Background
Clear cell chondrosarcoma (CCCS) was first described
as a clear cell variant of chondrosarcoma by Unni et al
(1). CCCS is rare, accounting for
only 2.5-2.7% of all chondrosarcomas (2,3).
CCCS more frequently affects males and is widely distributed across
different age groups (4). This
lesion characteristically appears at the epiphyses of long bones,
particularly in the proximal femur and humerus (5). Radiological and pathological
diagnoses are challenging due to the rarity of the condition and
this may commonly lead to inadequate surgical treatment. Patients
undergoing initial curettage reportedly had a high local recurrence
rate; however, patients who underwent wide resection had a low
recurrence rate (4). The initial
surgical margin for CCCS was observed to correlate with the
oncological outcome (5).
Biopsy has been the gold standard for diagnosing and
managing malignant bone tumours. Unfortunately, tumour cell seeding
in the biopsy tract is a risk factor for local recurrence.
Therefore, biopsy tract removal is widely accepted (6). This frequently requires sacrificing
more healthy tissues and may also lead to poor postoperative limb
function.
The present study reports on a typical case of CCCS
in the right femoral head that was highly suspected using only
radiological methods. The patient was successfully treated with an
en bloc resection without requiring a biopsy of the
lesion.
Case presentation
A 58-year-old male patient reported right hip pain
from June 2018. The patient had visited a nearby clinic and an
abnormality had been observed in the right femoral head on a plain
radiograph. The patient was then referred to Osaka City University
Hospital (Osaka, Japan) in November 2018. Plain radiography
revealed fuzzy, irregular calcifications on the femoral head with
an indistinct distal margin (Fig.
1). Magnetic resonance imaging (MRI) was performed with iso
signal intensity on the T1-weighted image (T1WI; Fig. 2A) and on T2WI, heterogeneously high
signal intensity with a focal enhancement of spotty areas was
observed (Fig. 2B). The lesion was
peripherally enhanced with contrast material on the T1
fat-suppressed image. The decreased spotty signal intensity in
central areas revealed matrix mineralisation (Fig. 2C). A computed tomography (CT) scan
also revealed a honeycomb-like calcification on the femoral head
(Fig. 2D). No cortical destruction
was observed. The tumour size was 40x30x42 mm. At this point, CCCS
was highly suspected in the patient.
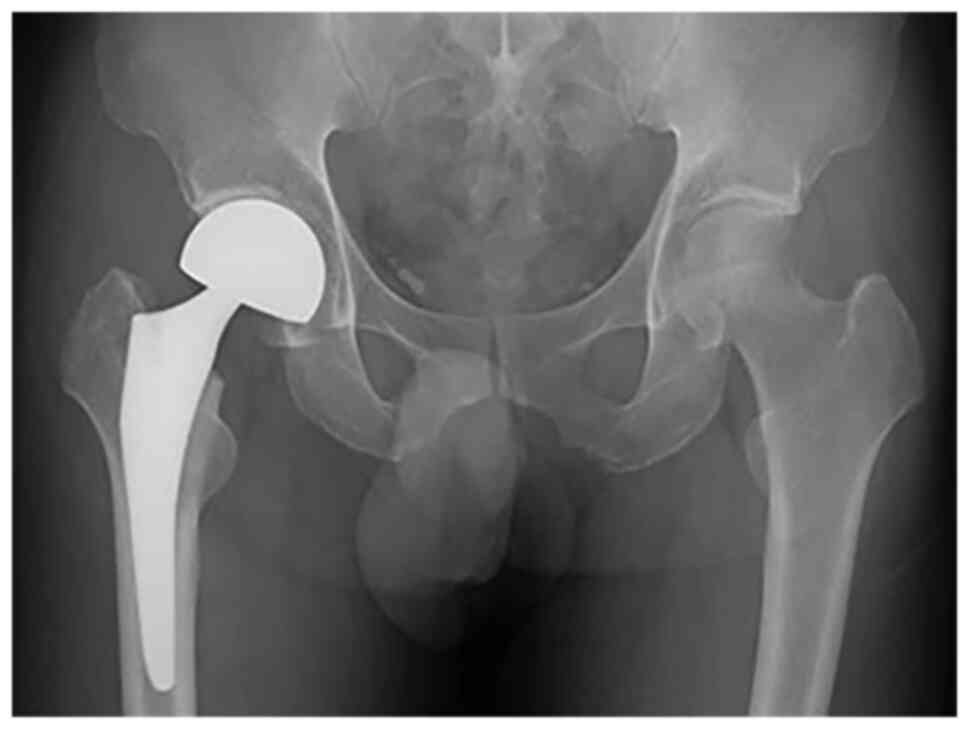
The hip pain was persistent and surgical treatment
was proposed to the patient. En bloc resection and a hip
hemiarthroplasty (Fig. 3) were
performed through an invasive mini-incision anterolateral approach
to detach the anterior third of the gluteus medius to expose the
hip joint (7). At two days after
the surgery, the patient was able to walk with a walker aid. There
were no adverse effects of surgical site infection and hip
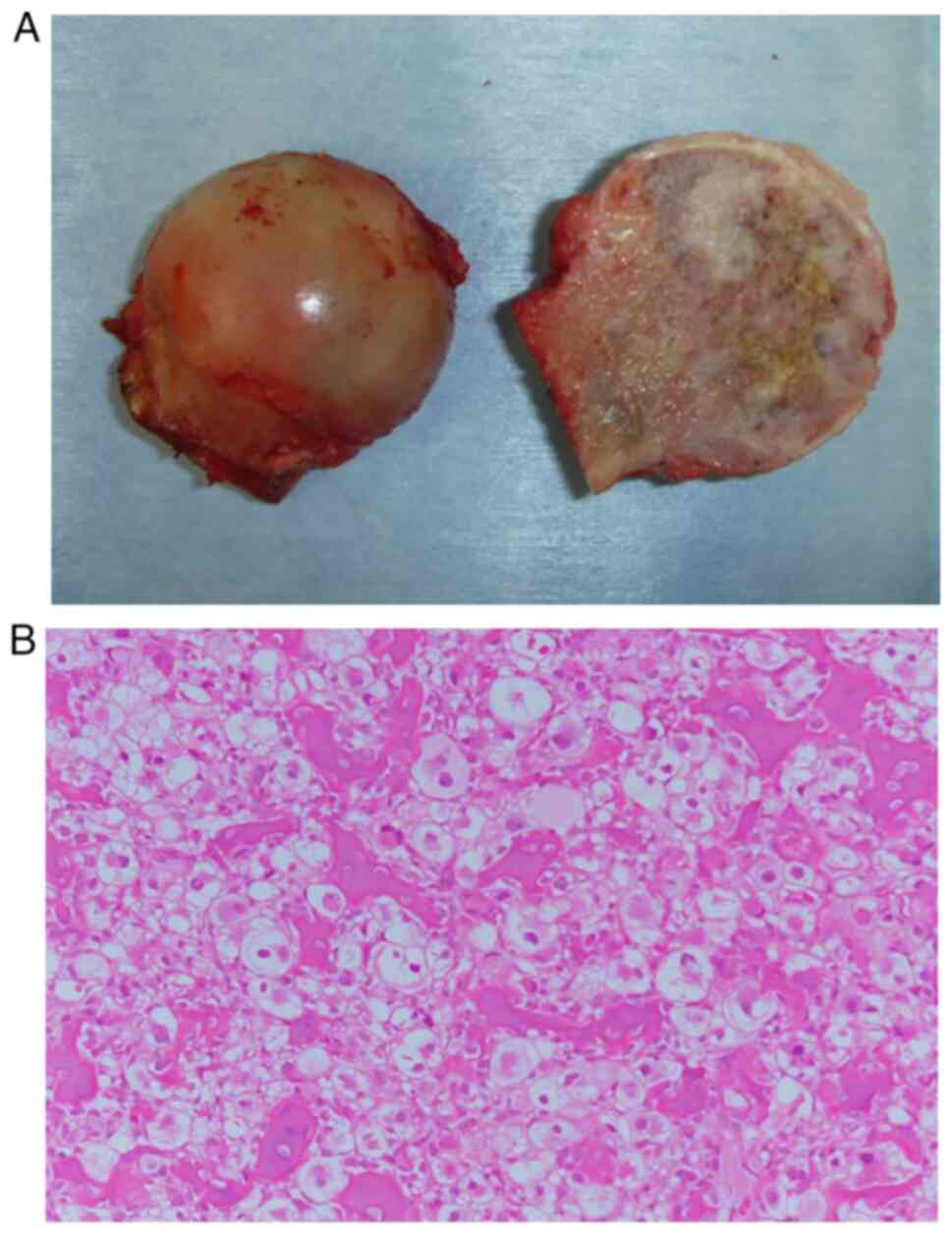
dislocation in his clinical course. The gross findings of the
resected femoral head tumour indicated a mixture of white and
yellow lesions with well-defined borders. Chondroid tissue and
ossification were also visible. The surface cartilage of the
femoral head was smooth and intact, without any evidence of a
pathological fracture (Fig. 4A).
Microscopic examination of the resected specimen indicated that the
tumour was composed of a sheet-like proliferation of atypical cells
with abundant clear cytoplasm, swollen nuclei and scattered bone
formation (Fig. 4B). These
pathological diagnoses were consistent with the typical
presentation of CCCS. A 2-cm-wide margin was obtained after
evaluating the site according to the Japanese Orthopaedic
Association evaluation system (8).
At the final follow-up at 32 months after surgery
(7), no local recurrence or
metastases were observed. The postoperative functional outcome was
measured using the International Symposium on Limb Salvage score
(9). The patient scored 30 points,
which is the highest possible outcome.
Discussion
In the current case, radiological imaging with plain
radiography, MRI and CT scan revealed a typical presentation of
CCCS in the right femoral head. Therefore, an incisional biopsy was
deemed unnecessary and an en bloc resection and hip
hemiarthroplasty were performed without any preoperative biopsy.
Pathological diagnosis confirmed the presence of CCCS and a clear
surgical margin was achieved. The postoperative limb function of
the patient was excellent at the final follow-up.
In cases of a suspicious malignant bone tumour
located in the femoral head, incisional biopsy is planned from the
lateral side of the proximal femur through the femoral neck to
prevent the tumour from contaminating the hip joint space (10). To remove a biopsy tract that
potentially contains tumour cells, hip replacement with a tumour
prosthesis is necessary after en bloc resection, resulting
in poor postoperative function compared to that achieved through
hip hemiarthroplasty. Therefore, after considering the surgical
margin and the postoperative function of the patient, en
bloc resection without performing a biopsy may be an acceptable
treatment option for radiologically typical CCCS.
Collins et al (11) explored certain typical radiological
features of CCCS on plain radiographs, CT scans and MRI, which
closely matched those in the present case. Specifically, the CT
scan revealing matrix mineralisation with characteristic chondroid
appearance was similar to that in the present case. The World
Health Organisation (12) has
stated that CCCS is a primary bone tumour primarily affecting the
ends of the bone, mainly in the proximal femur and humerus.
Radiographically, giant cell tumour of the bone, chondroblastoma,
chondrosarcoma and chondroblastic osteosarcoma, and osteonecrosis
of the femoral head were all differential diagnoses (3). It is likely that every experienced
orthopaedic oncologist in a specialised centre may be capable of
suspecting the presence of CCCS in the femoral head, just as in our
case.
Histological diagnosis is vital to initiate precise
treatment for bone tumours. Compared to an incisional biopsy, a
core needle biopsy may at times provide an incorrect diagnosis,
usually due to insufficient material quality (6). Therefore, Nakayama et al
(5) recommend an incisional biopsy
for suspected CCCS over a core needle biopsy. However, incisional
biopsy for preoperative diagnosis requires sampling of the tumour,
increasing the risk of potentially contaminating healthy
tissue.
The reconstruction method after en bloc
resection of the femoral head is also worth discussing. Total hip
replacement (THR) is able to better maintain the postoperative hip
function compared to hemiarthroplasty. However, if the CCCS
recurred after THR, particularly in the acetabulum, the second
operation would be complicated. Tumour seeding may potentially
expand in the overall operating field (8). In the current case, hemiarthroplasty
was selected as a prevention of potential tumour expansion in the
acetabulum.
CCCS is a low-grade, malignant chondrogenic tumour
resistant to chemotherapy and radiotherapy, and surgical removal
using adequate margins is the primary treatment strategy for it
(4). The surgical margin in these
tumours highly correlates with local recurrence and lung metastases
(2-5).
Itälä et al (2) determined
that the 5-year and 10-year survival rates were 100 and 89%,
respectively. Nakayama et al (5) reported that the 5- and 10-year
overall survival rates were both 89%. Local recurrence and lung and
bone metastases were discovered over five years after the initial
diagnosis (2,3,5).
Orthopaedic oncologists must be aware that careful long-term
follow-up is necessary to detect any recurrences or metastases over
time.
In conclusion, in the presence of typical
radiological findings for CCCS, en bloc resection without
any prior biopsy may be an acceptable treatment for CCCS located on
the femoral head.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
MH and HN were responsible for study design and
writing of the manuscript. NO and YO analyzed/interpreted the data.
AT was responsible for collection of data and scanning images from
medical records and performed the histological examination of the
tumour. All authors read and approved the final manuscript. NO and
YO checked and approved the authenticity of the raw data.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this case report and any accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Unni KK, Dahlin DC, Beabout JW and Sim FH:
Chondrosarcoma: Clear-cell variant. A report of sixteen cases. J
Bone Joint Surg Am. 58:676–683. 1976.PubMed/NCBI
|
|
2
|
Itälä A, Leerapun T, Inwards C, Collins M
and Scully SP: An institutional review of clear cell
chondrosarcoma. Clin Orthop Relat Res. 440:209–212. 2005.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Donati D, Yin JQ, Colangeli M, Colangeli
S, Bella CD, Bacchini P and Bertoni F: Clear cell chondrosarcoma of
bone: Long time follow-up of 18 cases. Arch Orthop Trauma Surg.
128:137–142. 2008.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Bjornsson J, Unni KK, Dahlin DC, Beabout
JW and Sim FH: Clear cell chondrosarcoma of bone. Observations in
47 cases. Am J Surg Pathol. 8:223–230. 1984.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Nakayama R, Hayakawa K, Kobayashi E, Endo
M, Asano N, Yonemoto T, Kawashima H, Hamada K, Watanabe I, Futani
H, et al: What factors are associated with treatment outcomes of
Japanese patients with clear cell chondrosarcoma? Clin Orthop Relat
Res. 478:2537–2547. 2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Traina F, Errani C, Toscano A, Pungetti C,
Fabbri D, Mazzotti A, Donati D and Faldini C: Current concepts in
the biopsy of musculoskeletal tumors. J Bone Joint Surg Am.
97(e7)2015.PubMed/NCBI
|
|
7
|
Berger RA: Mini-incision total hip
replacement using an anterolateral approach: Technique and results.
Orthop Clin North Am. 35:143–151. 2004.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Kawaguchi N, Ahmed AR, Matsumoto S, Manabe
J and Matsushita Y: The concept of curative margin in surgery for
bone and soft tissue sarcoma. Clin Orthop Relat Res. 419:165–172.
2004.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Enneking WF, Dunham W, Gebhardt MC,
Malawar M and Pritchard DJ: A system for the functional evaluation
of reconstructive procedures after surgical treatment of tumors of
the musculoskeletal system. Clin Orthop Relat Res. 286:241–246.
1993.PubMed/NCBI
|
|
10
|
Liu PT, Valadez SD, Chivers FS, Roberts CC
and Beauchamp CP: Anatomically based guidelines for core needle
biopsy of bone tumors: Implications for limb-sparing surgery.
Radiographics. 27:189–206. 2007.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Collins MS, Koyama T, Swee RG and Inwards
CY: Clear cell chondrosarcoma: Radiographic, computed tomographic,
and magnetic resonance findings in 34 patients with pathologic
correlation. Skeletal Radiol. 32:687–694. 2003.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Baumhoer D, Bloem JL and Oda Y: Clear cell
chondrosarcoma. In: WHO Classification of Tumours of Soft Tissue
and Bone. WHO classification of tumours editorial board (eds). IARC
Press, Lyon, pp383-384, 2020.
|