Introduction
At present, cancer is a major cause of death
worldwide; in 2021, there were 19.3 million new cases of cancer and
10 million cancer-associated deaths. Approximately one in five men
and one in six women will develop cancer during their lifetime
(1). Stereotactic body radiation
therapy (SBRT), also known as stereotactic ablative radiotherapy
(SABR), is an option for patients with cancer beyond chemotherapy
or surgery (2). SBRT refers to the
administration of high doses of radiation using several beams of
various intensities aimed at different angles to precisely target
the tumor. SBRT is a noninvasive technique that can deliver high
precision and dose-escalated treatment throughout the body with
excellent rates in local control. In addition, it has been widely
used to treat various types of cancer, including gastrointestinal
malignancies, prostate cancer and recurrent gastric cancer
(3-6).
Although SBRT has been widely used to treat cancer
for a number of years, the prognosis of the treatment is clinically
heterogeneous, characterized by increased local recurrence and
distant metastasis (7,8). Therefore, more effective and accurate
indicators to assist clinicians with patient risk stratification
and clinical therapy are required (9,10).
In recent years, numerous studies have reported that
tumor-associated inflammation and the tumor environment influence
cancer development, progression and metastasis, which has led to
much interest in the association between patient prognosis and
inflammatory hematological markers (11,12).
Among the inflammatory indexes, neutrophil-to-lymphocyte ratio
(NLR) is an emerging biomarker of interest for several types of
malignancy and is readily assessed from a serum complete blood
count (CBC) with differential; notably, increased NLR has been
reported to be associated with poor prognostic indicators,
particularly poor overall survival (OS) in patients with advanced
cancer (13).
Previous studies have shown that the number of
participants included in individual studies is not large and the
results are inconsistent (7,8). In
addition, the association between inflammation-based biomarkers and
oncological outcomes in patients with cancer who undergo SBRT is
unclear. It is well known that patients receiving radiation therapy
may experience a marked decline or a depletion of circulating
lymphocytes (14,15), and a decreased lymphocyte count has
been reported to be associated with a weaker anti-tumor immune
response and a poor prognosis (16,17).
It is therefore of great clinical importance to investigate the
predictive roles of NLR before and after SBRT in patients with
cancer.
The present study aimed to perform a meta-analysis
to quantify the prognostic value of NLR on the outcome of tumors
treated with SBRT. Furthermore, according to existing studies, the
present study determined whether a statistical difference existed
in the prognosis of cancer between pre-SBRT NLR and post-SBRT
NLR.
Materials and methods
Registration number
The present study performed a systematic review and
meta-analysis of the existing literature according to the Preferred
Reporting Items for Systematic Reviews and Meta-Analyses guidelines
(18). The present study was
registered in PROSPERO (registration no. CRD42020186132). All
analyses were based on previously published studies; therefore, no
ethics approval or patient consent were required.
Search strategy
A comprehensive retrieval of articles published
between January 1, 1990 and October 5, 2020 was performed using the
following databases: Embase (https://www.embase.com), PubMed (https://pubmed.ncbi.nlm.nih.gov), The Cochrane
Library (https://www.cochranelibrary.com) and Google Scholar
(https://scholar.google.com). Medical
subject headings and abstract fields were searched combined with
the related key words including ‘NLR’ (e.g., ‘neutrophil to
lymphocyte ratio’ OR ‘NLR’ OR ‘neutrophil-to-lymphocyte ratio’) AND
‘SBRT’ (e.g., ‘stereotactic body radiotherapy’ OR ‘SBRT’ OR
‘stereotactic ablative radiotherapy’ OR ‘SABR’) AND ‘cancer’ (e.g.,
‘cancer’ ‘carcinoma’ and ‘tumor’). No language restriction was
applied.
Study selection
Original assessment was based on the title and
abstract of each reference. Full articles of relevant references
were then reviewed for qualification using the following criteria:
i) Studies involving individuals with solid tumors who underwent
SBRT; ii) the association between NLR and OS was discussed; iii)
baseline levels of NLR were assessed before or after SBRT
treatment; iv) studies providing the hazard ratio (HR) with 95%
confidence interval (CI) for OS (19), or relevant information could be
estimated by Engauge Digitizer (https://markummitchell.github.io/engauge-digitizer/)
to obtain the aforementioned statistics; v) a Newcastle-Ottawa
Scale (NOS) score >5 (20,21).
Case reports, reviews, animal studies, conference proceedings,
letters to editors, abstract only and duplicated studies were
excluded.
Data extraction
All candidate literature was evaluated and extracted
by two independent authors. The two authors assessed all full
articles for eligibility and extracted data using a preset
spreadsheet. Any disagreement was resolved by a third researcher
(LH) or through discussion. The primary endpoint was OS.
Information summarized included: First author, publication year,
research country, age, ethnicity, sample size, follow-up duration,
primary location of the tumor, stage of cancer, method of treatment
and NLR cut-off value. Outcome indicators, and HRs from
multivariate and univariate analyses were preferred.
Data analysis
The present study evaluated the prognostic role of
NLR by pooling the HRs and corresponding 95% CIs for survival
analysis. I², calculated as follows: I² (%)=100 x (Q - df)/Q, where
Q is Cochran's heterogeneity statistic and df is the degrees of
freedom, and P-values were used to identify and quantify the degree
of heterogeneity (22). When I²
was ≥50% or P≤0.05 (significant heterogeneity) (23), random-effects model was used to
combine HRs, otherwise a fixed-effects model was adopted. Subgroup
analysis was used to detect sources of heterogeneity. Publication
bias was assessed by Egger's test and Begg's test (24,25).
Two-sided P<0.05 was considered statistically significant.
Forest plot, Egger's test and Begg's test were conducted using
STATA statistical software (version 12.0; StatCorp LLC). The flow
diagram was generated using GraphPad Prism (version 8.0; GraphPad
Software, Inc.). In addition, quality assessment was performed
using RevMan (version 5.3; Cochrane Collaboration).
Results
Search and selection of studies
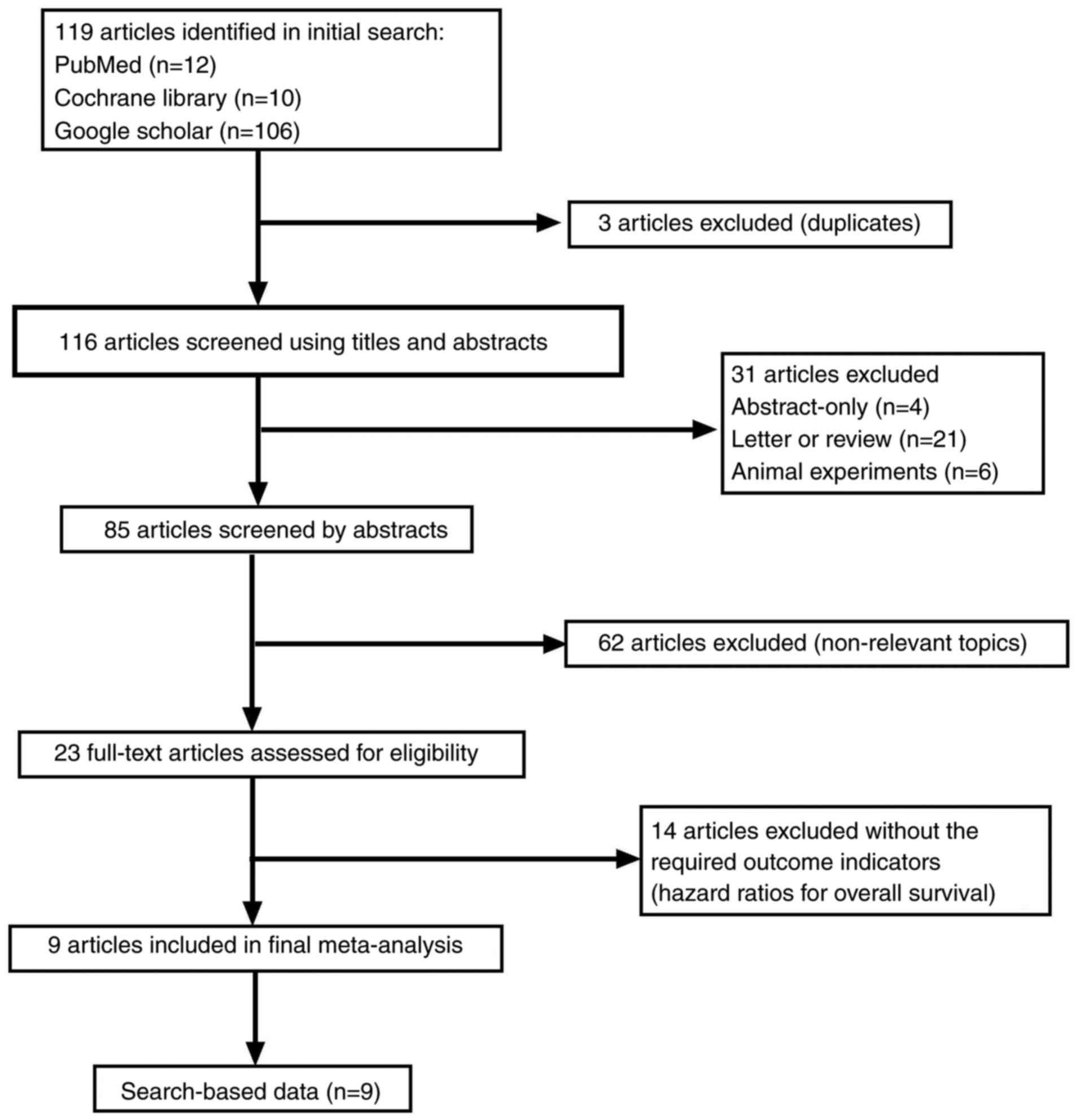
A total of 119 relevant articles were screened
following the initial search. The process of the selection is shown
in Fig. 1. Three of the studies
were duplicated articles and 62 were revealed to be not relevant
after scanning the abstract. A total of 31 studies were removed for
other reasons (four studies were abstracts only; 21 studies were
letters or reviews; and six studies were animal experiments).
Subsequently, 23 full-text articles were assessed for eligibility;
however, 14 articles failed to meet the inclusion criteria.
Finally, nine studies (26-34)
involving 1,010 participants were included for further
assessment.
Study characteristics
Two studies were from China (26,30),
six studies were from USA (27-29,32-34),
and one study was performed in Canada (31). Four of these cohorts enrolled
<100 participants (26,29,30,33)
and five studies recruited >100 patients (27,28,31,32,34).
Four studies investigated non-small cell lung cancer (NSCLC)
(27,28,31,33),
two studies investigated hepatocellular carcinoma (HCC) (26,30),
and the remaining studies investigated pancreatic adenocarcinoma
(34), brain metastases (32) and malignant adrenal lesions
(29). Furthermore, two studies
did not limit the stage of cancer (involved all disease stages)
(26,28), four studies included only
early-stage disease (I/I-II/I-III/II-IIIb) (27,30,31,33)
and three studies included only late-stage disease (III-IV/IIIb-IV)
(29,32,34).
Two studies were prospective design (28,31)
and seven studies were retrospective (26,27,29,30,32-34).
Notably, six studies conducted both multivariate analysis and
univariate analysis (26,28,29,31,32,34).
In these six studies, some variables were used as covariates for
Cox regression multivariate analysis; therefore, their covariates
are listed separately. The characteristics of the included studies
are shown in Table I.
 | Table IMain characteristics of all of the
studies included in the meta-analysis. |
Table I
Main characteristics of all of the
studies included in the meta-analysis.
| First author | Year | Study region | Ethnicity | Number of
participants (M/F) | Median follow-up,
months(range) | Disease type | Stage | Treatment | Median age, years
(range) | NLR cut-off | Outcome | HR | Covariates | (Refs.) |
|---|
| Alagappan | 2018 | USA | Caucasian | 208 (109/99) | 7.5 (4.6-12.0) | Pancreatic
adenocarcinoma | Advanced | Combined | 75.2
(65.9-86.1) | 5 | OS/LR | R (M/U) | Albumin; RBC; prior
chemotherapy (yes) | (34) |
| Cannon | 2015 | USA | Caucasian | 59 (31/28) | 17 | NSCLC | Early | SBRT | 70 (48-89) | 2.98 | OS | R (U) | - | (33) |
| Chowdhary | 2018 | USA | Caucasian | 188 (91/97) | 13.2 | Brain
metastases | Advanced | Combined | NR | 6 | OS | R (M/U) | Active systemic
disease; extracranial metastases; graded prognostic assessment;
targeted therapy post-SRS; immunotherapy post-SRS | (32) |
| Giuliani | 2016 | Canada | Caucasian | 122 (60/62) | 26.9
(1.3-99.3) | NSCLC | Early | SBRT | 76 (48-90) | 3 | OS | R (M/U) | Female sex; tumor
stage T2; hemoglobin | (31) |
| Lai | 2020 | China | Asian | 72 (61/11) | 67.2
(7.7-127.4) | HCC | Early | SBRT | 57 (30-84) | 1.88 | OS | R (M) | - | (30) |
| Mills | 2019 | USA | Caucasian | 27 (12-15) | 8 (1-66) | Malignant adrenal
lesions | Advanced | Combined | 63 (51-78) | 4.1 | OS | R (M/U) | Pretreatment ALC
>1x106/ml | (29) |
| Sebastian | 2019 | USA | Caucasian | 156 (89-67) | 13.4 | NSCLC | All stages | SBRT | 72 (51-92) | 3.6 | OS | R (M/U) | Age; sex; T stage;
histology; ECOG performance status; Charlson's Comorbidity Index;
smoking; BED Gy10 | (28) |
| Shaverdian | 2016 | USA | Caucasian | 118 | 28.9 | NSCLC | Early | SBRT | 76 | 2.18 | DMFS/DSS/OS | R (U) | - | (27) |
| Zhuang | 2019 | China | Asian | 60 (49/11) | 36.9
(4.1-73.5) | HCC | ALL stages | Combined | 61.0±12.8 | 2.7 | PFS/OS | R (M/U) | Presence of
hepatitis; tumor size (≥1.5cm); pre-treatment pre-treatment AFP
(≥20.0 ng/ml); pre-treatment RBC (≥4.5x1012/l);
post-treatment PLR (≥263.0) | (26) |
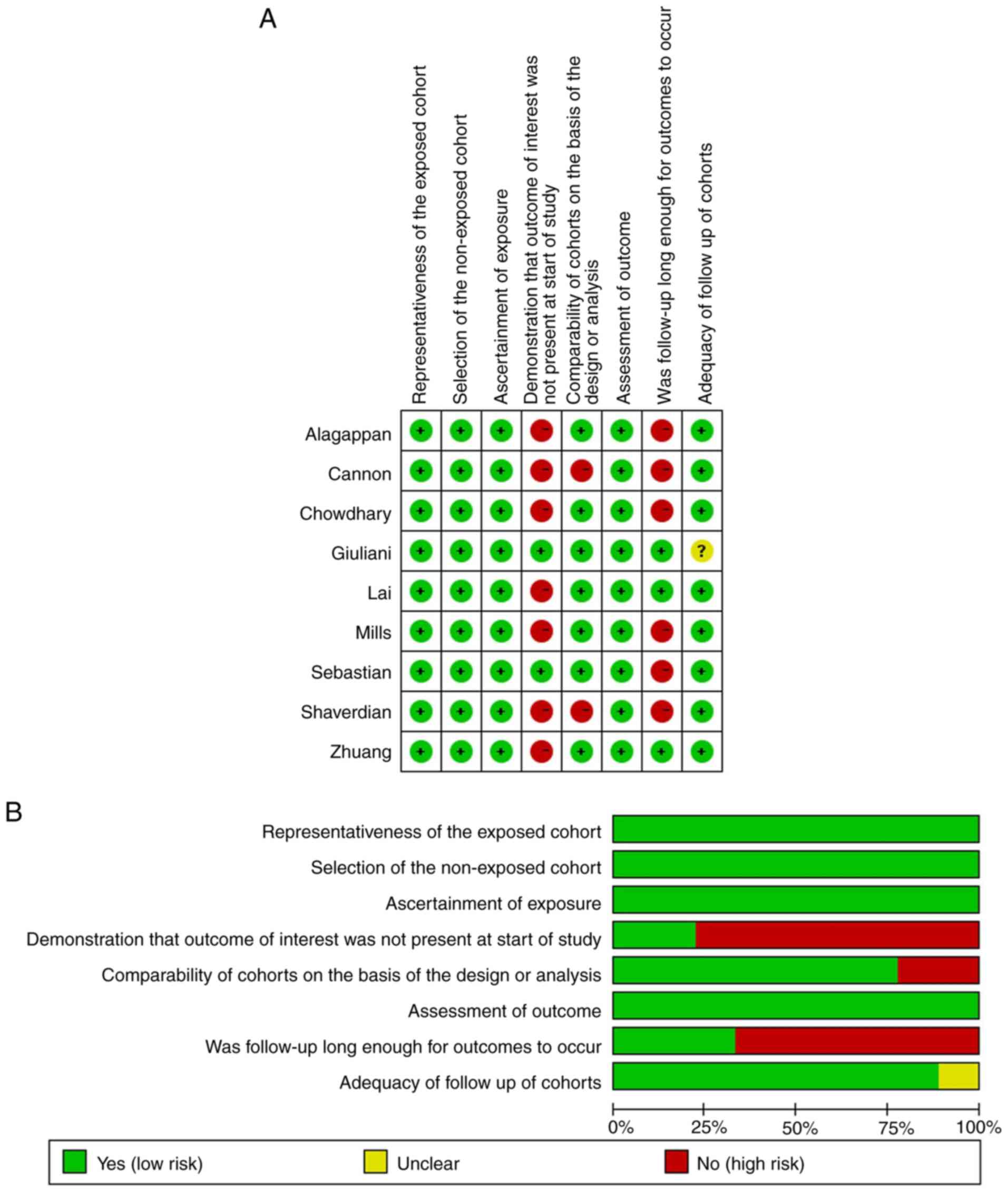
Quality assessment
The NOS was used to assess the quality of each of
the included studies by two independent authors. The NOS consists
of three parts: Selection, comparability and outcome assessment.
For the selection of cohort item, representative exposed groups
were selected for inclusion, and the non-exposed and exposed groups
were from the same population in all studies. Therefore, they were
considered as being at low risk of bias. Only two of the studies
were prospective and seven were retrospective, thus they were
regarded as high risk of bias. As for intergroup comparability,
seven studies applied multivariate analysis, whereas the remaining
were considered as high risk of bias because they only used
univariate analysis. With regard to outcome, all studies had record
linkage. Nevertheless, the follow-ups in only three studies were
long enough for outcomes to occur (median >2 years). Eight
studies had complete follow-ups, only one was vague in details,
which was labelled as unclear risk of bias. When items conform to
NOS, the circle in the figure is green; non-conforming items are
red; and unclear items are yellow (Fig. 2). Studies with ≥5 green circles
were assigned as mid-quality studies and those with ≥6 green
circles were assigned as high-quality studies. All of the studies
assessed in the present study were mid-quality or high-quality.
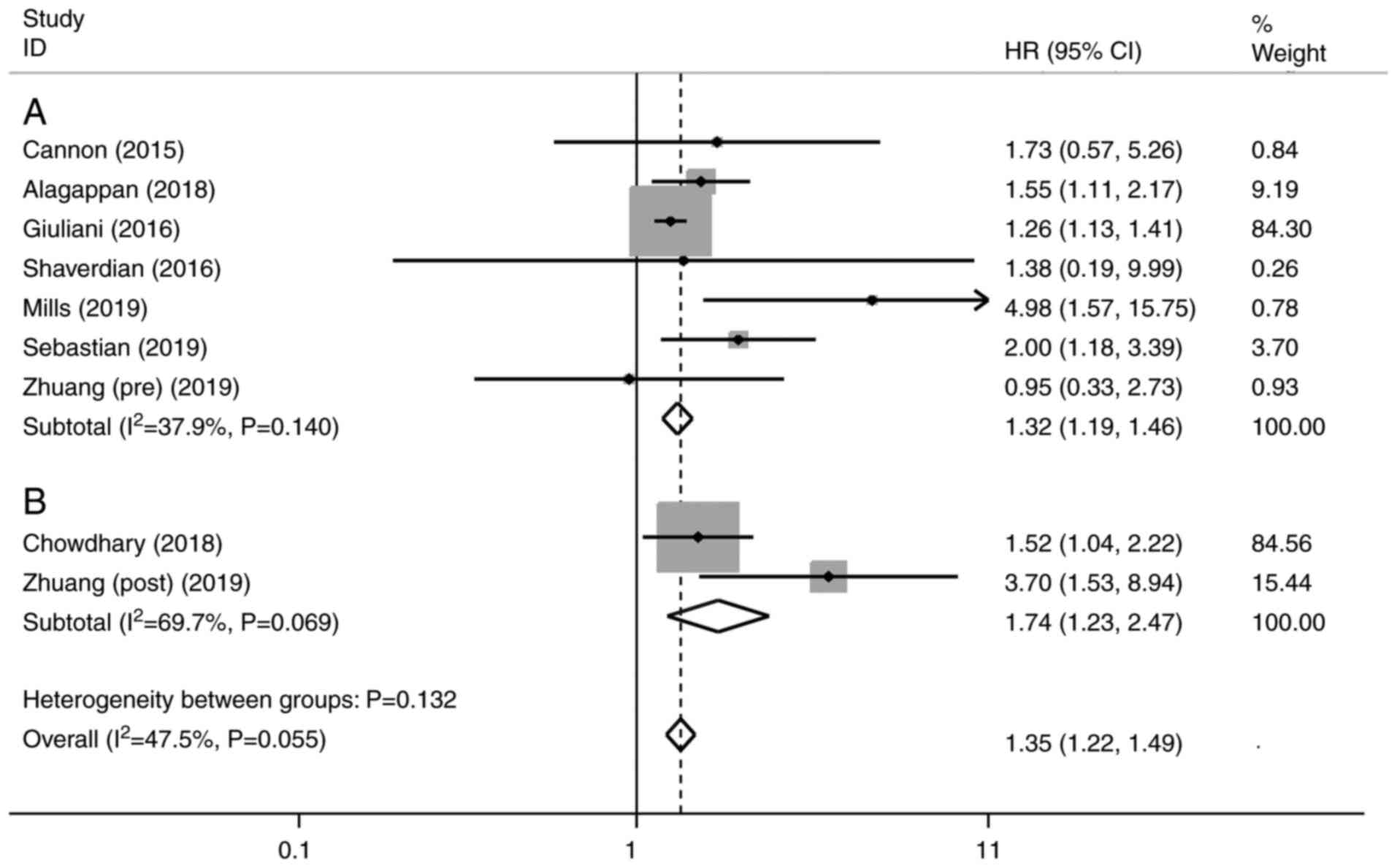
Univariate analysis of NLR and OS
A total of eight studies were included in the
univariate analysis of NLR and OS. Among them, one study evaluated
both pre-treatment and post-treatment NLR (26), one study assessed only
post-treatment NLR (32), and six
studies included only pre-treatment NLR (27-29,31,33,34).
The univariate analysis revealed that elevated NLR predicted a
worse outcome for OS with a combined HR of 1.35 (95% CI, 1.22-1.49,
P<0.001), without significant heterogeneity (I²=47.5%; P=0.055)
(Fig. 3). The subgroup analysis by
pre- or post-SBRT NLR showed that the pooled HRs were 1.32 (95% CI,
1.19-1.46; P<0.001; Fig. 3A)
and 1.74 (95% CI, 1.23-2.47; P<0.005; Fig. 3B), respectively.
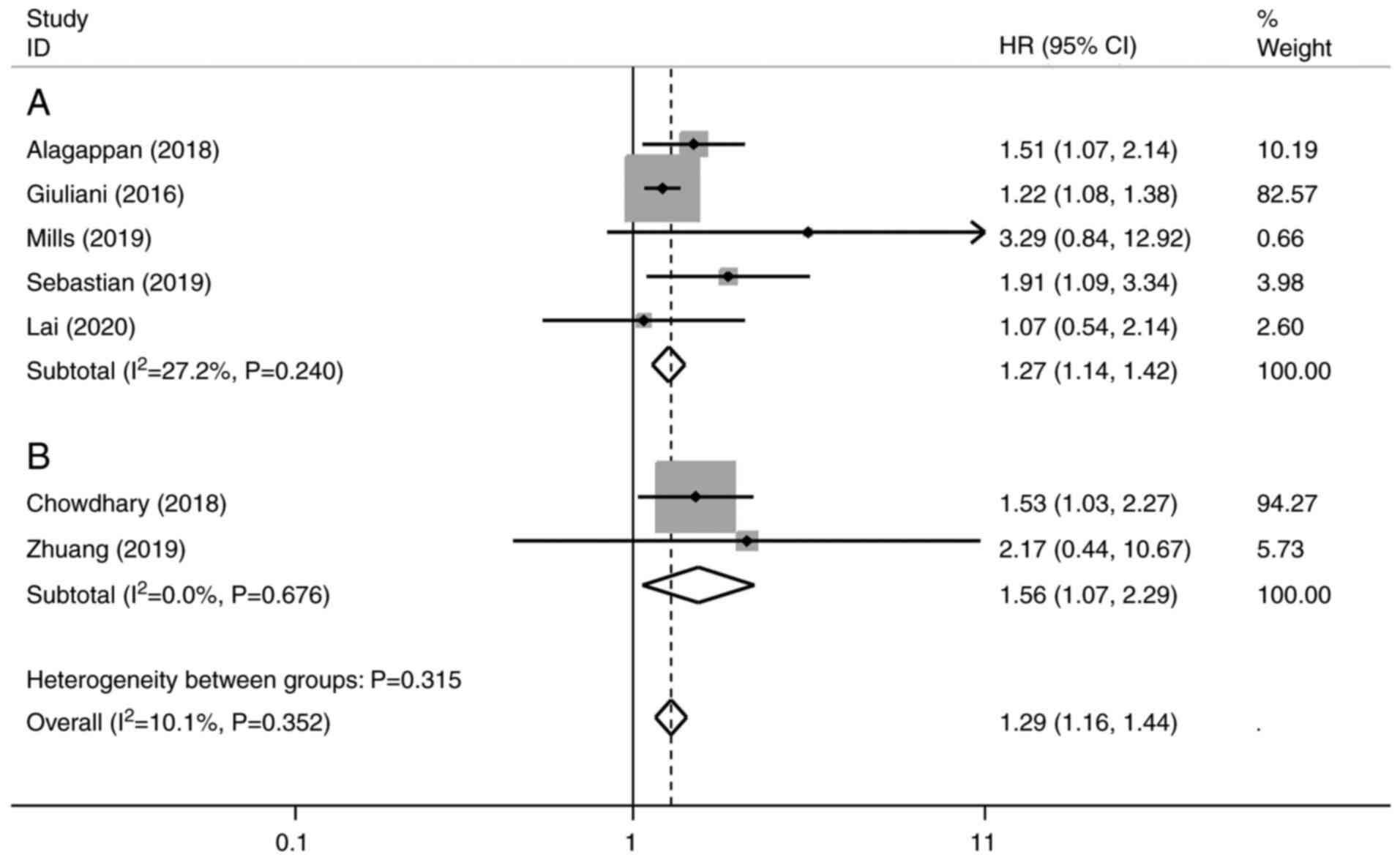
Multivariate analysis of NLR and
OS
In the multivariate analysis, five studies assessed
pre-treatment NLR (28-31,34)
and two studies included post-treatment NLR (26,32).
The results demonstrated that increased NLR was associated with a
poorer OS (HR, 1.29; 95% CI, 1.16-1.44; P<0.001), without
significant heterogeneity (I²=10.1%; P=0.352) (Fig. 4). Subgroup analysis by pre- or
post-SBRT NLR revealed the pooled HR was 1.27 (95% CI, 1.14-1.42;
P<0.001; Fig. 4A) and 1.56 (95%
CI, 1.07-2.29; P<0.005; Fig.
4B).
Subgroup analysis to explore sources
of heterogeneity
Subgroup analysis of univariate analysis was
performed based on the extracted data (Table II). Subgroup analysis of
retrospective or prospective data demonstrated that the pooled HRs
were 1.47 (95% CI, 1.17-1.84) and 1.25 (95% CI, 1.10-1.40),
respectively, and the prospective group showed more significant
heterogeneity (I2=57.7%; P=0.124) than overall
(I2=47.5%). The cut-off values applied in the studies
were not consistent, ranging between 1.88 and 6. Five studies had a
NLR cut-off value of ≤3, whereas four studies had a NLR cut-off
value of >3. Heterogeneity was not detected between cut-off
value ≤3 and cut-off value >3 groups (P=0.051), although the
P-value was close to significance, and the pooled HRs were 1.22
(95% CI, 1.08-1.38) and 1.58 (95% CI, 1.26-1.98), respectively.
| Table IISummary of the subgroup
meta-analysis. |
Table II
Summary of the subgroup
meta-analysis.
| | Heterogeneity |
|---|
| Analysis | N | References | Random-effects
model HR (95% CI) | Fixed-effects model
HR (95% CI) | I², % | P-value | P-value (between
groups) |
|---|
| Subgroup 1: Study
design | | | | | | | 0.210 |
|
Retrospective | 7 | (26,27,29,30,32-34) | 1.47
(1.17-1.84) | 1.47
(1.17-1.84) | 0.00 | 0.817 | |
|
Prospective | 2 | (28,31) | 1.40
(0.93-2.10) | 1.25
(1.10-1.40) | 57.70 | 0.124 | |
| Subgroup 2:
Therapy | | | | | | | 0.158 |
|
SBRT
only | 5 | (27,28,30,31,33) | 1.25
(1.11-1.40) | 1.25
(1.11-1.40) | 0.00 | 0.577 | |
|
Combined | 4 | (26,29,32,34) | 1.52
(1.18-1.95) | 1.52
(1.18-1.95) | 0.00 | 0.575 | |
| Subgroup 3:
Stage | | | | | | | 0.147 |
|
Early | 4 | (27,30,31,33) | 1.22
(1.08-1.38) | 1.22
(1.08-1.38) | 0.00 | 0.914 | |
|
Advanced | 3 | (29,32,34) | 1.56
(1.21-2.02) | 1.56
(1.21-2.02) | 0.00 | 0.553 | |
|
All
stages | 2 | (26,28) | 1.56
(0.84-2.90) | 1.64
(1.00-2.69) | 23.90 | 0.252 | |
| Subgroup 4: Cut-off
value | | | | | | | 0.051 |
|
NLR ≤3 | 5 | (26,27,30,31,33) | 1.22
(1.08-1.38) | 1.22
(1.08-1.38) | 0.00 | 0.914 | |
|
NLR
>3 | 4 | (28,29,32,34) | 1.58
(1.26-1.98) | 1.58
(1.26-1.98) | 0.00 | 0.639 | |
| Subgroup 5: Tumor
location | | | | | | | 0.230 |
|
NSCLC | 4 | (27,28,31,33) | 1.25
(1.11-1.41) | 1.25
(1.11-1.41) | 0.00 | 0.440 | |
|
HCC | 2 | (26,30) | 1.04
(0.58-1.84) | 1.04
(0.58-1.84) | 0.00 | 0.849 | |
|
Others | 3 | (29,32,34) | 1.56
(1.21-2.02) | 1.56
(1.21-2.02) | 0.00 | 0.553 | |
| Subgroup 6:
Ethnicity | | | | | | | 0.447 |
|
Caucasian | 7 | (27-29,31-34) | 1.33
(1.17-1.51) | 1.30
(1.17-1.45) | 4.00 | 0.396 | |
|
Asian | 2 | (26,29) | 1.04
(0.58-1.84) | 1.04
(0.58-1.84) | 0.00 | 0.849 | |
| Subgroup 7: Sample
size | | | | | | | 0.941 |
|
≤100 | 4 | (26,29,30,33) | 1.31
(0.81-2.12) | 1.31
(0.81-2.12) | 0.00 | 0.448 | |
|
>100 | 5 | (27,28,31,32,34) | 1.31
(1.16-1.48) | 1.29
(1.16-1.44) | 4.90 | 0.379 | |
In addition, subgroup analyses were performed
according to treatment methods (treatment by SBRT and combined),
disease stage (early stage, advanced stage and all stages), tumor
type (NSCLC, HCC and others), ethnicity (Caucasian and Asian) and
sample size (≤100 and >100), but no significant differences were
identified.
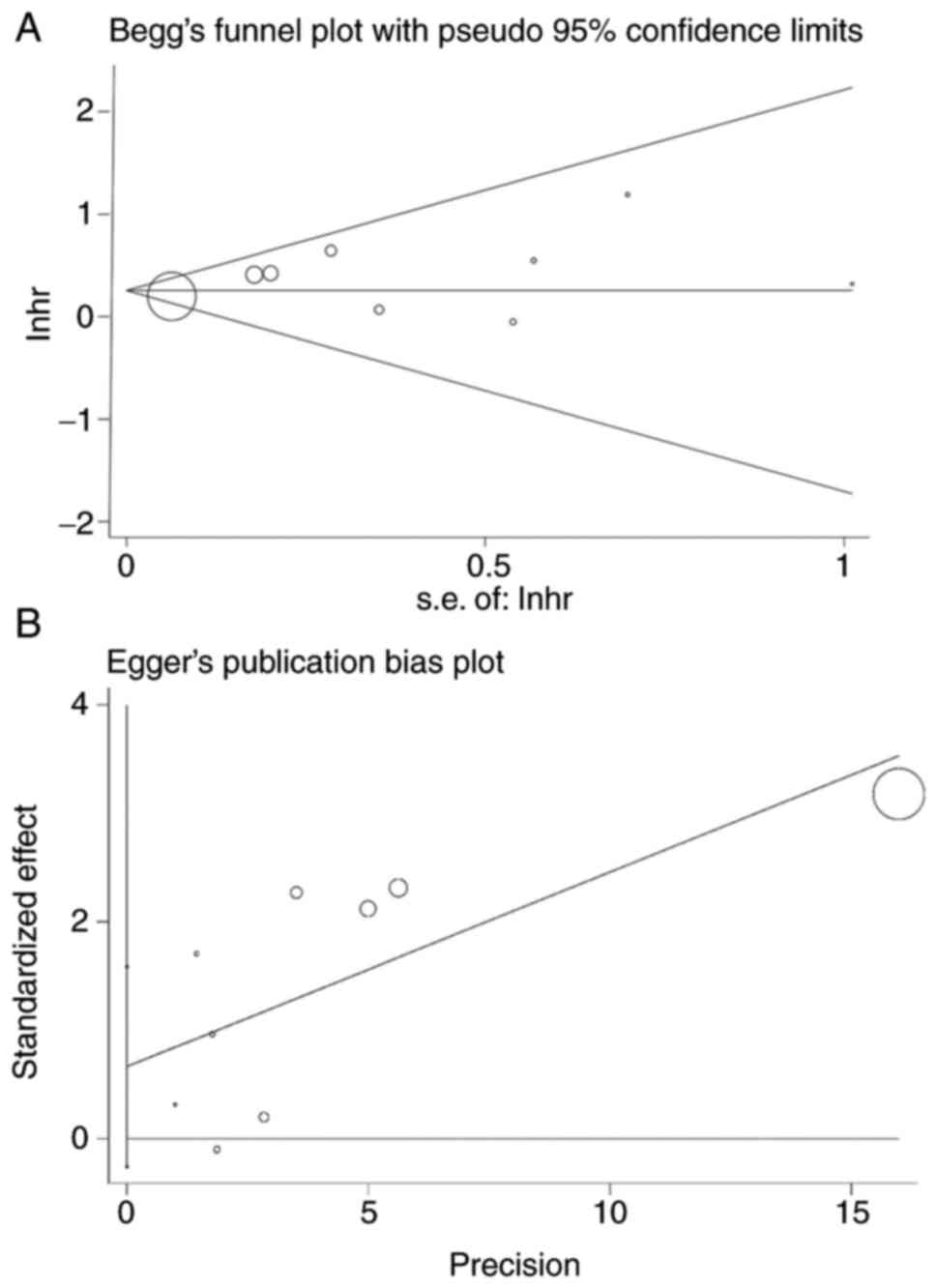
Publication bias
Begg's funnel plot and Egger's linear regression
test were performed to evaluate publication bias. The publication
biases were Pr>|z|=0.917 for Begg's test (Fig. 5A) and P>|t|=0.131 for Egger's
test (Fig. 5B). The size of the
circle indicates the weight of the article. No publication bias was
found.
Discussion
The present meta-analysis demonstrated that elevated
NLR was a significant predictor of poor survival outcomes in
patients that underwent SBRT alone or in combination with
chemotherapy or surgery. The results were consistent in both
univariate and multivariate analyses, thus indicating that NLR may
be an independent predictor for prognosis. Notably, the weights of
Giuliani et al (31) and
Chowdhary et al (32) were
particularly large (>80%), because these studies yielded CIs of
a smaller range and are thus considered more accurate. Subgroup
analyses showed that both elevated pre- and post-treatment NLR
could significantly reduce the survival of patients treated with
SBRT. Meanwhile, post-treatment NLR predicted poorer survival than
pre-treatment. Although there was no significance between pre- and
post-treatment groups, the induction of a leukocyte-predominant
inflammatory response after SBRT may predict a worse prognosis.
Moreover, heterogeneity was not found between cut-off value ≤3 and
cut-off value >3 groups (P=0.051), although the P-value was
close to significance. This may be caused by an insufficient sample
size.
The association of elevated NLR with a worse
prognosis may be based on the immune/inflammatory response.
Inflammation affects all stages of tumorigenesis; not only have
researchers confirmed that inflammation and immunity govern the
development of tumors (35), but
they have also verified the therapeutic value when targeting the
inflammasome for the prevention and treatment of cancer (36). The association between increased
NLR and poor outcome is not yet understood; however, the potential
mechanism may involve the association between NLR and inflammation.
Notably, previous studies have revealed that neutrophils may be
indicative of inflammation, which can induce production of
chemokines and cytokines, and suppress the cytolytic activity of
immune cells, such as activated T cells and natural killer cells
(37,38). Cancer cells together with its host
cells can produce inflammatory cytokines and chemokines that
contribute to malignant progression (39). Neutrophils can produce an
inflammatory response, which may stimulate the change of tumor
microenvironment, thus resulting in the proliferation and
metastasis of cancer cells. In addition, it has been reported that
elevated NLR can lead to elevated tumor growth-promoting factors,
such as TGF-β (40). Furthermore,
inflammatory factors can increase the number of neutrophils and
decrease the number of lymphocytes; in some reports, primary tumor
infiltration was revealed to be positively linked with lymphopenia
(41,42). Other studies have also reported
that tumor-infiltrating lymphocytes (TIL) serve an essential role
in guiding prognosis. Notably, CD3+ TILs have been
reported to exert a positive effect on survival of patients with
breast cancer and the importance of lymphocytes has been
highlighted (43-45).
Formerly regarded as a merely immunosuppressive treatment, pre- and
clinical observations have indicated that radiotherapy can elicit
an immune response against tumors (46,47).
The response was first observed as infrequent abscopal effects
emerged from the phenomenon of tumor remission outside the
radiation field in satellite secondary tumors (48). Elevated lymphocytes and low NLR may
be positive signs of abscopal effects.
There are some limitations in the present study.
Firstly, the number and sample size of the included eligible
studies were small. In addition, two (27,33)
of the HRs and 95% CIs were extracted from Kaplan-Meier survival
curves due to the unavailability of original data using Engauge
Digitizer, which could lead to imprecise risk estimates. Secondly,
among the included studies, only three studies were followed up for
>2 years. Insufficient follow-up may overestimate the survival
and prognosis of patients with cancer in the cohort to some extent.
Thirdly, the NLR cut-off value for the present study was
inconsistent; each study varied from another. The optimal NLR
cut-off value for various tumors needs to be investigated in
further large-scale prospective cohort studies. In addition, it is
well known that SBRT processing has an impact on NLR; however, with
the exception of Sebastian et al (28), the original studies did not provide
the specific measurement time of NLR. Sebastian et al
(28) mentioned that all patients
had an available CBC with differential within 6 months of
completion of treatment. Therefore, we cannot know whether the
post-NLR value given in these studies was obtained after the first
SBRT or measured after all SBRT was completed; this affects the
accuracy of the results to a certain extent. Finally, the
discrepancies between pre- and post-SBRT NLR require further
research; although the present results revealed there was no
statistical significance, this may be caused by insufficient sample
size.
Notably, more well-designed, large-scale studies
with a longer follow-up are required in the future. Furthermore,
further research is needed to clarify the mechanism underlying the
systemic inflammatory response to SBRT based on the change of pre-
and post-SBRT NLR.
In conclusion, both pre- and post-SBRT elevated NLR
may be considered an independent predictor of poor survival in
patients with cancer who received SBRT; the higher level of NLR
predicts a worse outcome. Therefore, NLR may be considered a
promising index for appropriately individualizing SBRT and
assessing prognosis.
Acknowledgements
Not applicable.
Funding
Funding: This work was supported by grants from the China
Postdoctoral Science Foundation (grant no. 2020M682578), the
Science and Technology Innovation Program of Hunan Province (grant
no. 2020RC2061), the Hunan Cancer Hospital Climb Plan (grant no.
YF2020006), the Hunan Cadres Health Care Department (grant no.
NCC2017A17), the Hunan Provincial Health Commission (grant no.
B2019098) and the Chinese National Cancer Center (grant no.
NCC2017A17, No NCC2017L01).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
YY, DT and HL designed the research and extracted
data. CL, ZH and PY performed the statistical analysis, and the
data visualization and interpretation. YY and DT drafted the first
manuscript. HL, PY and ZH made critical revisions to the manuscript
for key intellectual content and reviewed the data analysis. YY and
DT confirm the authenticity of all the raw data. All authors read
and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Miller KD, Fuchs HE and Jemal
A: Cancer statistics, 2021. CA Cancer J Clin. 71:7–33.
2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Timmerman RD, Herman J and Cho LC:
Emergence of stereotactic body radiation therapy and its impact on
current and future clinical practice. J Clin Oncol. 32:2847–2854.
2014.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Tandberg DJ, Tong BC, Ackerson BG and
Kelsey CR: Surgery versus stereotactic body radiation therapy for
stage I non-small cell lung cancer: A comprehensive review. Cancer.
124:667–678. 2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Abdelfatah MM and Gochanour EM: Fiducial
placement for recurrent gastric cancer. Arab J Gastroenterol.
20:56–58. 2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Schaub SK, Hartvigson PE, Lock MI, Hoyer
M, Brunner TB, Cardenes HR, Dawson LA, Kim EY, Mayr NA, Lo SS and
Apisarnthanarax S: Stereotactic body radiation therapy for
hepatocellular carcinoma: Current trends and controversies. Technol
Cancer Res Treat. 17(1533033818790217)2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Palma DA, Olson R, Harrow S, Gaede S,
Louie AV, Haasbeek C, Mulroy L, Lock M, Rodrigues GB, Yaremko BP,
et al: Stereotactic ablative radiotherapy versus standard of care
palliative treatment in patients with oligometastatic cancers
(SABR-COMET): A randomised, phase 2, open-label trial. Lancet.
393:2051–2058. 2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Mathew AS, Atenafu EG, Owen D, Maurino C,
Brade A, Brierley J, Dinniwell R, Kim J, Cho C, Ringash J, et al:
Long term outcomes of stereotactic body radiation therapy for
hepatocellular carcinoma without macrovascular invasion. Eur J
Cancer. 134:41–51. 2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Schonewolf CA, Heskel M, Doucette A,
Singhal S, Frick MA, Xanthopoulos EP, Corradetti MN, Friedberg JS,
Pechet TT, Christodouleas JP, et al: Five-year long-term outcomes
of stereotactic body radiation therapy for operable versus
medically inoperable stage I non-small-cell lung cancer: Analysis
by operability, fractionation regimen, tumor size, and tumor
location. Clin Lung Cancer. 20:e63–e71. 2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Costa-Pinheiro P, Montezuma D, Henrique R
and Jeronimo C: Diagnostic and prognostic epigenetic biomarkers in
cancer. Epigenomics. 7:1003–1015. 2015.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Cai D, Xu Y, Ding R, Qiu K, Zhang R, Wang
H, Huang L, Xie X, Yan H, Deng Y, et al: Extensive serum biomarker
analysis in patients with non-small-cell lung carcinoma. Cytokine.
126(154868)2020.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Grivennikov SI, Greten FR and Karin M:
Immunity, inflammation, and cancer. Cell. 140:883–899.
2010.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Guthrie GJ, Charles KA, Roxburgh CS,
Horgan PG, McMillan DC and Clarke SJ: The systemic
inflammation-based neutrophil-lymphocyte ratio: Experience in
patients with cancer. Crit Rev Oncol Hematol. 88:218–230.
2013.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Mei Z, Shi L, Wang B, Yang J, Xiao Z, Du
P, Wang Q and Yang W: Prognostic role of pretreatment blood
neutrophil-to-lymphocyte ratio in advanced cancer survivors: A
systematic review and meta-analysis of 66 cohort studies. Cancer
Treat Rev. 58:1–13. 2017.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Raben M, Walach N, Galili U and
Schlesinger M: The effect of radiation therapy on lymphocyte
subpopulations in cancer patients. Cancer. 37:1417–1421.
1976.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Ellsworth SG: Field size effects on the
risk and severity of treatment-induced lymphopenia in patients
undergoing radiation therapy for solid tumors. Adv Radiat Oncol.
3:512–519. 2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Venkatesulu BP, Mallick S, Lin SH and
Krishnan S: A systematic review of the influence of
radiation-induced lymphopenia on survival outcomes in solid tumors.
Crit Rev Oncol Hematol. 123:42–51. 2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Maehata Y, Onishi H, Kuriyama K, Aoki S,
Araya M, Saito R, Tominaga L, Oguri M and Araki T: Immune responses
following stereotactic body radiotherapy for stage I primary lung
cancer. Biomed Res Int. 2013(731346)2013.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Moher D, Liberati A, Tetzlaff J and Altman
DG: PRISMA Group. Preferred reporting items for systematic reviews
and meta-analyses: The PRISMA statement. PLoS Med.
6(e1000097)2009.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Hanahan D and Weinberg RA: Hallmarks of
cancer: The next generation. Cell. 144:646–674. 2011.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Zhang Z, Deng C, Ma X and Liu X:
rs10865331 in 2p15 increases susceptibility to ankylosing
spondylitis: A HuGE review and meta-analysis. Clin Exp Rheumatol.
38:993–1000. 2020.PubMed/NCBI
|
|
21
|
Rezapour M, Rezapour HA, Chegeni M and
Khanjani N: Exposure to cadmium and head and neck cancers: A
meta-analysis of observational studies. Rev Environ Health.
36:577–584. 2021.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Higgins JP, Thompson SG, Deeks JJ and
Altman DG: Measuring inconsistency in meta-analyses. BMJ.
327:557–560. 2003.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Higgins JP and Thompson SG: Quantifying
heterogeneity in a meta-analysis. Stat Med. 21:1539–1558.
2002.PubMed/NCBI View
Article : Google Scholar
|
|
24
|
Egger M, Davey Smith G, Schneider M and
Minder C: Bias in meta-analysis detected by a simple, graphical
test. BMJ. 315:629–634. 1997.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Begg CB and Mazumdar M: Operating
characteristics of a rank correlation test for publication bias.
Biometrics. 50:1088–1101. 1994.PubMed/NCBI
|
|
26
|
Zhuang Y, Yuan BY, Hu Y, Chen GW, Zhang L,
Zhao XM, Chen YX and Zeng ZC: Pre/post-treatment dynamic of
inflammatory markers has prognostic value in patients with small
hepatocellular carcinoma managed by stereotactic body radiation
therapy. Cancer Manag Res. 11:10929–10937. 2019.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Shaverdian N, Veruttipong D, Wang J,
Schaue D, Kupelian P and Lee P: Pretreatment immune parameters
predict for overall survival and toxicity in early-stage
non-small-cell lung cancer patients treated with stereotactic body
radiation therapy. Clin Lung Cancer. 17:39–46. 2016.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Sebastian N, Wu T, Bazan J, Driscoll E,
Willers H, Yegya-Raman N, Bond L, Dwivedi A, Mo X, Tan Y, et al:
Pre-treatment neutrophil-lymphocyte ratio is associated with
overall mortality in localized non-small cell lung cancer treated
with stereotactic body radiotherapy. Radiother Oncol. 134:151–157.
2019.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Mills MN, Reddy AV, Richardson L,
Richardson KM and Kersh CR: The prognostic role of pretreatment
neutrophil to lymphocyte ratio (NLR) in malignant adrenal lesions
treated with stereotactic body radiation therapy (SBRT). Am J Clin
Oncol. 42:945–950. 2019.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Lai L, Su T, Liang Z, Lu Y, Hou E, Lian Z,
Gao H and Zhu X: Development and assessment of novel predictive
nomograms based on APRI for hepatitis B Virus-associated small
solitary hepatocellular carcinoma with stereotactic body
radiotherapy. J Cancer. 11:6642–6652. 2020.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Giuliani M, Sampson LR, Wong O, Gay J, Le
LW, Cho BC, Brade A, Sun A, Bezjak A and Hope AJ: Prognostic value
of pretreatment circulating neutrophils, monocytes, and lymphocytes
on outcomes in lung stereotactic body radiotherapy. Curr Oncol.
23:e362–e368. 2016.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Chowdhary M, Switchenko JM, Press RH,
Jhaveri J, Buchwald ZS, Blumenfeld PA, Marwaha G, Diaz A, Wang D,
Abrams RA, et al: Post-treatment neutrophil-to-lymphocyte ratio
predicts for overall survival in brain metastases treated with
stereotactic radiosurgery. J Neurooncol. 139:689–697.
2018.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Cannon NA, Meyer J, Iyengar P, Ahn C,
Westover KD, Choy H and Timmerman R: Neutrophil-lymphocyte and
platelet-lymphocyte ratios as prognostic factors after stereotactic
radiation therapy for early-stage non-small-cell lung cancer. J
Thorac Oncol. 10:280–285. 2015.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Alagappan M, Pollom EL, von Eyben R, Kozak
MM, Aggarwal S, Poultsides GA, Koong AC and Chang DT: Albumin and
neutrophil-lymphocyte ratio (NLR) predict survival in patients with
pancreatic adenocarcinoma treated with SBRT. Am J Clin Oncol.
41:242–247. 2018.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Singh R, Mishra MK and Aggarwal H:
Inflammation, immunity, and cancer. Mediators Inflamm.
2017(6027305)2017.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Karki R, Man SM and Kanneganti TD:
Inflammasomes and cancer. Cancer Immunol Res. 5:94–99.
2017.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Petrie HT, Klassen LW and Kay HD:
Inhibition of human cytotoxic T lymphocyte activity in vitro by
autologous peripheral blood granulocytes. J Immunol. 134:230–234.
1985.PubMed/NCBI
|
|
38
|
el-Hag A and Clark RA: Immunosuppression
by activated human neutrophils. Dependence on the myeloperoxidase
system. J Immunol. 139:2406–2413. 1987.PubMed/NCBI
|
|
39
|
Balkwill F and Mantovani A: Inflammation
and cancer: Back to virchow? Lancet. 357:539–545. 2001.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Yuksel OH, Verit A, Sahin A, Urkmez A and
Uruc F: White blood cell counts and neutrophil to lymphocyte ratio
in the diagnosis of testicular cancer: A simple secondary serum
tumor marker. Int Braz J Urol. 42:53–59. 2016.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Nakamura Y, Watanabe R, Katagiri M, Saida
Y, Katada N, Watanabe M, Okamoto Y, Asai K, Enomoto T, Kiribayashi
T and Kusachi S: Neutrophil/lymphocyte ratio has a prognostic value
for patients with terminal cancer. World J Surg Oncol.
14(148)2016.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Takahashi Y, Horio H, Hato T, Harada M,
Matsutani N, Morita S and Kawamura M: Prognostic significance of
preoperative neutrophil-lymphocyte ratios in patients with stage I
non-small cell lung cancer after complete resection. Ann Surg Oncol
22 Suppl. 3:S1324–S1331. 2015.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Denkert C, Loibl S, Noske A, Roller M,
Muller BM, Komor M, Budczies J, Darb-Esfahani S, Kronenwett R,
Hanusch C, et al: Tumor-associated lymphocytes as an independent
predictor of response to neoadjuvant chemotherapy in breast cancer.
J Clin Oncol. 28:105–113. 2010.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Gooden MJ, de Bock GH, Leffers N, Daemen T
and Nijman HW: The prognostic influence of tumour-infiltrating
lymphocytes in cancer: A systematic review with meta-analysis. Br J
Cancer. 105:93–103. 2011.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Stanton SE and Disis ML: Clinical
significance of tumor-infiltrating lymphocytes in breast cancer. J
Immunother Cancer. 4(59)2016.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Boustani J, Grapin M, Laurent PA, Apetoh L
and Mirjolet C: The 6th R of radiobiology: Reactivation of
anti-tumor immune response. Cancers (Basel). 11(860)2019.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Arnold KM, Flynn NJ, Raben A, Romak L, Yu
Y, Dicker AP, Mourtada F and Sims-Mourtada J: The impact of
radiation on the tumor microenvironment: Effect of dose and
fractionation schedules. Cancer Growth Metastasis.
11(1179064418761639)2018.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Demaria S, Ng B, Devitt ML, Babb JS,
Kawashima N, Liebes L and Formenti SC: Ionizing radiation
inhibition of distant untreated tumors (abscopal effect) is immune
mediated. Int J Radiat Oncol Biol Phys. 58:862–870. 2004.PubMed/NCBI View Article : Google Scholar
|