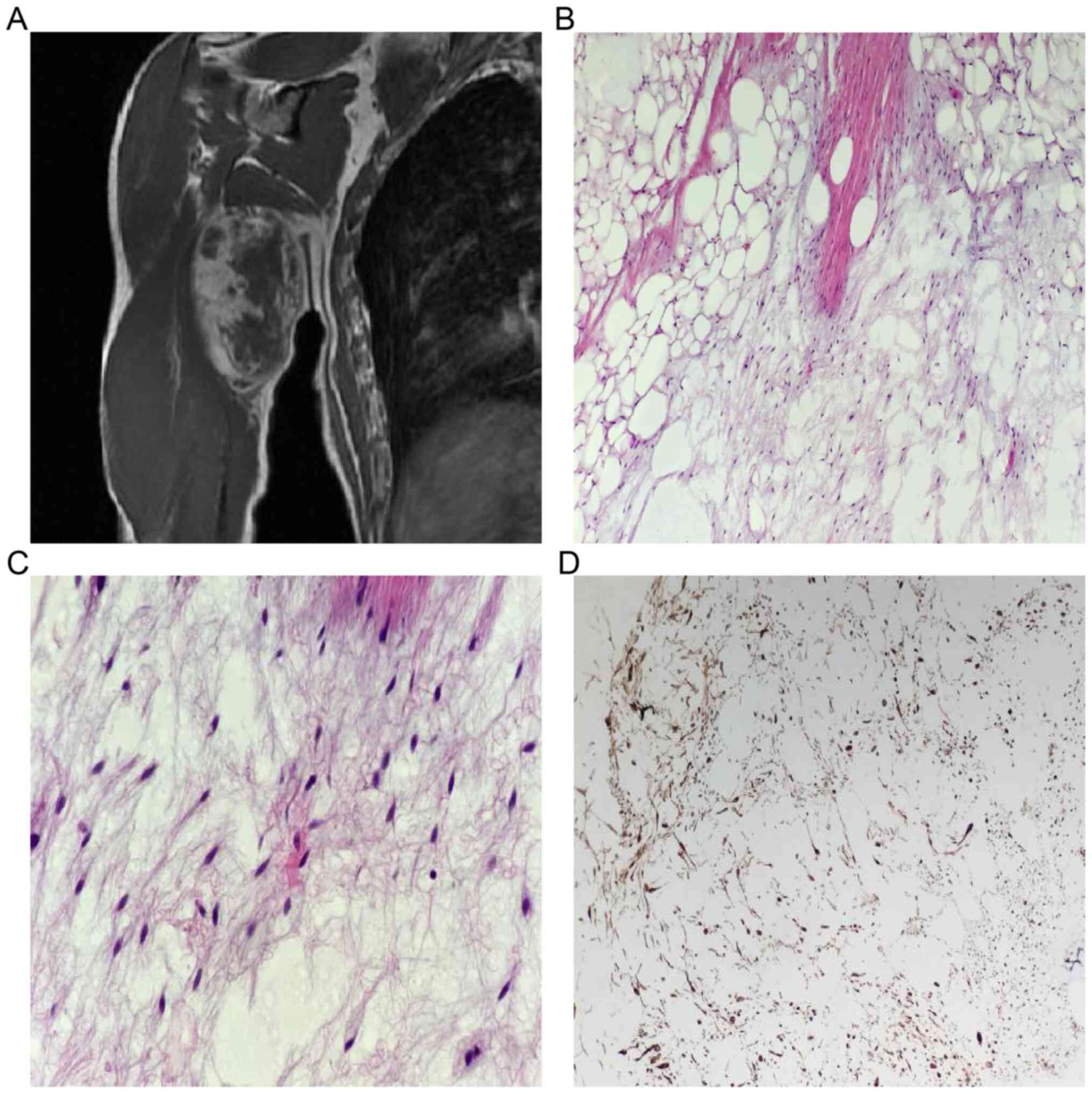
found in other locations. The magnetic resonance imaging (MRI)
showed a well-defined tumor mass measuring 79x46x100 mm in the
right upper arm. It showed a mixed-signal intensity on both T1 and
fat-suppression weighted imaging (Fig.
1A). The tumor was completely resected. Histopathologic
evaluation showed that the tumor was composed of mature adipocytes
with sparse slender spindle cells (Fig.
1B). The cellular atypia was not apparent. Strands of ropey
collagen bundles within the myxoid background were noted (Fig. 1C). Immunohistochemical staining
showed that the spindle cells were strongly positive for CD34
(Fig. 1D), but negative for CD99
and BCL-2. A diagnosis of DMFL was suggested. The patient was
uneventful during a 12-month's follow-up without evidence of
recurrence.
Case 2
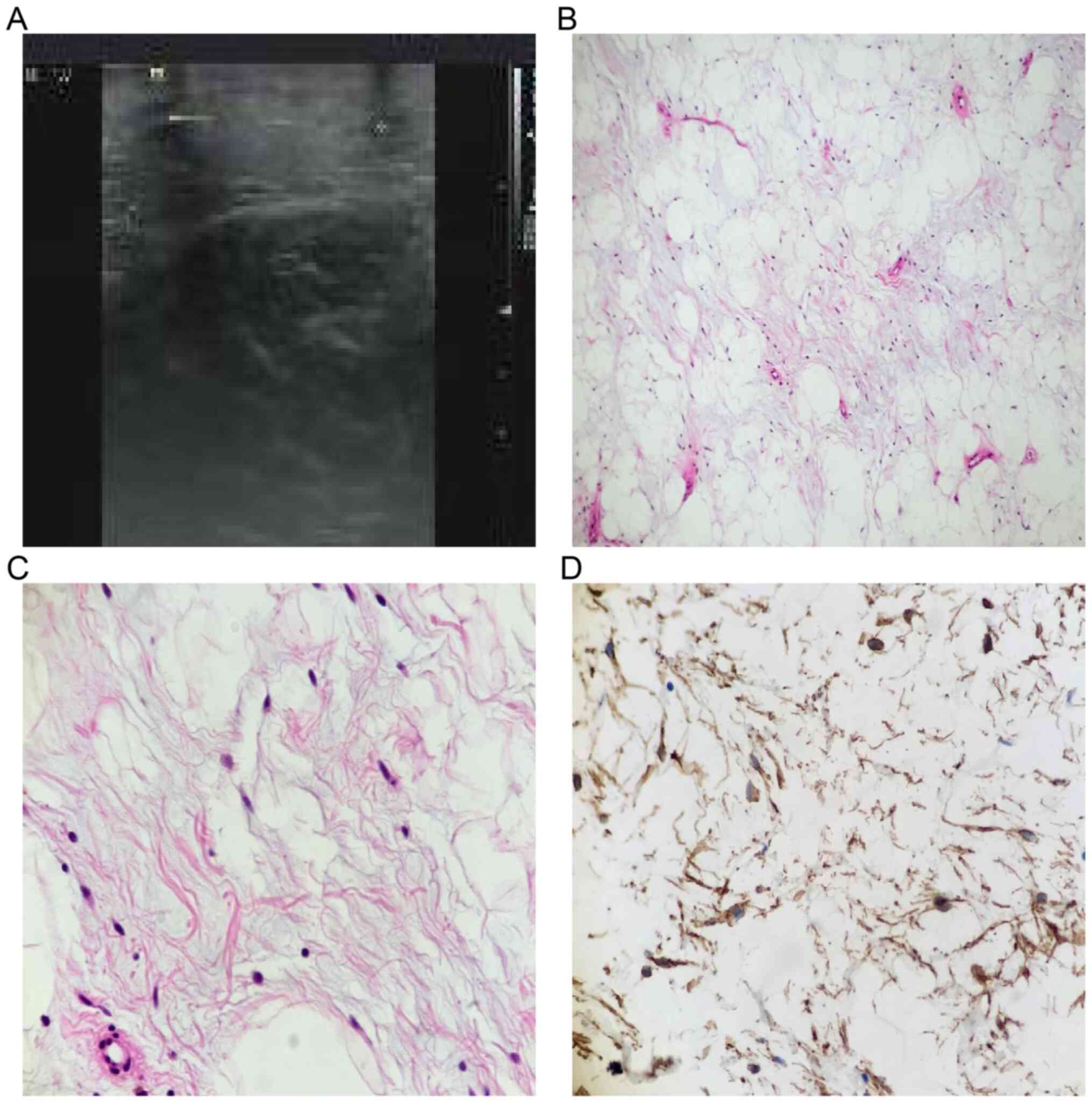
The patient was a 33-year-old male. He was presented
with a gradually growing right thigh mass for three years. In March
2014, he was admitted to Qingdao Municipal Hospital for the first
time. It measured 3x3 cm, and it did not cause any local
discomfort. The ultrasound revealed a subcutaneous well-defined
hyperechoic mass, which suggested a lipoma (Fig. 2A). It was resected completely.
Grossly, the tumor was lobulated with an intact capsule. The cut
surface was yellowish and soft. Histopathologically, the tumor was
composed of mature adipocytes and sparse spindle cells with a
myxoid background (Fig. 2B and
C). The tumor cells were positive
for CD34 (Fig. 2D) and negative for
CD99 and BCL-2.
Case 3
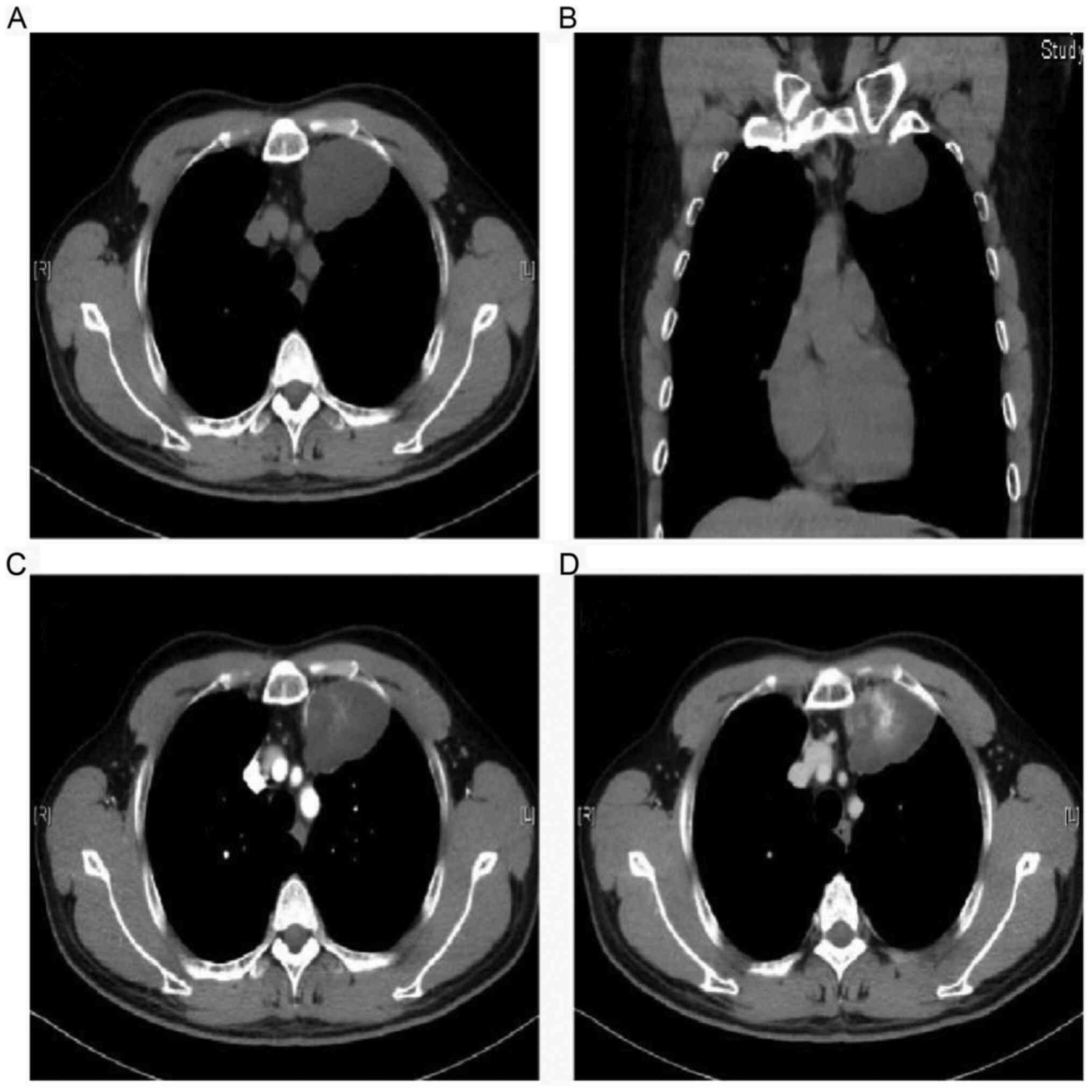
The patient was a 48-year-old male who presented
with a left thoracic tumor mass. He appeared asymptomatic, and the
medical history was unremarkable. In July 2015, he was admitted to
Qingdao Municipal Hospital for the first time. The tumor was
incidentally observed during a routine physical examination. No
other mass was found in other locations. The computed tomography
(CT) showed a homogenous low-density mass in the left thoracic
cavity beside the mediastinum. It measured 43x60x36 mm and had a
well-defined boundary (Fig. 3A and
B). The tumor center was
heterogeneously enhanced, indicating the presence of blood vessels.
The tumor center was enhanced more obviously in the venous phase
(Fig. 3D) than the arterial phase
(Fig. 3C). Considering the tumor
location, a pleural SFT was suggested. In addition, a fine needle
biopsy was performed, but as no adipocytes were observed, a
pathologic diagnosis of myxoid subtype of SFT was made. The tumor
was completely resected by video-assisted thoracic surgery.
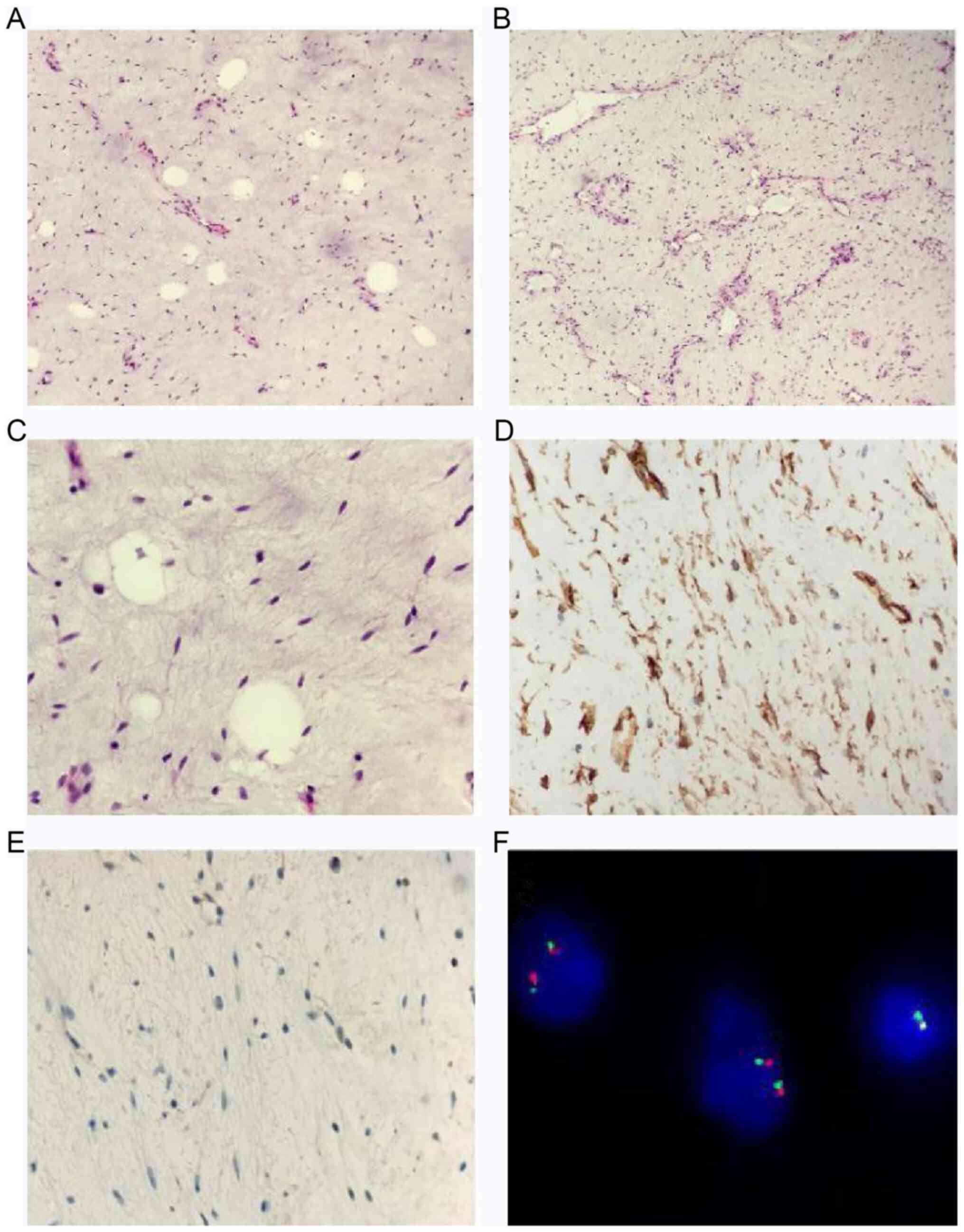
Histopathologic evaluation showed that the tumor predominantly
comprised slender spindle cells embedded in an abundant myxoid
stroma with strands of ropey collagen bundles (Fig. 4A and B). The cellular atypia was not apparent.
Red collagen bundles were apparent under high power (Fig. 4C). Immunohistochemical staining
showed that the spindle cells were strongly positive for vimentin
and CD34 (Fig. 4D), but negative
for BCL-2 (Fig. 4E), CD99, STAT6,
S100, SMA and Desmin. The Ki-67 index was <1%. Focal mature
adipocytes were present within the myxoid background. In addition,
a prominent delicate, arborizing vascular pattern was observed in
some areas, which was similar to a MLS. However, the fluorescence
in situ hybridization (FISH) analysis with the DDIT3
break apart probe (ZytoLight; cat. no. Z-2100-200) showed negative
DDIT3 rearrangement (Fig.
4F). Therefore, a pathologic diagnosis of DFML was rendered.
The patient was uneventful during a follow-up of 15 months without
evidence of recurrence and metastasis.
Discussion
A literature search was performed in Pubmed, CNKI
and Wanfang database to identify eligible studies published prior
to October 9, 2019. Search terms were ‘dendritic fibromyxolipoma’
or ‘DFML’. The inclusion criteria was: case report or case series
on patients with DFML. The exclusion criteria was: articles that
were reviews, comments, news, letters and that did not meet the
inclusion criteria were excluded. Articles not in the English or
Chinese language were also excluded. 20 studies were eligible
involving 59 patients with DFML, including 48 males and 11 females
(Table I).
 | Table IClinical findings of 61 reported cases
of dendritic fibromyxolipoma. |
Table I
Clinical findings of 61 reported cases
of dendritic fibromyxolipoma.
| Author, year | Age, years | Sex | Presentations | Location | Size (cm) | Follow-up | (Refs.) |
|---|
| Suste et al,
1998 | 33-81 (mean, 64) | 11 Males; 1
Female | - | Head and neck region
or the chest and back. | 3-11 | Seven cases with 2-13
years' follow-up | (1) |
| Tan and Wen,
2003 | 45-75 (mean, 65) | 8 Males | - | Head and neck region,
shoulder, back, calf and foot | 2-9.5 | Five cases with 0.5-3
years' follow-up | (3) |
| Karim et al,
2003 | 73 | Male | A painless mass | Right shoulder | 13x8x5.5 | - | (4) |
| Al-Maskery et
al, 2011 | 36 | Female | A progressive
painless swelling | Lower lip | 2x1.6x2 | 2 years | (5) |
| Dahlin and Ljungberg,
2012 | 65 | Female | Hypertension | Left volar
forearm | 2x3.2x1 | 3 years | (6) |
| Qiao et al,
2012 | 39-67 (mean, 54) | 9 Males; 1
Female | Painless subcutaneous
nodules | Neck region, back and
shoulder | 1-6 | 13-27 months | (7) |
| Zhang et al,
2013 | 32 | Female | A painless
subcutaneous mass for 3 years | Right inguinal and
perineum | 24x10.5x5 | 9 months | (8) |
| Wong et al,
2014 | 67 | Male | A gradually
enlarging, painless left shoulder swelling for 1 year | Left shoulder | 7 | - | (2) |
| Han et al,
2014 | 69 | Male | A skin-colored lesion
for 4 years | Nasal tip | 1 | - | (9) |
| Yuan et al,
2014 | 33-81 (mean, 64) | 3 Males | Gradually growing
mass without symptoms | Neck region, back,
and shoulder | 3.7-8.6 | 2-16 months | (10) |
| Xu et al,
2015 | 24 | Male | A painless, slowly
growing mass for 2 years | Left shoulder | 14x8.5x8 | 4 years | (11) |
| Liu et al,
2015 | 53 | Male | A mass for 1
month | Right back | 2x1.5x1.5 | 1 year | (12) |
| Guo et al,
2015 | 45-80 (mean, 59) | 3 Males | Local mass and
pressure symptoms | Neck region, back,
and shoulder | 3-8 | 6-18 months | (13) |
| Song et al,
2016 | 34 | Female | A recurrent jaw
tumor mass | Jaw | 4x3x3 | - | (14) |
| Ciloglu et
al, 2016 | 59 | Female | A painless
subcutaneous mass for 10 years | Left inguinal
region | 17x13x10 | 3 years | (15) |
| AlAbdulrahim and
Arafah, 2016 | 38 | Male | A progressive
dysphagia for 1 year | Hypopharynx | 3.4x3.4x2.8 | - | (16) |
| Xiao et al,
2017 | 38, 53 | 1 Male; 1
Female | A pain mass | Abdominal
cavity | 7 cm, 16 | 6-18 months | (17) |
| Li et al,
2017 | 27-73 (mean,
50) | 4 Males; 2
Females | A painless slowly
growing mass | Shoulder, waist,
back, thigh, iliac fossa and mesentery | 2.5-18.5 | Several months-
several years | (18) |
| Ruiz Molina et
al, 2018 | 69 | Male | A painless soft
tissue mass for 8 years | Infraclavicular
region | 5x1.7 | 2 years | (19) |
| Fu et al,
2018 | Mean 50 | 2 Males; 1
Female | - | Upper arm, shoulder
and oral cavity | 4-5.5 | - | (20) |
DFML is an uncommon benign tumor that was initially
described by Suster et al in 1998. A total of 12 cases were
introduced in their report (1).
Since then, a total of 47 additional cases have been reported and
cited in PubMed and Chinese journals (Table I) (1-20).
Although its incidence is relatively low, DFML can occur in almost
all parts of the body, including the left inguinal region (15), hypopharynx (16), infraclavicular region (19), and other uncommon parts. The tumor
develops primarily in the sub-cutis or muscular fascia. Among the
62 reported cases (including the current three cases), the age of
patients ranges from 24 to 81 years with a male/female ratio of
51/11. The tumor size ranges from 1 to 24 cm, with an average of
8.2 cm. Gradually growing up mass without symptoms is the most
common clinical manifestation. The medical history ranged from 1
month to 13 years. When the tumor is superficial, it often
manifests as a painless tumor mass for several years. To the best
of our knowledge, no more than 10 cases of DFML of extremities have
been reported. The clinical presentations and imaging features are
rather non-specific, and the definite diagnosis relies on the
histopathology. The differential diagnosis includes other myxoid
mesenchymal tumors, for instance, MLS and SFT. When the blood
vessels are abundant, and ‘chicken-wire’ like, or the fat component
is not apparent, a diagnosis is rather difficult.
It has been reported that the 13q14.3 deletion, the
hall marker of spindle cell lipoma, was detected in DFML. Thus,
DFML is considered as a myxoid variant of spindle cell lipoma
(2). It is mainly composed of mild
spindle cells and unequal amounts of mature adipocytes. The spindle
cells are small and deeply stained, without obvious atypia. The
cytoplasm has long and narrow protrusions, which are dendritic. The
mitotic figures are rare. According to a report, the bland spindle
cells were positive for CD34, vimentin and BCL-2. However, BCL-2
was not invariably positive in the present three cases, which had
also been observed for two previous cases (6,11).
The tumor may be confused with other myxoid
mesenchymal tumors. i) MLS and DFML: they may share a distinct
myxoid background and mature adipocytes. They are easy to be
confused, especially when the lesions occur in non-superficial
sites (such as case 3). However, they can be distinguished from
each other by histology, immunohistochemistry and molecular
genetics (3,21,22).
DFML is mostly located in the superficial tissues. Morphologically,
DFML consists of abundant delicate, arborizing blood vessels and
bland spindle or stellate-shaped cells in a myxoid with a
collagenous matrix. The adipocytes were scattered, and definite
lipoblasts were not identified. The short spindle cells were sparse
and lacked atypia and mitosis. Thus, it may be somewhat difficult
to make a definite diagnosis. In contrast, MLS occurs mostly in the
deep soft tissues of the lower extremities. The tumor is mainly
composed of three components: Adipocytes with different degrees of
differentiation, myxoid stroma, and plexiform capillaries. In
immunohistochemistry, CD34, BCL-2, and vimentin were expressed in
DFML, but S-100 and Desmin were negative, while in MLS, the
opposite result was found. In molecular genetics, 13q14.3 deletion
exists in DFML, while FUS-DDIT3 (>90%) or
EWSR1-DDIT3 (<5%) gene fusion exists in MLS
(23). In case 3, the FISH
detection for FUS-DDIT3 was negative, and the
immunohistochemistry for NY-ESO-1 (a specific immunomarker for MLS)
was also negative. These results can rule out an MLS. Since 13q14.3
detection is an important biomarker for spindle cell lipoma
(2), the lack of its detection is a
limitation of this study. And the tissues obtained from the 3
patients were for the purposes of diagnosis only, not for testing
novel biomarkers. The clinical history, histological morphology and
immunohistochemistry were mainly used to identify these two
diseases. ii) Myxofibrosarcoma (MFS) and DFML: in case 3, a
possible diagnosis of MFS invading the pre-existing adipose tissues
should be ruled out. The diagnosis of MFS mostly depends on the
morphology, and immunohistochemistry may be not very helpful. MFS
is a kind of malignant soft tissue tumor. The histologic features
of MFS included the following: a commonly nodular growth pattern; a
myxoid matrix containing elongated, curvilinear capillaries; and
fusiform, round or stellate tumor cells with indistinct cell
margins, slightly eosinophilic cytoplasm and hyperchromatic
atypical nuclei. For the present case, it was well defined and had
a clear boundary without involving the surrounding tissues. In
addition, the adipocytes were evenly distributed and rather
scattered. Thus, we believe the adipocytes were tumor components.
Furthermore, the flow-up result also favors the diagnosis of a
benign tumor. iii) Low-grade fibrous myxoid sarcoma (LGFMS) and
DFML: The morphology of LGFMS is a vortex structure composed of
fusiform fibroblast-like cells, and alternating collagen-like and
myxoid regions are observed. In addition, arch vessels and
perivascular hyalinosis can be seen. (4) Lipoblastoma and DFML: likewise, in
addition to mucin-like interstitial and branched blood vessels,
there are also fat vacuoles stellate and fusiform stromal cells.
However, 90% of lipoblastomas occur in infants under three years of
age, while DFML often occurs in middle-aged and older adults, and
spindle cells are positive for CD34. (5) SFT: It can undergo extensive myxoid
degeneration, and the spindle cells are positive for STAT-6, CD99,
CD34 and BCL-2. However, the mature fat component is absent.
DFML is a special subtype of spindle cell lipoma.
Complete resection is the best treatment choice. A diagnostic
pitfall is other myxoid mesenchymal tumors, such as LMS and LGFMS,
which may lead to ‘overtreatment.’ The postoperative recurrence and
metastasis are rare after complete resection. Only one recurrent
case was reported until now (14).
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or data analyzed during the
present study are available from the corresponding author on
reasonable request.
Authors' contributions
HL, SH and HC conceived the present study. JW, QZ,
XY and HC performed the experiments. HL, SH, JW, QZ and XY wrote
the manuscript. XY and HC critically reviewed the manuscript. All
authors read and approved the final version of the manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of the Qingdao Municipal Hospital (approval no.
2020-049). All patients provided their written informed
consent.
Patient consent for publication
All patients provided their consent for the
publication of their data and associated images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Suster S, Fisher C and Moran CA: Dendritic
fibromyxolipoma: Clinicopathologic study of a distinctive benign
soft tissue lesion that may be mistaken for a sarcoma. Ann Diagn
Pathol. 2:111–120. 1998.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Wong YP, Chia WK, Low SF, Mohamed-Haflah
NH and Sharifah NA: Dendritic fibromyxolipoma: A variant of spindle
cell lipoma with extensive myxoid change, with cytogenetic
evidence. Pathol Int. 64:346–351. 2014.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Tan GM and Wen P: Clinicopathologic
features of dendritic fibromyxolipoma. Zhonghua Bing Li Xue Za Zhi.
32:404–408. 2003.PubMed/NCBI(In Chinese).
|
|
4
|
Karim RZ, McCarthy SW, Palmer AA, Bonar SF
and Scolyer RA: Intramuscular dendritic fibromyxolipoma: Myxoid
variant of spindle cell lipoma? Pathol Int. 53:252–258.
2003.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Al-Maskery AY, Al-Sidairy SM and
Al-Hamadani AS: Dendritic myxofibrolipoma: Often misdiagnosed as
sarcoma. Craniomaxillofac Trauma Reconstr. 4:171–174.
2011.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Dahlin LB and Ljungberg O: Dendritic
fibromyxolipoma adherent to the median nerve in the forearm. J
Plast Surg Hand Surg. 46:120–123. 2012.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Qiao HG, Zhang C, Zhuang YL and Wang J:
Dendritic fibromyxolipoma: A clinicopathological analysis of 10
cases. J Clin Exp Pathol. 28:1332–1335. 2012.
|
|
8
|
Zhang XJ, Zhou S, Nie K, Chen DF, Kui GJ
and Zhang XH: Dendritic fibromyxolipoma in the right inguinal and
perineum regions: A case report and review of the literature. Diagn
Pathol. 8(157)2013.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Han XC, Zheng LQ and Shang XL: Dendritic
fibromyxolipoma on the nasal tip in an old patient. Int J Clin Exp
Pathol. 7:7064–7067. 2014.PubMed/NCBI
|
|
10
|
Yuan XX, Yuan JP, Yang YH, Yin YB and Luo
B: CliIlicopathological characteristics of dendritic
fibromyxolipoma in muscIe: An anaIysis of 3 cases. J Diagn Pathol.
21(1)2014.
|
|
11
|
Xu X, Xiong W, Zheng L and Yu J:
Intramuscular dendritic fibromyxolipoma in a 24-year-old male: A
case report and review of the literature. Oncol Lett. 9:583–586.
2015.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Liu S, Wang X, Lei B, Ma H, Li J, Guo D
and Xu S: Dendritic fibromyxolipoma in the latissimus dorsi: A case
report and review of the literature. Int J Clin Exp Pathol.
8:8650–8654. 2015.PubMed/NCBI
|
|
13
|
Guo WW, Huang WQ, Kong QN and Han ZL:
Clinicopathologic analysis of dendritic fibromyxolipoma. J Clin
Pathol Res. 35:622–626. 2015.
|
|
14
|
Song L, Wang Z, Xu JW and Qin YJ:
Dendritic fibromyxolipoma of jaw: Report of a case. Zhonghua Bing
Li Xue Za Zhi. 45:276–277. 2016.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
15
|
Ciloglu S, Duran A, Keskin E and Yigit A:
Dendritic fibromyxolipoma of left inguinal region. Indian J Pathol
Microbiol. 59:250–251. 2016.PubMed/NCBI View Article : Google Scholar
|
|
16
|
AlAbdulsalam A and Arafah M: Dendritic
fibromyxolipoma of the pyriform sinus: A case report and review of
the literature. Case Rep Pathol. 2016(7289017)2016.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Xiao XW, Zhang LF, Li WS and Liu Y:
Clinicopathological characteristics of dendritic fibromyxolipoma in
abdominal cavity: An analysis of two cases. Diagn Pathol.
24(7)2017.
|
|
18
|
Li YQ, Ma Q, Chen Y, Tang Y and Qian ZH:
Dendritic fibromyxolipoma: A clinicopathologic analysis of 6 cases
and review of the literature. J Clin Pathol Res. 37:527–530.
2017.
|
|
19
|
Ruiz Molina I, Solis Garcia E and Civico
Amat V: Dendritic infraclavicular fibromyxolipoma: At the boundary
between spindle cell lipoma and solitary fibrous tumour. Rev Esp
Patol. 51:44–48. 2018.PubMed/NCBI View Article : Google Scholar : (In Spanish).
|
|
20
|
Fu WL, Tang XF and Guo QN: A
Clinicopathologic study of dendritic fibromyxolipoma. Med J West
China. 30:503–506. 2018.
|
|
21
|
Abaricia S and Hirbe AC: Diagnosis and
treatment of myxoid liposarcomas: Histology matters. Curr Treat
Options Oncol. 19(64)2018.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Hei SM, Wei HJ, Chen H and Wang JG:
Pathological significance of NY-ESO-1 expression in the diagnosis
of myxoid liposarcoma. Zhonghua Bing Li Xue Za Zhi. 48:225–230.
2019.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
23
|
Yu JS, Colborne S, Hughes CS, Morin GB and
Nielsen TO: The FUS-DDIT3 interactome in myxoid liposarcoma.
Neoplasia. 21:740–751. 2019.PubMed/NCBI View Article : Google Scholar
|