Introduction
Chordomas are rare and aggressive tumors that are
derived from notochordal remnants and represent 1-4% of all bone
tumors. The reported incidence of chordomas ranges from 0.3-0.4 to
as high as 0.84 cases per million individuals per year worldwide
(1), whereas the National Cancer
Database of the United States reported a total of 936 cases of
cranial chordoma between 2004 and 2014(2). The sacrococcygeal region, skull base
and spine account for 50-65, 25-30 and 15-20% of chordoma
localizations, respectively (3-5).
The median age at diagnosis is 47-50 years and the tumor exhibits a
preponderance for males (54.8-56.2%) (2,6).
Virchow was the first to describe the presence of
small nodules along the clivus in 1846, and Luschka in 1856 also
described small jelly-like protrusions from the clivus (7). Virchow named these cartilaginous
nodules ‘ecchordosis physaliphora’ in 1857, as he suggested these
vacuolated mucus containing tumors were of cartilaginous origin
(7). Muller established the
notochordal origin of these nodules in 1895, and Ribbert was the
first to apply the term ‘chordoma’ in 1894 (8,9).
Klebs reported the first case of chordoma of the
clivus in 1864, in which the patient died from tumor-induced
tetanic convulsions (10), and
Burrow described the case of a 30-year-old male French soldier who
presented with a slow growing chordoma of the skull base in 1923;
the soldier experienced headaches, blindness of the left eye, left
3rd, 4 and 6th cranial nerve palsy and lower leg weakness for 3
years, and eventually died from respiratory failure. Postmortem
examination revealed a 6.5x5.5x3.5 cm skull base tumor with
invasion to the ethmoid and sphenoid sinus (10). The tumor was composed of alveolar
cells with and abundance of cytoplasmic vacuolation due to mucin
(physaliphorous cell). Seltzer (11) reported the case of a 24-year-old
female patient in 1961 who experienced difficulty swallowing, neck
and throat pain, and nasal speech for 6 months. Examination
revealed a 4-cm tumor in the left nasopharynx, tumor excision was
performed, and pathological analysis described the tumor as
containing mucus, consistent with a diagnosis of chordoma.
Chordomas usually originate from the notochordal
remnants in bones, whereas extraosseous chordomas are tumors
derived from soft tissue harboring notochordal remnants. Chordoma
of the nasopharynx is very rare and may exhibit similarities with
other lesions of the nasopharynx (12). Chordomas are amenable to complete
surgical removal if there is no involvement of major neurovascular
structures (11,12). The silent onset of these tumors and
lack of specific initial symptoms may prevent early diagnosis and,
although these tumors may appear benign, local invasion and
metastatic spread indicate that they behave more like malignant
tumors (13).
Jallo et al (14) proposed a classification of chordoma
based on the presence or absence of osseous origin: Type I, osseous
extradural; type II, extraosseous extradural; type III, osseous
intradural; and type IV, extraosseous intradural. In the present
publication, the case of a type II extraosseous chordoma of the
nasopharynx in an elderly female patient is presented, and a review
of the current literature on chordomas is discussed.
Case report
A 63-year-old female patient was admitted to Tungs'
Taichung Metroharbor Hospital on May 24, 2019. The patient
experienced insidious onset of left temporal headaches and
dizziness 6 months prior to admission, and subsequently complained
of left nasal obstruction, left maxillary area numbness, left ear
hearing loss and swallowing difficulty for 2 months prior to
admission. Nasopharyngoscopy performed on 24/05/2019 revealed a
left nasopharyngeal mass occupying the left Rosenmüller fossa with
extension to the oropharynx. A computed tomography (CT) scan on
31/05/2019 revealed a 6-cm left lateral nasopharyngeal
heterogeneously enhanced lobulated mass in contact with the deep
lobe of the left parotid gland. A biopsy and microscopic
examination revealed pleomorphic adenoma, with myoepithelial cells
with scant ductal epithelium in abundant chondromyxoid substance.
The tumor stained positive for cytokeratin (CK)AE1/AE3 and S100,
and negative for CD38, p53 and mucicarmine.
The patient developed a recurring left-sided
headache, pain in the left maxillary area, left nasal obstruction
and left ear deafness for 2-3 weeks; the patient was then seen on
05/09/2019 by a physician, and physical examination revealed a firm
3x3-cm indurated left aural mass and a 2x2-cm firm left
submandibular mass with slight tenderness on palpation.
Nasopharyngoscopy revealed a large nasopharyngeal mass completely
obstructing the choanae. A subsequent CT scan on 06/09/2019
revealed an 8.2x3.2x5.7-cm space-occupying lesion with central
necrosis of the nasopharynx and oropharynx, partially occluding the
pharyngeal lumen, and the mass infiltrated the left parapharyngeal
space, the left medial and lateral pterygoid muscle and left
parotid gland, along with bone erosion of the left mandible. A
whole-body positron emission tomography CT scan on 14/09/2019
revealed a heterogenous 18F-fluorodeoxyglucose
(FDG)-avid soft tissue lesion over the left ear, nasopharynx,
oropharynx, left petrous bone and left mandibular bone. The
oropharyngeal tumor exhibited a maximal FDG initial and delayed
standardized uptake value of 6.4 and 6.3, respectively. There was
no evidence of bone, lung or liver metastases.
A transoral robotic intralesional surgery was
performed on 24/09/2019 for tumor resection. The resected chordoma
tissues were fixed in 10% buffered formalin for 1 h at 35˚C,
processed and embedded in paraffin with Surgipath®
Paraplast Regular (Leica Microsystems GmbH) through a Sakura
Tissue-Tek VIP automated tissue processor system (Sakura Finetek
USA, Inc.). All tissue blocks were then cut into 3-µm sections
using a semiautomatic rotary microtome (Leica RM2245; Leica
Microsystems GmbH). The histopathological sections were stained
with hematoxylin solution Gill 2 (Leica Microsystems GmbH) and
eosin Y solution (alcoholic) (EYA999; ScyTek laboratories, Inc.)
using a Sakura Tissue-Tek DRS 2000 automated stainer (Sakura
Finetek USA, Inc.). Immunohistochemical staining was performed
using Novocastra antibodies against CK, epithelial membrane antigen
(EMA), p63, S100, Ki67 and smooth muscle actin (SMA) (product codes
PA0094, PA0035, PA0103, PA0031, PA0118 and PA0943, respectively;
catalog 190642 Rev B, Leica Microsystems GmbH) was performed with a
Leica Bond III automated stainer (Leica Microsystems GmbH).
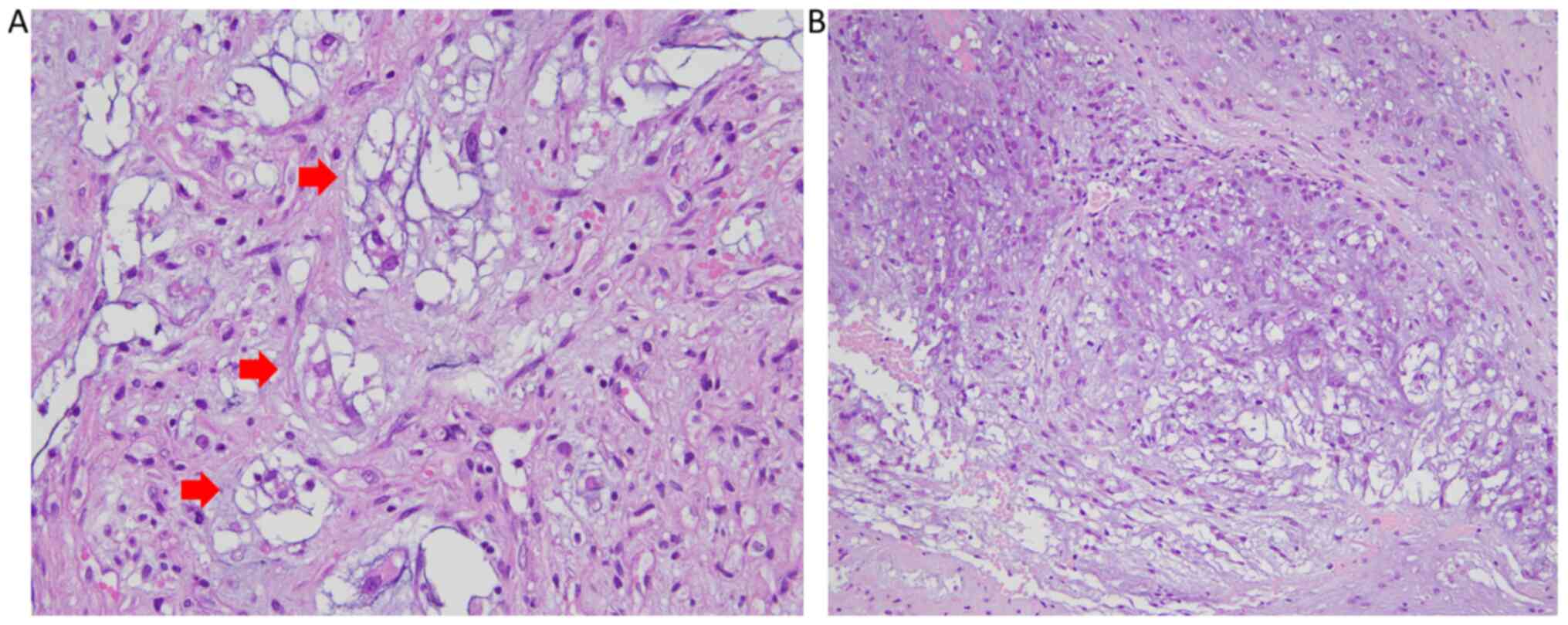
Hematoxylin and eosin (H&E) staining of the
histopathological specimen revealed a lobular architecture with
fibrous bands separating lobules with a discernible infiltrative
border; the cytoarchitecture within the lobules consisted of cells
forming short chords and dense epithelioid sheets of single cells
within the myxoid matrix. The cells exhibited an abundance of clear
to eosinophilic cytoplasm, with a bubbly, vacuolated appearance
(physaliphorous cells), and occasional mitotic figures were
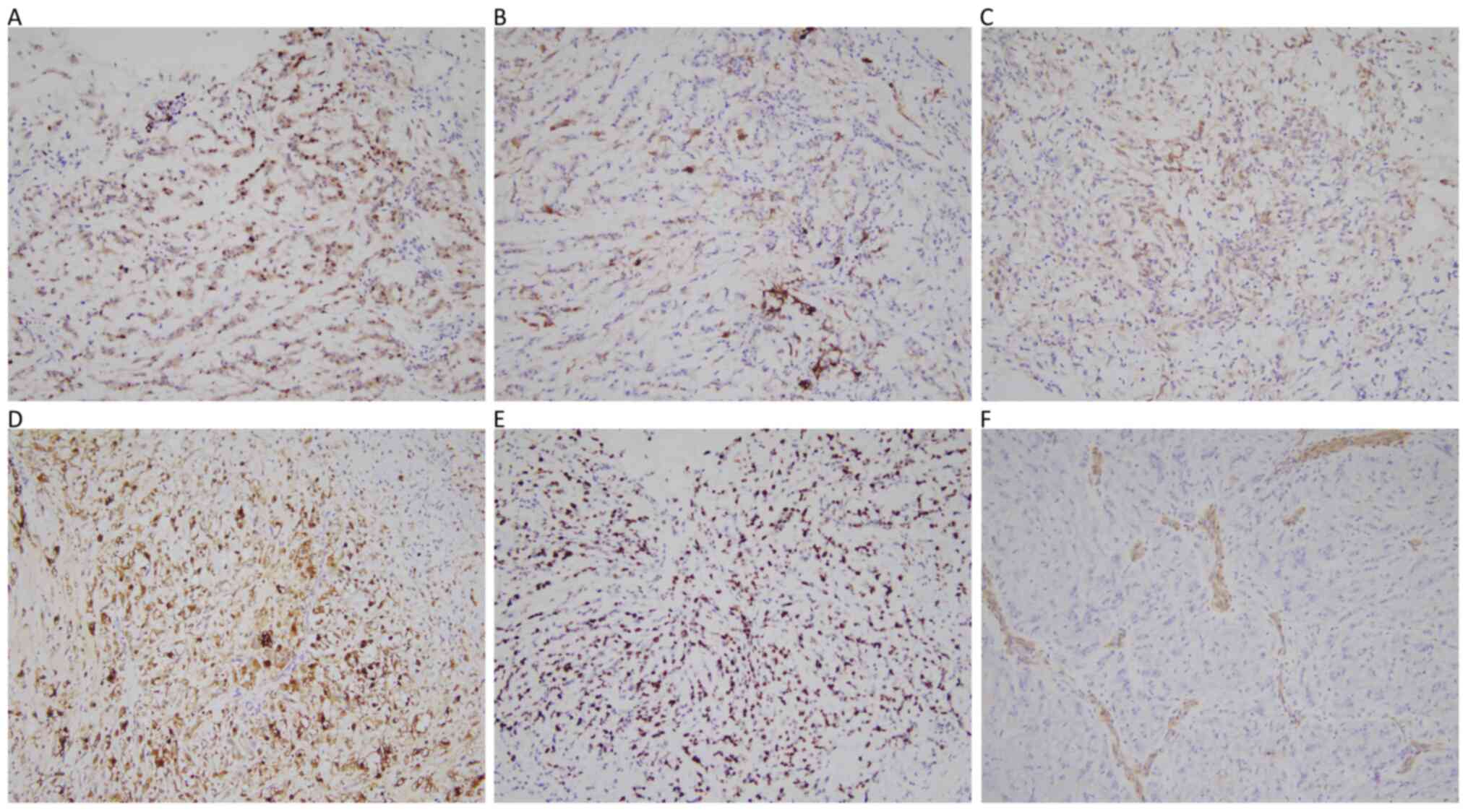
observed (Fig. 1). On
immunohistochemical staining (Fig.
2), the tumor tissues were positive for CK, EMA, p63, S100 and
Ki67 (30%), whereas SMA staining was negative. Brachyury stain was
not available in our hospital. Additionally, bone, fat, muscle and
vascular invasion in the tissue cross sections were also observed.
The histopathological findings were consistent with a diagnosis of
chordoma, conventional type (9).
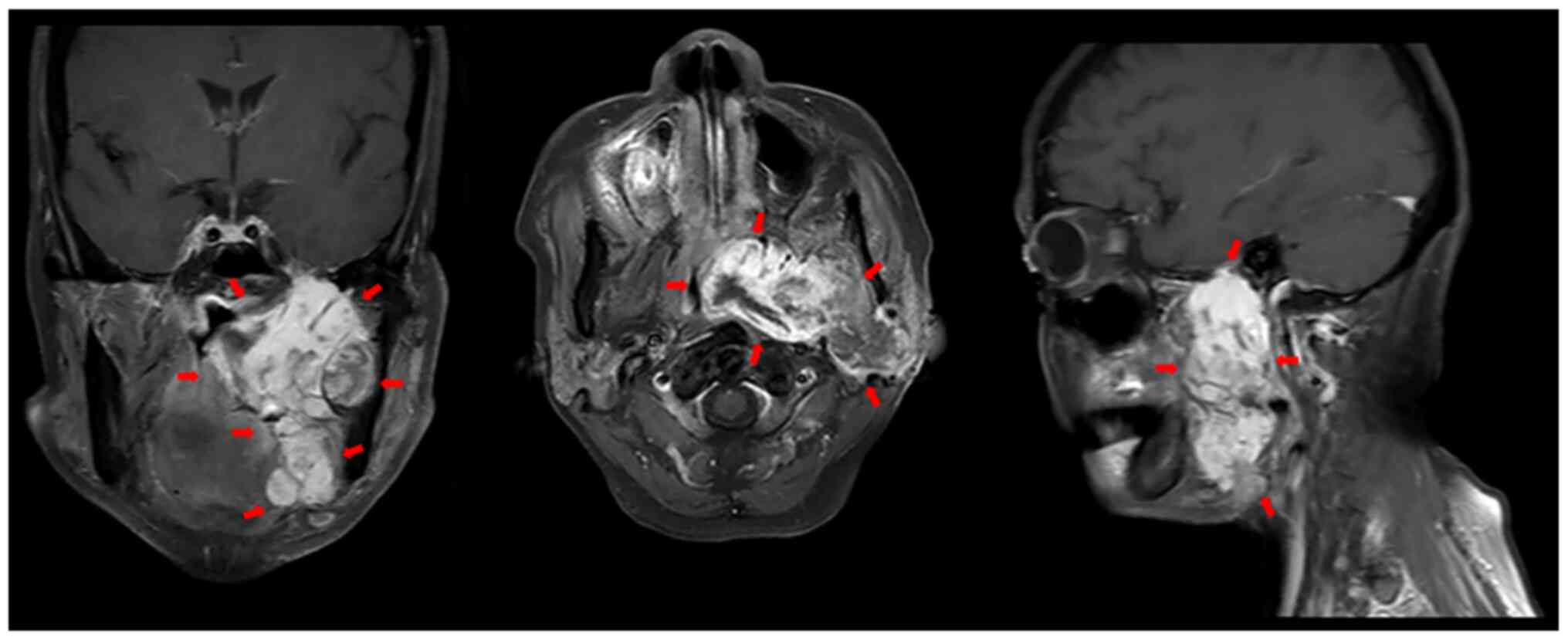
Magnetic resonance imaging (MRI) on 22/10/2019
identified a recurrent huge left parapharyngeal mass lesion
(~8.6x4.0x6.1 cm) extending from the nasopharynx to the oropharynx,
with intracranial extension to the left middle cranial fossa, left
foramen ovale, left jugular foramen, left hypoglossal canal, left
parotid gland and encasement of the left internal carotid artery
and jugular vein (Fig. 3).
Under the clinical suspicion of nasopharyngeal
chordoma pG2T2N0M0 stage IIB (15),
the patient was treated with definitive radiotherapy with a
cumulative dose of 70 Gy in 35 fractions between 04/10/2019 and
22/11/2019. The radiation dose to the brainstem, parotid glands,
submandibular glands, optic nerves, optic chiasm, spinal cord,
lens, cochlea and auditory nerves were within normal tissue
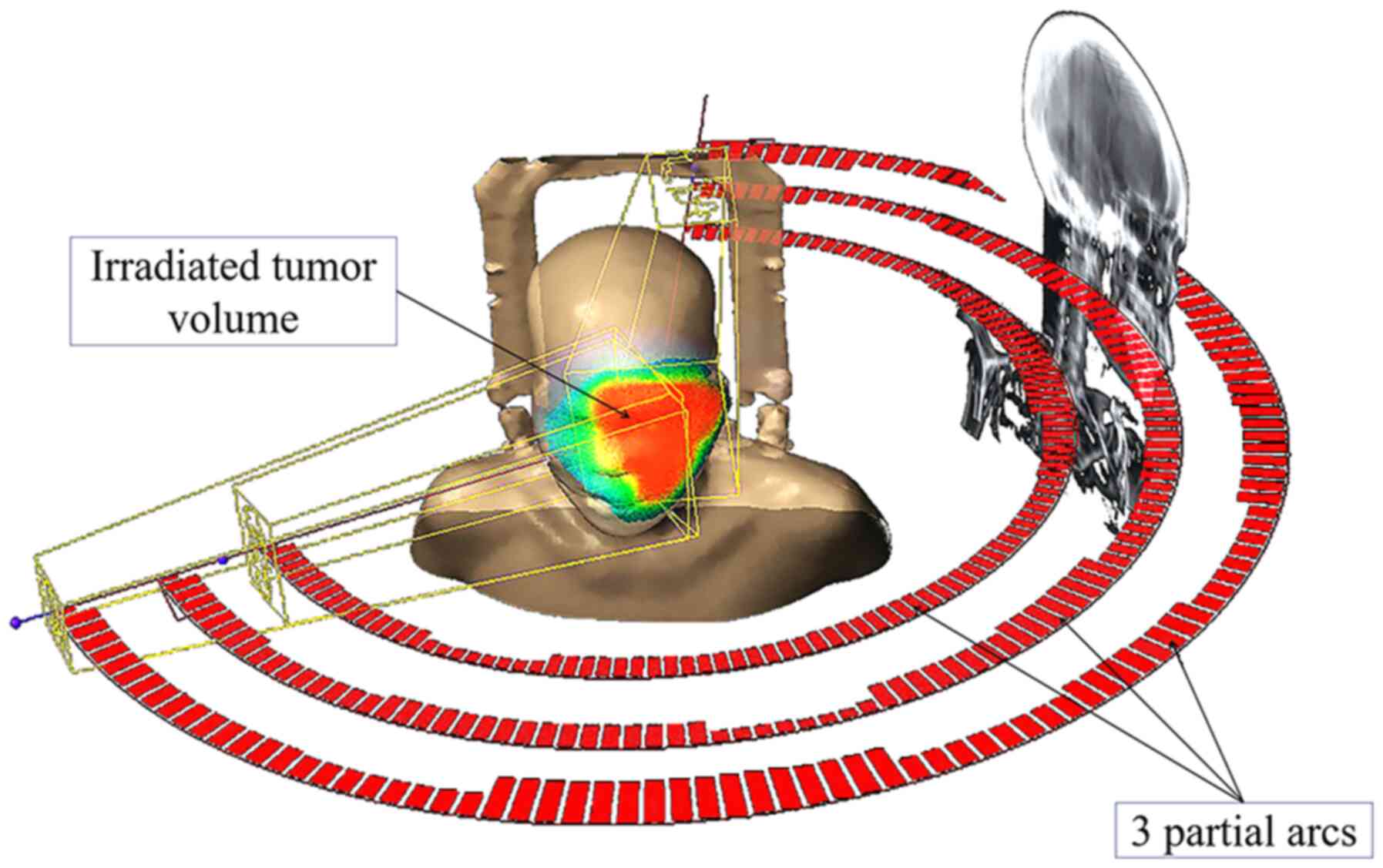
tolerance doses (16). The patient
was treated using the image-Guided Radiotherapy (RapidArc)
technique (Varian Medical Systems, Inc.); this is a type of
volumetric modulated arc therapy (VMAT) in which a triple 6-MV
photon beam partial arc was delivered through a continuously arced
motion of the Varian TrueBeam linear accelerator (Fig. 4). The treated tumor volume was
estimated to be 213.7 cm3 using the tumor contouring
function of the Varian Eclipse radiotherapy treatment planning
system, version 13.0 (Varian Medical Systems, Inc.). The patient's
headache and nasal obstruction were partially relieved, but the
treatment course was complicated by a left otitis media with
purulent discharge; this condition was managed with antibiotics. An
MRI scan on 06/01/2020 revealed large areas of necrosis of the
nasopharyngeal mass and slight tumor shrinkage. Further
radiotherapy with 40 Gy using the VMAT technique was used to treat
the residual tumor (84 cm3) between 11/02/2020 and
22/02/2020. The patient was regularly followed up in the outpatient
setting up to 16/04/2020, when the patient developed a
non-productive cough. A chest X-ray revealed multiple left lower
and right whole-lung metastases. As the patient developed
progressive shortness of breath and moderate dry cough, a chest
X-ray was performed on 02/05/2020 and revealed multiple bilateral
lung metastases, right-sided pneumonia and mild right pleural
effusion. The patient suffered a sudden cardiac arrest and was
subjected to endotracheal intubation and cardiopulmonary
resuscitation; however, she succumbed to the disease on
03/5/2020.
Discussion
Chordomas of the nasopharyngeal area represent a
major challenge in terms of effective treatment due to the relative
inaccessibility of the region, tumor involvement of critical
neurovascular structures and invasive growth to the skull base,
predisposing the tumor to local recurrence and early metastasis
(12).
Chordomas are classified into three different
subtypes: Conventional or classical type (accounting for the
majority of the cases); chondroid type; and dedifferentiated type
(9,17). The different types of chordoma and
their characteristics are summarized in Table I. The patient in the present case
report had a conventional-type chordoma; the tumor was composed of
lobules of cells arranged in cords and nests, and it is common for
one tumor cells to wrap around its neighbor as if one cell is
‘hugging’ the other (9). The
histological hallmarks of chordoma are the large physaliphorous
cells (Greek: Physalis: Bubbles, phoros: Bearing)
observed on H&E staining; these cells are characterized by the
large, intracytoplasmic vacuoles embedded in a homogeneous,
intercellular substance, and are arranged like beads on a string,
unlike chondrosarcomas, in which the individual cells are embedded
in cartilage (9). A distinguishing
feature of the tumor is that it stains strongly positive for
brachyury, CK, S100 and EMA, as was observed in the present case
(17,18). Studies have suggested that
brachyury, a transcription factor encoded by the T (brachyury) gene
for notochord development, is implicated in the initiation and
progression of chordoma (9,19).
 | Table ITypes of chordomas. |
Table I
Types of chordomas.
| Type | Histological
appearance | Gross appearance | Site of
involvement |
|---|
| Conventional or
classical | Lobules of cells
arranged in cords and nest a solid, hyalinized matrix | Soft, mucoid | Sacrum, skull
base |
| Chondroid | Lacunar spaces filled
with neoplastic cells surrounded by | Chondroid regions
merged with classical component | Skull base, mobile
spine |
| Dedifferentiated | Tightly packed,
small, atypical epithelioid cells arranged in nests and sheets in a
fibrous background and lack of physaliphorous cells | Dedifferentiated
components are usually distinct from the areas of conventional
chordoma | Sacrococcygeal area;
aggressive tumor with systemic spread in 90% of cases |
Extraosseous chordoma of the nasopharynx is a rare
malignancy that originates from the remnants of the notochord, a
primitive tissue of embryonic origin around which the skull base
and axial skeleton develop (12,20-22).
Extraosseous chordomas commonly affect individuals aged 50-60 years
(23,24). The nasopharynx is, in itself, an
unusual site for chordoma, accounting for only 0.2% of all
nasopharyngeal neoplasms (25), and
nasopharyngeal chordoma has been hypothesized to originate from the
medial basal canal of the clivus, which is the notochord's cephalad
exit tract from its ventral clivus location in the nasopharyngeal
soft tissues (12,21). To the best of our knowledge, there
have only been 20 reported cases of this type of tumor in the
medical literature (26). Late
diagnosis is due to the non-specific and insidious onset of signs
and symptoms and the slow growth rate of the tumor (13,25),
which is typically only detected when it has grown to a size large
enough to cause a notable effect to the surrounding tissues. In the
present case report, the patient presented with cranial
neuropathies, pain and difficulty swallowing. Local recurrence with
an incidence of 50-68% is common due to the aggressive nature of
this tumor (12,20,22,27),
and systemic metastasis to the lungs, bones, liver and lymph nodes
are found in 17.8-43% of patients with chordoma (4,27).
In a retrospective study of 219 patients with
chordoma, Young et al (27)
found that the lung accounts for 53.8% of all metastatic sites
aside from the bone, soft tissue, sternum and liver. Their study
reported that cervical spine chordoma had the shortest time
interval from onset to metastasis (16 months) compared with the
lumbar spine (49.2 months) and sacrum (58.3 months). Young female
patients were more likely to present with an aggressive chordoma of
the cervical spine in the study by Young et al (27). The overall median survival was 130.4
and 159.3 months for the metastatic and non-metastatic groups,
respectively. In the present case report, the patient's tumor also
exhibited aggressive clinical behavior, with early lung metastasis
(after 8 months) and a short survival period (9 months) after
diagnosis. A study of 28 patients with skull base chordoma reported
a median survival and 5-year survival rate of 4 months and 48.9%,
respectively, with radiotherapy alone (2).
Adverse prognostic factors include subtotal
resection, dedifferentiated histological subtype, age >40 years,
a history of prior treatment, tumor size ≥4 cm, gross tumor volume
>25 cm3, pharyngeal involvement, optic nerve and
brainstem compression, none or low-dose radiation therapy and
female sex (1). In the present case
report, the patient's gross tumor volume was 213.7 cm3,
she was female and aged 63 years, and the tumor extended to the
oropharynx, which collectively predicted a poorer prognosis.
Adequate wide surgery to obtain a safe margin
without penetration of the capsule is the cornerstone of successful
chordoma treatment; however, this is almost impossible due to the
anatomical origin and involvement of nasopharyngeal and skull base
neurovascular structures. Additionally, these tumors contain
gelatinous material that can spill into the resection cavity,
markedly increasing the risk of recurrence. The complete resection
rate is only 29-50% in some studies, and subtotal resection with
residual tumor is used in order to minimize surgery-related
neurological deficits (19,24).
A standalone endonasal approach for chordomas of the
skull base is considered as a viable alternative to open resection
owning to its advantages of direct tumor exposure, minimal
invasiveness and favorable cosmetic appearance. Zhang et al
(28) treated 32 patients with
chordomas of the skull base between July 2006 and June 2015. The
surgical approach was an extended endoscopic endonasal surgery.
Gross total resection, subtotal resection (>10% and <90%
tumor mass reduction) and partial resection (>90% tumor mass
reduction) was achieved in 9 (28.1%), 16 (50.0%) and 12 (21.9%)
patients, respectively. The postoperative radiotherapy dose was
54-70 Gy (mean, 62.7 Gy). Their results revealed a 3- and 5-year
progression-free survival (PFS) of 44.0 and 16.5%, respectively.
The 3- and 5-year overall survival (OS) rate was 79.4 and 69.5%,
respectively. The PFS between the surgery and radiation group and
the surgery alone group exhibited no significant differences;
however, there was a significant increase in OS for the surgery
plus radiation group compared with the surgery alone group. It was
concluded that gross total resection is associated with improved
PFS and OS, and postoperative adjuvant radiation therapy is
recommended to improve OS for chordomas of the skull base.
Postoperative radiotherapy with photon or proton
beam currently serves an important role in chordoma management and
has been reported to show a positive outcome (2,4,13,19).
Radiotherapy for head and neck cancer, such as in the present case
report, is a challenging task due to the complex anatomy of the
head and neck region, with these tumors being located in close
proximity to radiation dose-limiting critical structures. These
tumors behave aggressively and grow rapidly due to the rich
lymphatic supply in the head and neck region, and almost always
manifest at a locally advanced stage (29).
Foweraker et al (6) treated 9 adult cases of chordoma and 3
cases of chondrosarcoma of the skull base with preoperative
radiotherapy of 50-60 Gy, and a postoperative boost radiotherapy of
5 Gy, with a cumulative dose of 65 Gy delivered in 39 fractions.
Local control was achieved in 11 of the 12 cases, and the 3- and
5-year cause-specific survival for the 12 patients was 88 and 75%,
respectively; 1 patient developed local recurrence 23 months after
radiotherapy, while another patient developed lymph node metastasis
7 months after radiotherapy and succumbed to distant metastasis 20
months later. In the present case report, the patient also
exhibited a similar clinical course and succumbed to the disease 7
months after radiotherapy. Thus, high-dose radiotherapy may be a
viable palliative treatment option for this disease.
Image-guided intensity-modulated radiotherapy
(IG-IMRT) was used to treat 24 chordomas and 18 chondrosarcomas of
the skull base postoperatively, as reported by Sahgal et al
(30), with a median dose of 76 and
70 Gy for chordoma and chondrosarcoma, respectively. The 5-year OS
and local control rate for skull base chordoma and chondrosarcoma
were 85.6, 65.3, 87.8 and 88.1%, respectively. A total of 6
patients (14.3%) developed radiation-induced late toxicity after a
mean follow-up period of 3.2 years, including hearing loss,
hypothyroidism, hypopituitarism, vestibular nerve injury and
cranial nerve IV injury; these patients were treated for skull base
chordoma with 78 Gy in 39 fractions. Thus, careful treatment
planning can achieve acceptable local control with tolerable
radiation-induced toxicity.
Gatfield et al (31) treated 28 patients with chordoma of
the skull base and spine with postoperative radiotherapy; these
patients were treated with IG-IMRT with a median dose of 65 Gy
(range, 65-70 Gy) and were able to achieve a 5-year local control
rate and cause-specific survival rate of 74 and 85%, respectively.
It was concluded that postoperative high-dose radiotherapy may
result in long-term control of the disease.
Salazar Guilarte et al (22) reported the case of a 7-year-old girl
with a 4x3x5-cm nasopharyngeal chordoma, who first underwent
transoral endoscopic resection. Subsequently, stereotactic ablative
radiotherapy was used to treat the 2-cm residual tumor with good
results; dynamic IMRT was used to deliver 42 Gy in 4 fractions. The
patient has remained disease-free 20 months after radiotherapy.
High-dose radiotherapy using modern techniques, such
as the RapidArc VMAT for nasopharyngeal chordoma deliver promising
results. This advanced technique has been used extensively to treat
nasopharyngeal carcinoma, achieving a 3-year locoregional control
rate and 3-year OS rate of 92.2 and 97.0%, respectively (31). RapidArc is an advanced technique in
which radiotherapy treatment is delivered using a continuous arc
motion of the linear accelerator gantry, accompanied with
simultaneous variation of the multileaf collimator position, gantry
rotation speed and dose rate output; this technique delivers a
highly conformal radiation dose to the tumor, whilst limiting the
dose to the organs at risk surrounding the tumor (29).
Prognostic factors for local control in primary
chordomas include tumor size, extent of resection, quality of
surgery, patient age, technique and quality of radiotherapy
(32).
A dose of at least 74 Gy is recommended using
conventional fractionation for photon and proton therapy (PT).
Target volumes should be delineated considering the primary tumor
location and its recurrence sites. The high-dose volume should
include any macroscopic disease as well as surgical margins,
whereas the low-dose volume should encompass areas at risk of
microscopic spread, skip metastases, or seeding due to previous
surgical procedures (32).
Particle beam with PT or carbon ion therapy (CIT)
have also been reported to obtain excellent results in terms of
local control and survival; the reduced lateral scatter due to the
Bragg peak offers a more conformal dose distribution when compared
with photon beam radiotherapy; this will enable a higher
tumoricidal radiation dose to chordomas of the skull base, without
incurring any severe late neurovascular toxicities (33). Takagi et al (33) treated 24 patients with skull base
chordoma with PT and CIT between April 2003 and May 2014. The
radiation dose constraints of the optic nerve, chiasma, cochlea,
spinal cord and brainstem were limited to ≤47 Gy. The study
reported a 5-year local control, PFS and OS rates of 85, 81 and
86%, respectively, during a median follow-up of 71.5 months (range,
14-175 months) for all patients. Patients who received
postoperative particle therapy achieved a statistically significant
improvement in local control, PFS and OS. Of note, 2 patients
developed brain necrosis associated with moderate cognitive and
memory dysfunction, and 1 patient developed bleeding from the
nasopharynx that was treated with coil embolization (33). Thus, particle beam therapy was
deemed to be an effective and safe treatment for chordomas of the
skull base in the postoperative setting to improve local
control.
Systemic therapy is an option for unresectable,
locally recurrent or metastatic chordomas. Meng et al
(34) reviewed a variety of
molecular target inhibitors (MTIs), such as imantinib, erlotinib,
cetuximab, sorafenib, pazopanib, sunitinib, sirolimus, thalidomide,
bevacizumab, gefitinib, linsitinib and everolimus, which were
included in 32 clinical trials.
Imatinib is a tyrosine kinase inhibitor targeting
platelet-derived growth factor b, and it is the most extensively
studied MTI for the treatment of chordomas. Overexpression and
activation of platelet-derived growth factor receptor b is
hypothesized to play a role in the growth of chordomas. Across four
studies, with a total of 181 chordoma patients treated with
imatinib, partial response was achieved in 4 patients (2.2%),
whereas stable disease was reported in 133 patients (73.5%) and
progressive disease in 44 cases (24.3%). Meng et al
(34) concluded that MTI
monotherapy may be recommended as first-line treatment. Combination
therapy with two MTIs may be administered for drug-resistant
chordoma.
In conclusion, extraosseous nasopharyngeal chordoma
is a rare type of tumor that is amenable to surgery and
postoperative radiotherapy. RapidArc VMAT is a technique that
achieves excellent local control of these tumors with a greater
sparing effect of normal tissues. However, additional studies are
required to further elucidate the clinical behavior and determine
the optimal treatment strategy for nasopharyngeal chordoma.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
CHY collected all the pertinent data of the patient,
wrote and edited the final manuscript.
Ethics approval and consent to
participate
The study was approved by the institutional review
board of the Tungs' Taichung Metroharbor Hospital (IRB no.
109033).
Patient consent for publication
The present study was granted an exemption from
requiring patient's informed consent for publication by the
institutional review board of the Tungs' Taichung Metroharbor
Hospital (IRB no. 109033).
Competing interests
The author declares no competing interests.
References
|
1
|
Bakker SH, Jacobs WCH, Pondaag W,
Gelderblom H, Nout RA, Dijkstra PDS, Peul WC and Vleggeert-Lanamo
CLA: Chordoma: A systematic review of the epidemiology and clinical
prognostic factors predicting progression-free and overall
survival. Eur Spine J. 27:3043–3058. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Hulou MM, Garcia CR, Slone SA, Dugan A,
Lei F, Huang B, Pittman T and Villano JL: Comprehensive review of
cranial chordomas using national databases in the USA. Clin Oncol
(R Coll Radiol). 31:e149–e159. 2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Cha YJ and Suh YL: Chordomas:
Histopathological study in view of anatomical location. J Korean
Med Sci. 34(e107)2019.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Kataria SP, Batra A, Singh G, Kumar S and
Sen R: Chordoma of skull base presenting as nasopharyngeal mass. J
Neurosci Rural Pract. 4 (Suppl 1):S95–S97. 2013.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Vaz-Guimaraes F and Harsh IV GR: Chapter
5: Demographics, presentation, and diagnosis: Chordomas and
chondrosarcomas of the skull base and spine. 2nd edition. Harsh IV
GR and Vas-Guimaraes F (eds). Academic press, London, pp45-51,
2018.
|
|
6
|
Foweraker KL, Burton KE, Maynard SE, Jena
R, Jefferies SJ, Laing RJC and Burnet NG: High-dose radiotherapy in
the management of chordoma and chondrosarcoma of the skull base and
cervical spine: Part 1-clinical outcomes. Clin Oncol (R Coll
Radiol). 19:509–516. 2007.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Goodwin CR, Liang LJ, Zadnik PL and
Sciubba DM: Chapter 155: Chordomas and chondrosarcomas. In: Youmans
and Winn neurological surgery. Richard WH (ed). Vol 4. 7th edition.
Elsevier, Philadelphia, PA, pp1243-1250, 2017.
|
|
8
|
Windeyer BW: Chordoma. Proc R Soc Med.
52:1088–1100. 1959.PubMed/NCBI
|
|
9
|
Kerr DA and Rosenberg AE: Chapter 2:
Pathology of chordoma and chondrosarcoma of the axial skeleton. In:
Chordomas and chondrosarcomas of the skull base and spine. Harsh IV
GR and Vas-Guimaraes F (eds). 2nd edition. Academic press, London,
pp11-21, 2018.
|
|
10
|
Burrow Jle F and Stewart MJ: Original
papers: Malignant spheno-occipital chordoma. J Neurol Psychopathol.
4:205–217. 1923.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Seltzer AP: Nasopharyngeal chordoma. A
case report. J Natl Med Assoc. 53:41–42. 1961.PubMed/NCBI
|
|
12
|
Nguyen RP, Salzman KL, Stambuk HE, Ahuja
AT and Harnsberger HR: Extraosseous chordoma of the nasopharynx.
AJNR Am J Neuroradiol. 30:803–807. 2009.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Vasudevan V, Manjunath V, Devaraju D and
Murali R: Chordoma arising from cranial base extending to
oropharynx: An unusual presentation. J Maxillofac Oral Surg. 14
(Suppl 1):S103–S107. 2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Jallo J, Nathan D, Bierbrauer K and Farber
E: Chordoma: A case report. Surg Neurol. 48:46–48. 1997.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Kneisl JS, Rosenberg AE, Anderson PM,
Antonescu CR, Bruland OS, Cooper K, Horvai AE, Holt GE, O'Sul|ivan
B, Patel SR, et al: Chapter 38: Bone. In: AJCC cancer staging
manual. Amin MB, Edge S, Greene F, Byrd DR, Brookland RK,
Washington MK, Gershenwald JE, Compton CC, Hess KR, Sullivan DC,
et al (eds). 8th edition. Springer International Publishing,
New York, NY, pp471-486, 2017.
|
|
16
|
Guo R, Tang LL, Mao YP, Zhou GQ, Qi ZY,
Liu LZ, Lin AH, Liu MZ, Ma J and Sun Y: Clinical outcomes of
volume-modulated arc therapy in 205 Patients with nasopharyngeal
carcinoma: An analysis of survival and treatment toxicities. PLoS
One. 10(e0129679)2015.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Wasserman JK, Gravel D and Purgina B:
Chordoma of the head and neck: A review. Head Neck Pathol.
12:261–268. 2018.PubMed/NCBI View Article : Google Scholar
|
|
18
|
McKeever PE and Venneti S: Chapter 20:
Immunohistology of the nervous system. In: Diagnostic
immunohistochemistry, theranostic and genomic applications. Dabbs
DJ (ed). 5th edition. Elsevier, Inc., Philadelphia PA, pp824-826,
2019.
|
|
19
|
Mohyeldin A, Vaz-Guimaraes F, Carrau RL
and Prevedello DM: Chapter 3: Molecular drivers in chordoma. In:
Chordomas and chondrosarcomas of the skull base and spine. Harsh IV
GR and Vas-Guimaraes F (eds). 2nd edition. Academic press, London,
pp23-29, 2018.
|
|
20
|
Mitra B, Sengupta S, Rai A, Mehta J,
Quader AR, Roy S and Borges A: Chordoma in nasopharynx in a
70-year-old female: A rare occurrence. Int J Otolaryngol Head Neck
Surg. 3:342–346. 2014.
|
|
21
|
Sajisevi M, Hoang JK, Eapen R and Jang DW:
Nasopharyngeal masses arising from embryologic remnants of the
clivus: A case series. J Neurol Surg Rep. 76:e253–e257.
2015.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Salazar Guilarte JX, Sancho Mestre M and
Gras Albert JR: Extraosseous chordoma of nasopharynx in pediatric
age. Acta Otorrinolaringol Esp. 63:321–323. 2012.PubMed/NCBI View Article : Google Scholar : (In Spanish).
|
|
23
|
Orecchia R, Leonardi MC, Krengli M,
Zurrida S and Brambilla MG: External radiotherapy plus
intracavitary brachytherapy for recurrent chordoma of the
nasopharynx. Acta Oncol. 37:301–304. 1998.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Walcott BP, Nahed BV, Mohyeldin A, Coumans
JV, Kahle KT and Ferreira MJ: Chordoma: Current concepts,
management, and future directions. Lancet Oncol. 13:e69–e76.
2012.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Radzikowska J, Gronkiewicz Z, Kukwa A,
Lisik W, Czarnecka AM, Krzeski A and Kukwa W: Nasopharyngeal
chordoma in a patient with a severe form of sleep-disordered
breathing: A case report. Oncol Lett. 10:1805–1809. 2015.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Dwianingsih EK, Snak Y, Rinonce HT, Wasita
B, Antoro EL and Amr SS: Primary chordoma of the nasopharynx: A
rare case report and review of the literatures. Case Rep Pathol.
2019(3826521)2019.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Young VA, Curtis KM, Temple HT, Eismont
FJ, DeLaney TF and Hornicek FJ: Characteristics and patterns of
metastatic disease from chordoma. Sarcoma.
2015(517657)2015.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Zhang HK, Sun XC, Hu L, Wang JJ and Wang
DH: Endonasal endoscopic resection and radiotherapy in skull base
chordomas. J Craniofac Surg. 27:e709–e713. 2016.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Teoh M, Clark CH, Wood K, Whitaker S and
Nisbet A: Volumetric modulated arc therapy: A review of current
literature and clinical use in practice. Br J Radiol. 84:967–996.
2011.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Sahgal A, Chan MW, Atenafu EG, Masson-Cote
L, Bahl G, Yu E, Millar BA, Chung C, Catton C, O'Sullivan B, et al:
Image-guided, intensity-modulated radiation therapy (IG-IMRT) for
skull base chordoma and chondrosarcoma: Preliminary outcomes. Neuro
Oncol. 17:889–894. 2015.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Gatfield ER, Noble DJ, Barnett GC, Early
NY, Hoole ACF, Kirkby NF, Jefferies SJ and Burnet NG: Tumor volume
and dose influence outcome after surgery and high-dose photon
radiotherapy for chordoma and chondrosarcoma of the skull base and
spine. Clin Oncol (R Coll Radiol). 30:243–253. 2018.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Stacchiotti S, Gronchi A, Fossati P,
Akiyama T, Alapetite C, Baumann M, Blay JY, Bolle S, Boriani S,
Bruzzi P, et al: Best practices for the management of
local-regional recurrent chordoma: A position paper by the chordoma
global consensus group. Ann Oncol. 28:1230–1242. 2017.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Takagi M, Demizu Y, Nagano F, Terashima K,
Fujii O, Jin D, Mima M, Niwa Y, Katsui K, Suga M, et al: Treatment
outcomes of proton or carbon ion therapy for skull base chordoma: A
retrospective study. Radiat Oncol. 13(232)2018.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Meng T, Jin J, Jiang C, Huang R, Yin H,
Song D and Cheng L: Molecular targeted therapy in the treatment of
chordoma: A systematic review. Front Oncol. 9(30)2019.PubMed/NCBI View Article : Google Scholar
|