Introduction
Malignant melanoma as a whole is less frequent in
Asian populations including Japanese population, compared with
Caucasian populations. In the field of ophthalmology, melanoma can
be encountered rarely in uvea (choroid) (1), lacrimal sac (2), conjunctiva and eyelid skin (3,4).
Among these melanomas in ophthalmic practice, conjunctival
malignant melanoma is relatively frequent in Asian populations and
Caucasian populations (3,4). However, no standard treatment has
been established in conjunctival melanoma which is basically at
very low incidence (5).
In case of cutaneous melanoma, its excision with
ample margin of the surrounding normal skin is the standard of care
for local control of malignancy. In contrast, excision of
conjunctival melanoma with ample normal margin cannot be achieved
since the conjunctiva of limited width is the essential mucosa to
maintain the ocular surface and hence, the vision. Due to this
anatomical limitation, it is difficult to excise conjunctival
melanoma at the early phase with ample margin of the surrounding
normal tissue as is the standard of care for cutaneous melanoma. At
present, local recurrence is a common sequela to the initial
excision of conjunctival melanoma. Orbital exenteration is a final
surgical option to achieve the local control in the advanced stages
when conjunctival melanoma shows infiltration into the surrounding
tissue such as the eyelid skin and the sclera of the eyeball. It
would be disastrous for patients to lose the vision of one eye
abruptly by the orbital exenteration. Invasive surgery of the
orbital exenteration would also put physical and psychological
burdens on the aged people who are prone to develop conjunctival
melanoma.
In the general belief that melanoma would not
respond sufficiently to external beam radiation, radiotherapy has
played a limited role only in adjunct or palliative treatment for
metastatic diseases of cutaneous melanoma (6,7),
conjunctival melanoma (5) and head
and neck mucosal melanoma (8,9).
Under the circumstances, proton beam therapy has been tried as a
treatment option for the local control of conjunctival melanoma and
has been indeed shown to be effective (5,10-15).
In Japan, proton beam therapy for head and neck cancer including
melanoma (16-18)
has been covered by reimbursement from the national health
insurance since April 2018. Within the framework of the national
health insurance, immune checkpoint inhibitors and molecular target
drugs such as MEK inhibitors and BRAF inhibitors can be also used
in the case of unresectable and metastatic malignant melanoma,
based on the genetic testing of BRAF mutations in melanoma
tissues (19,20).
The present study dealt with an aged patient who
showed giant conjunctival melanoma at the initial presentation and
who decided to choose proton beam therapy as a first-line
therapeutic option for the local control. Furthermore, based on no
BRAF mutation detected in the melanoma tissue,
pembrolizumab, PD-1 immune checkpoint inhibitor (19,20),
was introduced as a current standard therapy toward metastatic lung
lesions after the proton beam therapy.
Case report
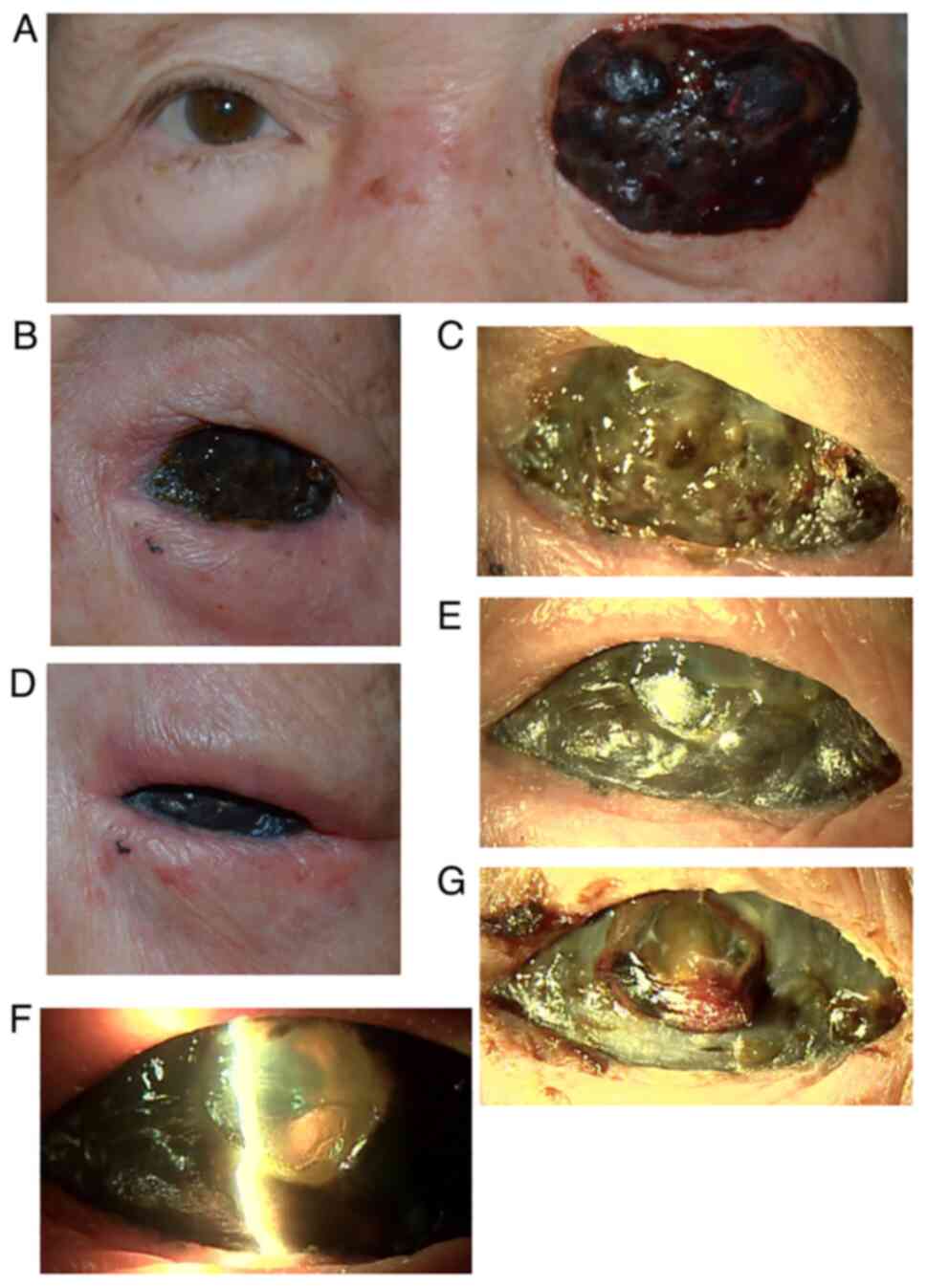
An 80-year-old woman noticed injection and
hemorrhage in the left eye one year previously and she removed the
painless ocular surface scab by herself frequently. One month
previously, the black mass grew out of the lid fissure rapidly and
she could not close the left eye (Fig.
1A). She visited a local hospital and was referred to Okayama
University Hospital. At the initial visit, the best-corrected
visual acuity was 1.2 in the right eye and light perception in the
left eye. The intraocular pressure in the right eye was 12 mmHg and
the optic nerve disc had glaucomatous cupping as a cup/disc ratio
of 0.9. Otherwise, the right eye had nothing notable. She had
undergone cataract surgery in the left eye four years previously.
She had no other medical history and took no medication. A black,
elastic hard, hemorrhage-prone, thickened mass in the size of 30x40
mm with a presumed wide stalk covered the total area of the lid
fissure on the left side (Fig. 1A)
and the mass moved slightly with eye movement, indicative of the
tumor origin on the ocular surface.
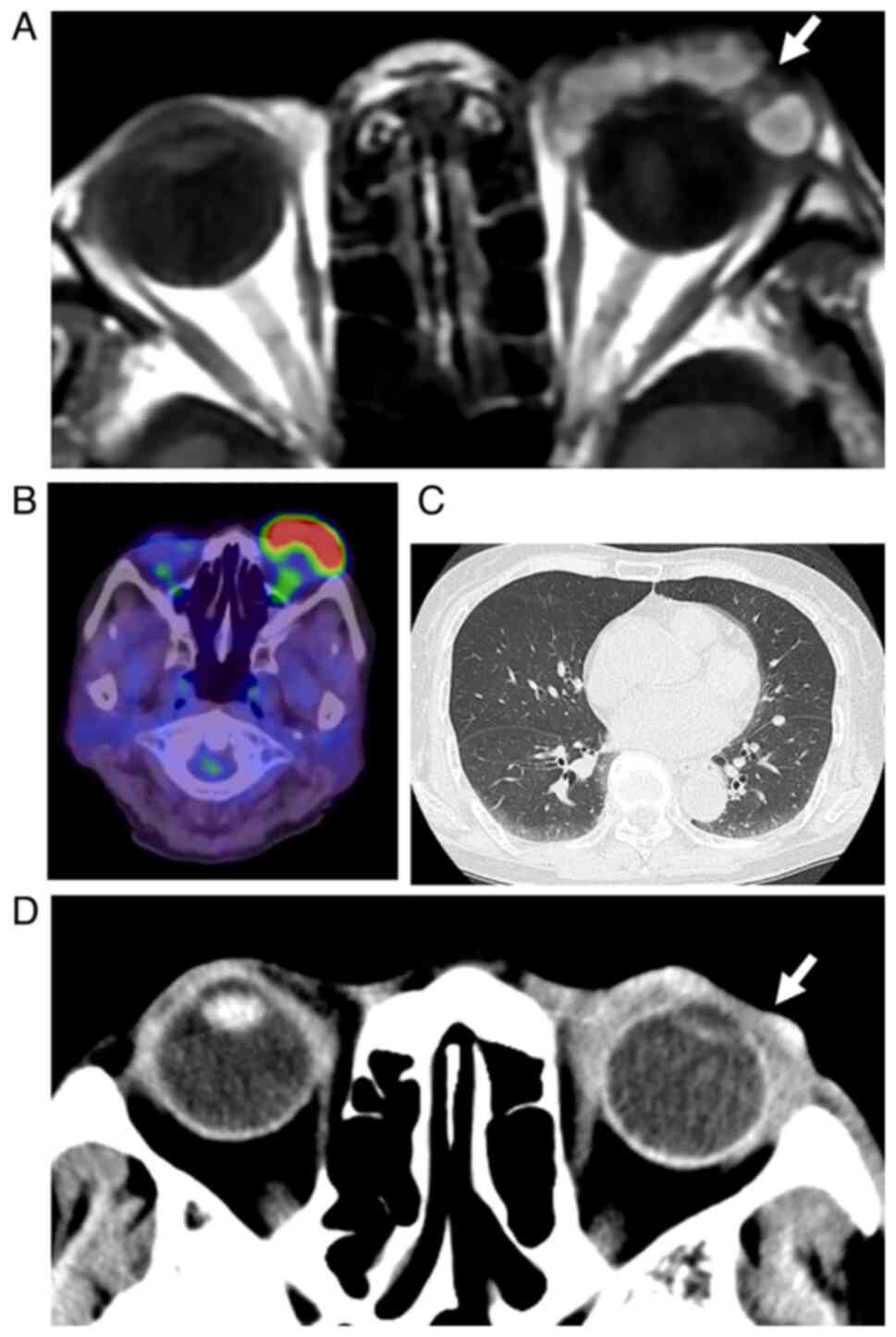
Magnetic resonance imaging showed the intact eye
ball on the left side and no infiltration deeply into the orbit
(Fig. 2A). Whole-body
2-[18F]fluoro-2-deoxy-D-glucose positron emission
tomography (FDG-PET) showed high uptake in the eyelid area with the
mass on the left side (Fig. 2B,
maximum standardized uptake value, SUVmax=14.04) and had no
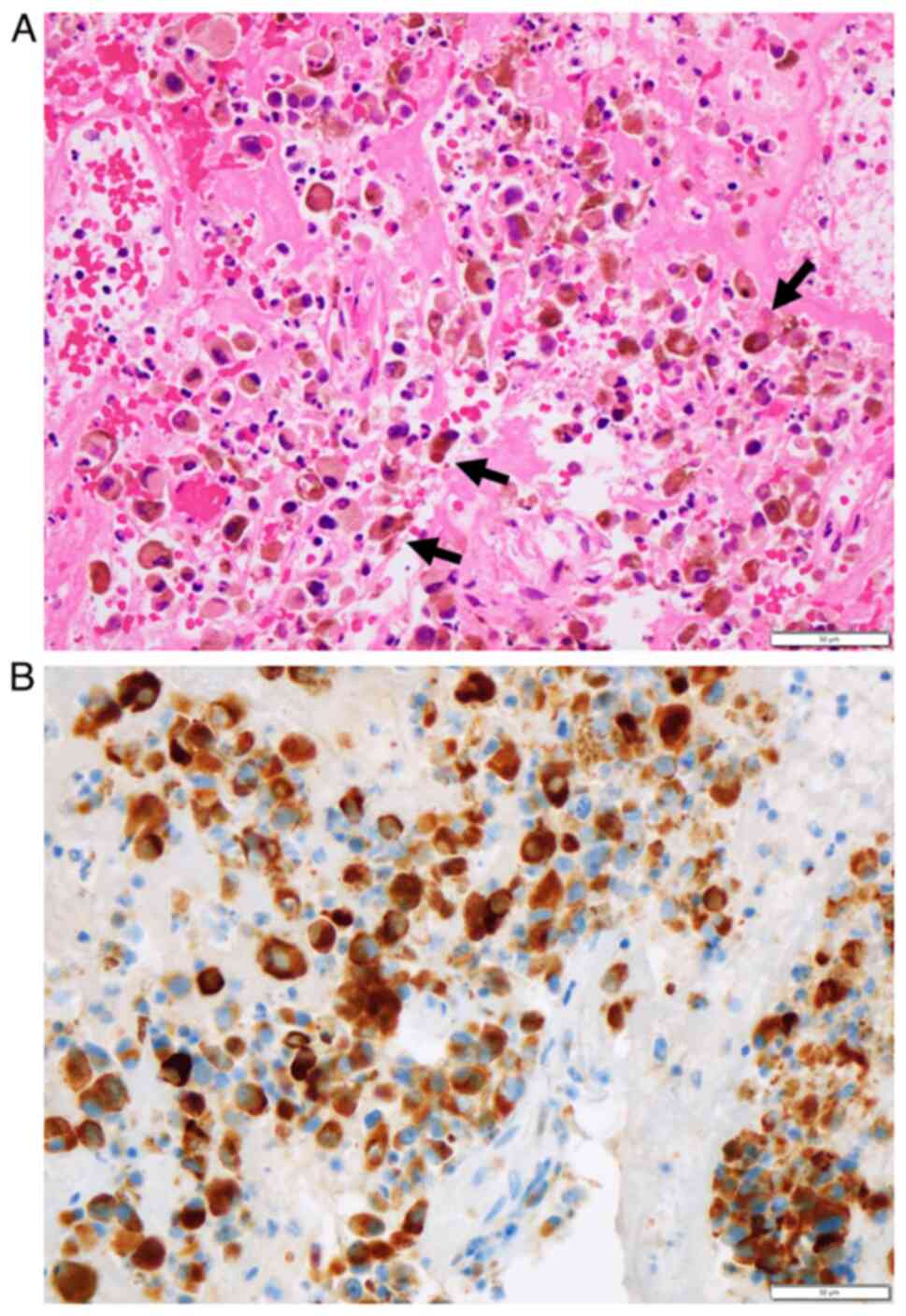
abnormal uptake in other sites of the body. Surface biopsy of the
mass and the neutral formalin-fixed paraffin sections demonstrated
anomalous melanin-containing cells in fibrin and hemorrhage
(Fig. 3A). Immunostaining at the
in-house pathology laboratory showed that anomalous cells were
positive for cocktail-mix antibodies against tyrosinase, melanoma
antigen recognized by T cells-1 and human melanoma black-45
(Fig. 3B), leading to pathological
diagnosis of malignant melanoma.
The patient underwent proton beam therapy one month
after the initial visit, at the total dose of 70.4 Gy (relative
biological effectiveness) in 32 fractions (~10 min each) for one
and a half months. One month after the conclusion of proton beam
therapy and three and a half months from the initial visit, the
patient was found by computed tomographic scan to have multiple
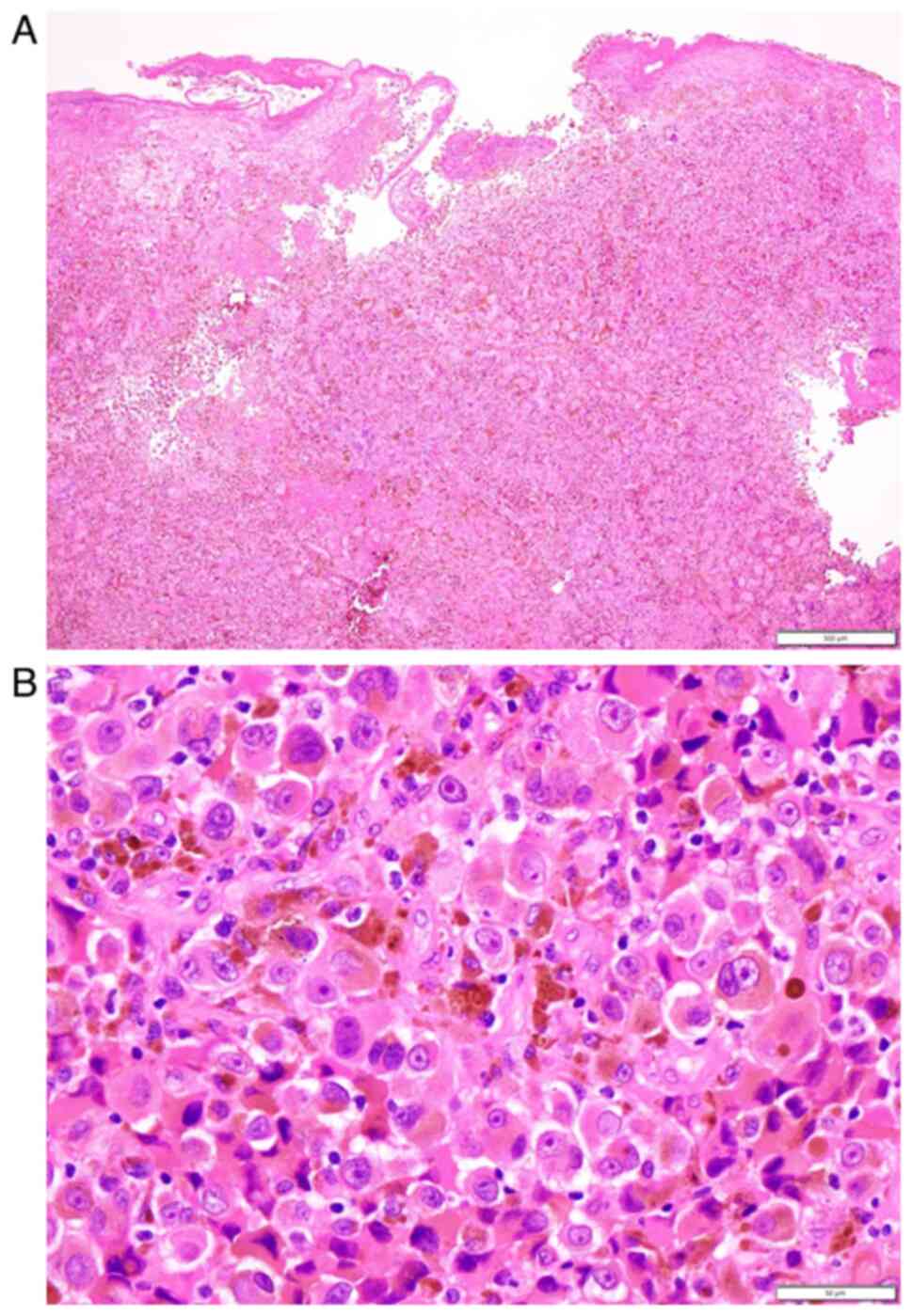
metastatic lesions in bilateral lung fields (Fig. 2C). Excisional biopsy of residual
melanotic lesions in the upper eyelid skin on the left side
(Fig. 1B and D) showed melanin-containing epithelioid
cells with large nuclei and apparent nucleoli (Fig. 4A and B) arranged in alveolar pattern, which
confirmed the pathological diagnosis of malignant melanoma at the
in-house pathology laboratory. BRAF mutations (V600E and
V600K) were tested by real-time PCR in the DNA sample extracted
from the neutral formalin-fixed paraffin sections and were shown to
be absent at an external diagnostic laboratory (LSI Medience
Corporation). The patient then, underwent intravenous
administration of pembrolizumab 77.2 mg every three weeks five
times in total.
At three months after the conclusion of proton beam
therapy, five and a half months from the initial visit, ocular
surface melanoma almost subsided (Fig.
1D and E) and the clear cornea
allowed visualization of the intraocular lens inside the eye
(Fig. 1F). In three weeks,
spontaneous corneal perforation was plugged with iris incarceration
(Fig. 1G). Around the same time,
the patient felt malaise and was found to have hypothyroidism which
was evidenced by low free T3 at 1.75 pg/ml, low free T4 at 0.90
ng/dl, high TSH at 39.9 µU/ml, high anti-thyroglobulin antibody
(TgAb) at 20,664 IU/ml and high anti-thyroid peroxidase antibody
(TPOAb) at 2,580 IU/ml. The patient started to take levothyroxine
sodium hydrate 0.25 µg daily. She died suddenly of unknown cause
7.5 months from the initial visit.
Discussion
The clinical question in the present study is that
proton beam therapy might be a treatment option in the standard of
care for advanced conjunctival malignant melanoma in the era when
proton beam therapy is included in the reimbursement of the
national health insurance in Japan. Orbital exenteration was
initially indicated for the local control of malignancy as the
standard of care in this patient. However, the patient and her
family wished to avoid radical surgery and the clinicians, also
wished to search for the other options because of the patient's
advanced age. Proton beam therapy was thus chosen as the first-line
treatment for unresectable melanoma in the head and neck according
to the rule of the national health insurance in Japan (16-18).
The patient had satisfactory outcome and regained better quality of
life: She had covered the left-side tumor with gauze eye patch for
cosmetic reasons before the therapy while she could blink and close
the eye with the eyelid on the left side after the therapy.
On the initial presentation, biopsy could only
obtain superficial hemorrhage-prone tissue of the tumor and
pathological diagnosis was based on immunocytochemical
examinations. Following the proton beam therapy, excisional biopsy
of the residual eyelid lesion was done again to confirm the
pathological diagnosis of malignant melanoma and also to examine
BRAF mutations in the melanoma tissue. Around the same time,
the patient was found to have multiple metastatic lesions in
bilateral lung fields. According to the standard protocol for
unresectable and metastatic malignant melanoma (19,20),
pembrolizumab was introduced, instead of the combination of MEK
inhibitor and BRAF inhibitor, based on the absence of the
BRAF mutation in the melanoma tissue. The sequence of events
in this patient, namely, proton beam therapy for local control of
unresectable conjunctival malignant melanoma, followed later by the
administration of immune checkpoint inhibitors or the combination
of MEK inhibitor and BRAF inhibitor, could become the standard of
care in the modern era. Indeed, in the present patient,
pembrolizumab appeared to have an effect on the reduction of
malignant melanoma in the original and metastatic lesions, but
actual evaluation of the effect could not be accomplished since the
patient suddenly succumbed.
The patient was reported to have succumbed suddenly
to unknown causes by the emergency transportation to a local
hospital. The patient had hypothyroidism, probably induced by the
administration of pembrolizumab, and thus was taking oral thyroid
hormone. Autoimmune diseases, such as thyroiditis, pneumonitis and
uveitis, should be kept in mind in patients who receive immune
checkpoint inhibitors (21). The
sudden mortality might be attributed to possible carditis or
pneumonitis as a manifestation of pembrolizumab-induced autoimmune
diseases, but the exact situation was not confirmed clinically in
the patient. Until the sudden mortality, the patient was healthy
and had normal activities of daily life.
A major limitation in this case report is that the
patient's presentation was unusual and that the sequence of event
was thus out of the standard. First, only the surface biopsy could
be done in the large protruding hemorrhage-prone melanoma instead
of standard resection. Secondly, proton beam therapy was chosen as
the first-line treatment for this giant conjunctival melanoma. The
aim of therapeutic strategy at the initial presentation was to
enhance the quality of life in this aged woman and the corneal melt
as a sequel to proton beam therapy was anticipated in advance. On
the initial phase of the patient's presentation, it was planned to
use immune checkpoint inhibitors or molecular target drugs as an
adjunct therapy since distant metastases to lung or liver would be
unavoidable at the stage of the disease. In this context, it was
not expected the complete response to proton beam therapy alone and
residual melanoma lesions in the eyelid skin could be used as the
biopsy site for examining the BRAF mutation to determine the
appropriate adjunct therapy. It should be emphasized that the
present case would not be recognized as the standard for local
control of conjunctival melanoma at the current time.
In conclusion, proton beam therapy could be placed
as a treatment option for local control of unresectable
conjunctival malignant melanoma. Proton beam therapy as the
first-line treatment, followed by adjunct therapy with immune
checkpoint inhibitors, could become the standard of care in near
future for unresectable giant conjunctival melanoma. This
conclusion, based on a single patient, naturally has a limitation
to being generalized to the other patients with conjunctival
malignant melanoma.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
TM, as an ophthalmologist and OY, as a
dermatologist, followed and treated the patient, TT, as a
pathologist, made the pathological diagnosis and KK and TW, as
radiologists, treated the patient. TM wrote the manuscript and OY,
TT, KK and TW did critical review of the manuscript. All authors
confirm the authenticity of all the raw data and approved the final
version of the manuscript.
Ethics approval and consent to
participate
Ethics committee review was not applicable to case
reports, based on the Ethical Guidelines for Medical and Health
Research Involving Human Subjects, issued by the Government of
Japan.
Patient consent for publication
Verbal informed consent was obtained from the
patient for her anonymized information to be published in this
article.
Competing interests
The authors declare that they have no competing
interests
References
|
1
|
Matsuo T, Ogino Y, Ichimura K, Tanaka T
and Kaji M: Clinicopathological correlation for the role of
fluorodeoxyglucose positron emission tomography computed tomography
in detection of choroidal malignant melanoma. Int J Clin Oncol.
19:230–239. 2014.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Matsuo T, Tanaka T and Yamasaki O:
Lacrimal sac malignant melanoma in 15 Japanese patients: Case
report and literature review. J Investig Med High Impact Case Rep.
7(2324709619888052)2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Seregard S: Conjunctival melanoma. Surv
Ophthalmol. 42:321–350. 1998.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Vora GK, Demirci H, Marr B and
Mruthyunjaya P: Advances in the management of conjunctival
melanoma. Surv Ophthalmol. 62:26–42. 2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Jain P, Finger PT, Fili M, Damato B,
Coupland SE, Heimann H, Kenawy N, Brouwer NJ, Marinkovic M, Van
Duinen SG, et al: Conjunctival melanoma treatment outcomes in 288
patients: A multicentre international data-sharing study. Br J
Ophthalmol. 105:1358–1364. 2021.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Ballo MT and Ang KK: Radiotherapy for
cutaneous malignant melanoma: Rationale and indications. Oncology
(Williston Park). 18:99–110, 113-114. 2004.PubMed/NCBI
|
|
7
|
Gorayski P, Burmeister B and Foote M:
Radiotherapy for cutaneous melanoma: Current and future
applications. Future Oncol. 11:525–534. 2015.PubMed/NCBI View Article : Google Scholar
|
|
8
|
López F, Rodrigo JP, Cardesa A,
Triantafyllou A, Devaney KO, Mendenhall WM, Haigentz M Jr, Strojan
P, Pellitteri PK, Bradford CR, et al: Update on primary head and
neck mucosal melanoma. Head Neck. 38:147–155. 2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Grant-Freemantle MC, O'Neill BL and Clover
AJP: The effectiveness of radiotherapy in the treatment of head and
neck mucosal melanoma: Systematic review and meta-analysis. Head
Neck. 43:323–333. 2021.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Wuestemeyer H, Sauerwein W, Meller D,
Chauvel P, Schueler A, Steuhl KP, Bornfeld N and Anastassiou G:
Proton radiotherapy as an alternative to exenteration in the
management of extended conjunctival melanoma. Graefes Arch Clin Exp
Ophthalmol. 244:438–446. 2006.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Westekemper H, Anastassiou G, Sauerwein W,
Chauvel P, Bornfeld N, Steuhl KP and Meller D: Analysis of ocular
surface alterations following proton beam radiation in eyes with
conjunctival malignant melanoma. Ophthalmologe. 103:588–595.
2006.PubMed/NCBI View Article : Google Scholar : (In German).
|
|
12
|
Krause L, Mladenova A, Bechrakis NE,
Kreusel KM, Plath T, Moser L and Foerster M: Treatment modalities
for conjunctival melanoma. Klin Monbl Augenheilkd. 226:1012–1016.
2009.PubMed/NCBI View Article : Google Scholar : (In German).
|
|
13
|
Maschi-Cayla C, Doyen J, Gastaud P and
Caujolle JP: Conjunctival melanomas and proton beam therapy. Acta
Ophthalmol. 91(e647)2013.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Scholz SL, Hérault J, Stang A, Griewank
KG, Meller D, Thariat J, Steuhl KP, Westekemper H and Sauerwein W:
Proton radiotherapy in advanced malignant melanoma of the
conjunctiva. Graefes Arch Clin Exp Ophthalmol. 257:1309–1318.
2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Thariat J, Salleron J, Maschi C, Fevrier
E, Lassalle S, Gastaud L, Baillif S, Claren A, Baumard J, Herault J
and Caujolle JP: Oncologic and visual outcomes after postoperative
proton therapy of localized conjunctival melanomas. Radiation
Oncol. 14(239)2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Zenda S, Kawashima M, Nishio T, Kohno R,
Nihei K, Onozawa M, Arahira S and Ogino T: Proton beam therapy as a
nonsurgical approach to mucosal melanoma of the head and neck: A
pilot study. Int J Radiat Oncol Biol Phys. 81:135–139.
2011.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Fuji H, Yoshikawa S, Kasami M, Murayama S,
Onitsuka T, Kashiwagi H and Kiyohara Y: High-dose proton beam
therapy for sinonasal mucosal malignant melanoma. Radiat Oncol.
9(162)2014.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Sakurai H, Ishikawa H and Okumura T:
Proton beam therapy in Japan: Current and future status. Jpn J Clin
Oncol. 46:885–892. 2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Larsen AC, Dahmcke CM, Dahl C, Siersma VD,
Toft PB, Coupland SE, Prause JU, Guldberg P and Heegaard S: A
retrospective review of conjunctival melanoma: Presentation,
treatment and outcome and an investigation of features associated
with BRAF mutations. JAMA Ophthalmol. 133:1295–1303.
2015.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Kiyohara T, Tanimura H, Miyamoto M,
Shijimaya T, Nagano N, Nakamaru S, Makimura K and Iwai H: Two cases
of BRAF-mutated, bulbar conjunctival melanoma, and review of the
published literature. Clin Exp Dermatol. 45:207–211.
2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Matsuo T and Yamasaki O:
Vogt-Koyanagi-Harada disease-like posterior uveitis in the course
of nivolumab (anti-PD-1 antibody), interposed by vemurafenib (BRAF
inhibitor), for metastatic cutaneous malignant melanoma. Clin Case
Rep. 5:694–700. 2017.PubMed/NCBI View
Article : Google Scholar
|