Introduction
Gastric cancer (GC) is the fifth most frequently
diagnosed type of malignancy and the fourth cause of cancer death
worldwide; in 2020, 1,09 million new cases were diagnosed and
769,000 deaths were attributed to this tumor type (1). GC is a highly heterogeneous disease
displaying genetic and molecular alterations (2) with a median overall survival of ≤12
months for advanced stage (3). The
most common site of metastasis is the liver, followed by the lungs,
bone, and the peritoneum (4,5).
Multidiscipline management is the treatment of choice in GC while
surgical resection enhanced by standardized lymphadenectomy remains
the gold standard towards GC therapy (6,7).
According to the World Health Organization, GC can
be classified as adenocarcinoma, signet ring-cell carcinoma (SRCC),
and undifferentiated carcinoma (7). Despite that currently the overall
prevalence has decreased (7), a
number of studies indicate that the incidence of the SRCC subtype
has been constantly increasing (8,9).
Furthermore, SRCC seems to demonstrate a pattern of specific
signatures that may be associated with poor response to systematic
treatment; for example, it exhibits less chemosensitivity to the
‘traditional’ therapy regimens (i.e. epirubicin, cisplatin, and
fluorouracil), whereas it appears to have greater sensitivity to
taxane-based chemotherapy (10).
Poor prognosis may also be attributed to the fact that most
patients present quite late in the course of the disease when
progression may already be present (11).
The exact underlying mechanisms for the development
of GC remain not well understood. Some reports in the existing
literature implicate i) alterations in immune function or an
underlying immunodeficiency, ii) the presence of pathogens, iii)
molecular biological abnormalities and iv) genetic predisposition
(2,12-14).
Moreover, several risk factors have been described such as alcohol
intake and obesity, whereas approximately 70% of GC cases have been
correlated with H. pylori infection (13). Positive correlations between
Epstein-Barr virus (EBV) infection and gastric carcinoma have also
been reported (14). In addition,
genetic disorders (i.e. familial adenomatous polyposis and
hereditary nonpolyposis colorectal cancer) have been also linked
with gastric tumorigenesis (2).
Finally, the treatment of a primary gastric lymphoma has been also
associated with increased risk for developing gastric
adenocarcinomas (15).
Cutaneous metastases develop in 0.7-9% of patients
with internal cancers. The most common primary site is the breast,
followed by the lung and colon (5). Skin metastases originating from
systemic cancer typically present as nodular, nontender, firm,
erythematous or pigmented lesions, with increased vascularity or
ulceration (16). Less frequently,
they appear like cellulitis, erysipelas (carcinoma erysipeloides)
or other unusual morphologies (17). Skin metastasis from GC rarely
occurs with an incidence of approximately 0.8-1.0%. In this
article, we describe an interesting and rare case of an extensive
skin rash masquerading as erysipelas which was eventually
identified as gastric cancer metastases. The patient gave fully
informed written consent to the publication of this report and any
accompanying images.
Case report
Α 42-year old man presented to a general hospital
(Elpis Hospital, Athens, Greece; November 2018) because of several
abnormally enlarged left cervical and supraclavicular lymph nodes
(LNs). The patient had also a two-month history of dyspepsia and
gastroesophageal reflux. He was a 30 pack-year smoker
(approximately one and a half pack daily) and had a previous
medical history of two ischemic strokes. His father was diagnosed
and died from gastric cancer at the age of 50. The FNA (November
2018) was positive for metastatic involvement of the examined lymph
node from a low-grade carcinoma of unknown origin. The
esophagogastroduodenoscopy revealed a crater-like, circular lesion
in the prepyloric antrum, with an ulcer of about 10 mm in diameter;
the lesion was bleeding, while it caused stenosis in antrum and
pylorus; extensive gastritis was also confirmed in the stomach
corpus and fundus. Microscopic examination revealed a poorly
differentiated adenocarcinoma with multiple signet ring cells; H.
pylori test was negative. Subsequently, the patient was referred to
our hospital for further treatment (General Oncology Hospital of
Kifissia ‘Agioi Anargiroi’, Athens, Greece; December 2018).
CT and MRI scans revealed a 38 mm lesion in the
pylorus, the presence of a lymph node block [diameter (d)=30 mm] by
the aorta and multiple LNs in the left perihepatic space (d=22 mm).
Ascites, liver metastasis or peritoneal carcinomatosis were not
confirmed. Moreover, thrombosis of the left subclavian vein,
enlarged left cervical (d=20 mm) and supraclavicular LNs (d=13 mm)
were reported. The tumor was characterized inoperable at that time
and capecitabine-oxaliplatin chemotherapy (XELOX regimen) was
initiated (December 2018). The treatment effects were classified as
partial response according to Response Evaluation Criteria in Solid
Tumors version 1.1 and the patient received six cycles of XELOX.
However, in April 2019 the patient developed subcutaneous oedema in
the left ambit, sub- and supraclavicular space, as well as multiple
palpable LNs and oedema in the left cervical space (lymphoedema);
paclitaxel-ramucirumab were administered due to disease
progression; he received a total of nine cycles.
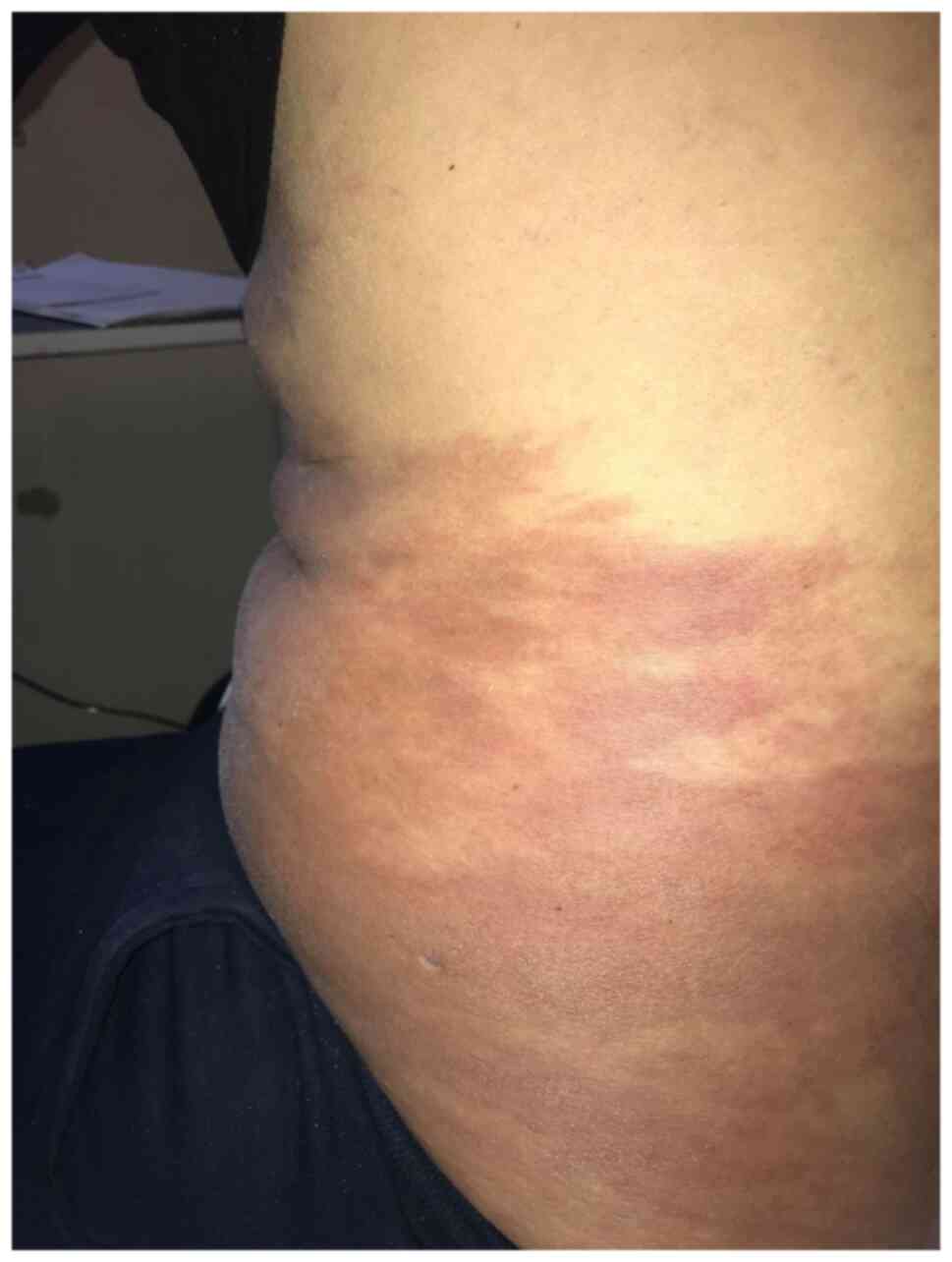
In January 2020, the patient presented with an
extensive rash in his left hemithorax, abdomen and back (especially
on the left) accompanied by mild pruritus and low fever (Fig. 1). On examination, the rash was hard
but painless in palpation with large erythematous plaques but no
skin ulceration; it was initially considered as erysipelas, but it
did not respond to pharmaceutical therapy with antibiotics,
corticosteroids and antihistamines (Fig. 2). The patient also developed
ascites, and thrombosis of the external iliac and femoral vein,
whereas the subcutaneous oedema was constantly deteriorating. Two
weeks later, there was no clinical improvement, and a skin biopsy
was obtained and confirmed the diagnosis of a low-grade carcinoma,
consistent with metastasis from the known gastric cancer [AE1/3(+),
CDX-2(+), CK20(-), CK7(+), and HER2(-)]. The treatment regimen
switched to 5-FU, irinotecan and folinic acid (FOLFIRI), and the
patient's rash decreased in size after three cycles; nonetheless,
the patient suffered from disease deterioration with lung
metastases, pleural effusion (chylothorax), respiratory failure and
eventually died four months after the diagnosis of the skin
metastasis.
Discussion
According to previous observations, poorly
differentiated adenocarcinoma with signet-ring cell features can be
linked with the development of skin metastases. The pathogenesis of
cutaneous metastasis remains unclear. Some potential mechanisms
that have been implicated are i) hematogenous or lymphatic spread,
ii) direct invasion of gastric cancer (consistent with the most
frequent sites of cutaneous metastases), and iii) intraoperative
implantation of cancer cells into the skin (surgical scars are also
quite common sites due to iatrogenic implantation) (5). Regarding our patient, the first two
mechanisms seem most relevant.
Between 2013-2020, according to Şahin et al,
only ten cases have been reported in Pubmed database. The most
common metastatic sites include the neck, the back, the abdomen,
and the inguinal region; the lesions may evolve as single or
multiple nodules with an erysipelas-like morphology (also confirmed
in our patient). Gender-wise, men have been suggested to have a
higher risk for developing skin metastases (18).
In cases of cutaneous metastasis originating from
primary gastric cancer, the prognosis is poor. In six out of the
ten described case reports, the survival time after diagnosis of
skin metastases was reported to be between 1-16 months (18). Treatment plans vary depending on
the extent of the cutaneous lesions and the systemic disease, as
well as the performance status of the patient; they usually include
local excision, irradiation, or systemic chemotherapy. To conclude,
better prognosis has been associated with patients with a
completely resectable cutaneous metastasis in the setting of a good
primary tumor control (16).
Although uncommon, a skin lesion either upon
diagnosis or during the course of the disease, should always raise
suspicion for metastasis and a biopsy specimen should be obtained
as soon as possible for further evaluation. In any case, a
multidisciplinary approach and close collaboration between medical
oncologists and dermatologists are of great significance.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
Data sharing is not applicable to this article, as
no datasets were generated or analyzed during the current
study.
Authors' contributions
EP conceptualized the present case report; EP, DIL,
DN and GA designed the case report; EP and DIL wrote the initial
draft; EP, DIL, DN and GA collected clinical data; EP, DIL, DN and
GA wrote, reviewed and edited the final draft. All authors read and
approved the final manuscript. EP, DIL, DN and GA confirm the
authenticity of all the raw data.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The patient gave fully informed written consent for
the publication of the present case report and accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249.
2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Gigek CO, Calcagno DQ, Rasmussen LT,
Santos LC, Leal MF, Wisnieski F, Burbano RR, Lourenço LG,
Lopes-Filho GJ and Smith MAC: Genetic variants in gastric cancer:
Risks and clinical implications. Exp Mol Pathol. 103:101–111.
2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2019. CA Cancer J Clin. 69:7–34. 2019.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Fukui Y, Kubo N, Sakurai K, Tamamori Y,
Maeda K and Ohira M: Metachronous port site, muscular and
subcutaneous metastases from a gastric adenocarcinoma: A case
report and review of articles. Surg Case Rep. 7(124)2021.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Hu SC, Chen GS, Wu CS, Chai CY, Chen WT
and Lan CC: Rates of cutaneous metastases from different internal
malignancies: Experience from a Taiwanese medical center. J Am Acad
Dermatol. 60:379–387. 2009.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Panda SK, Sahoo PK, Agarwala SK, Houghton
TT, Chandrapattan PP, Sankar KV and Nag R: Evolution of treatment
in gastric cancer-a systematic review. J Egypt Natl Canc Inst.
34(12)2022.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Sitarz R, Skierucha M, Mielko J, Offerhaus
GJA, Maciejewski R and Polkowski WP: Gastric cancer: Epidemiology,
prevention, classification, and treatment. Cancer Manag Res.
10:239–248. 2018.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Bamboat ZM, Tang LH, Vinuela E, Kuk D,
Gonen M, Shah MA, Brennan MF, Coit DG and Strong VE:
Stage-stratified prognosis of signet ring cell histology in
patients undergoing curative resection for gastric adenocarcinoma.
Ann Surg Oncol. 21:1678–1685. 2014.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Taghavi S, Jayarajan SN, Davey A and
Willis AI: Prognostic significance of signet ring gastric cancer. J
Clin Oncol. 30:3493–3498. 2012.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Machlowska J, Pucułek M, Sitarz M,
Terlecki P, Maciejewski R and Sitarz R: State of the art for
gastric signet ring cell carcinoma: From classification, prognosis,
and genomic characteristics to specified treatments. Cancer Manag
Res. 11:2151–2161. 2019.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Orditura M, Galizia G, Sforza V,
Gambardella V, Fabozzi A, Laterza MM, Andreozzi F, Ventriglia J,
Savastano B, Mabilia A, et al: Treatment of gastric cancer. World J
Gastroenterol. 20:1635–1649. 2014.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Shi J, Qu YP and Hou P: Pathogenetic
mechanisms in gastric cancer. World J Gastroenterol.
20:13804–13819. 2014.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Testerman TL and Morris J: Beyond the
stomach: An updated view of Helicobacter pylori pathogenesis,
diagnosis, and treatment. World J Gastroenterol. 20:12781–12808.
2014.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Tavakoli A, Monavari SH, Solaymani
Mohammadi F, Kiani SJ, Armat S and Farahmand M: Association between
Epstein-Barr virus infection and gastric cancer: A systematic
review and meta-analysis. BMC Cancer. 20(493)2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Inaba K, Kushima R, Murakami N, Kuroda Y,
Harada K, Kitaguchi M, Yoshio K, Sekii S, Takahashi K, Morota M, et
al: Increased risk of gastric adenocarcinoma after treatment of
primary gastric diffuse large B-cell lymphoma. BMC cancer.
13(499)2013.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Koyama R, Maeda Y, Minagawa N, Shinohara T
and Hamada T: Late cutaneous metastasis originating from gastric
cancer with synchronous metastasis. Case Rep Gastroenterol.
13:95–101. 2019.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Acikalin MF, Vardareli EN, Saricam T and
Urer S: Erysipelas-like cutaneous metastasis from gastric signet
ring cell carcinoma. J Eur Acad Dermatol Venereol. 19:642–643.
2005.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Şahin M, Ekinci F, Çelik C, Temiz P,
Erdoğan AP and Göksel G: A Rare case report of skin metastasis in
gastric cancer. J Gastrointest Cancer. 52:1156–1158.
2021.PubMed/NCBI View Article : Google Scholar
|