Introduction
External auditory canal carcinoma (EACC) is an
extremely rare disease with an incidence of approximately one in a
million and accounts for <1% of all head and neck cancers
(1,2). EACC often requires substantial
clinical time from the onset of symptoms to the diagnosis because
of its low incidence. The initial clinical symptoms of EACC are
nonspecific and include otorrhea, tinnitus, otalgia, hearing loss,
clogged ears, and bleeding. In patients with advanced stages of
EACC, facial paralysis is also present and is associated with poor
survival. Chronic stimulation, such as habitual ear picking, has
also been recognized as an important factor in the carcinogenesis
of EACC (3).
Squamous cell carcinoma is the most common
histological type of EACC and accounts for 80-90% of cases,
followed by adenoid cystic carcinoma, basal cell carcinoma, and
adenocarcinoma (4). Several
criteria have been formulated in the clinical staging system of
EACC. According to the 8th edition of the American Joint Committee
on Cancer staging manual on the tumor, node, and metastasis staging
system, EACC is classified as cutaneous cancers of the head and
neck. The Stell and McCormick staging system is based on staging of
external auditory canal and middle ear carcinomas (5). The modified Pittsburgh staging system
(6) is also widely used in external
auditory squamous cell carcinoma, which originates from the Arriaga
staging system (7) based on
preoperative clinical examination and computed tomography (CT)
findings. Although there is no universally accepted staging system,
the modified Pittsburgh staging system is valuable for clinical
decision-making (8).
Surgery is the mainstay of treatment for early stage
EACC (9). Radiotherapy is indicated
in the following cases: i) Radical treatment for patients unable to
undergo surgery, ii) postoperative treatment for patients who have
undergone surgical resection, but having a high risk of recurrence
(e.g., positive margins and locally advanced cases), and iii)
preoperative treatment for medically operable and locally advanced
cases. Multimodal treatment combining local and systemic treatment
approaches is advised for locally advanced cases; however, optimal
treatment remains controversial.
Performing a large statistical examination is often
difficult in a single institution because of the limited number of
cases. Hence, careful consideration of these cases is important.
This retrospective study aimed to evaluate the feasibility and
efficacy of external beam radiotherapy (EBRT) with or without
surgery for patients with EACC. We reviewed approximately 20 years
of EACC treatment in our institution.
Materials and methods
We retrospectively reviewed 34 consecutive patients
with EACC treated by curative EBRT with or without surgery between
February 2001 and January 2019. The inclusion criteria were as
follows: histologically confirmed cases of primary EACC, cases
treated using EBRT with curative intent, cases with no evidence of
distant metastasis at the time of diagnosis, and no prior
radiotherapy to the temporal bone region. The exclusion criteria
were as follows: Radiotherapy for palliative intent cases and lack
of sufficient medical records to confirm EACC or to decide the
treatment modality. The clinical staging was performed according to
the modified Pittsburgh staging system, because a recent study had
been reported the clinical usefulness of that staging system
(8). Acute and late adverse events
were graded according to the National Cancer Institute Common
Toxicity Criteria for Adverse Events, version 4.0.
CT of the patients for planning the radiation
therapy was performed while wearing a thermoplastic mask. All
patients underwent radiotherapy with 4-6 MV photon linear
accelerators by radiation technologies of three-dimensional
conformal radiotherapy (3D-CRT), static intensity-modulated
radiotherapy (IMRT), or volumetric modulated arc therapy (VMAT).
The CT image data were reconstructed with a slice thickness of 5 mm
for 3D-CRT and 2 mm for IMRT or VMAT. The clinical target volume
(CTV) included the primary tumor and clinically positive lymph
nodes. The CTV included the tumor bed for the postoperative cases.
The planning target volume included the CTV with a minimum added
margin of 3-5 mm. No patient received prophylactic irradiation for
the clinically negative neck.
Statistical analysis
The R statistical package (The R Foundation for
Statistical Computing, Vienna, Austria) was used for data analyses.
For comparison of the proportions of patient's characteristics in
two groups, the Fisher exact test was used. Overall survival (OS),
progression-free survival (PFS), and cancer-specific survival (CSS)
rates were calculated from the first day of initial therapy by the
Kaplan-Meier method. PFS was defined as the time from initial
therapy to first evidence of radiological or clinical tumor
progression, or until death from any cause. A univariate Cox
proportional hazard analysis was performed, since a small sample
size made it difficult to conduct a multivariate analysis to reach
a valid conclusion. The P-values of <0.05 were considered
statistically significant.
Results
In this study, 34 patients were retrospectively
analyzed. The median follow-up period for these patients was 22.4
months (range: 2-205 months). The pathological diagnosis of all
patients was predominantly squamous cell carcinoma (31 patients),
followed by adenoid cystic carcinoma (1 patient), undifferentiated
carcinoma (1 patient), and poorly differentiated adenocarcinoma (1
patient). Of all the patients, 18 received definitive radiotherapy
(dRT) and 16 received EBRT combined with surgery (S+RT). The median
follow-up period for the dRT and S+RT groups was 15.3 (range: 2-205
months) and 75.1 months (range: 5-169 months), respectively.
Patient characteristics for both the groups are presented in
Table I. The S+RT group had a
higher ratio of male patients and better Karnofsky Performance
Status (KPS) compared to the dRT group. No statistically
significant difference was observed between the two groups in terms
of patient age, clinical stage, pathology, and prescribed dose. The
entire cohort consisted of 19 men and 15 women, with a median age
of 66 years (range: 32-86 years). According to the modified
Pittsburgh staging system, 21% of the patients were classified in
early stage and 79% in advanced stage of EACC.
 | Table IPatient characteristics of 34 patient
with external auditory canal carcinoma in our institution. |
Table I
Patient characteristics of 34 patient
with external auditory canal carcinoma in our institution.
| Characteristics | dRT group (n
=18) | S+RT group (n
=16) | P-value |
|---|
| Age, median
(range) | 68 (46-86) | 65 (32-75) | 0.925 |
| Sex | | | 0.045 |
|
Male | 7 (39%) | 12 (75%) | |
|
Female | 11 (61%) | 4 (25%) | |
| KPS, median
(range) | 80 (70-100) | 90 (80-100) | 0.008 |
| Clinical stage | | | 0.214 |
|
Early
(I/II) | 2 (11%) | 5 (31%) | |
|
Advanced
(III/IV) | 16 (89%) | 11 (69%) | |
| Pathology | | | 0.591 |
|
SqCC | 17 (94%) | 14 (88%) | |
|
ACC | 0 | 1 (6%) | |
|
Others | 1 (6%) | 1 (6%) | 0.446 |
| Prescribed dose,
median (range) | 70 Gy (50-70 Gy) | 66 Gy (60-70 Gy] | |
The radiotherapy characteristics of the patients are
shown in Table II. In the dRT
group, 13 patients underwent EBRT concurrently with chemotherapy or
biotherapy, which consisted of the docetaxel platinum plus
5-fluorouracil (DCF) regimen, platinum plus 5-fluorouracil (CF)
regimen, single-agent platinum regimen, and cetuximab.
| Table IIRadiotherapy characteristics of 34
patient with external auditory canal carcinoma in the University of
Tokyo Hospital. |
Table II
Radiotherapy characteristics of 34
patient with external auditory canal carcinoma in the University of
Tokyo Hospital.
| Treatment type | N | Percentage (%) |
|---|
| Definitive
radiotherapy | 18 | 53 |
|
Bioradiotherapy
(cetuximab) | 1 | |
|
CCRT | 12 | |
|
Docetaxel +
Cisplatin + 5FU (DCF) | 8 | |
|
Cisplatin +
5-FU (CF) | 2 | |
|
Daily
Cisplatin | 2 | |
|
RT
alone | 5 | |
| Radiotherapy with
surgery | 16 | 47 |
|
Postoperative
(RT alone) | 10 | |
|
Pre +
postoperative | 6 | |
|
RT
alone | 4 | |
|
Chemoradiotherapy
(including NAC) | 2 | |
The S+RT group underwent postoperative radiotherapy
(n=10) and pre- and/or postoperative radiotherapy (n=6). According
to the surgical treatment modalities, one patient underwent
mastoidectomy, seven patients underwent lateral temporal bone
resection, and eight patients underwent subtotal temporal bone
resection. All patients who received postoperative radiotherapy
underwent EBRT without chemotherapy. In total, there were six
patients in the pre- and/or postoperative radiotherapy group; four
patients received radiation therapy alone (without chemotherapy),
one patient received a daily low-dose of cisplatin concurrently
undergoing the pre- and/or postoperative radiation therapy, and one
patient received neoadjuvant chemotherapy consisting of cisplatin
and 5-fluorouracil prior to preoperative radiotherapy. The median
prescribed doses for the S+RT and dRT groups were 66 (range: 50-70
Gy) and 70 Gy (range: 60-70 Gy), respectively.
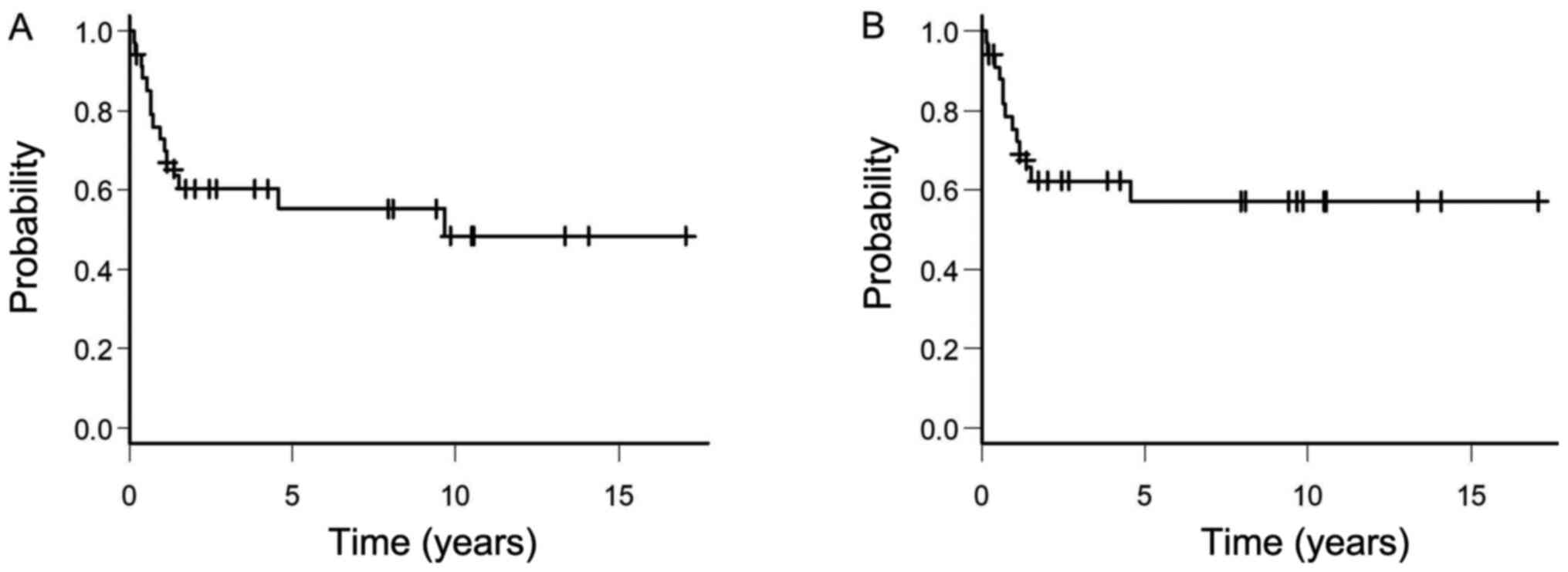
Of all the patients, 19 (56%) patients were alive at
the time of this analysis; the 5-year OS and CSS rates for the
entire cohort were 55.2 (95% confidence interval [CI]: 35.7-71.1%)
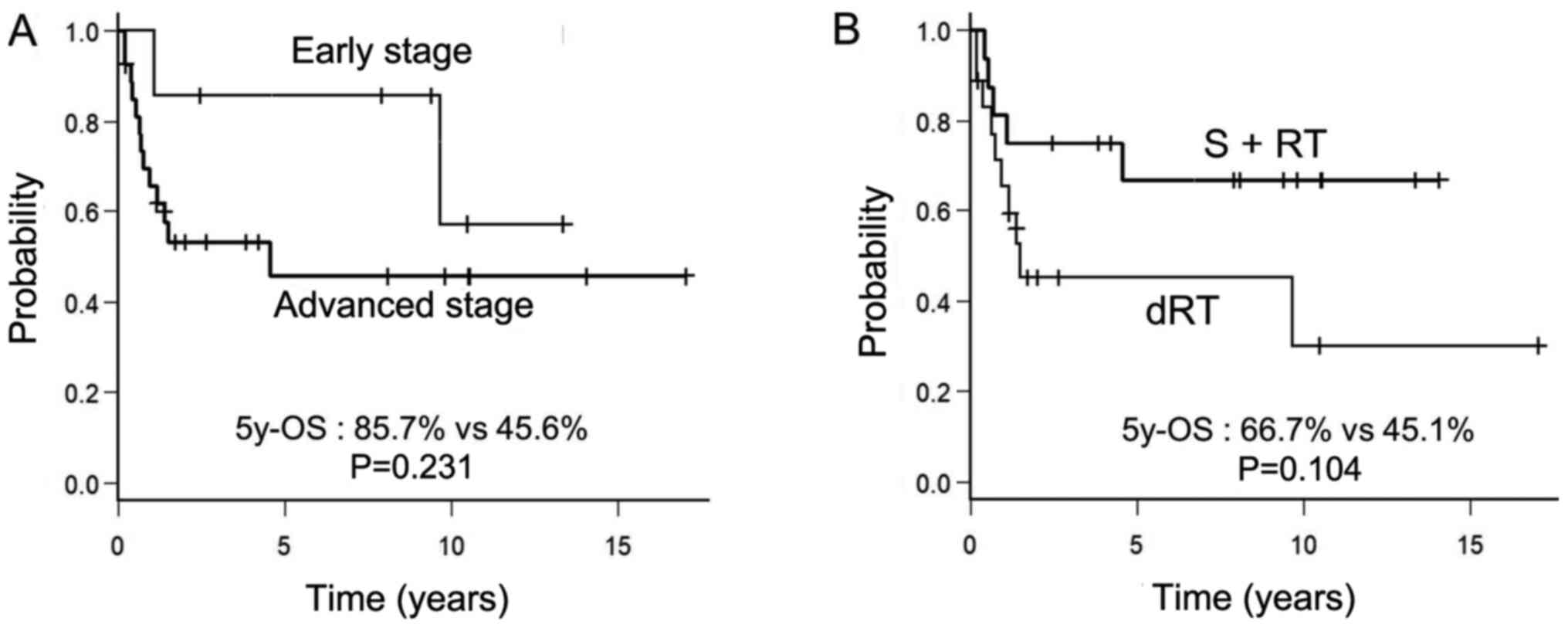
and 57.1% (95% CI: 37.0-72.9%), respectively (Fig. 1). The 5-year OS rates for the early
and advanced stages were 85.7 and 45.6%, respectively (Fig. 2A). There was no significant
statistical difference between the 5-year OS rates of both the
groups (Fig. 2B, 66.7 vs. 45.1%,
P=0.104). With reference to the univariate analysis (Table III), a factor associated with a
favorable OS rate included a good performance status of over or
equal to 90% (hazard ratio: 0.137, 95% CI: 0.043-0.434, and
P<0.001).
| Table IIIUnivariate Cox proportional hazard
analysis of overall survival. |
Table III
Univariate Cox proportional hazard
analysis of overall survival.
| Covariables | N | Hazard ratio | 95% CI | P-value |
|---|
| Age | | | | |
|
≤65 years
old | 16 | 1 | | |
|
>65 years
old | 18 | 1.529 | 0.542-4.312 | 0.422 |
| Sex | | | | |
|
Female | 15 | 1 | | |
|
Male | 19 | 0.647 | 0.234-1.788 | 0.401 |
| Performance
status | | | | |
|
<90% | 10 | 1 | | |
|
≥90% | 24 | 0.137 | 0.043-0.434 | <0.001 |
| Clinical stage | | | | |
|
Early | 7 | 1 | | |
|
Advanced | 27 | 2.493 | 0.558-11.130 | 0.231 |
| Pathological
type | | | | |
|
SqCC | 31 | 1 | | |
|
non
SqCC | 3 | 0.976 | 0.127-7.525 | 0.982 |
| Surgery | | | | |
|
No | 18 | 1 | | |
|
Yes | 16 | 0.406 | 0.137-1.204 | 0.104 |
| Chemotherapy | | | | |
|
No | 20 | 1 | | |
|
Yes | 14 | 1.300 | 0.460-3.679 | 0.621 |
Of all the patients, 14 (41.2%) developed
recurrences, including nine with local recurrences, two with
combined locoregional recurrences, and three with distant
metastases. The PFS rate at 5-year was 55.6% (95% CI: 36.5-71.1%)
for the entire cohort. A wide variety of metastatic sites,
including the lungs, liver, and bone, was observed in cases with
distant metastases. Salvage surgery was performed in one patient,
while chemotherapy was performed in three patients for patients
with recurrence. The remaining patients selected the option of best
supportive care. Among the patients treated with chemotherapy, one
patient received the CF regimen and two patients received oral S-1
administration. The median survival time after recurrence in
patients with recurrence was 2.9 months (range: 0.2-23 months).
Severe (Grade 3 or higher) radiation-induced late complications
were not observed.
Discussion
Our study evaluated the clinical outcomes of
patients treated with EBRT for EACC. Our results were consistent
with those of previous reports. A meta-analysis of 742 patients
reported that patients with external auditory canal squamous cell
carcinoma treated with chemoradiotherapy had a similar survival
rate (10). A multi-institutional
review of 87 patients that focused primarily on the roles of
surgery and radiotherapy in these patients discovered that the
5-year OS and disease-free survival rates were 55 and 54%,
respectively (11). Furthermore,
this review indicated that the clinical stage and treatment
modality were significant prognostic factors.
To the best of our knowledge, there are no
prospective or randomized trials about EACC treatment. For the
patient in early stage EACC, surgical resection with tumor free
margin is the most standard treatment (12,13).
Radical conventional radiotherapy also achieves favorable outcome,
which was considered as treatment option (14). Murai et al reported the
effectiveness of the stereotactic radiotherapy for a new treatment
option of EACC (15).
However, there is no clear consensus about treatment
strategies in advanced cases. Surgical resection in combination
with perioperative radiotherapy is more effective compared to a
single modality treatment (16-18).
Nakagawa et al used preoperative radiotherapy; their study
revealed that the tumor-free surgical margin had a significant
correlation with patient survival in locally advanced cases
(19). In another study conducted
by Choi et al they considered the necessity of postoperative
radiotherapy in accordance with the clinical stage (20). The disease control rates for
patients with early vs. advanced stages were 55.6 vs. 50% in the
postoperative radiotherapy group and 66.7 vs. 37.5% in the dRT
group. In this study, while the 5-year OS rate was higher in the
S+RT group, the difference did not reach statistical significance
(66.7 vs. 45.1%, P=0.104).
Despite the aggressive multidisciplinary treatment,
locoregional failure remains the most frequent recurrence; Yoon
et al reported a high propensity for locoregional failure of
EACC (21). Furthermore, they
reported nine local recurrences, eight regional recurrences, and
three distant metastases among 20 patients with recurrence. In our
study, locoregional failure was detected in 76% of patients with
recurrence. Therefore, a more aggressive local therapy could be
beneficial to some extent. Hayashi et al reported the
clinical outcome of carbon ion radiotherapy for external auditory
canal and middle ear carcinomas in a retrospective multicenter
study (22). They revealed that the
3-year local control and OS rates were 55 and 59%,
respectively.
The optimal chemotherapy regimen for concurrent
chemoradiotherapy in definitive radiotherapy is still
controversial. Several anticancer drugs, such as cisplatin,
carboplatin, fluorouracil, docetaxel, and mitomycin, are widely
used (10). Nagano et al
reported that the DCF regimen was potentially the most effective
method, with reference to their study that revealed a 100% 2-year
OS and locoregional control rate in six patients with advanced EACC
who had received this regimen (23). Other studies supported the use of an
intra-arterial cisplatin infusion in combination with radiotherapy
for locally advanced cases of EACC (24,25).
Several limitations existed in our study. First, the
most important limitation of present study is the low number of
cases and the retrospective nature of the study could have produced
a selection bias. Second, a long observation period resulted in a
substantial heterogeneity of treatment modality, such as
chemotherapy regimens, treatment modality, radiation technology,
and surgical procedure. Third, there was unclearness about decision
making process of the therapeutic strategies at the time of the
treatment because of retrospective data analysis. Fourth, our study
included different pathological types, which could have caused
inaccurate results in the study. Fifth, our data were dependent on
the medical records, which may be insufficient for accurately
describing all the patient characteristics and events, especially
in adverse event detection. This factor limited the availability of
patient covariates, and unmeasured confounding variables most
likely existed during the study.
In conclusion, our retrospective study reported the
clinical outcomes of EACC in our institution. No statistically
significant difference between the dRT and S+RT groups was
observed. However, the S+RT group had a better prognosis tendency
than the dRT group, which was consistent with a previous report.
Further studies and accumulation of data are needed to determine
the optimal treatment strategy for EACC in the future.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
AK was a major contributor to writing this report.
AK collected and assembled the data. HY and AK analyzed and
interpreted the clinical data. HY conceived of this study and
participated in its design and coordination. RT, MA, MY, TA and YS
contributed to the acquisition of data. OA and KN made substantial
contributions to interpretation of data. RT, HY, MA, MY, YS, TA, OA
and KN revised this report critically for important intellectual
content. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
Written informed consent was obtained from all
patients. The current study was approved the institutional review
board in the University of Tokyo Hospital (Tokyo, Japan).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kuhel WI, Hume CR and Selesnick SH: Cancer
of the external auditory canal and temporal bone. Otolaryngol Clin
North Am. 29:827–852. 1996.PubMed/NCBI
|
|
2
|
Nyrop M and Grøntved A: Cancer of the
external auditory canal. Arch Otolaryngol Head Neck Surg.
128:834–837. 2002.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Tsunoda A, Sumi T, Terasaki O and
Kishimoto S: Right dominance in the incidence of external auditory
canal squamous cell carcinoma in the Japanese population: Does
handedness affect carcinogenesis? Laryngoscope Investig
Otolaryngol. 2:19–22. 2017.PubMed/NCBI View
Article : Google Scholar
|
|
4
|
Devaney KO, Boschman CR, Willard SC,
Ferlito A and Rinaldo A: Tumours of the external ear and temporal
bone. Lancet Oncol. 6:411–420. 2005.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Stell PM and McCormick MS: Carcinoma of
the external auditory meatus and middle ear Prognostic factors and
a suggested staging system. J Laryngol Otol. 99:847–850.
1985.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Moody SA, Hirsch BE and Myers EN: Squamous
cell carcinoma of the external auditory canal: An evaluation of a
staging system. Am J Otol. 21:582–588. 2000.PubMed/NCBI
|
|
7
|
Arriaga M, Curtin H, Takahashi H, Hirsch
BE and Kamerer DB: Staging proposal for external auditory meatus
carcinoma based on preoperative clinical examination and computed
tomography findings. Ann Otol Rhinol Laryngol. 99:714–721.
1990.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Morita S, Mizumachi T, Nakamaru Y,
Sakashita T, Kano S, Hoshino K, Fukuda A, Fujiwara K and Homma A:
Comparison of the university of pittsburgh staging system and the
eighth edition of the american joint committee on Cancer TNM
classification for the prognostic evaluation of external auditory
canal cancer. Int J Clin Oncol. 23:1029–1037. 2018.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Matoba T, Hanai N, Suzuki H, Nishikawa D,
Tachibana E, Okada T, Murakami S and Hasegawa Y: Treatment and
outcomes of carcinoma of the external and middle Ear: The validity
of En bloc resection for advanced tumor. Neurol Med Chir (Tokyo).
58:32–38. 2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Takenaka Y, Cho H, Nakahara S, Yamamoto Y,
Yasui T and Inohara H: Chemoradiation therapy for squamous cell
carcinoma of the external auditory canal: A meta-analysis. Head
Neck. 37:1073–1080. 2015.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Ogawa K, Nakamura K, Hatano K, Uno T, Fuwa
N, Itami J, Kojya S, Nakashima T, Shinhama A, Nakagawa T, et al:
Treatment and prognosis of squamous cell carcinoma of the external
auditory canal and middle ear: A multi-institutional retrospective
review of 87 patients. Int J Radiat Oncol Biol Phys. 68:1326–1334.
2007.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Bacciu A, Clemente IA, Piccirillo E,
Ferrari S and Sanna M: Guidelines for treating temporal bone
carcinoma based on long-term outcomes. Otol Neurotol. 34:898–907.
2013.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Fleiner F, Jumah M and Göktas O: Cancer of
the external auditory canal-diagnostic and treatment. Indian J
Otolaryngol Head Neck Surg. 61:270–274. 2009.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Pemberton LS, Swindell R and Sykes AJ:
Primary radical radiotherapy for squamous cell carcinoma of the
middle Ear and external auditory Cana-an historical series. Clin
Oncol (R Coll Radiol). 18:390–394. 2006.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Murai T, Kamata SE, Sato K, Miura K, Inoue
M, Yokota N, Ohta S, Iwabuchi M, Iwata H and Shibamoto Y:
Hypofractionated stereotactic radiotherapy for auditory canal or
middle ear cancer. Cancer Control. 23:311–316. 2016.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Shinomiya H, Hasegawa S, Yamashita D,
Ejima Y, Kenji Y, Otsuki N, Kiyota N, Sakakibara S, Nomura T,
Hashikawa K, et al: Concomitant chemoradiotherapy for advanced
squamous cell carcinoma of the temporal bone. Head Neck. 38 (Suppl
1):E949–E953. 2016.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Austin JR, Stewart KL and Fawzi N:
Squamous cell carcinoma of the external auditory canal. Therapeutic
prognosis based on a proposed staging system. Arch Otolaryngol Head
Neck Surg. 120:1228–1232. 1994.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Hahn SS, Kim JA, Goodchild N and Constable
WC: Carcinoma of the middle ear and external auditory canal. Int J
Radiat Oncol Biol Phys. 9:1003–1007. 1983.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Nakagawa T, Kumamoto Y, Natori Y,
Shiratsuchi H, Toh S, Kakazu Y, Shibata S, Nakashima T and Komune
S: Squamous cell carcinoma of the external auditory canal and
middle Ear: An operation combined with preoperative
chemoradiotherapy and a free surgical margin. Otol Neurotol.
27:242–249. 2006.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Choi J, Kim SH, Koh YW, Choi EC, Lee CG
and Keum KC: Tumor stage-related role of radiotherapy in patients
with an external auditory canal and middle Ear carcinoma. Cancer
Res Treat. 49:178–184. 2017.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Yoon M, Chougule P, Dufresne R and Wanebo
HJ: Localized carcinoma of the external ear is an unrecognized
aggressive disease with a high propensity for local regional
recurrence. Am J Surg. 164:574–577. 1992.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Hayashi K, Koto M, Demizu Y, Saitoh JI,
Suefuji H, Okimoto T, Ohno T, Shioyama Y, Takagi R, Ikawa H, et al:
A retrospective multicenter study of carbon-ion radiotherapy for
external auditory canal and middle Ear carcinomas. Cancer Med.
8:51–57. 2019.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Nagano T, Yoshimura RI, Kojima M, Nakagawa
K and Toda K: Outcomes of radiotherapy in advanced external
auditory canal cancer. J Radiat Res. 60:380–386. 2019.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Sugimoto H, Ito M, Yoshida S, Hatano M and
Yoshizaki T: Concurrent superselective intra-arterial chemotherapy
and radiotherapy for late-stage squamous cell carcinoma of the
temporal bone. Ann Otol Rhinol Laryngol. 120:372–376.
2011.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Fujiwara M, Yamamoto S, Doi H, Takada Y,
Odawara S, Niwa Y, Ishikura R, Kamikonya N, Terada T, Uwa N, et al:
Arterial chemoradiotherapy for carcinomas of the external auditory
canal and middle ear. Laryngoscope. 125:685–689. 2015.PubMed/NCBI View Article : Google Scholar
|