Introduction
Every year, ~500,000 women are affected with
cervical cancer worldwide and ~270,000 women succumb to this
disease (1). The cervical cancer
frequency is higher in still-advancing countries that typically
have far fewer medical resources (2). As the world's population grows and
ages, cases of cervical cancer have the potential to increase
significantly.
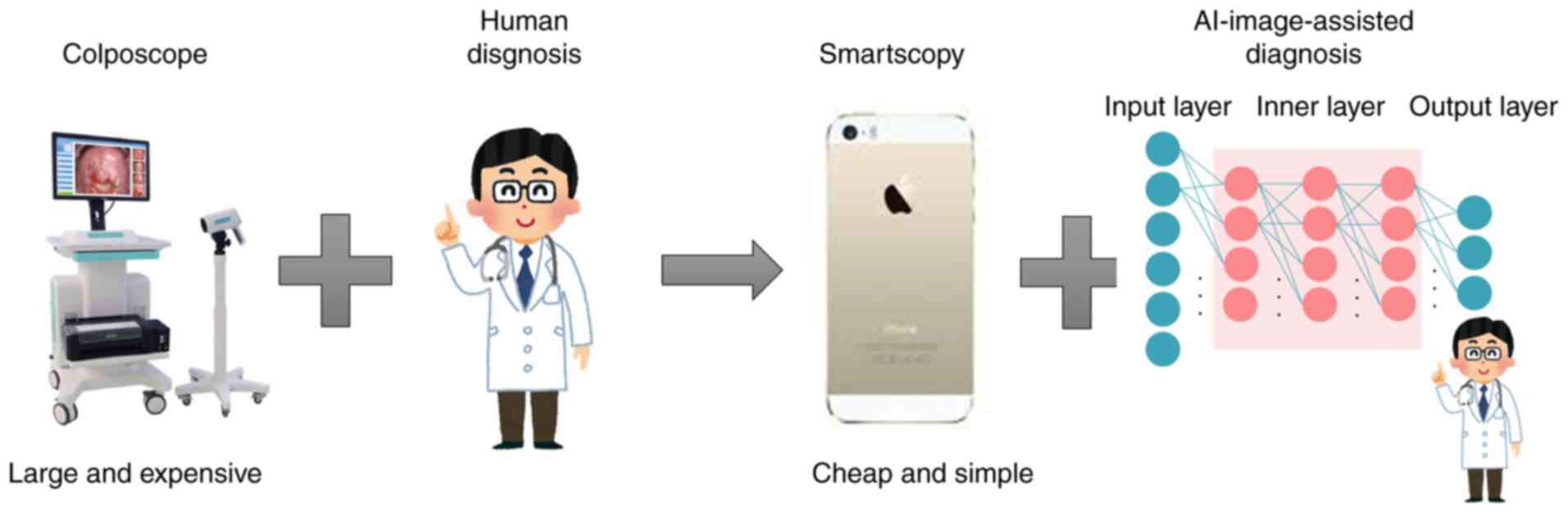
The traditional biopsy routine for cervical cancer
diagnosis is that gynecologists manually observe the uterine cervix
with a colposcope and decide where to obtain a tissue sample for
more detailed microscopic examination. There are problems to this
method. First, colposcopes are large and expensive. Second,
gynecologists require a great deal of practical experience in
deciding correctly from which part of the cervix is best to obtain
the tissue.
To address this shortcoming, the present study
created a system of AI-assisted image diagnosis (AISD) for cervical
lesions. This AI system can guide the inexperienced in their
selection of the best biopsy sites. If AISD for cervical lesions
could be normalized for use in professional practice, the biopsy
itself might become obsolete, or used only when absolutely needed
for a definitive opinion. This economical and simple improvement in
diagnostic capabilities would reduce the burden for gynecologists
and could be expanded to medical facilities in localities, regions
and advancing countries that have fewer medical resources. This
would be conducive for provision of proper medical treatments and
decreasing the overall cervical cancer burden (Fig. 1).
Tanaka et al (3) were the first to report the capability
of a smartphone for diagnostic-assistance (Smartscopy; Apple Inc.).
They found that it can detect 90.8% of the same pathological
cervical lesion detectable by colposcopy. The detection sensitivity
of pathological lesions that were for cervical intraepithelial
neoplasia (CIN)2 or greater was 92%. From this work, they concluded
that the imaging quality of Smartscopy is appropriate for
diagnosis.
The aim of the present study was to achieve AISD for
cervical lesion using images taken by Smartscopy and report the
performance assessment of AISD for cervical lesions taken by
colposcope. This system could be subsequently applied toward
Smartscopy images.
Materials and methods
The present study was a cooperative research project
with Kyocera Corporation, a maker of advanced smartphones and AI
software. University Clinical Research Review Committee approved
this research [17257(T7)-8]. All methods were performed in
accordance with the relevant guidelines and regulations.
Patients
Colposcopy and biopsy were performed on 463 patients
by gynecologic oncologists at the Osaka University Hospital between
January 2010 and August 2019. The median age of the patients was 46
years (range 23-82). This is a retrospective study in which the
patient data was fully de-identified. The present study was
approved by the Institutional Review Board and the Ethics Committee
of the Osaka University Hospital [approval no. 17257(T7)-8]. The
researchers obtained informed consent from participants of the
survey on the questionnaire, which was anonymous. The present study
included only those who consented to participate.
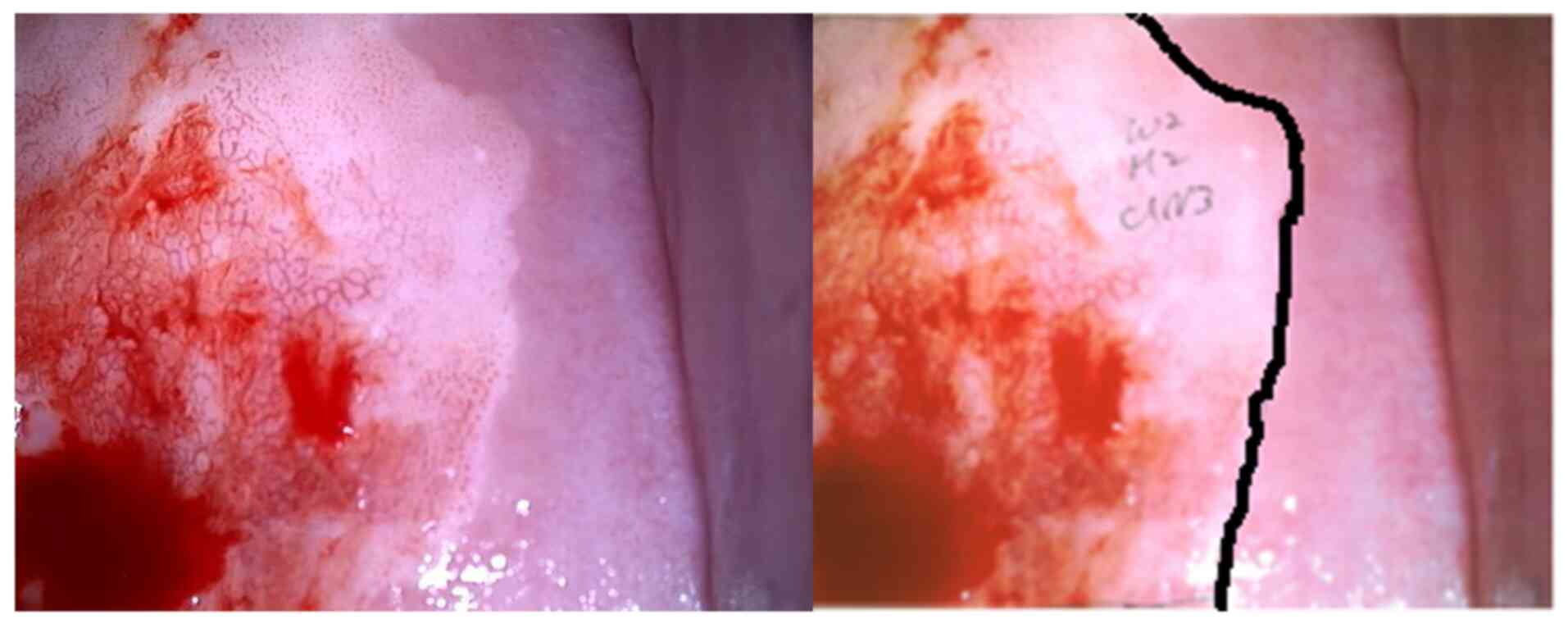
Images of pathological lesions
A total of 463 images from 463 patients taken by
colposcope were analyzed. The images were of pathological cervical
lesions processed with acetic acid prior to biopsy. These images
were cropped to 224x224 pixels and saved as JPEG files. Gynecologic
oncologists annotated the images according to pathological lesions
(Fig. 2). The images were used
retrospectively as the input data for deep learning by Kyocera. Of
463 images, 120 were normal, 120 were CIN1, 113 were CIN2-3 and 110
were of invasive cancer (Table
I).
 | Table IThe distribution of images. |
Table I
The distribution of images.
| | Normal | CIN1 | CIN2-3 | Invasive cancer | Total |
|---|
| Images | 120 | 120 | 113 | 110 | 463 |
| | Training | Test | Training | Test | Training | Test | Training | Test | Training | Test |
| | 90 | 30 | 90 | 30 | 85 | 28 | 83 | 27 | 348 | 115 |
Preparation
A randomly selected subset of 115 of the 463 images
was employed as a ‘test dataset’ and the remaining 348 images were
used as the training dataset (Table
I). Next, 25% of the training dataset was used in Group 1, 50%
in Group 2, 75% in Group 3 and all of the training dataset was used
in Group 4.
The number of images was also increased. The use of
triple images for the training dataset was investigated by adding
rotated or blurred images and quadruple images were tested by
changing the hue, chroma (purity or intensity of color) and
brightness (HSV), as is the standard practice in computer image
analysis.
AI image diagnosis
GoogLeNet (Inception v1) (4) software was used with a convolutional
neural network. After the images for the training dataset were
investigated using deep learning with a convolutional neural
network, the traditional colposcopy diagnosis and AI image
diagnosis for the test dataset were compared.
Human accuracy assisted with AI
During the period between October of 2020 and
January of 2021, 100 images (25 images for each pathology category)
were presented to a panel of 32 gynecologists in the Osaka
University Graduate School of Medicine, Niigata University Graduate
School of Medicine, Kanazawa Medical University, University of
Occupational and Environmental Health, Kawasaki Medical University,
Hiramatsu Obstetrics and Gynecology Clinic, Saito Women Clinic,
Ladies Clinic Yagi and Maki Ladies Clinic. They diagnosed each
image as belonging to one of the four categories. Next, they
re-diagnosed every image after the AI diagnosis was revealed to
them. Changes in human diagnosis and the accuracy of the AI-image
diagnosis was assessed.
Statistical analysis
Using Medcalc (https://www.medcalc.org), differences between groups
were calculated by the χ2 test and the logistic
regression test for categorical variables. P<0.05 was considered
to indicate a statistically significant difference.
Results
Performance of AI for diagnosis for
pathological lesions
The average accuracy of diagnosis for pathological
lesions solely by AI was 43.5%. For the four categories, the
accuracy was 57.8% for normal, 35.4% for CIN1, 40.5% for CIN2-3 and
44.2% for invasive cancer (Table
II).
| Table IIThe accuracy of AI image
diagnosis. |
Table II
The accuracy of AI image
diagnosis.
| | Accuracy (%) |
|---|
| Normal | 57.8 |
| CIN1 | 35.4 |
| CIN2-3 | 40.5 |
| Invasive cancer | 44.2 |
| Total | 43.5 |
To improve accuracy, the number of images per slide
for the training dataset were changed. Table III shows the accuracy for each
category. In group 1, 25% images were used for the training dataset
and the accuracy was 48.2% for normal, 19.9% for CIN1, 30.4% for
CIN2-3 and 54.1% for invasive cancer. In group 2, 50% images were
used for the training dataset, 25% images more than for group 1;
the group 2 accuracy was 47.7% for normal, 29.7% for CIN1, 29.5%
for CIN2-3 and 52.5% for invasive cancer. In group 3, 75% images
were used for the training dataset; the accuracy was 53.6% for
normal, 30.1% for CIN1, 42.9% for CIN2-3 and 46.3% for invasive
cancer. In group 4, 100% images were used for the training dataset
and the accuracy improved to 57.8% for normal, 35.4% for CIN1,
40.5% for CIN2-3 and 44.2% for invasive cancer. Increasing the
number of images in the training dataset beyond 25% did not lead to
a significant improvement in the accuracy for the four categories
(Table III).
| Table IIIAccuracy of AI image diagnosis of each
group. |
Table III
Accuracy of AI image diagnosis of each
group.
| | Group 1 25% of
training case (%) | Group 2 50% of
training case (%) | Group 3 75% of
training case(%) | Group 4 100% of
training case (%) |
|---|
| Normal | 48.2 | 47.7 | 53.6 | 57.8 |
| CIN1 | 19.9 | 29.7 | 30.1 | 35.4 |
| CIN2-3 | 30.4 | 29.5 | 42.9 | 40.5 |
| Invasive cancer | 54.1 | 52.5 | 46.3 | 44.2 |
| Total | 36.4 | 37.9 | 42.1 | 43.5 |
Next, whether increasing the number of images per
slide could improve the accuracy of image diagnosis, as is standard
practice in computer science was investigated. Tripling the number
of images for the training dataset by adding rotated and blurred
images and quadrupling the images by changing HSV was also
investigated. However, none of these efforts improved upon the
accuracy of using a single image.
AI-assisted image diagnosis
The accuracy of the human diagnosis of cervical
pathological images by gynecologists before knowing the diagnosis
from AI was 64.8% for normal, 54.4% for CIN1, 54.4% for CIN2-3 and
38.9% for invasive cancer. Once they became aware of the AI
diagnosis, the human diagnosis accuracy was 63.3% for normal, 51.1%
for CIN1, 58.0% for CIN2-3 and 48.5% for invasive cancer (Table IV).
| Table IVSignificance of AI-assisted image
diagnosis. |
Table IV
Significance of AI-assisted image
diagnosis.
| Lesions | Initial | AI-assisted | P-value |
|---|
| Normal | 518/800 (64.8%) | 506/800 (63.3%) | 0.57 |
| CIN 1 | 435/800 (54.4%) | 409/800
(51.1%) | 0.21 |
| CIN 2-3 | 435/800
(54.4%) | 464/800
(58.0%) | 0.14 |
| Invasive
cancer | 311/800
(38.9%) | 388/800
(48.5%) | <0.01 |
Discussion
AI is being applied across various disciplines,
including phonetic recognition, image recognition, face recognition
and automated driving technology. Similarly, AI applications are
expected to evolve rapidly in many medical fields (5). The medical sector is heavily burdened
with many challenges to overcome. There is scarcity of medical
professionals, area to area medical bias, bias between treatment
departments, crushing labor hours, lapses in safety and stability
of the medical delivery system. AI can potentially reduce or
resolve many of these problems.
Incorporating AI into medical practices is expected
to improve the medical environment across Japan. Patients could
receive safer and more adequate medical services, the overload of
medical professionals could be reduced and new methods of diagnosis
and treatment could be developed.
The Japanese Ministry of Health, Labor and Welfare
has selected six important areas for AI development (6). These encompass genomic medicine,
diagnostic imaging, assistance with diagnosis and treatment, drug
development, caregiving for dementia and surgical assistance. Among
these areas, diagnostic imaging is regarded the most practical for
rapid AI adoption as most medical images are already digitized and
application of established AI-associated technology would be
easier.
The number of AI image recognition software has seen
dramatic recent increase and there have already been reports of AI
automated diagnosis being conducted (Table V).
| Table VSummary of AI reports. |
Table V
Summary of AI reports.
| Author (year) | Subject | (Refs.) |
|---|
| Hu et al
(2019) | Pioneer of
automated visual evaluation of cervigrams | (7) |
| Xue et al
(2020) | AI assistance in
colposcopy imaging judgment | (8) |
| Yuan et al
(2020) | High performance of
AI diagnostic system | (9) |
| Xue et al
(2020) | Automated visual
evaluation on smartphones | (10) |
| Miyagi et al
(2020) | AI colposcopy
combined with HPV types | (11) |
| Tan et al
(2021) | AI assistance in
thin-prep cytological test images | (12) |
As pioneers in this field, Hu et al (7) report that automated visual evaluation
of cervigrams can identify precancer/cancer cases with great
accuracy [area under the curve (AUC)=0.91]. Xue et al
(8) report the potential of AI to
address the colposcopic bottleneck, which could assist
colposcopists in colposcopy image diagnosis, the detection of
underlying CINs and the guidance of biopsy sites.
Yuan et al (9) report that the sensitivity,
specificity and accuracy of the classification model to
differentiate negative cases from positive cases were 85.38, 82.62
and 84.10%, respectively, with an AUC of 0.93. The recall and
Sørensen-Dice coefficient of the segmentation model to segment
suspicious lesions in acetic acid images were 84.73 and 61.64%,
with an average accuracy of 95.59%. Furthermore, 84.67% of
high-grade lesions were detected by the acetic detection model.
Compared to colposcopists, the diagnostic system showed improved
performance for ordinary colposcopy images but was slightly
unsatisfactory for high-definition images.
Furthermore, Xue et al (10) report that automated visual
evaluation by smartphones can be a useful adjunct to health-worker
visual assessment with acetic acid, a cervical cancer screening
method commonly used in low- and middle-resource settings. Miyagi
et al (11) report the
feasibility of using deep learning to classify cervical squamous
epithelial lesions (SILs) from colposcopy images combined with
human papillomavirus (HPV) types. The sensitivity, specificity,
positive predictive value, negative predictive value and the AUC ±
standard error for AI colposcopy combined with HPV types and
pathological results were 0.956 (43/45), 0.833 (5/6), 0.977
(43/44), 0.714 (5/7) and 0.963±0.026, respectively.
Tan et al (12) report that computer-based deep
learning methods can achieve high-accuracy fast cancer screening
using thin-prep cytological test images. This system could classify
the images and generate a test report in ~3 min with high
performance (the sensitivity and specificity was 99.4 and 34.8%,
respectively, with an AUC of 0.67).
In all of these reports, cervical pathology was
divided into two or three categories, atypical squamous cells of
undetermined significance, low grade (L)SIL (normal and CIN1) and
high grade (H)SIL (CIN2 and over). The present study is the first
(to the best of the authors' knowledge) to report the evaluation of
AI image diagnosis using four categories. The average accuracy was
43.5% particularly for CIN2-3 and 44% for invasive cancer. This is
lower than the accuracy of the other two categories. To further
improve AI accuracy, the number of training dataset images for
various methods was increased, but this was unsuccessful.
In the future, diagnosis using images captured by
the Smartscope will be evaluated. It is hypothesized that AI
accuracy might be improved with improved context and timing of
image-acquisition.
The present study reported, for first time to the
best of the authors' knowledge, on the integration of AI and human
image diagnosis for uterine cervical pathological lesions. It was
evident that AI-assisted image diagnosis could significantly
improve the gynecologist's accuracy for diagnosing of the category
of invasive cervical cancer and it tended to improve diagnosis
accuracy for CIN2-3, but not CIN1 and normal.
When comparing the initial accuracy of AI and humans
diagnoses, the accuracy of humans was higher for normal and CIN1
(64.8 and 54.4%, respectively. AI-assisted accuracy was higher for
CIN2-3 and invasive cancer (58 and 48.5%, respectively).
For mammography screening, AI advances could be used
to increase screening accuracy by reducing missed cancers and false
positives. Salim et al (13) performed AI computer-aided detection
algorithms as independent mammography readers and assessed the
screening performance when combined with radiologists. The results
indicate that AI computer-aided detection algorithms can assess
screening mammograms with a sufficient diagnostic performance that
could be further evaluated as an independent readers in prospective
clinical trials.
Schaffter et al (14) evaluated whether AI could overcome
human mammography interpretation limitations; >1,100 subjects,
comprising 126 teams from 44 countries participated. The
top-performing algorithms achieved an AUC of 0.858 (United States)
and 0.903 (Sweden) and a specificity of 66.2% (United States) and
81.2% (Sweden) compared with the radiologists' sensitivity, which
was lower than community-practice radiologists' specificity of
90.5% (United States) and 98.5% (Sweden). Combining top-performing
algorithms and US radiologist assessments resulted in a higher AUC
of 0.942 and achieved a significantly improved specificity (92.0%)
at the same sensitivity.
Humans are still responsible for any AI-assisted
diagnosis in Japan. At present, it need not be argued ‘Which is
better, human or AI?’ or ‘Will humans be dumped into the dustbin of
medical history?’ Instead, we are looking toward a way to realize
the powerful potential of human and AI cooperation in medicine.
The present study has a limitation. The accurate
diagnosis rate of AI-based diagnosis is in the 40% range, which
cannot be used in clinical practice. This could be attributed to
the evaluation of AI image diagnosis in four categories in the
current study. In previous reports (7,9-12),
the cervical pathology was divided into two or three categories. In
the present study, the diagnostic accuracy when divided into two
categories was 79.4% in HSIL and 87.0% in LSIL, comparable to other
reports (7,9-12).
In some reports, the accuracy for detecting HSIL by colposcopy was
~80-90%, the sensitivity was ~80% and specificity was ~70%
(15,16). This level is felt necessary for
clinical utility, which might be a limitation in colposcopic
diagnosis.
For four categories of cervical cancer pathology
diagnosis, the accuracy of AI image diagnosis was 57.8% for normal,
35.4% for CIN1, 40.5% for CIN2-3 and 44.2% for invasive cancer.
AI-assisted image diagnosis significantly improved the diagnostic
accuracy of the gynecologist for invasive cancer and tended to
improve slightly the gynecologist's accuracy for CIN2-3, but it did
not improve the gynecologist's accuracy regarding the categories of
CIN1 and normal cervix.
Acknowledgements
The authors would like to thank Dr GS Buzard
(Department of Obstetrics and Gynecology, Osaka University Graduate
School of Medicine) for his constructive criticism and editing of
our manuscript.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets during and/or analyzed during the
current study available from the corresponding author on reasonable
request.
Authors' contributions
YI designed the study and interpreted the results,
AM wrote the manuscript, designed the study and interpreted the
results, YU designed the study and interpreted the results, YT, RN,
AM, MSh, TE, MSe, TE, TS, KY, HH, TN, TM, KH, JS, JY, YT and TK
performed sample preparation. AM and YI confirm the authenticity of
all the raw data. All authors reviewed and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Review Board and the Ethics Committee of the Osaka University
Hospital [approval no. 17257(T7)-8]. The researchers obtained
informed consent from participants of the survey on the
questionnaire, which was anonymous. The present study included only
those who consented to participate.
Patient consent for publication
Not applicable.
Competing interest
The present study was a cooperative research project
with Kyocera Corporation.
References
|
1
|
WHO Disease and Injury Country Estimates.
Available from: https://www.who.int/healthinfo/global_burden_disease/estimates_country/en/.
|
|
2
|
Hull R, Mbele M, Makhafola T, Hicks C,
Wang SM, Reis RM, Mehrotra R, Mkhize-Kwitshana Z, Kibiki G, Bates
DO and Dlamini Z: Cervical cancer in low and middle-income
countries. Oncol Lett. 20:2058–2074. 2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Tanaka Y, Ueda Y, Kakubari R, Kakuda M,
Kubota S, Matsuzaki S, Okazawa A, Egawa-Takata T, Matsuzaki S,
Kobayashi E and Kimura T: Histologic correlation between smartphone
and coloposcopic findings in patients with abnormal cervical
cytology: Experiences in a tertiary referral hospital. Am J Obstet
Gynecol. 221:241.e1–241.e6. 2019.PubMed/NCBI View Article : Google Scholar
|
|
4
|
https://towardsdatascience.com/a-simple-guide-to-the-versions-of-the-inception-network-7fc52b863202.
|
|
5
|
Jiang F, Jiang Y, Zhi H, Dong Y, Li H, Ma
S and Wang Y, Dong Q, Shen H and Wang Y: Artificial intelligence in
healthecare: Past, present and future. Strole Vasc Neurol.
2:230–243. 2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
WHO: The Global Health Observatory.
Explore a world of health data. Available from: https://www.mhlw.go.jp/content/10601000/000568486.pdf.
|
|
7
|
Hu L, Bell D, Antani S, Xue Z, Yu K,
Horning MP, Gachuhi N, Wilson B, Jaiswal MS, Befano B, et al: An
observational study of deep learning and automated evaluation of
cervical images for cancer screening. J Natl Cancer Inst.
111:923–932. 2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Xue P, Ng MT and Qiao Y: The challenges of
colposcopy for cervical cancer screening in LMICs and solutions by
artificial intelligence. BMC Med. 18(169)2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Yuan C, Yao Y, Cheng B, Cheng Y, Li Y, Li
Y, Liu X, Cheng X, Xie X, Wu J, et al: The application of deep
learning based diagnostic system to cervical squamous
intraepithelial lesions recognition in colposcopy images. Sci Rep.
10(11639)2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Xue Z, Novetsky AP, Einstein MH, Marcus
JZ, Befano B, Guo P, Demarco M, Wentzensen N, Long LR, Schiffman M
and Antani S: A demonstration of automated visual evaluation of
cervical images taken with a smartphone camera. Int J Cancer.
147:2416–2423. 2020.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Miyagi Y, Takehara K, Nagayasu Y and
Miyake T: Application of deep learning to the classification of
uterine cervical squamous epithelial lesion from colposcopy images
combined with HPV types. Oncol Lett. 19:1602–1610. 2020.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Tan X, Li K, Zhang J, Wang W, Wu B, Wu J,
Li X and Huang X: Automatic model for cervical cancer screening
based on convolutional neural network: A retrospective,
multicohort, multicenter study. Cancer Cell Int.
21(35)2021.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Salim M, Wåhlin E, Dembrower K, Azavedo E,
Foukakis T, Liu Y, Smith K, Eklund M and Strand F: External
evaluation of 3 commercial artificial intelligence algorithms for
independent assessment of screening mammograms. JAMA Oncol.
6:1581–1588. 2020.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Schaffter T, Buist DSM, Lee CI, Nikulin Y,
Ribli D, Guan Y, Lotter W, Jie Z, Du H, Wang S, et al: Evaluation
of combined artificial intelligence and radiologist assessment to
interpret screening mammograms. JAMA Netw Open.
3(e200265)2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Stuebs FA, Schulmeyer CE, Mehlhorn G, Gass
P, Kehl S, Renner SK, Renner SP, Geppert C, Adler W, Hartmann A, et
al: Accuracy of colposcopy-directed biopsy in detecting early
cervical neoplasia: A retrospective study. Arch Gynecol Obstet.
299:525–532. 2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Fatahi MN, Meybodi NF, Karimi-Zarchi M,
Allahqoli L, Sekhavat L, Gitas G, Rahmani A, Fallahi A, Hassanlouei
B and Alkatout I: Accuracy if triple test versus colposcopy for the
diagnosis of premalignant and malignant cervical lesions. Asian Pac
J Cancer Prev. 21:3501–3507. 2020.PubMed/NCBI View Article : Google Scholar
|