Introduction
Breast cancer is the leading global cause of
cancer-related death in females, and represents a major worldwide
health issue (1). In Egypt, breast
cancer is a major threat to the female population, representing
18.9% of total cancer cases (2).
Toll-like receptors (TLRs) are usually expressed by
immune cells such as macrophages, dendritic cells, mast cells and
eosinophils, as well as some epithelial cells (3). TLRs play a central role in the
recognition of harmful molecules from invading microorganisms or
internal tissue damage, activating specific transcriptional
responses including the NF-κB, Mitogen-activated protein kinase and
interferon regulatory factor pathways, which result in inflammation
(4). TLR4 was the first TLR to be
discovered in humans, and is one of the most conspicuous members of
the TLR family, expressed by both immune and non-immune cells
(5). Upregulation of TLR4 is
positively associated with the increased occurrence of metastasis
in patients with breast cancer (6).
TLR2 is expressed by numerous cell types of the
innate and adaptive immune systems (7). Stimulation of TLR2 on the surface of
breast cancer cells has been reported to increase disease severity
by promoting NF-κB signaling (8).
Furthermore, increasing evidence suggests that TLR2 signaling may
protect tumor cells from host immune surveillance and attack
(8).
Dynamic regulation of TLR signaling is essential to
the prevention of chronic inflammation and tissue destruction
(9). A number of mechanisms have
been reported to negatively regulate TLR responses, including cell
membrane-bound TLR suppressors and soluble TLRs (sTLRs) (9). One of the major negative regulators of
TLR-signaling is the generation of extracellular sTLRs, which serve
as decoy receptors to impede ligand-induced signaling (10). In the human immune system, sTLR2 is
reported to suppress TLR2-mediated inflammation in part by
preventing binding to its co-receptor CD14(11). sTLR2 is believed to be generated by
protease cleavage or ectodomain shedding, resulting in ≥6 distinct
sTLR2 polypeptides, which have been identified in human breast
milk, plasma and monocyte culture supernatants (12). A soluble form of the extracellular
TLR4 domain (sTLR4) and myeloid differentiation factor 2 (MD-2)
combine to form an sTLR4/MD-2 complex which inhibits TLR4
signaling, potentially by preventing the interaction between
membrane-bound TLR4 and its ligand (13).
In summary, numerous research groups have reported
that TLRs are expressed on both host immune and tumor cells, where
they influence the immune response, uncontrolled tumor
proliferation, resistance to apoptosis, metastasis and tumor cell
escape from immune surveillance (14).
A number of concerns about the impact of the
endogenous negative regulation of TLR signaling on host immune and
tumor cells remain unresolved. On this basis, the aim of the
present study was to assess the serum levels of sTLR2 and 4 as
negative regulators of TLR2 and TLR4 signaling, and to investigate
their association with the clinicopathological parameters of
patients with breast cancer.
Subjects and methods
Subjects
A total of 150 female subjects were recruited into
the present study, and were classified into the following groups:
Group I, 50 healthy control subjects with no history of breast
cancer; Group II, 50 subjects recently diagnosed with
non-metastatic breast cancer; and Group III, 50 subjects with
metastatic breast cancer. All patients were recruited from the
Damanhour Oncology Center (Damanhour, Egypt) between August 2016
and December 2018. Demographics data were obtained from all
participants and included age, menopausal status, number of
children, lactation history, marital status and family history of
breast cancer. The present study was approved by the ethics
committee of Damanhour oncology center (reference no. 3/8 PB4) and
informed consent was obtained from each participant.
Exclusion criteria
Patients with autoimmune diseases, other types of
malignancy, liver and kidney diseases were excluded from the
present study.
Sample collection
A 5-ml sample of whole blood was collected from each
subject after an overnight fast. The blood samples were allowed to
clot for 15 min at room temperature and then centrifuged for 10 min
at 12,000 x g (14.810 g). The separated serum was stored at -20˚C
for the assessment of serum sTLR2 and sTLR4 levels by ELISA.
Measurement of serum sTLRs
The levels of serum sTLR2 and 4 were determined
using Human Soluble Toll-like receptor 2 and 4 ELISA kits (cat.
nos. In-Hu4102 and In-Hu4103, respectively; Bioneovan Co., Ltd.),
according to the manufacturer's protocols.
Statistical analysis
The data were analyzed using the SPSS software
package version 20.0 (IBM Corp). Qualitative data are presented as
counts and percentages. Comparisons between the categorical
variables of different groups were assessed using the χ2
test. Normally distributed quantitative data are presented as the
mean ± standard deviation, while non-normally distributed data are
expressed as the median, minimum and maximum values. For normally
distributed data, comparisons between ≥2 groups were conducted
using the F-test (one-way ANOVA) Duncan method. For correlation
analysis, the Pearson's correlation coefficient (r) was
calculated.
Receiver operating characteristic (ROC) curve
statistics were applied to determine assay sensitivity and
specificity. In order to determine the diagnostic accuracy of the
combination of biomarkers, logistic regression analysis was used to
estimate the predicted probabilities, which were subsequently used
to generate a ROC curve. The method described by DeLong was used
for comparing the area under the ROC curves (AUCs). P≤0.05 was
considered to indicate a statistically significant difference, and
significance test results are quoted as two-tailed
probabilities.
Results
Demographical data
Patients in both the metastatic and non-metastatic
breast cancer groups were significantly older than those in the
control group (P=0.013 and P=0.002, respectively; Table I). A family history of breast cancer
was also significantly more likely in patients with non-metastatic
breast cancer than in healthy controls (P=0.025; Table I). No significant differences were
detected between patients with breast cancer and the controls with
respect to lactation history and number of children (Table I).
 | Table IClinical characteristics of the
studied group. |
Table I
Clinical characteristics of the
studied group.
| Characteristics | Group I control | Group II ‘non
metastatic’ | Group III
‘metastatic’ | χ2
test | P-value | P1 | P2 | P3 |
|---|
| Age, years | | | | 12.25 | 0.013a | 0.013a | 0.002a | 0.282 |
|
Range | 28-66 | 30-69 | 32-71 | | | | | |
|
Mean ±
SD | 46.0±11.05 | 50.9±10.62 | 52.0±8.67 | | | | | |
| Family history, n
(%) | | | | 5.21 | 0.026a | 0.025a | 0.311 | 0.070 |
|
Negative | 39 (78.0) | 46 (92.0) | 41 (82.0) | | | | | |
|
Positive | 11 (22.0) | 4 (8.0) | 9 (18.0) | | | | | |
| Lactation history,
n (%) | | | | 2.32 | 0.125 | 0.365 | 0.111 | 0.189 |
|
No | 8 (16.0) | 5 (10.0) | 4 (8.0) | | | | | |
|
Yes | 42 (84.0) | 45 (90.0) | 46 (92.0) | | | | | |
| No of children, n
(%) | | | | 1.65 | 0.366 | 0.296 | 0.216 | 0.409 |
|
1-3 | 22 (44.0) | 19 (38.0) | 22 (44.0) | | | | | |
|
4-5 | 18 (36.0) | 22 (44.0) | 22 (44.0) | | | | | |
|
6+ | 4 (8.0) | 4 (8.0) | 6 (12.0) | | | | | |
A significant increase in the number of grade III
patients was detected among those with metastatic, compared with
those with non-metastatic breast cancer (P=0.0001; Table II). Patients with non-metastatic
breast cancer showed a significant increase in tumor size and
regional lymph node involvement compared with the metastatic
patients (P=0.001). Moreover, a significant increase in distant
metastasis was also observed in the metastatic, compared with the
non-metastatic patients (P=0.0001; Table II).
| Table IIClinical characteristics of patients
with breast cancer. |
Table II
Clinical characteristics of patients
with breast cancer.
| | Group II ‘non
metastatic’ | Group III
‘metastatic’ | |
|---|
| Patient
characteristics | No. | % | No. | % | χ2
test | P-value |
|---|
| Menopausal
status | | | | | 2.36 | 0.2140 |
|
Premenopausal | 21 | 42.0 | 24 | 48.0 | | |
|
Postmenopausal | 29 | 58.0 | 26 | 52.0 | | |
| Pathology | | | | | 2.08 | 0.1060 |
|
Infiltrating
ductal carcinoma | 44 | 88.0 | 48 | 96.0 | | |
|
Infiltratin
globular carcinoma | 6 | 12.0 | 2 | 4.0 | | |
| HER2 | | | | | 4.083 | 0.0433a |
|
Positive | 30 | 60.0 | 37 | 74.0 | | |
|
Negative | 20 | 40.0 | 13 | 26.0 | | |
| PR | | | | | 4.504 | 0.0330a |
|
Positive | 16 | 32.0 | 9 | 18.0 | | |
|
Negative | 34 | 68.0 | 41 | 82.0 | | |
| ER | | | | | 0.000 | >0.9999 |
|
Positive | 10 | 20.0 | 10 | 20.0 | | |
|
Negative | 40 | 80.0 | 40 | 80.0 | | |
| Lymphovascular
invasion | | | | | 13.2 | 0.0010a |
|
Positive | 12 | 24.0 | 23 | 46.0 | | |
|
Negative | 38 | 76.0 | 27 | 54.0 | | |
| T stage | | | | | 173.1 | 0.0010a |
|
I | 2 | 4.0 | 20 | 40.0 | | |
|
II | 27 | 54.0 | 24 | 48.0 | | |
|
III | 19 | 38.0 | 5 | 10.0 | | |
|
IV | 2 | 4.0 | 1 | 2.0 | | |
| N stage | | | | | 297.5 | 0.0010a |
|
0 | 1 | 2.0 | 18 | 36.0 | | |
|
1 | 11 | 22.0 | 9 | 18.0 | | |
|
2 | 24 | 48.0 | 19 | 38.0 | | |
|
3 | 14 | 28.0 | 4 | 8.0 | | |
| M stage | | | | | 25.6 | 0.0001a |
|
Positive | 0 | 0.0 | 50 | 100.0 | | |
|
Negative | 50.0 | 100.0 | 0 | 0.0 | | |
| Grade | | | | | 36.2 | 0.0001a |
|
I | 38 | 76.0 | 3 | 6.0 | | |
|
II | 11 | 22.0 | 44 | 88.0 | | |
|
III | 1 | 2.0 | 3 | 6.0 | | |
| Presentation | | | | | 504.417 | 0.001a |
|
Breast
lump | 38 | 76.0 | 0 | 0.0 | | |
|
Nipple
retraction | 4 | 8.0 | 47 | 94.0 | | |
|
Inflammed
swollen breast | 1 | 2.0 | 1 | 2.0 | | |
|
Nipple and
areola ulcer | 1 | 2.0 | 1 | 2.0 | | |
|
Nipple
discharge | 6 | 12.0 | 1 | 2.0 | | |
The patients with metastatic breast cancer also
exhibited a significant increase in human epidermal growth factor 2
receptor (HER2) expression compared with the non-metastatic
patients (P=0.0433). However, a significant increase in
progesterone receptor (PR) expression was detected in the
non-metastatic, compared with the metastatic patients (P=0.033;
Table II). A significant increase
in the number of breast lumps was detected in non-metastatic breast
cancer compared with metastatic patients. On the other hand, a
significant increase in nipple retraction was observed in the
metastatic patients compared with the non-metastatic patients
(P=0.001; Table II). No significant
differences in estrogen receptor (ER) expression, menopausal status
and pathology were detected between patients with metastatic and
non-metastatic breast cancer (Table
II).
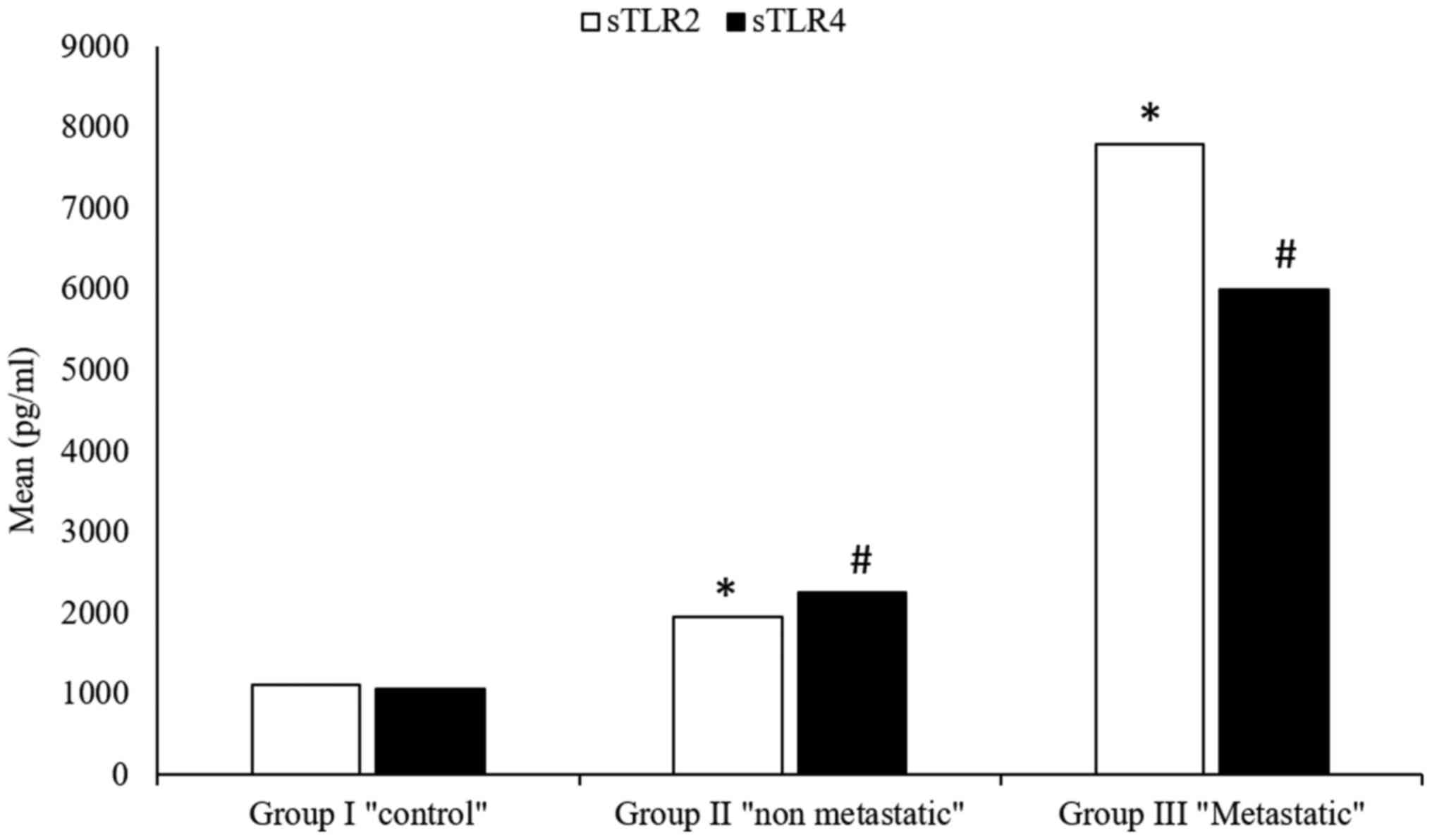
Serum sTLR2
A high significant increase in the levels of serum
sTLR2 were detected in patients with both metastatic
(5,997.4±8,585.23) and non-metastatic (2,258.2±1,832.44) breast
cancer, compared with the control group (1,106.8±99.93) (P=0.0001;
Table III) (Fig. 1). Furthermore, a highly significant
increase in serum sTLR2 was detected in metastatic breast cancer
patients (5,997.4±8,585.23) compared with non-metastatic patients
(2,258.2±1,832.44; P=0.0001; Table
III) (Fig. 1).
| Table IIIsTLR2 in the studied groups. |
Table III
sTLR2 in the studied groups.
| sTLR2 | Group I
control | Group II ‘non
metastatic’ | Group III
‘metastatic’ | ANOVA test | P-value | P1 | P2 | P3 |
|---|
| Range, pg/ml | 823-1349 | 1,043.5-8,460 | 1,143.5-23,895 | | | | | |
| Mean ± SD,
pg/ml | 1,106.8±99.93 |
2,258.2±1,832.44 |
5,997.4±8,585.23 | 33.2 | 0.0001a | 0.0001a | 0.0001a | 0.0001a |
Serum sTLR4
Compared with the healthy control group
(1,106.8±108.32), a highly significant increase in serum sTLR4
level was detected in both metastatic (7,800.1±13,041.28) and
non-metastatic (1,945.2±1,709.53) patients (P=0.0001; Table IV) (Fig. 1). The increase in serum sTLR4
between metastatic and non-metastatic patients was also observed
(P=0.0001) (Table IV) (Fig. 1).
| Table IVSerum sTLR4 in the studied
groups. |
Table IV
Serum sTLR4 in the studied
groups.
| sTLR4 | Group I
control | Group II ‘non
metastatic’ | Group III
‘metastatic’ | ANOVA test | P-value | P1 | P2 | P3 |
|---|
| Range, pg/ml | 923-1,296 | 1,210.5-7,285 | 1,002-33,615 | | | | | |
| Mean ± SD,
pg/ml | 1,106.8±108.32 |
1,945.2±1,709.53 |
7,800.1±13,041.28 | 32.1 | 0.0001a | 0.0001a | 0.0001a | 0.0001a |
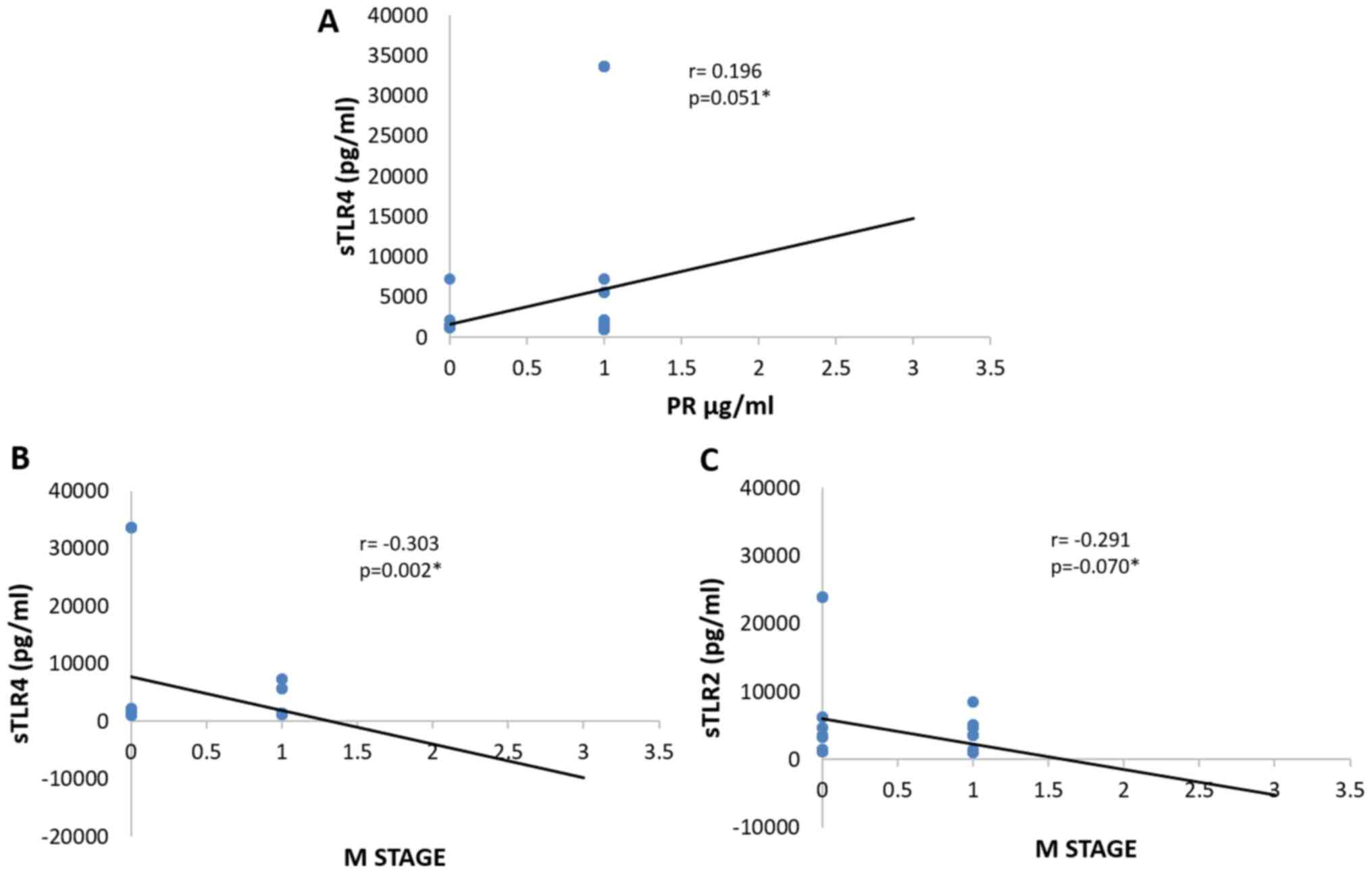
Correlation between serum sTLR2 and 4
expression and clinicopathological parameters of patients with
breast cancer
A significant negative correlation between serum
sTLR4 and distant metastasis (r=-0.303; P=0.002) (Table V and Fig. 2B) was observed in patients with
breast cancer. A negative correlation was also detected between
serum sTLR2 and distant metastasis (r=-0.291; P=0.003) (Table V and Fig. 2C). sTLR4 expression was positively
correlated with that of PR (r=0.196; P=0.05) (Table V and Fig. 2A), but not with HER-2 and ER
expression, lymphovascular invasion, number of lymph nodes, tumor
size and tumor grade in patients with breast cancer (Table V).
| Table VPearson's correlation between both
serum sTLR2 and serum sTLR4 and clinical characteristics of
patients with breast cancer. |
Table V
Pearson's correlation between both
serum sTLR2 and serum sTLR4 and clinical characteristics of
patients with breast cancer.
| Parameters | sTLR4 | sTLR2 |
|---|
| HER2 | | |
|
R value | -0.004 | -0.018 |
|
P-value | 0.971 | 0.859 |
| PR | | |
|
R value | 0.196 | 0.142 |
|
P-value | 0.051a | 0.160 |
| ER | | |
|
R value | 0.098 | 0.099 |
|
P-value | 0.332 | 0.327 |
| Lymphovascular
invasion | | |
|
R value | 0.192 | -0.011 |
|
P-value | 0.056 | 0.914 |
| M stage | | |
|
R value | -0.303 | -0.291 |
|
P-value | 0.002a | 0.003a |
| N stage | | |
|
R value | 0.093 | -0.070 |
|
P-value | 0.355 | 0.487 |
| T stage | | |
|
R value | -0.023 | -0.101 |
|
P-value | 0.819 | 0.316 |
| Grade | | |
|
R value | 0.009 | -0.101 |
|
P-value | 0.928 | 0.319 |
On the other hand, breast cancer patients showed no
significant correlation between serum sTLR2 and other
clinicopathological parameters, such as HER2, progesterone and
estrogen receptor expression, lymphovascular invasion, number of
lymph nodes, tumor size and tumor grade (Table V).
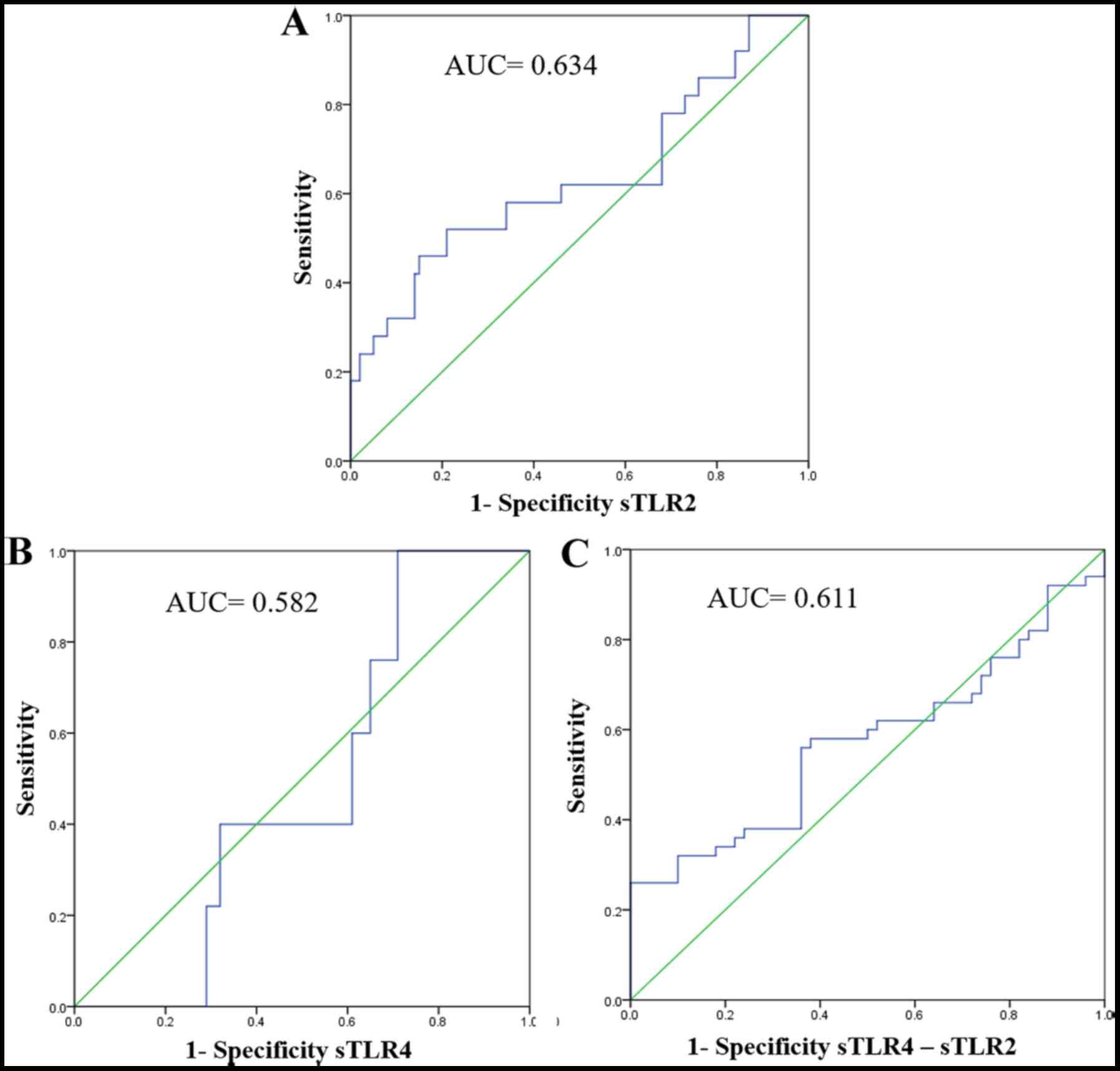
Sensitivity and specificity of serum
sTLR2
ROC analysis revealed a significant increase in
sensitivity, specificity and accuracy (P=0.008). For sTLR2, the AUC
was 0.634, sensitivity was 65%, specificity was 70% and accuracy
was 69% (Table VI and Fig. 3A).
| Table VISensitivity, specificity and accuracy
of sTlr2, sTLR4 and sTLR4/sTLR2 detection. |
Table VI
Sensitivity, specificity and accuracy
of sTlr2, sTLR4 and sTLR4/sTLR2 detection.
| | Asymptotic 95%
confidence interval | |
|---|
| sTLR | AUC | Std. Error | P-value | Lower bound | Upper bound | Sensitivity, % | Specificity, % | Accuracy, % | PPV, % | NPV, % |
|---|
| sTlr2 | 0.634 | 0.052 | 0.008 | 0.532 | 0.735 | 65.0 | 70.0 | 69.0 | 72.0 | 64.0 |
| sTLR4 | 0.582 | 0.047 | 0.323 | 0.390 | 0.574 | 59.0 | 64.0 | 62.0 | 55.0 | 67.0 |
| sTLR4-sTLR2 | 0.611 | 0.059 | 0.217 | 0.457 | 0.686 | 63.0 | 64.0 | 62.0 | 58.0 | 69.0 |
Table VI.
Sensitivity, specificity and accuracy of sTlr2 detection.
Sensitivity and specificity of serum
sTLR4
ROC curve analysis revealed no significant
sensitivity, specificity or accuracy for the detection of sTLR4 as
a marker for breast cancer (Table
VI and Fig. 3B).
Sensitivity and specificity of serum
sTLR2 and serum TLR4 detection in patients with breast cancer
ROC curve analysis revealed non-significant
increases in sensitivity, specificity and accuracy for combination
detection of sTLR2 and sTLR4 (P=0.217). The area under the ROC
curve was 0.611 with a sensitivity of 63%, specificity of 64% and
an accuracy of 62% (Table VI and
Fig. 3C).
Discussion
TLRs are widely expressed on tumor cells and are
involved in the initiation and progression of breast cancer
(15). TLR2 stimulation on the
surface of breast cancer cells has been demonstrated to increase
invasive potential by promoting NF-κB signaling (8). Breast cancer cells possess high
expression levels of TLR4, indicating that this receptor is
critical to the development of breast cancer (16).
The role of TLR2 and 4 signaling in breast cancer
progression has been documented in a number of different studies,
and both receptors have been implicated in the activation of
various transcription factors, including NF-κB (17). It is therefore critical that the TLR
system be tightly regulated in both the physiological and
pathological state, as aberrant inflammatory reactions result in
detrimental effects to the host (9).
To the best of our knowledge, the present study is
the first to investigate the roles of sTLRs in breast cancer
progression. On this basis, the aim of the present study was to
assess the serum levels of sTLR2 and 4 as endogenous negative
regulators of TLR2 and TLR4 signaling in patients with breast
cancer, and to investigate their correlation with different
clinicopathological parameters. The present study revealed an
increase in serum sTLR2 and 4 levels, indicating their roles as
endogenous negative regulators of TLR2 and TLR4 signaling in breast
cancer. This finding is consistent with a study conducted by
Houssen et al (9) in 2016.
In 2018, Hossain et al (18)
also observed increased serum sTLR2 concentrations in a number of
inflammatory diseases and disease models, including severe
bacterial infection (19), multiple
sclerosis (18), experimental human
endotoxemia (13) and the
autoimmune disease systemic lupus erythematous (SLE), where it
serves as a biomarker for disease activity (9). This increase was attributed to the
negative regulatory roles of sTLRs, which are achievable via
different molecular mechanisms (18). Firstly, sTLRs act as decoy receptors
by binding to ligands recognized by TLR2, without activating
intracellular signaling cascades, thus reducing the efficiency of
TLR2 signaling (18). The second
mechanism is via the disruption of the close proximity between TLR2
and its coreceptor CD14, which is crucial for efficient signaling.
Such disruption most likely results from the capacity of sTLR2 to
interact with CD14(20).
Alternatively, sTLR2 may homodimerize with cell surface TLR2 to
inhibit signaling via the membrane bound receptor (20).
Another novel observation of the present study was
that serum sTLR4 levels are significantly elevated in patients with
non-metastatic and metastatic breast cancer. This is in agreement
with a previous study by Ten Oever et al (13), who demonstrated that sTLR4 levels
were increased in those with inflammatory diseases, compared the
controls subjects. Furthermore, Wei et al (21) investigated the clinical significance
of serum sTLR4 in non-small cell lung cancer (NSCLC), and revealed
a significant increase in sTLR4 in patients, compared with healthy
controls.
As for the association between sTLR4 and
clinicopathological parameters, a significant positive correlation
was detected between sTLR4 and PR expression in patients with
breast cancer. This was also in agreement with the study by Wei
et al (21), who found a
positive correlation between serum sTLR4 levels and tumor stage in
patients with NSCLC.
Moreover, a negative correlation was also detected
between sTLR2 expression and distant metastasis. This was in
agreement with the 2016 study by Houssen et al (9), where a significant negative
correlation was observed between sTLR2 and the clinicopathological
parameters of patients with SLE. Serum sTLR2 was not significantly
correlated with clinicopathological parameters such as HER2 and PR
expression, lymphovascular invasion, the number of effected lymph
nodes, tumor size, grade and presentation of breast cancer, which
was also in agreement with Houssen et al (9) in patients with SLE. This negative
correlation may be ascribed to the role of TLR2 and 4 signaling in
the activation of NF-κB, that hence leads to increased expression
of cytokines and chemokines associated with leukocyte recruitment,
and subsequent inflammatory responses (8).
In the present study, the results of the ROC curve
analysis for sTLR4 were similar between patients with metastatic
and non-metastatic breast cancer. This is supported by Ten Oever
et al (13), who indicated
that the level of sTLR4 could not significantly differentiate
infectious from non-infectious inflammation when compared with c-
reactive protein. The elevated levels of sTLR4 and 2 as endogenous
negative regulators may be of prognostic and therapeutic value,
counteracting tumor immune evasion mediated by tumor cell TLRs
signaling, which results in the production of the proinflammatory
interleukins 6 and 12. These factors result in tumor cell
resistance to natural killer cell attack and evasion from immune
surveillance (22). These
observations are in agreement with those of Huang et al
(23), who found that TLR4
expression may contribute to tumor cell immune evasion, since
blocking the TLR4 pathway using small inhibitory RNA or TLR4
inhibitory peptides delays tumor growth and prolongs the survival
of tumor-bearing mice.
The primary limitation of the current study is the
small sample population. The expression levels of the studied
markers were only detected by ELISA, therefore we can only
hypothesize the role of sTLR2 and 4 as diagnostic and prognostic
markers of breast cancer.
In conclusion, the results of the present study
indicate that as endogenous negative regulators of TLR2 and TLR4
signaling, sTLR2 and 4 may be susceptible diagnostic and prognostic
markers for breast cancer. Further future studies are warranted to
validate the prognostic roles of these soluble receptors, and as a
promising target for personalized immunotherapy in patients with
breast cancer.
Acknowledgements
The authors acknowledge the efforts of Dr Doaa Ali
Abdelmonsif (Assistant Professor of Biochemistry, Faculty of
Medicine, Alexandria University) for her valuable support.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
MH designed the study and constructed the research
plan, collected and reviewed the literature, revised all draft
versions of the manuscript (including approving the final version)
and supervised all experimental research. GEK performed laboratory
analyses, reviewed the literature, and wrote the first and last
versions of the paper. AG recruited the patients and collected the
clinical data. TO revised the final version of the manuscript and
contributed to the biochemical analysis. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of the Faculty of Pharmacy, Damanhour University
(Damanhour, Egypt; reference no. 3/8 PB4). All patients provided
written informed consent prior to study commencement.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Nur Husna SM, Tan HT, Mohamud R, Dyhl-Polk
A and Wong KK: Inhibitors targeting CDK4/6, PARP and PI3K in breast
cancer. A review. Ther Adv Med Oncol.
10(1758835918808509)2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Dubey AK, Gupta U and Jain S: Breast
cancer statistics and prediction methodology: A systematic review
and analysis. Asian Pacific J Cancer Prev. 16:4237–4245.
2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ayala-Cuellar AP, Cho J and Choi KC:
Toll-like receptors: A pathway alluding to cancer control. J Cell
Physiol. 234:21707–21715. 2019.PubMed/NCBI View Article : Google Scholar
|
|
4
|
McGettrick AF and O'Neill LA: Localisation
and trafficking of Toll-like receptors: An important mode of
regulation. Curr Opin Immunol. 22:20–27. 2010.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Kawai T and Akira S: The role of
pattern-recognition receptors in innate immunity: Update on
Toll-like receptors. Nat Immunol. 11:373–384. 2010.PubMed/NCBI View
Article : Google Scholar
|
|
6
|
Ahmed A, Wang JH and Redmond HP: Silencing
of TLR4 increases tumor progression and lung metastasis in a murine
model of breast cancer. Ann Surg Oncol. 20 (Suppl 3):S389–S396.
2013.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Grimmig T, Moench R, Kreckel J, Haack S,
Rueckert F, Rehder R, Tripathi S, Ribas C, Chandraker A, Germer CT,
et al: Toll like receptor 2, 4, and 9 signaling promotes
autoregulative tumor cell growth and VEGF/PDGF expression in human
pancreatic cancer. Int J Mol Sci. 17(2060)2016.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Al-Harras MF, Houssen ME, Shaker ME, Farag
K, Farouk O, Monir R, El-Mahdy R and Abo-Hashem EM: Polymorphisms
of glutathione S-transferase π 1 and toll-like receptors 2 and 9:
Association with breast cancer susceptibility. Oncol Lett.
11:2182–2188. 2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Houssen ME, El-Mahdy RH and Shahin DA:
Serum soluble toll-like receptor 2: A novel biomarker for systemic
lupus erythematosus disease activity and lupus-related
cardiovascular dysfunction. Int J Rheum Dis. 19:685–692.
2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Dulay AT, Buhimschi CS, Zhao G, Oliver EA,
Mbele A, Jing S and Buhimschi IA: Soluble TLR2 is present in human
amniotic fluid and modulates the intraamniotic inflammatory
response to infection. J Immunol. 182:7244–7253. 2009.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Henrick BM, Yao XD, Taha AY, German JB and
Rosenthal KL: Insights into soluble Toll-like receptor 2 as a
downregulator of virally induced inflammation. Front Immunol.
7(291)2016.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Langjahr P, Díaz-Jiménez D, De la Fuente
M, Rubio E, Golenbock D, Bronfman FC, Quera R, González MJ and
Hermoso MA: Metalloproteinase-dependent TLR2 ectodomain shedding is
involved in soluble toll-like receptor 2 (sTLR2) production. PLoS
One. 9(e104624)2014.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Ten Oever J, Kox M, van de Veerdonk FL,
Mothapo KM, Slavcovici A, Jansen TL, Tweehuysen L,
Giamarellos-Bourboulis EJ, Schneeberger PM, Wever PC, et al: The
discriminative capacity of soluble Toll-like receptor (sTLR)2 and
sTLR4 in inflammatory diseases. BMC Immunol. 15(55)2014.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Domenis R, Cifù A, Marinò D, Fabris M,
Niazi KR, Soon-Shiong P and Curcio F: Toll-like receptor-4
activation boosts the immunosuppressive properties of tumor
cells-derived exosomes. Sci Rep. 9(8457)2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Bhattacharya D and Yusuf N: Expression of
toll-like receptors on breast tumors: Taking a toll on tumor
microenvironment. Int J Breast Cancer. 2012(716564)2012.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Yang CX, Li CY and Feng W: Toll-like
receptor 4 genetic variants and prognosis of breast cancer. Tissue
Antigens. 81:221–226. 2013.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Yusuf N: Toll-like receptors and breast
cancer. Front Immunol. 5(84)2014.
|
|
18
|
Hossain MJ, Morandi E, Tanasescu R,
Frakich N, Caldano M, Onion D, Faraj TA, Erridge C and Gran B: The
soluble form of toll-like receptor 2 is elevated in serum of
multiple sclerosis patients: A novel potential disease biomarker.
Front Immunol. 9(457)2018.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Holst B, Szakmany T, Raby AC, Hamlyn V,
Durno K, Hall JE and Labéta MO: Soluble Toll-like receptor 2 is a
biomarker for sepsis in critically ill patients with multi-organ
failure within 12 h of ICU admission. Intensive Care Med Exp.
5(2)2017.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Liew FY, Xu D, Brint EK and O'Neill LA:
Negative regulation of toll-like receptor-mediated immune
responses. Nat Rev Immunol. 5:446–458. 2005.PubMed/NCBI View
Article : Google Scholar
|
|
21
|
Wei F, Yang F, Li J, Zheng Y, Yu W, Yang L
and Ren X: Soluble Toll-like receptor 4 is a potential serum
biomarker in non-small cell lung cancer. Oncotarget. 7:40106–40114.
2016.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Huang B, Zhao J, Unkeless JC, Feng ZH and
Xiong H: TLR signaling by tumor and immune cells: A double-edged
sword. Oncogene. 27:218–224. 2008.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Huang B, Zhao J, Li H, He KL, Chen Y, Chen
SH, Mayer L, Unkeless JC and Xiong H: Toll-like receptors on tumor
cells facilitate evasion of immune surveillance. Cancer Res.
65:5009–5014. 2005.PubMed/NCBI View Article : Google Scholar
|