Introduction
Modern therapies in childhood acute lymphoblastic
leukemia (ALL) increased cure rate to more than 80% (1). There are many potential reasons for
this contemporary breakthrough. It has been attributed to the
introduction of new chemotherapeutic agents, enhanced supportive
care and risk-adapted therapy (1,2). As
survival rates have significantly increased, more emphasis has been
paid on the long-term side effects of the ALL treatment. Both
chemotherapy and radiotherapy cause damage to the central nervous
system. It should be remembered that brain is protected by
blood-brain barrier. To obtain propter drugs concentrations in the
CNS high doses of drugs penetrating to it has to be given together
with intrathecal chemotherapy. Both causes brain damage. It was
also proved that radiotherapy is the main reason for tissue damage
(3).
As shown repeatedly, ALL therapeutic protocols cause
changes in the central nervous system. Undoubtedly, white matter
disturbances induced by demyelination and vascular abnormalities
play a role in cognitive impairment caused by radiotherapy
(4). In turn, there is a
significant gap in the knowledge of central nervous system-related
chemotherapy toxicity. Direct destructive effects on cerebral
endothelial cells, brain white matter, blood flow and glucose
metabolism as well as modification of immunological mechanisms
might be involved in the development of central nervous system
damage (5-7).
The above-described changes may contribute to the development of
cognitive impairment in ALL survivors.
In the complex neurologic assessment evoked
potentials (EP) take an important place. They are the response of
brain cortex or other part of central nervous system to stimulation
and appear in a close temporal relationship with the stimulus used
for stimulation. Depending on the time of occurrence of the
response to the stimulus (latency), EP is divided into exo- and
endogenous. Endogenous potentials (also called cognitive potentials
or cognitive event-induced potentials) are the result of changes in
electrical voltage associated with information processing. They do
not directly depend on the type of stimulus, but on the processes
of thinking. The P300 potential is defined as the positive highest
wave deflection, recorded in the leads from the central-parietal
region and appearing in 250-700 msec from the action of an acoustic
or visual stimulus. The biggest advantages of these
neurophysiological techniques include their high sensitivity,
non-invasiveness and the possibility of multiple repetition at a
relatively low cost. It can be compared to common biochemical
markers in oncology like LDH (8).
The aim of our study was to assess the value of
screening of subtle P300 event-related potentials changes in
childhood ALL survivors as well as to compare the observed changes
in irradiated and non-irradiated groups of patients.
Materials and methods
Study groups and treatment
protocols
A group of consecutive 136 patients, 66 males
(48.5%), aged 4.9 to 27.9 (average 13.5±5.3) years who have
completed ALL therapy, were included in the study. The psychomotor
development at the beginning of the treatment and follow-up of all
included patients was compliant with calendar age and all patients
carried out their school duty in an undisturbed manner or they
worked and were fully independent after completing their education.
Moreover, no symptoms of central nervous system focal injury were
found in any patient in the studied and control groups during the
clinical evaluation. No preliminary psychological or
neurophysiological tests were performed before starting treatment.
The study group was divided in 3 subgroups according to treatment
protocols introduced gradually by Polish Leukemia/Lymphoma Study
Group. Applied modifications of treatment protocols were previously
published (9). ALL therapy was
conducted according to modified New York (NY) (30 patients, 17
males, 56.7%) and subsequent revisions of modified
Berlin-Frankfurt-Münster (BFM) (106 patients, 49 males, 46.2%)
regimens. Patients treated with BFM protocols were divided into two
further groups. 32 children (14 males, 43.8%, 18 females, 66,2%)
were treated with previous modified BFM (pBFM) protocols (BFM 81,
83, 86 and 87) in which, as in the NY program, prophylactic and/or
therapeutic central nervous system radiotherapy in addition to
chemotherapy was used. In turn, 74 children (35 males, 47.3%, 39
females, 52,7%) were treated with the BFM95 protocol without
radiotherapy. Two of these children also received a second-line
chemotherapy due to recurrence of the disease. Central nervous
system involvement was found in 7 children, including single
patients treated with NY and BFM95 and 5 patients treated with
pBFM. None of the analyzed patients underwent allogeneic
hematopoietic stem cell transplantation.
Cumulative doses of vincristine in NY programs
amounted 26 to 89 mg/m2 (60.8 mg/m2 on
average) and 30 mg/m2 in BFM programs. In two children
with recurrent disease the cumulative dose of vincristine was 35
mg/m2. The radiotherapy dose in pBFM group was 13-36.4
Gy (mean 18.4 Gy), while in the group treated with NY programs
-18.2-24 Gy (mean 18.3 Gy).
The study group was a part of the total historical
group of ALL patients composed of 559 children (all patients with
ALL treated in studied period). It included 74 NY, 384 pBFM and 91
BFM95 patients.
The control group consisted of 58 patients, 34 males
(58.6%), aged 6-17 years (mean 12.2±3.3 years), who were
hospitalized after a single syncope episode (n=29) and healthy
subjects (n=29) who volunteered for consultation and consented to
the examination. All patients in the control group were completely
asymptomatic in everyday functioning and in neurological
examination.
Methodology of P300 event-related
potentials analysis
The auditory evoked P300 potential was performed in
accordance with the recommendations of the International Federation
of Clinical Neurophysiology (IFCN) (10). In the study, a method of acoustic
stimulation with two contrasting stimuli was used. Each time 60
responses to stimuli different from the background were averaged.
Responses were recorded with surface cup electrodes located in the
frontal (Fz), central (Cz) and parietal (Pz) zones. The reference
electrodes were placed on the earlobes. Each patient underwent
three procedures for averaging distinctive stimuli. The attention
of the patients was controlled by pressing the counter at the
moment of the appearance of the stimulus. To exclude the influence
of body temperature on the conduction speed, the temperature was
measured with a validated surface thermometer in each patient. To
avoid the impact of emotional factors on the course of the study
and the obtained results, all measurements were made in a quiet
shaded room after a thorough explanation of the purpose and course
of the study. In addition, none of the patients had been treated
pharmacologically for at least 1 week prior to P300 potentials
assessment.
According to the IFCN recommendations, the P300
potential was assumed as the positive wave with the highest
amplitude recorded in the Pz lead, which appeared in the range of
280-500 msec. The latency, amplitude of the P300 wave and response
time were evaluated in detail. Prolongation of the latency and the
reaction time of the P300 wave above 2SD and a decrease in the
amplitude below 1SD from the mean value were assumed as abnormal.
To evaluate the effect of treatment, comparisons of ALL patients
(NY, pBFM, BFM95) were made with the control group. In turn, to
assess the impact of radiotherapy on the obtained P300 parameters,
the NY + pBFM group was isolated and compared with the
non-irradiated group (BFM95).
The study protocol complied with the Declaration of
Helsinki and was approved by the Jagiellonian University Medical
College Ethics Committee (Consent No. KBET/131/B/207). All parents
and patients above 16 years old signed written informed consent
before inclusion in the study.
Statistical analysis
Statistical analyses were performed with Statistica
12.0 (StatSoft, Statistica 12.0, Tulsa, Oklahoma, USA) software.
Continuous variables are expressed as mean ± standard deviation and
categorical variables as number (percentage). Continuous variables
were first checked for normal distribution by the Shapiro-Wilk
statistic. Differences among two groups were compared by unpaired
Student's t-test when normally distributed or by the Mann-Whitney
test with test for non-normally distributed variables. In turn,
differences among multiple groups were compared by one-way ANOVA
test followed by Scheffe test when normally distributed or by the
Kruskal-Wallis test followed by Dunn's post-hoc test for multiple
comparisons for non-normally distributed variables. Categorical
variables were analyzed by the χ2 test and Fisher's
exact test depending on the size of the analyzed groups. P<0.05
was considered statistically significant. Due to similar age and
gender distribution in the patient and control groups, no
additional statistical analysis of those parameters was
performed.
Results
Analysis of study groups
Mean age of children at the time of starting
treatment was 5.1±3.2 years. In turn, mean age at the time of
screening for cognitive disorders was 13.5±5.3 years. The time that
elapsed from the completion of treatment to performed screening
ranged from 1.5 to 21.8 years.
Mean age of starting treatment in NY group was
6.5±4.5 years and mean control age -14.0±5.6 (Table I). Children treated with pBFM
developed ALL at younger age (4.4±3.1 years) and were controlled at
older age (18.3±4.0 years). In this group, the average time from
onset of the disease to control was therefore the longest. In turn,
the difference between the average age of ALL onset (4.9±2.5 years)
and the average age of control (11.2±4.0 years) was the shortest in
the BFM95 group. However, the statistical analysis did not show any
significant differences in the mean age of ALL onset. In turn, the
mean age of cognitive control was significantly different
(P<0.001). Intergroup differences were shown between particular
treatment regimens as well as in their direct comparisons with the
control group (Table I).
 | Table IComparison of P300 potential
parameters among the individual protocols and the control
group. |
Table I
Comparison of P300 potential
parameters among the individual protocols and the control
group.
| Characteristic | NY (n=30) | pBFM (n=32) | BFM95 (n=74) | Control group
(n=58) | P-value |
|---|
| Starting treatment,
years | 6.5±4.5 | 4.4±3.1 | 4.9±2.5 | - | 0.120 |
| Mean age, years | 14.0±5.6 | 18.3±4.0 | 11.2±4.0 | 12.2±3.3 |
<0.001a |
| Total sum of
abnormalities | 10 (33.33%) | 5 (15.63%) | 21 (28.38%) | - | 0.247 |
| Prolonged P300
latency | 1 (3.33%) | 0 | 4 (5.41%) | - | 0.522 |
| Decreased P300
amplitude | 0 | 0 | 0 | - | - |
| Prolonged reaction
time | 10 (33.33%) | 3 (15.63%) | 16 (21.62%) | - | 0.007b |
| P300 latency,
msec | 329.13±28.07 | 332.97±23.97 | 331.47±31.05 | 298.14±41.57 |
<0.001c |
| P300 amplitude,
mV | 9.29±4.81 | 11.43±6.37 | 12.74±6.51 | 9.64±7.29 | 0.036 |
| P300 reaction time,
msec | 461.8±140.3 | 395.1±99.08 | 449.7±115.77 | 380.1±78.04 | 0.006d |
In groups with or without radiotherapy, the average
age of starting treatment was similar, while patients with
radiotherapy were significantly older at the time of control
examination (mean age: 16.3±5.2 vs. 11.2±4.0 years, P<0.001)
(Table II).
| Table IIComparison of P300 potential
parameters in irradiated and non-irradiated groups of patients. |
Table II
Comparison of P300 potential
parameters in irradiated and non-irradiated groups of patients.
| Characteristic | NY + pBFM
(n=62) | BFM95 (n=74) | P-value |
|---|
| Starting treatment,
years | 5.3±3.7 | 4.9±2.5 | 0.690 |
| Mean age,
years | 16.3±5.2 | 11.2±4.0 | <0.001 |
| Total sum of
abnormalities | 15 (24.19%) | 21 (28.38%) | 0.581 |
| Prolonged P300
latency | 1 (10.0%) | 4 (5.41%) | 0.522 |
| Decreased P300
amplitude | 0 | 0 | - |
| Prolonged reaction
time | 13 (15.85%) | 16 (21.62%) | 0.007 |
| P300 latency,
msec | 331.113±25.891 | 331.473±31.048 | 0.941 |
| P300 amplitude,
mV | 10.395±5.727 | 12.739±6.508 | 0.027 |
| P300 reaction time,
msec |
427.371±124.423 |
449.689±115.772 | 0.284 |
The psychomotor development was compliant with
calendar age and all patients carried out their school duty in an
undisturbed manner. Moreover, no symptoms of central nervous system
focal injury were found in any patient during the clinical
evaluation.
Analysis of P300 evoked potentials in
individual protocols
The total group of ALL survivors had a significantly
prolonged mean P300 latency (331.31±28.71 vs. 298.14±38.76 msec,
P<0.001) and reaction time (439.51±119.86 vs. 380.11±79.94 msec,
P=0.002) compared to the control group. No differences were
observed in the average amplitude of the P300 potentials
(11.67±6.25 vs. 9.64±7.32 mV, P=0.179).
Mean P300 latencies in NY, pBFM and BFM95 were
329.13±28.07, 332.97±23.97 and 331.47±31.05, respectively. The
average amplitude of the P300 potentials and P300 reaction time in
studied groups were 9.29±4.8, 11.43±6.37, 12.74±6.51 and
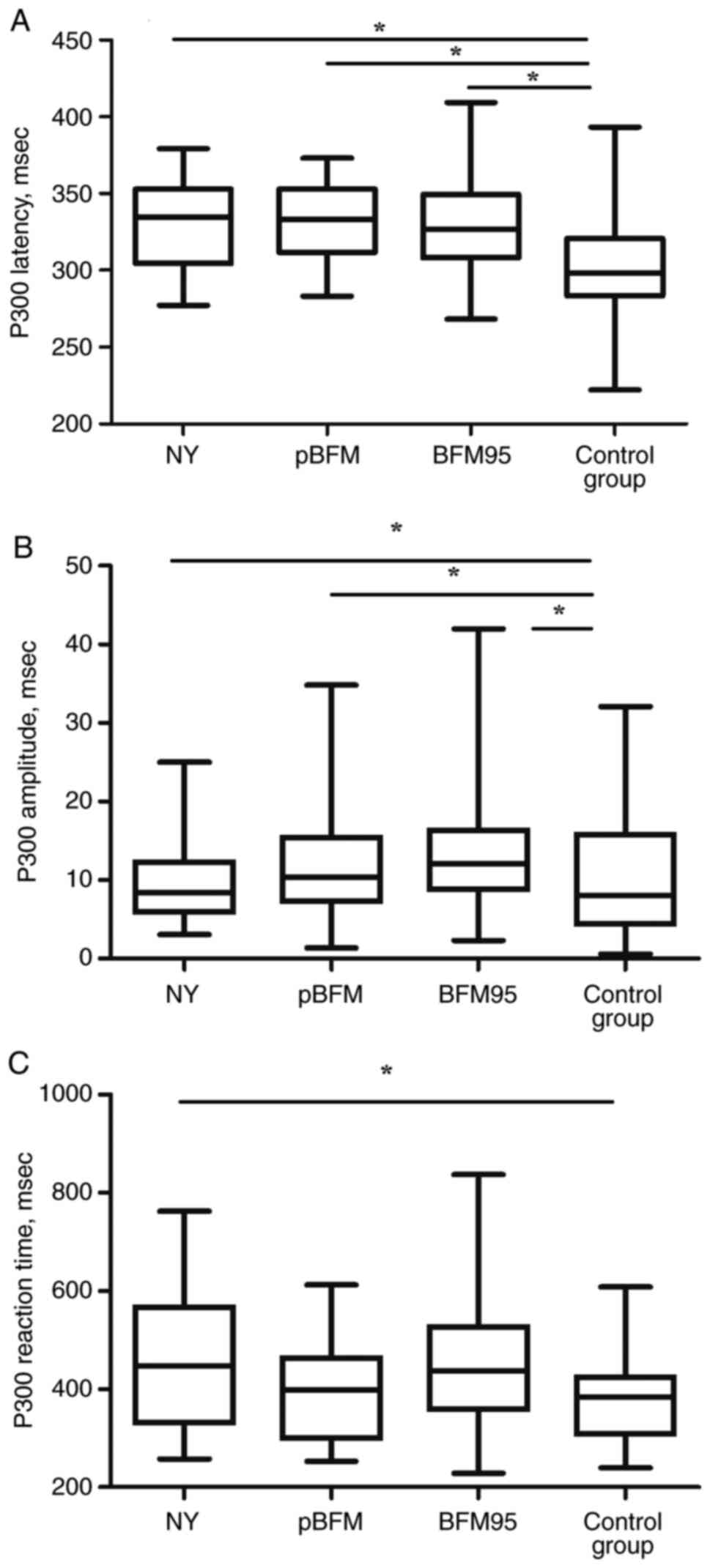
461.8±140.3, 395.1±99.08, 449.7±115.77 respectively (Table I). No statistically significant
differences in comparison of analyzed parameters between groups
with ALL were noticed. The differences in P300 potentials
parameters between study groups were presented in Fig. 1.
Significant changes were found in the screening with
endogenous evoked potentials in 10 (33.33%) NY patients. In turn,
the results of this study were abnormal in 5 (15.63%) pBFM and 21
(28.38%) BFM95 patients. There was no significant difference in the
total frequency of their occurrence in individual treatment groups
(Table I). In the NY group,
prolonged P300 latency was found in 1 patient and a prolonged
reaction time in 10 patients. The incidence of prolonged reaction
time was significantly higher than in other groups (P=0.007). In
the pBFM group, P300 latency was normal in all patients, while in
the BFM95 group latency was abnormal in 4 patients. In contrast,
the prolonged reaction time was recorded in 3 pBFM and 16 BFM95
patients. There was no reduction in P300 amplitude in any
patient.
Significant differences between the individual
protocols were observed in all measured parameters characterizing
the P300 evoked potentials (Table
I). The mean latency time was significantly longer compared to
the control group (298.14±41.57 msec) in all analyzed protocols
(Fig. 1A). The highest values were
observed in pBFM patients (NY: 329.13±28.07 msec, P=0.001; pBFM:
332.97±23.97 msec, P<0.001; BFM95: 331.47±31.05 msec,
P<0.001) (Fig. 1A). At the same
time, however, no intergroup differences were found between the
protocols analyzed in this study.
The combined analysis of the P300 wave amplitude in
individual groups using the Kruskal-Wallis test signaled a
significant difference (P=0.036) (Fig.
1B). However, further analysis of the average amplitude values
in the pair-comparison test did not reveal differences between
individual groups.
The reaction time was similarly prolonged compared
to the control group. Its largest and significant prolongation was
noted in the group treated with NY (461.8±140.3 vs. 380.1±78.04
msec, P=0.039) (Fig. 1C).
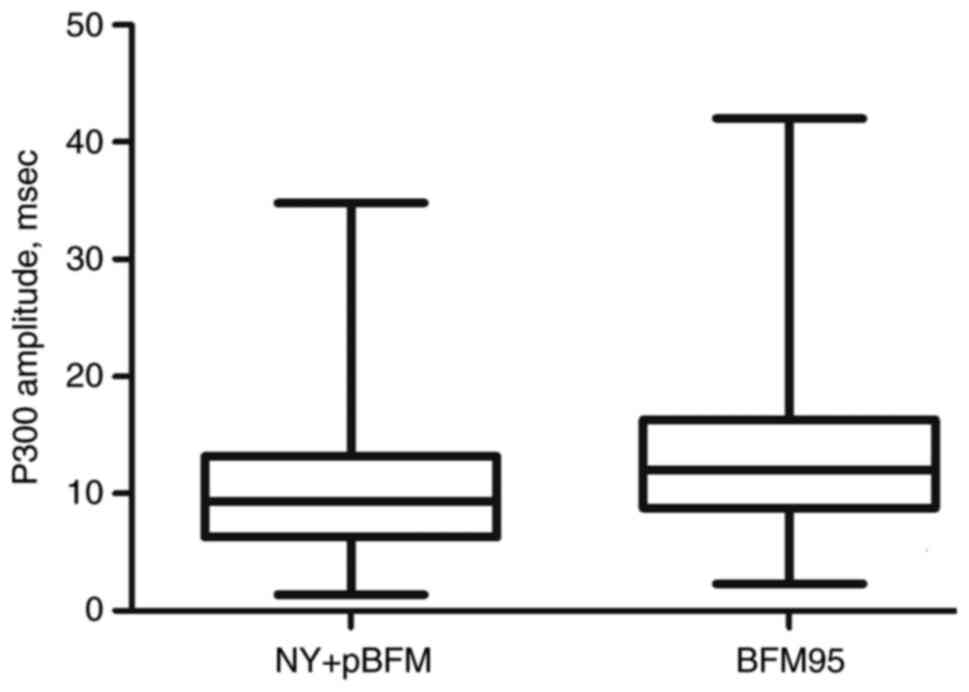
Impact of radiotherapy on P300
potential parameters
Abnormalities in the screening with endogenous
evoked potentials were observed in 15 (24.19%) patients treated
with NY + pBFM protocols. Analyzing the frequency of individual
P300 potential abnormalities, a significantly higher frequency of
reaction time prolongation was found in non-radiated patients
treated with BFM95 (21.62 vs. 15.85%, P=0.007). Despite the lack of
a decrease in P300 amplitude meeting adopted criteria in both
analyzed groups, a statistical analysis showed a significant
lowering impact of radiotherapy on the P300 wave amplitude (mean
values: 10.395±5.727 vs. 12.739±6.508 mV, P=0.027) (Fig. 2). No significant differences were
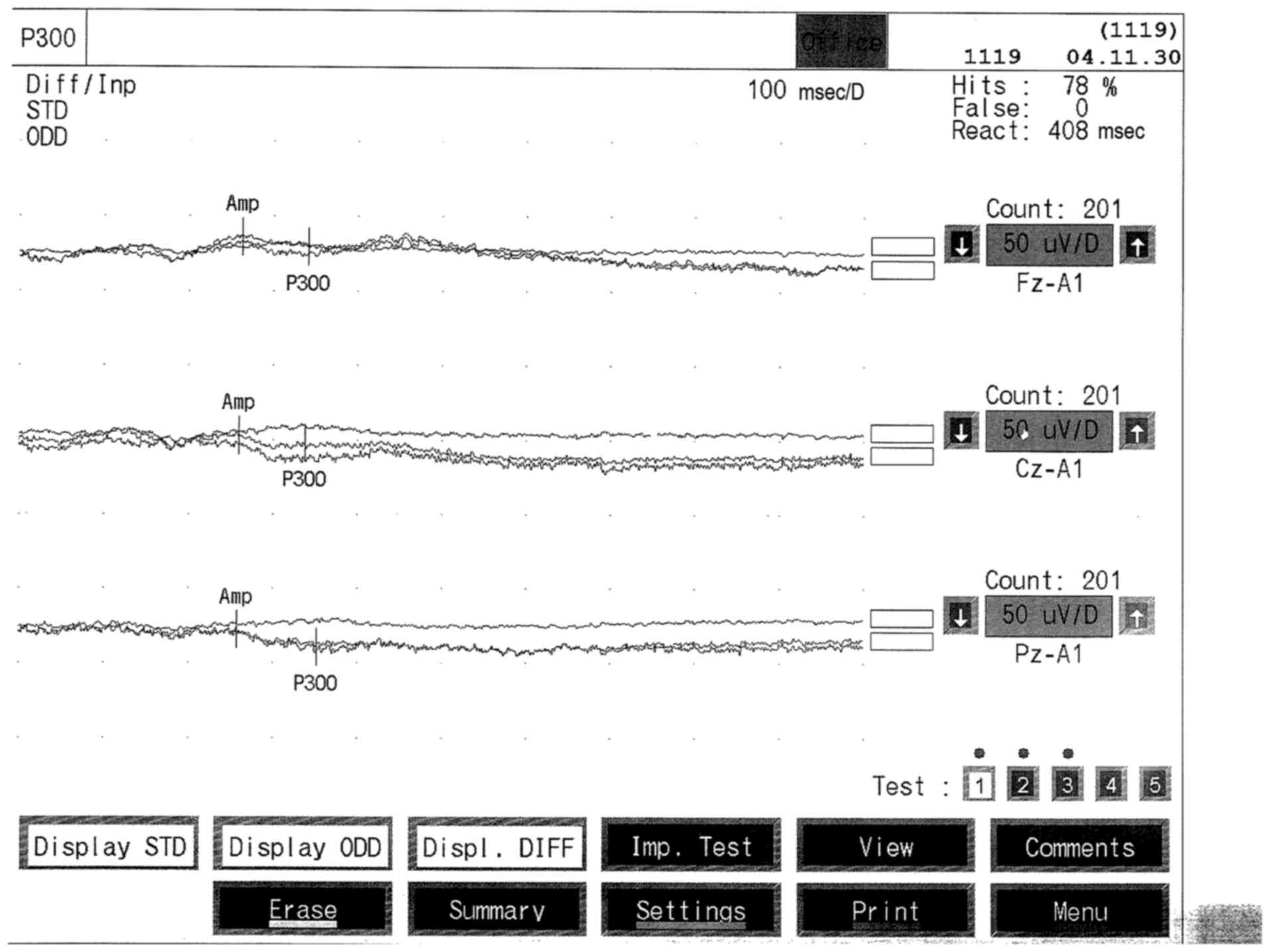
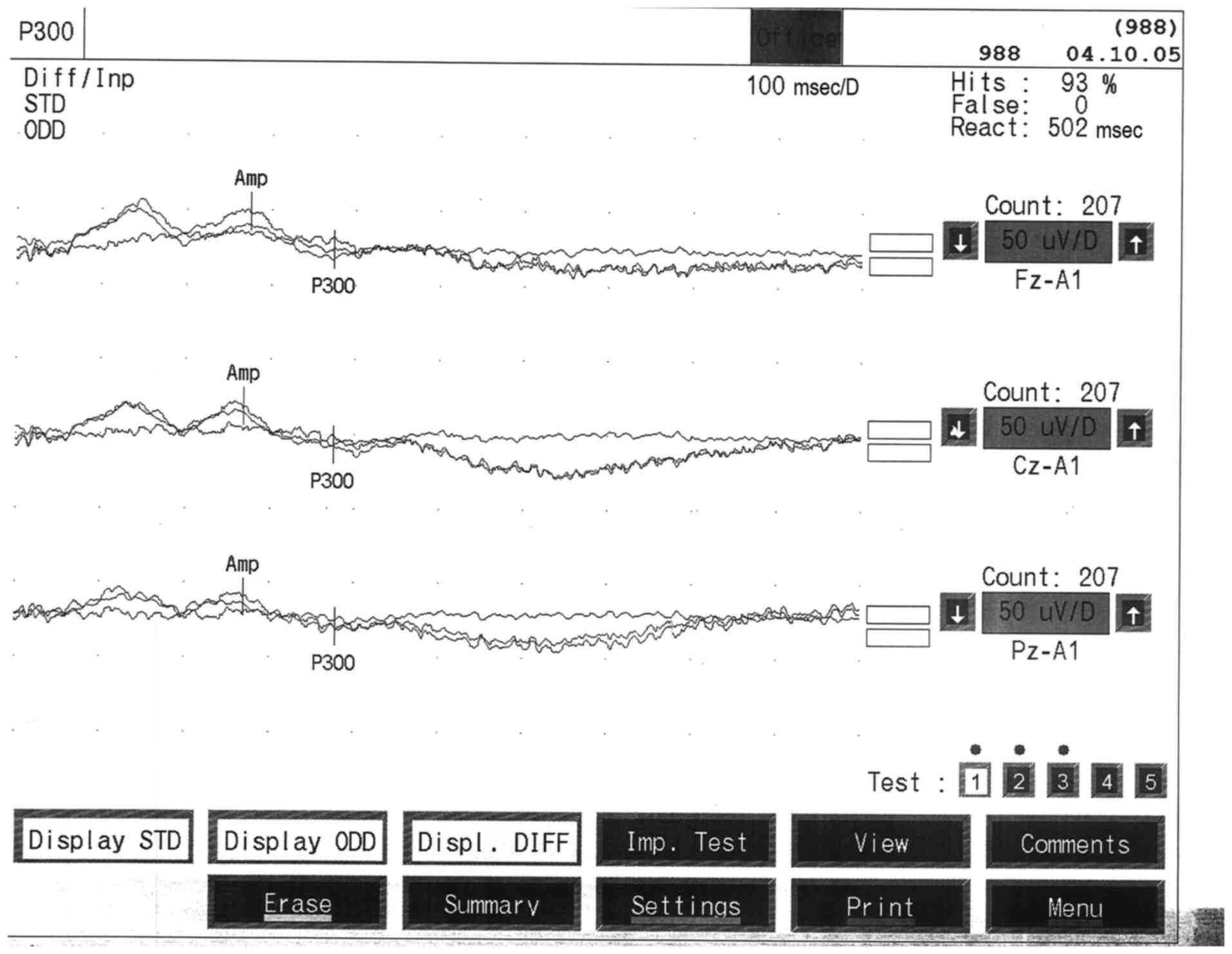
observed in the other analyzed parameters. The examples of P300
wave in patients treated with NY and BFM95 protocols were shown in
Figs. 3 and 4.
Discussion
P300 are an objective but non-target diagnostic
tool. The analysis of the results included the assessment of the
morphology, the record of the latency and amplitude of the obtained
potentials. Latency elongation above 2-2.5 SD, amplitude changes
above 50%, as well as incorrect morphology were considered
abnormal. The parameters of evoked potentials change with the
maturation of the nervous system and it is assumed that P300
latencies reach values similar to those in adults at the end of the
first decade of life (10). In
turn, the results of somatosensory evoked potentials latency are
the result of two processes: on the one hand, the growth of the
child and the elongation of limbs (and thus the extension of
latency), and on the other hand, the maturation of the nervous
system (shortening latency). Currently, it is assumed that the
values of P300 parameters are similar to those of adults at the end
of the first decade of life (10).
Stimulation with two distinctive acoustic stimuli
(oddball paradigm) is commonly used, and the P300 wave is formed
after 300-800 msec from the action of the stimulating stimulus. It
is generally accepted that its latency is a measure of the time
needed for the course of cognitive processes preceding the
cognitive assessment of the task situation, while the size of the
amplitude of this fraction is a measure of the involvement of
cognitive structures (10). In
turn, the correct reaction time indicates a good focus of
attention. This breakdown occurs when the recognition of a stimulus
is associated with a high level of subjective uncertainty and is a
measure of the degree of attention paid to a specific cognitive
task. The P300 wave arises at the end of a specific cognitive
process and has the highest amplitude in the leads from the
parietal region. It is assumed that it is generated in the
hippocampus area and in the temporal and parietal lobes of the
cerebral cortex (11). The P300
was first used in the diagnosis and monitoring of dementia
syndromes. Successively in the diagnosis of demyelinating diseases,
metabolic diseases, CNS tumors, phakomathoses, neuroinfections and
post-traumatic lesions. Of particular interest is the application
of endogenous potentials in patients with attention deficits with
hyperactivity and specific learning difficulties (12).
Several meta-analyses concerning neuropsychological
outcomes after treatment for childhood ALL have been developed so
far. All of them unanimously emphasize the heterogeneity of the
studied populations and the lack of a uniform cognitive impairment
analysis scheme in ALL patients. In the literature review of
neuropsychological consequences of ALL chemotherapy approximately
two thirds of analyzed studies found declines in different aspects
of cognitive functioning (13).
Cousens et al (14)
analyzed 31 studies reporting cognitive function in ALL children
after cranial irradiation. Decrements were found in intellectual
function, amounting to 10 intelligence quotient points. Campbell
et al (15) performed a
complex meta-analysis of 28 studies, those with cranial
irradiation, as well as studies in which treatment solely consisted
of chemotherapy. As has been shown, ALL survivors show significant
deficits in intellectual and neurocognitive functioning which
resulted in worse academic achievements. Moreover, ALL patients
treated with cranial irradiation performed worse intellectually
than those who received only intrathecal chemotherapy. In turn,
Peterson et al (16)
analyzed neuropsychological results of ALL treatment with
chemotherapy only. Based on 13 articles published until 2004, some
evidence for mild fine motor, executive function and verbal memory
weaknesses existed in these patients. In addition, the direct
relationship between higher levels of methotrexate and executive
dysfunction has been recently reported (17). This was also confirmed by the
diverse activity of particular brain regions visualized with
structural and functional magnetic resonance imaging (15).
Currently, the American Academy of Pediatrics
indicates neuropsychological follow-up as an important element of
long-term care for cancer survivors (18). However, this recommended approach
is not without drawbacks. There is still insufficient evidence to
guide the specific timing of comprehensive neuropsychological
assessment for children with ALL. Moreover, neuropsychometric
evaluation can be expensive, time-consuming and provide limited
insight into the neurobiological basis of cognitive dysfunction. As
a consequence, there is a need for simple functional methods to
screen which patients need extensive neuropsychological testing and
possible rehabilitation to optimize their learning capabilities and
academic achievements. Conventional EEG (electroencephalography)
recordings have not turned out to be useful in predicting late
effects of oncological treatment (19) but the endogenous event-related
potentials, which detect the neuronal electrical activity
associated with cognitive processing, seem to be more promising and
encouraging as earlier studies suggested (20). These diagnostic methods are known
to give objective information about both attention-dependent and
independent central auditory processing with quite simple and
inexpensive test arrangements.
According to our best knowledge, the presented data
constitute the largest report about the implementation of
event-related potentials in childhood ALL population. As we showed
in our study, abnormalities in screening assessment of P300
potential were detected in more than a quarter of ALL survivors.
Moreover, due to the inclusion of ALL patients treated with
different protocols, a significant effect of the type of treatment
on the nature of neuropsychological disorders in endogenous evoked
potentials was observed. The analyzed protocols contribute to the
prolongation of latency and reaction time of P300 potential. In
turn, the use of therapeutic protocols quite similar in terms of
used chemotherapy regimens but containing radiotherapy reduces its
amplitude. These abnormalities can be used to provide a more
accurate characterization of subtle and subclinical P300 potentials
changes in childhood ALL survivors.
The endogenous potentials analyzed in current study
are the result of changes in the electrical voltage associated with
information processing. They do not depend directly on the type of
stimulus but on thinking processes and are classified as
long-latency potentials constituting an electrophysiological
indicator of cognitive processes (10). The P300 potential is determined by
the positive wave with the highest amplitude recorded in the
central-parietal midline leads in response to the processing of the
auditory or visual stimulus. Stimulation with two distinct acoustic
stimuli (oddball paradigm) is commonly used. The P300 wave arises
after 300-800 msec. This wave occurs when the stimulus recognition
is associated with a high level of subjective uncertainty and is a
measure of the degree of attention devoted to a particular
cognitive task. It is assumed that it is generated in the
hippocampus and in the temporal and parietal lobes of the cerebral
cortex (21).
Among the greatest advantages of neurophysiological
techniques are their high sensitivity, non-invasiveness and the
ability to repeat them at relatively low costs. They are an
objective although non-specific neurological diagnostic tool.
Endogenous potentials are widely used in clinical practice, in
particular in the diagnosis of oligosymptomatic disease processes,
mainly dementia syndromes (22).
Their serial execution also allows to track the dynamics of the
disease process and monitor the treatment; therefore they are
helpful in determining the prognosis.
However, the usefulness of event-related potentials
in the diagnosis and monitoring of adverse effects of childhood ALL
treatment has not been sufficiently understood yet. As already
mentioned, event-related potentials reflect the synchronized
post-synaptic potentials generated by the depolarization of
neurons, primarily the large pyramidal cells of the cerebral
cortex. Its latency is a measure of the time needed for the
cognitive processes preceding the cognitive assessment of the task
situation, while the wave amplitude defines the involvement of
cognitive structures. The changes observed by us indicate slower
and more effortful target detection. Prolonged latency and a
reduction in the amplitude of the P300 potential have already been
shown in ALL survivors. However, all previous studies have been
conducted on small groups of patients. P300 latency has been found
to peak later and to have a smaller amplitude in childhood cancer
survivors (20,23). However, a study by Lähteenmäki
et al (20) was performed
on a heterogeneous group of only 19 cancer survivors, in which
there were 11 patients with ALL. In turn, Uberall et al
included only 13 long-time ALL survivors in their study (23). Our results are also consistent with
the results by Sato et al (24) who showed a significant increase in
P300 latency in 33 patients treated with chemotherapy and
radiotherapy compared to patients treated with chemotherapy alone
and to the control group. Moore et al also made similar
observations on an equally large group of childhood cancer
survivors (25). Järvelä et
al demonstrated the usefulness of P300 potentials in monitoring
of central nervous system toxicity of ALL therapy in 27 patients.
They showed a relationship between progressive deterioration of
mental performance and prolongation of the peak latency as well as
poorer enhancement of P300 amplitude after treatment (26). The previous observations presented
above have also been confirmed by recently published preliminary
results by Brace et al (13). Decreased amplitude of particular
P300 components were observed in the analyzed small group of 8 ALL
survivors treated exclusively with chemotherapy protocols.
Our study may also have potential therapeutic
implications in the future. N-methyl-D-aspartate (NMDA) channels
have a central role in the generation of event-related potentials
(27). Differences in particular
parameters of P300 potentials between ALL survivors and controls
are consistent with altered neurotransmission through NMDA
receptors (28). Recent
preclinical study has revealed that memantine, non-competitive NMDA
receptor antagonist, reduces the incidence of cognitive deficits in
rats treated with intrathecal methotrexate (28). Memantine has also shown promising
effects in randomized trial among adults treated with cranial
radiation for brain tumors (29).
Potentially, a group of patients with subtle neurocognitive
dysfunction identified on the basis of screening with P300
event-related potentials can therefore experience the benefits of
prophylactic use of NMDA antagonists. Such behavior may protect
this selected group of patients from the development of symptomatic
cognitive impairment. However, large randomized trials using NMDA
antagonists in patients with childhood ALL are necessary to confirm
this hypothesis.
Our study has several limitations. First, our study
compared different protocols previously used in clinical practice.
However, it was our deliberate intention. Thanks to this it is
possible to study the impact of radiotherapy withdrawn from many
protocols currently used in ALL on P300 potentials. Second,
neuroimaging and neuropsychological correlations with
neurophysiological results were not performed. However, the purpose
of our study was only to evaluate the value of electrophysiological
P300 potentials changes. The performed neurophysiological studies
informed about maintaining the functional integrity of the nervous
system. None of the patients exceeded the 5% margin of uncounted
discriminating stimuli which indicates the correct concentration of
attention. Third, genetic methods, which are increasingly used in
the diagnosis of cognitive disorders in the pediatric population,
have not been used (30).
As we did not study the neurological status of the
patients at diagnosis, we could not prove the unambiguous cause of
observed changes in P300. In case of primary localization all
symptoms usually resolve after therapy. Therefore the observed
changes were most likely consequences of therapy. Other limitation
was lack of psychological assessment in the study protocol.
In conclusion, endogenous P300 event-related
potentials may be useful in screening assessment of ALL survivors.
The type of treatment protocol significantly modulates the
individual parameters of the registered P300 potentials.
Understanding with the analysis of event-related potentials how ALL
survivors brain responses are affected post-treatment will
elucidate the type of the cognitive deficits and provide insights
into new potential targets for intervention or prevention
strategies.
Acknowledgements
The pilot findings of the present study were
presented during an annual congress: Kroczka S, et al.
Screening of Cognitive Impairment in Childhood Acute Lymphoblastic
Leukemia Survivors With P300 Event-Related Potentials, The 52nd
Annual Congress of the International Society of Paediatric Oncology
(SIOP 2020), Ottava, October 14-17, 2020 Pediatric Blood and Cancer
2020,67(54), 364. doi.org/10.1002/pbc.28742.
Funding
Funding: The present study was supported by the following
Jagiellonian University grant numbers: WŁ/570/KL/L
(Electromyographic evaluation of the consequences of treatment of
acute lymphoblastic leukemia in children) and 501/NKL/206/L
(Neurophysiological consequences of acute lymphoblastic leukemia in
cured children).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
SK and SS contributed to the study concept and
design. SK, KK, AGe, OG and SS performed diagnostic tests and
collected relevant clinical data. SK, KK and AGr conducted
statistical analysis and wrote sections of the manuscript. SK and
SS critically revised the article. SK and SS confirm the
authenticity of all the raw data. All authors were responsible for
the integrity and accuracy of the data and approved the submitted
version. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study protocol complied with the Declaration of
Helsinki and was approved by the Jagiellonian University Medical
College Ethics Committee (consent no. KBET/131/B/207). All parents,
and patients over 16 years of age signed written informed consent
before inclusion in the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Howlader N, Noone AM, Krapcho M, Miller D,
Brest A, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, et al:
SEER Cancer Statistics Review, 1975-2016. National Cancer
Institute, Bethesda, MD, 2019. https://seer.cancer.gov/csr/1975_2016/. Accessed
October 28, 2019.
|
|
2
|
Czogała M, Balwierz W, Sztefko K and
Rogatko I: Antithrombin III as the indicator of L-asparaginase
activity in children treated for acute lymphoblastic leukemia. J
Pediatr Hematol Oncol. 39:114–120. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Mrdjanović J, Šolajić S, Srđenović-Čonić
B, Bogdanović V, Dea KJ, Kladar N and Jurišić V: The oxidative
stress parameters as useful tools in evaluating the DNA damage and
changes in the complete blood count in hospital workers exposed to
low doses of antineoplastic drugs and ionizing radiation. Int J
Environ Res Public Health. 18(8445)2021.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Pearlstein RD, Whitten C and Haerich P:
Assessing neurocognitive dysfunction in cranial radiotherapy: Can
cognitive event-related potentials help? Technol Cancer Res Treat.
5:109–125. 2006.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Ball WS Jr, Prenger EC and Ballard ET:
Neurotoxicity of radio/chemotherapy in children: Pathologic and MR
correlation. AJNR Am J Neuroradiol. 13:761–776. 1992.PubMed/NCBI
|
|
6
|
Vezmar S, Becker A, Bode U and Jaehde U:
Biochemical and clinical aspects of methotrexate neurotoxicity.
Chemotherapy. 49:92–104. 2003.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kahkonen M, Harila-Saari A, Metsahonkala
L, Korhonen T, Norvasuo-Heilä MK, Utriainen T, Ahonen A, Bergman J,
Salmi TT and Minn H: Cerebral blood flow and glucose metabolism in
long-term survivors of childhood acute lymphoblastic leukaemia. Eur
J Cancer. 35:1102–1108. 1999.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Jurisic V, Radenkovic S and Konjevic G:
The actual role of LDH as tumor marker, biochemical and clinical
aspects. Adv Exp Med Biol. 867:115–124. 2015.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Kwiecinska K, Zakrzewska Z, Strojny W,
Cwiklinska M, Balwierz W and Skoczen S: Extended follow-up of
children with high-risk acute lymphoblastic leukemia treated with
American and European Protocols-A clash of different ideas. Clin
Oncol. 5(1759)2020.
|
|
10
|
Goodin D, Desmedt J, Maurer K and Nuwer
MR: IFCN recommended standards for long latency auditory
event-related potentials. Report of an IFCN committee.
International federation of clinical neurophysiology.
Electroencephalogr Clin Neurophysiol. 91:18–20. 1994.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Halgren E, Marinkovic K and Chauvel P:
Generators of the late cognitive potentials in auditory and visual
oddball tasks. Electroencephalogr Clin Neurophysiol. 106:156–164.
1998.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Meador KJ, Hammond EJ, Loring DW, Allen M,
Bowers D and Heilman KM: Cognitive evoked potentials and disorders
of recent memory. Neurology. 37:526–529. 1987.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Brace KM, Lee WW, Cole PD and Sussman ES:
Childhood leukemia survivors exhibit deficiencies in sensory and
cognitive processes, as reflected by event-related brain potentials
after completion of curative chemotherapy: A preliminary
investigation. J Clin Exp Neuropsychol. 41:814–831. 2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Cousens P, Waters B, Said J and Stevens M:
Cognitive effects of cranial irradiation in leukaemia: A survey and
meta-analysis. J Child Psychol Psychiatry. 29:839–852.
1988.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Campbell LK, Scaduto M, Sharp W, Dufton L,
Van Slyke D, Whitlock JA and Compas B: A meta-analysis of the
neurocognitive sequelae of treatment for childhood acute
lymphocytic leukemia. Pediatr Blood Cancer. 49:65–73.
2007.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Peterson CC, Johnson CE, Ramirez LY,
Huestis S, Pai AL, Demaree HA and Drotar D: A meta-analysis of the
neuropsychological sequelae of chemotherapy-only treatment for
pediatric acute lymphoblastic leukemia. Pediatr Blood Cancer.
51:99–104. 2008.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Krull KR, Cheung YT, Liu W, Fellah S,
Reddick WE, Brinkman TM, Kimberg C, Ogg R, Srivastava D, Pui CH, et
al: Chemotherapy pharmacodynamics and neuroimaging and
neurocognitive outcomes in long-term survivors of childhood acute
lymphoblastic leukemia. J Clin Oncol. 34:2644–2653. 2016.PubMed/NCBI View Article : Google Scholar
|
|
18
|
American Academy of Pediatrics Section on
Hematology/Oncology Children's Oncology Group. Long-term follow-up
care for pediatric cancer survivors. Pediatrics. 123:906–915.
2009.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Ueberall MA, Skirl G, Strassburg HM,
Wenzel D, Hertzberg H, Langer T, Meier W, Berger-Jones K, Huk WJ,
Korinthenberg R and Beck JD: Neurophysiological findings in
long-term survivors of acute lymphoblastic leukaemia in childhood
treated with the BFM protocol 81 SR-A/B. Eur J Pediatr.
156:727–733. 1997.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Lähteenmäki PM, Holopainen I, Krause CM,
Helenius H, Salmi TT and Heikki LA: Cognitive functions of
adolescent childhood cancer survivors assessed by event-related
potentials. Med Pediatr Oncol. 36:442–450. 2001.PubMed/NCBI View
Article : Google Scholar
|
|
21
|
Sur S and Sinha VK: Event-related
potential: An overview. Ind Psychiatry J. 18:70–73. 2009.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Vecchio F and Määttä S: The use of
auditory event-related potentials in Alzheimer's disease diagnosis.
Int J Alzheimers Dis. 2011(653173)2011.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Uberall MA, Haupt K, Meier W, Hertzberg H,
Beck JD and Wenzel D: P300 abnormalities in long-time survivors of
acute lymphoblastic leukemia in childhood-side effects of CNS
prophylaxis? Neuropediatrics. 27:130–135. 1996.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Sato T, Miyao M, Muchi H, Gunji Y, Iizuka
A and Yanagisawa M: P300 as indicator of effects of prophylactic
cranial radiation. Pediatr Neurol. 8:130–132. 1992.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Moore BD III, Copeland DR, Ried H and Levy
B: Neurophysiological basis of cognitive deficits in long-term
survivors of childhood cancer. Arch Neurol. 49:809–817.
1992.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Järvelä LS, Hurme S, Holopainen IE, Leino
M, Hatanpää AM, Mikola H, Kärki T, Salmi TT and Lähteenmäki PM:
Auditory event related potentials as tools to reveal cognitive late
effects in childhood cancer patients. Clin Neurophysiol. 122:62–72.
2011.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Tikhonravov D, Neuvonen T, Pertovaara A,
Savioja K, Ruusuvirta T, Näätänen R and Carlson S: Effects of an
NMDA-receptor antagonist MK-801 on an MMN-like response recorded in
anesthetized rats. Brain Res. 1203:97–102. 2008.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Cole PD, Vijayanathan V, Ali NF, Wagshul
ME, Tanenbaum EJ, Price J, Dalal V and Gulinello ME: Memantine
protects rats treated with intrathecal methotrexate from developing
spatial memory deficits. Clin Cancer Res. 19:4446–4454.
2013.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Brown PD, Pugh S, Laack NN, Wefel JS,
Khuntia D, Meyers C, Choucair A, Fox S, Suh JH, Roberge D, et al:
Memantine for the prevention of cognitive dysfunction in patients
receiving whole-brain radiotherapy: A randomized, double-blind,
placebo-controlled trial. Neuro Oncol. 15:1429–1437.
2013.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Cole PD, Finkelstein Y, Stevenson KE,
Blonquist TM, Vijayanathan V, Silverman LB, Neuberg DS, Sallan SE,
Robaey P and Waber DP: Polymorphisms in genes related to oxidative
stress are associated with inferior cognitive function after
therapy for childhood acute lymphoblastic leukemia. J Clin Oncol.
33:2205–2211. 2015.PubMed/NCBI View Article : Google Scholar
|