Introduction
Large cell neuroendocrine carcinoma (LCNEC) is a
high-grade neoplasm most commonly presenting in the lung, although
it has been noted in the literature to occasionally arise in other
locations including the gastrointestinal tract, bladder, prostate,
gallbladder, ovary, uterus and submandibular gland (1-7).
LCNEC is a rare cancer, estimated to comprise between 2.1 and 3.5%
of surgically resected lung tumors (8,9). It is
morphologically different from small cell lung cancer (SCLC) and
has a higher mitotic count than low-grade neuroendocrine carcinoma
(10-12).
These tumors have unique histological features including large
nuclei with prominent nucleoli, vesicular or open chromatin,
rosette-like structures, and trabecular palisading patterns
(13). When a diagnosis of LCNEC
cannot be made on a morphological basis, immunohistochemical
markers exist that can differentiate the disease from SCLC
(14). A strong association between
LCNEC and cigarette smoking has been documented (8,9,15).
Unfortunately, prognosis for LCNEC is generally poor, with a 5-year
all-stage survival rate of about 40% (16).
Investigations into the LCNEC genome via
next-generation sequencing have found that the cancer clusters into
two different groups, a SCLC-like subset and a NSCLC-like subset
(17,18). There is no morphological difference
between tumor cells belonging to either subset; however, the
SCLC-like tumors tend to have higher proliferative activity
(18). SCLC-like LCNEC tumors are
characterized by inactivating mutations in TP53 and RB1, while
NSCLC-like LCNEC has frequent mutations in STK11 (60%), KRAS (40%),
and KEAP1 (36%) (18). Mutations in
PIK3CA (3%), PTEN (4%), and FGFR (5%) are uncommon in LCNEC
(19), and mutations for which
targeted therapy exists, including EGFR, BRAF and ALK, are very
unusual (<1%) (13,17,19).
Due to the relative rarity of LCNEC, no large-scale
randomized controlled trials have been conducted and no
standardized treatment regimen has been established as clearly
superior. It is well-established that surgical resection is the
only curative treatment modality and that adjuvant chemotherapy
appears to confer a survival benefit (20). Thoracic radiotherapy (RT) also
appears to show a survival benefit when combined with chemotherapy
(21). Most patients are not
surgical candidates (22), and
typically are treated with chemotherapy regimens similar to those
used for small cell lung carcinoma, most often platinum and
etoposide. However, studies have not conclusively demonstrated the
superiority of this regimen over platinum and gemcitabine
chemotherapy regimens used for non-small cell lung cancer (23,24).
Targeted therapy has been used against these tumors, but LCNEC
rarely harbors targetable mutations (13,17,25).
In the future, the incorporation of molecular data may ultimately
impact treatment decisions and patient outcomes by identifying an
optimal, personalized treatment regimen for a tumor's specific
molecular makeup. In one study, patients found to be wild-type for
RB1 had significantly longer survival when treated with gemcitabine
and a taxane than those treated with cisplatin/etoposide (26). Loss of P16 expression was also
predictive of superior survival with gem/taxane chemotherapy
(26).
Case report
A 56 year old male presented to the hospital after a
month of progressive dyspnea. He attested to significant weight
loss over the past 6 months and had also developed a cough with
occasional hemoptysis. He was an active smoker, having smoked a
pack of cigarettes a day for the past 20 years. He had been
experiencing intermittent chest pain, but denied any fevers,
chills, or night sweats. All initial laboratory data were
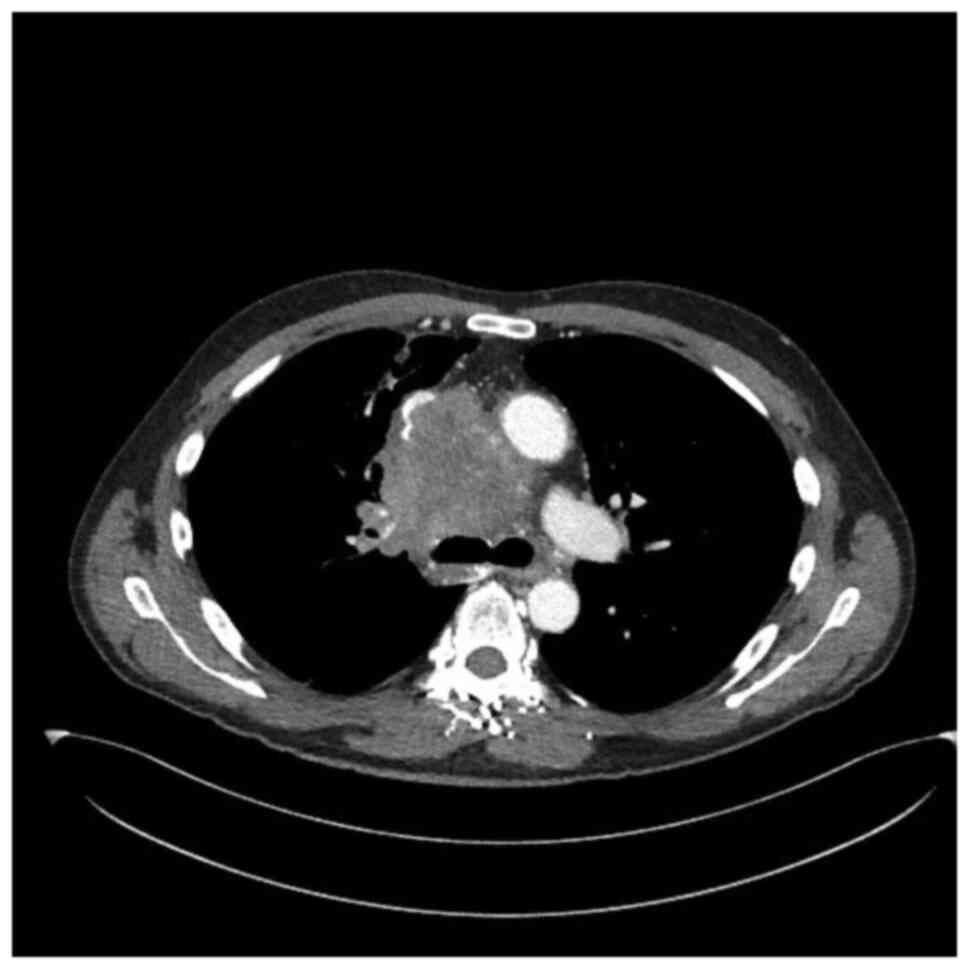
unremarkable. A chest X-ray taken in the emergency department
revealed a large perihilar opacity and follow-up chest computed
tomography (CT) demonstrated a 7.9x8.5 cm right-sided anterior
mediastinal mass with left tracheal deviation. The mass encased the
superior vena cava (SVC) and right bronchus but both structures
were patent. Tumor marker labs revealed an elevated lactate
dehydrogenase (254 U/l) and an increased level (158 IU/ml) of
α-fetoprotein (AFP), suggestive initially of teratoma. B-hCG was
undetectable. The tumor was biopsied via endobronchial ultrasound
(EBUS) guided bronchoscopy, which revealed sheets of large cells
with eosinophilic cytoplasm, enlarged nuclei, and prominent
nucleoli (Fig. 1A). Necrosis,
apoptotic bodies and conspicuous mitotic activity was present.
Immunohistochemical studies were performed on the Dako Omnis
(Agilent) platform using a polymer detection method, utilizing
horseradish peroxidase substrate 3,3'-diaminobenzidine
tetrahydrochloride (DAB) for visualization. The tumor cells showed
immunohistochemical positivity for pancytokeratin, chromogranin,
synaptophysin and CD56. Rare cells showed cytoplasmic positivity
for AFP (Fig. 1B-D). SALL4 showed
patchy and weak nuclear positivity (Fig. 1E). Ki67 (MIB-1) showed an elevated
proliferative index of over 95% (Fig.
1F). The tumor cells did not stain with TTF-1, napsin A, p40,
CD30, OCT3/4 or PLAP. The findings were consistent with LCNEC.
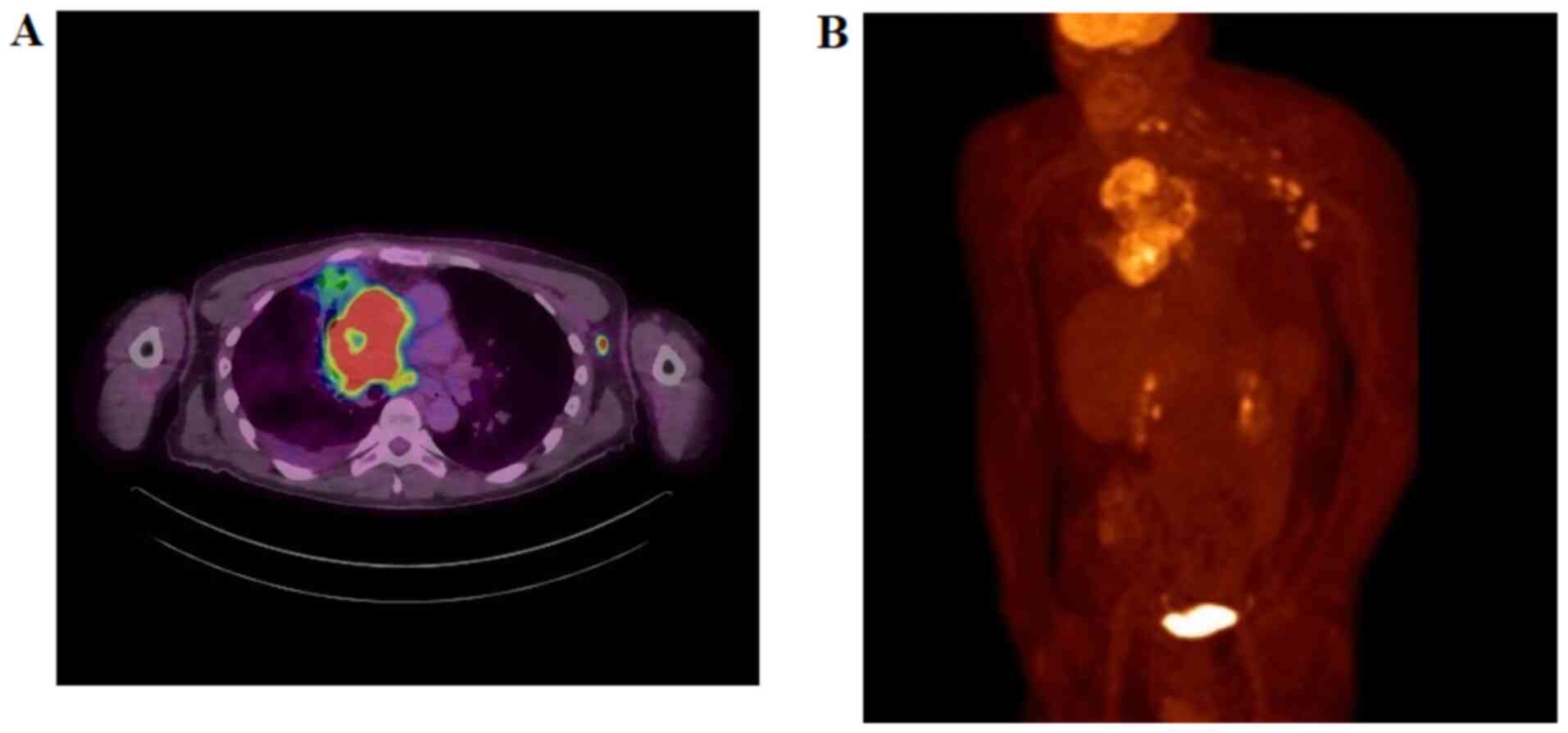
Follow-up staging with positron emission tomography (PET) revealed
hypermetabolic mediastinal, right hilar, and left axillary lymph
nodes (non-regional lymphadenopathy) suggestive of metastasis,
making this stage IV (Fig. 2).
Molecular studies performed on the biopsy tissue revealed the tumor
to be ALK, ROS1, KRAS, BRAF and EGFR wild type. PD-L1 (clone 22C3)
expression was 3%. The biopsy tissue stained negative for AFP. The
patient was not a surgical candidate and was started on a
palliative chemotherapy regimen of cisplatin (80 mg/m2)
and etoposide (100 mg/m2). He completed five cycles of
cisplatin/etoposide, with a dose reduction on the fifth cycle due
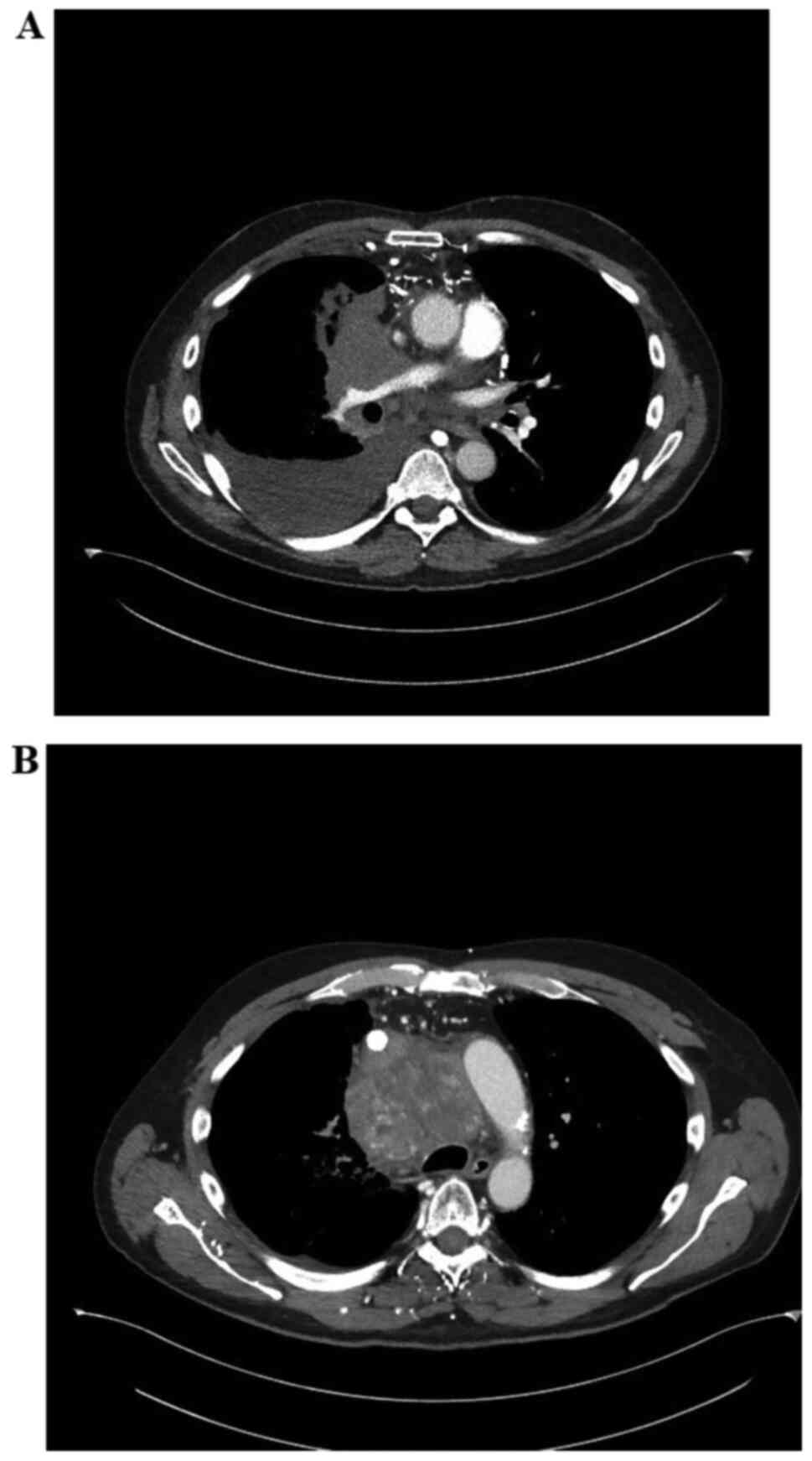
to anemia. A follow-up CT scan after the second cycle of
chemotherapy revealed interval decrease in size of the mediastinal
mass to 7.0x7.6 cm, however AFP had almost doubled in this time to
267 IU/ml (Fig. 3). Another
follow-up CT scan at the time of his last cycle revealed interval
development of a 3.2 cm right upper lobe mass. AFP was now 392
IU/ml. He was recommended to undergo palliative radiotherapy. No
concomitant chemotherapy was administered during this period. He
received 15 fractions of external beam RT to the mediastinal mass
totaling 37.5 Gy. AFP measured at the conclusion of radiotherapy
was 161 IU/ml. Follow-up CT scan 2 months after conclusion of
radiotherapy revealed the mediastinal mass to be roughly unchanged
in size at 6.8x8.2 cm. A moderate size right pulmonary effusion was
noted and the SVC was also noted to be completely occluded. The
patient underwent thoracentesis and no malignant cells were
detected within the thoracentesis sample. The SVC was recanalized
and stented successfully by interventional radiology (Fig. 4). Several months after this incident
he experienced a rapid decline in functional status and passed
away.
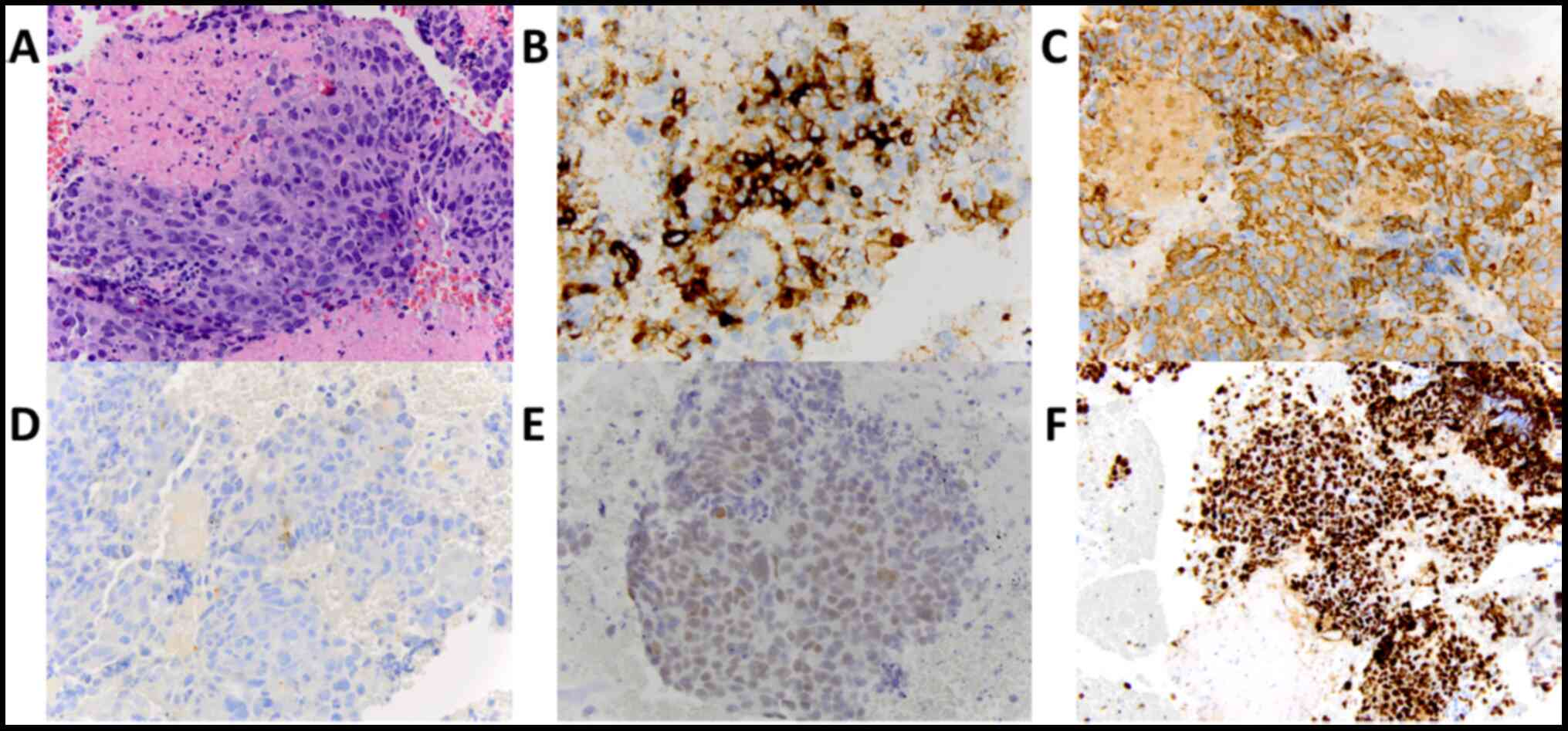 | Figure 1Immunohistochemical staining of tumor.
(A) Chromogranin staining, magnification, x40. (B) Hematoxylin and
Eosin staining, magnification, x40. (C) Pancytokeratin staining,
magnification, x40. (D) AFP staining, magnification, x40. (E) SALL4
staining, magnification, x40. (F) Ki67 staining, magnification,
x20. AFP, α-fetoprotein. |
Discussion
LCNEC is a rare form of cancer most frequently seen
in the lung. Here, we report a case of LCNEC presenting in the
anterior mediastinum associated with elevated AFP, which has only
been reported in the literature once before (27). The differential for this tumor
included lung adenocarcinoma extending into the mediastinum, SCLC,
and other tumors of the anterior mediastinum: Thymoma, thymic
carcinoma, lymphoma, and teratoma (28,29).
Our patient was initially suspected to have a teratoma as these
tumors have been known to present as a large mediastinal tumor with
elevated AFP (30). His tumor was
initially marginally responsive to standard SCLC
cisplatin/etoposide chemotherapy, but then the disease quickly
progressed on this regimen with development of a new lung mass. In
a previous study, 73% of LCNEC patients treated with
cisplatin/etoposide achieved at least a partial response, defined
as a 30% reduction in the sum of tumor diameters (23). Our patient unfortunately did not
achieve even this partial response, which could have been due to
the size of the tumor at the onset of therapy, or the inability of
the patient to complete the full course of chemotherapy.
AFP is known to be a valuable tumor marker in
hepatocellular carcinoma (HCC) to evaluate response to chemotherapy
and radiotherapy (31). In this
case, the patient's disease progressed while on chemotherapy,
associated with a significant rise in AFP. After receiving
palliative radiotherapy to the mediastinal mass, AFP decreased and
the patient's disease was stable for some time. While the biopsy
sample did not stain positive for AFP, these tumors are known to be
heterogenous and this does not rule out the possibility that a
portion of the mass that was not captured by biopsy was producing
AFP. The patient did not have HCC or a germ-cell tumor that could
have been responsible for this elevated AFP. These findings suggest
that the use of AFP as a tumor marker for some LCNECs may be worthy
of future exploration.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
Data sharing is not applicable to this article, as
no datasets were generated or analyzed during the current
study.
Authors' contributions
JK and DM wrote the manuscript. DM was the patient's
primary medical oncologist. MJV performed immunohistochemical
staining. HQ was the patient's primary radiation oncologist and
helped generate figures. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written consent was unobtainable as the patient
passed away prior to publication and it was not possible to contact
next of kin. The IRB of the University of Rochester reviewed this
work and confirmed that there is no identifying information and
that there are significant public interest considerations in the
publication of this work.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Buscemi S, Orlando E, Damiano G, Portelli
F, Palumbo VD, Valentino A, Marrazzo A, Buscemi G and Lo Monte AI:
‘Pure’ large cell neuroendocrine carcinoma of the gallbladder.
Report of a case and review of the literature. Int J Surg. 28
(Suppl 1):S128–S132. 2016.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Radović N, Turner R and Bacalja J: Primary
‘pure’ large cell neuroendocrine carcinoma of the urinary bladder:
A case report and review of the literature. Clin Genitourin Cancer.
13:e375–e377. 2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Okoye E, Choi EK, Divatia M, Miles BJ,
Ayala AG and Ro JY: De novo large cell neuroendocrine carcinoma of
the prostate gland with pelvic lymph node metastasis: A case report
with review of literature. Int J Clin Exp Pathol. 7:9061–9066.
2014.PubMed/NCBI
|
|
4
|
Ki EY, Park JS, Lee KH, Bae SN and Hur SY:
Large cell neuroendocrine carcinoma of the ovary: A case report and
a brief review of the literature. World J Surg Oncol.
12(314)2014.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Kawaratani H, Tsujimoto T, Yoshikawa M,
Kawanami F, Shirai Y, Yoshiji H, Morita K and Fukui H: Large cell
neuroendocrine carcinoma presenting with neck swelling in the
submandibular gland: A case report. J Med Case Rep.
7(81)2013.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Ogura J, Adachi Y, Yasumoto K, Okamura A,
Nonogaki H, Kakui K, Yamanoi K, Suginami K, Koyama T and Ikehara S:
Large-cell neuroendocrine carcinoma arising in the endometrium: A
case report. Mol Clin Oncol. 8:575–578. 2018.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kobayashi A, Yahata T, Nanjo S, Mizoguchi
M, Yamamoto M, Mabuchi Y, Yagi S, Minami S and Ino K: Rapidly
progressing large-cell neuroendocrine carcinoma arising from the
uterine corpus: A case report and review of the literature. Mol
Clin Oncol. 6:881–885. 2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Gu J, Gong D, Wang Y, Chi B, Zhang J, Hu S
and Min L: The demographic and treatment options for patients with
large cell neuroendocrine carcinoma of the lung. Cancer Med.
8:2979–2993. 2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Naidoo J, Santos-Zabala ML, Iyriboz T, Woo
KM, Sima CS, Fiore JJ, Kris MG, Riely GJ, Lito P, Iqbal A, et al:
Large Cell neuroendocrine carcinoma of the lung: Clinico-pathologic
features, treatment, and outcomes. Clin Lung Cancer. 17:e121–e129.
2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Gollard R, Jhatakia S, Elliott M and Kosty
M: Large cell/neuroendocrine carcinoma. Lung Cancer. 69:13–18.
2010.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Xuan WX, Li JJ, Shi YJ and Zhang XJ:
Atypical carcinoid: A rare finding of a man with mediastinal mass:
A case report. Mol Clin Oncol. 12:325–328. 2020.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Melosky B: Advanced typical and atypical
carcinoid tumours of the lung: Management recommendations. Curr
Oncol. 25 (Suppl 1):S86–S93. 2018.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Hiroshima K and Mino-Kenudson M: Update on
large cell neuroendocrine carcinoma. Transl Lung Cancer Res.
6:530–539. 2017.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Bari MF, Brown H, Nicholson AG, Kerr KM,
Gosney JR, Wallace WA, Soomro I, Muller S, Peat D, Moore JD, et al:
BAI3, CDX2 and VIL1: A panel of three antibodies to distinguish
small cell from large cell neuroendocrine lung carcinomas.
Histopathology. 64:547–556. 2014.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Filosso PL, Rena O, Guerrera F, Moreno
Casado P, Sagan D, Raveglia F, Brunelli A, Welter S, Gust L,
Pompili C, et al: Clinical management of atypical carcinoid and
large-cell neuroendocrine carcinoma: A multicentre study on behalf
of the European Association of Thoracic Surgeons (ESTS)
neuroendocrine tumours of the lung working group. Eur J
Cardiothorac Surg. 48:55–64. 2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Asamura H, Kameya T, Matsuno Y, Noguchi M,
Tada H, Ishikawa Y, Yokose T, Jiang SX, Inoue T, Nakagawa K, et al:
Neuroendocrine neoplasms of the lung: A prognostic spectrum. J Clin
Oncol. 24:70–76. 2006.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Rossi G, Bertero L, Marchiò C and Papotti
M: Molecular alterations of neuroendocrine tumours of the lung.
Histopathology. 72:142–152. 2018.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Rekhtman N, Pietanza MC, Hellmann MD,
Naidoo J, Arora A, Won H, Halpenny DF, Wang H, Tian SK, Litvak AM,
et al: Next-generation sequencing of pulmonary large cell
neuroendocrine carcinoma reveals small cell carcinoma-like and
non-small cell carcinoma-like subsets. Clin Cancer Res.
22:3618–3629. 2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Miyoshi T, Umemura S, Matsumura Y, Mimaki
S, Tada S, Makinoshima H, Ishii G, Udagawa H, Matsumoto S, Yoh K,
et al: Genomic profiling of large-cell neuroendocrine carcinoma of
the lung. Clin Cancer Res. 23:757–765. 2017.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Filosso PL, Guerrera F, Evangelista A,
Galassi C, Welter S, Rendina EA, Travis W, Lim E, Sarkaria I,
Thomas PA, et al: Adjuvant chemotherapy for large-cell
neuroendocrine lung carcinoma: Results from the European Society
for Thoracic Surgeons Lung Neuroendocrine Tumours Retrospective
Database. Eur J Cardiothorac Surg. 52:339–345. 2017.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Prelaj A, Rebuzzi SE, Del Bene G, Giròn
Berrìos JR, Emiliani A, De Filippis L, Prete AA, Pecorari S, Manna
G, Ferrara C, et al: Evaluation of the efficacy of
cisplatin-etoposide and the role of thoracic radiotherapy and
prophylactic cranial irradiation in LCNEC. ERJ Open Res.
3:00128–2016. 2017.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Cao L, Zhao L, Wang M, Zhang XH, Yang ZC
and Liu YP: Clinicopathological characteristics and prognosis of
pulmonary large cell neuroendocrine carcinoma aged 65 years. PeerJ.
7(e6824)2019.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Sun JM, Ahn MJ, Ahn JS, Um SW, Kim H, Kim
HK, Choi YS, Han J, Kim J, Kwon OJ, et al: Chemotherapy for
pulmonary large cell neuroendocrine carcinoma: Similar to that for
small cell lung cancer or non-small cell lung cancer? Lung Cancer.
77:365–370. 2012.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Rieber J, Schmitt J, Warth A, Muley T,
Kappes J, Eichhorn F, Hoffmann H, Heussel CP, Welzel T, Debus J, et
al: Outcome and prognostic factors of multimodal therapy for
pulmonary large-cell neuroendocrine carcinomas. Eur J Med Res.
20(64)2015.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Daido W, Yamasaki M, Saito N, Ishiyama S,
Deguchi N, Taniwaki M, Daga H and Ohashi N: Effectiveness of
nivolumab in large-cell neuroendocrine carcinoma of the lung-A
report of two cases. Gan To Kagaku Ryoho. 44:59–62. 2017.PubMed/NCBI(In Japanese).
|
|
26
|
Derks JL, Leblay N, Thunnissen E, van
Suylen RJ, den Bakker M, Groen HJM, Smit EF, Damhuis R, van den
Broek EC, Charbrier A, et al: Molecular subtypes of pulmonary
large-cell neuroendocrine carcinoma predict chemotherapy treatment
outcome. Clin Cancer Res. 24:33–42. 2018.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Takezawa K, Okamoto I, Fukuoka J, Tanaka
K, Kaneda H, Uejima H, Yoon HE, Imakita M, Fukuoka M and Nakagawa
K: Large cell neuroendocrine carcinoma of the mediastinum with
alpha-fetoprotein production. J Thorac Oncol. 3:187–189.
2008.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Juanpere S, Cañete N, Ortuño P, Martínez
S, Sanchez G and Bernado L: A diagnostic approach to the
mediastinal masses. Insights Imaging. 4:29–52. 2013.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Almeida PT and Heller D: Anterior
Mediastinal Mass. In: StatPearls (Internet). Available from:
urihttps://www.ncbi.nlm.nih.gov/books/NBK546608/simplehttps://www.ncbi.nlm.nih.gov/books/NBK546608/.
|
|
30
|
Yendamuri S: Resection of a giant
mediastinal teratoma. Ann Thorac Surg. 102:e401–e402.
2016.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Sanchez AIP, Roces LV, Garcia IZ, Lopez
EL, Hernandez MAC, Parejo MIB and Pena-Diaz J: Value of
α-fetoprotein as an early biomarker for treatment response to
sorafenib therapy in advanced hepatocellular carcinoma. Oncol Lett.
15:8863–8870. 2018.PubMed/NCBI View Article : Google Scholar
|