Introduction
Osteoblastoma is a rare, benign, bone-forming tumor
accounting for less than 1% of all primary bone tumors and 3.5% of
benign bone tumors (1); most
osteoblastomas frequently arise in the spine (approximately 30-40%)
and long (approximately 30%) and small tubular bones of the hands
and feet (approximately 10-20%) and infrequently arise in the flat
bones and jaw bones (2,3). Osteoblastoma mainly affects
adolescents and young adults; 75-90% of patients are aged between 6
and 30 years, with a male-to-female ratio of 2:1 (2,3). The
patella is an uncommon site for the occurrence and development of
bone tumors. The vast majority of tumors of the patella are benign,
with a significant incidence of giant cell tumor and
chondroblastoma, accounting for 33 and 16% of all tumors of the
patella, respectively (4).
Osteoblastoma of the patella is extremely rare, accounting for
approximately 2% of all tumors of the patella (4,5). To
the best of our knowledge, very few cases of osteoblastoma of the
patella have been reported (Table
I) (6-10).
Therefore, herein, we reported an extremely rare case of
osteoblastoma of the patella in a 22-year-old young male adult. The
patient was treated with thorough intralesional curettage and with
subsequent autologous iliac cancellous bone grafting; he had an
uneventful recovery with no clinical and radiological evidence of
recurrence after a follow-up of 2 years. The patient was informed
that medical documentation and information regarding the case would
be submitted for publication, and he provided consent.
 | Table ISummary of all published cases of
patellar osteoblastoma to date. |
Table I
Summary of all published cases of
patellar osteoblastoma to date.
| Cases | Year | Language | Age (years)/
Gender | Symptoms | Therapies | Follow-up
(months) | Outcomes | (Refs.) |
|---|
| Sicard et
al | 1979 | French | N/A | N/A | Patellectomy after
failed wide curettage | N/A | Cure | (6) |
| De Coster et
al | 1989 | English | 29/Male | Sudden pain and
swelling | Intralesional
curettage and autologous iliac cancellous bone grafting | 18 | No evidence of
recurrence and a normal incorporation of the cancellous | (7) |
| Shen et
al | 2001 | English | 34/Male | Pain and mild
swelling, tenderness | Intralesional
curettage and allogeneic bone grafting | 24 | Graft Complete
healing of the lesion without evidence of recurrence | (8) |
| Bhagat et
al | 2008 | English | 38/Male | Pain | Excision of the
lesion | 48 | Living | (9) |
| Zhong et
al | 2010 | Chinese | 20/Female | Pain and swelling,
tenderness | Intralesional
curettage and autologous iliac cancellous bone grafting | 3 | No evidence of
recurrence and the cancellous graft healed well | (10) |
| Current case | 2023 | English | 22/Male | Intermittent pain,
tenderness | Intralesional
curettage and autologous iliac cancellous bone grafting | 24 | No clinical and
radiological evidence of recurrence | |
Case presentation
A 22-year-old male young adult was admitted to the
940th Hospital of Joint Logistics Support Force of Chinese People's
Liberation Army (Lanzhou, Gansu, China) on December 5, 2020, with a
6-month history of intermittent pain in his right knee in absence
of trauma. He did not have a significant personal or family medical
history. His physical examination showed no obvious swelling or
redness, and he had a normal skin temperature on the right knee.
However, there was direct tenderness on the right patella. The
range of motion of the right knee was full. The floating patella
test, patella grind test, McMurray's test, anterior-posterior
drawer test, and valgus-varus stress test were all negative. His
neurological examination was normal. Laboratory tests revealed that
his routine blood, liver function, kidney function, erythrocyte
sedimentation rate, C-reactive protein, and tumor marker results
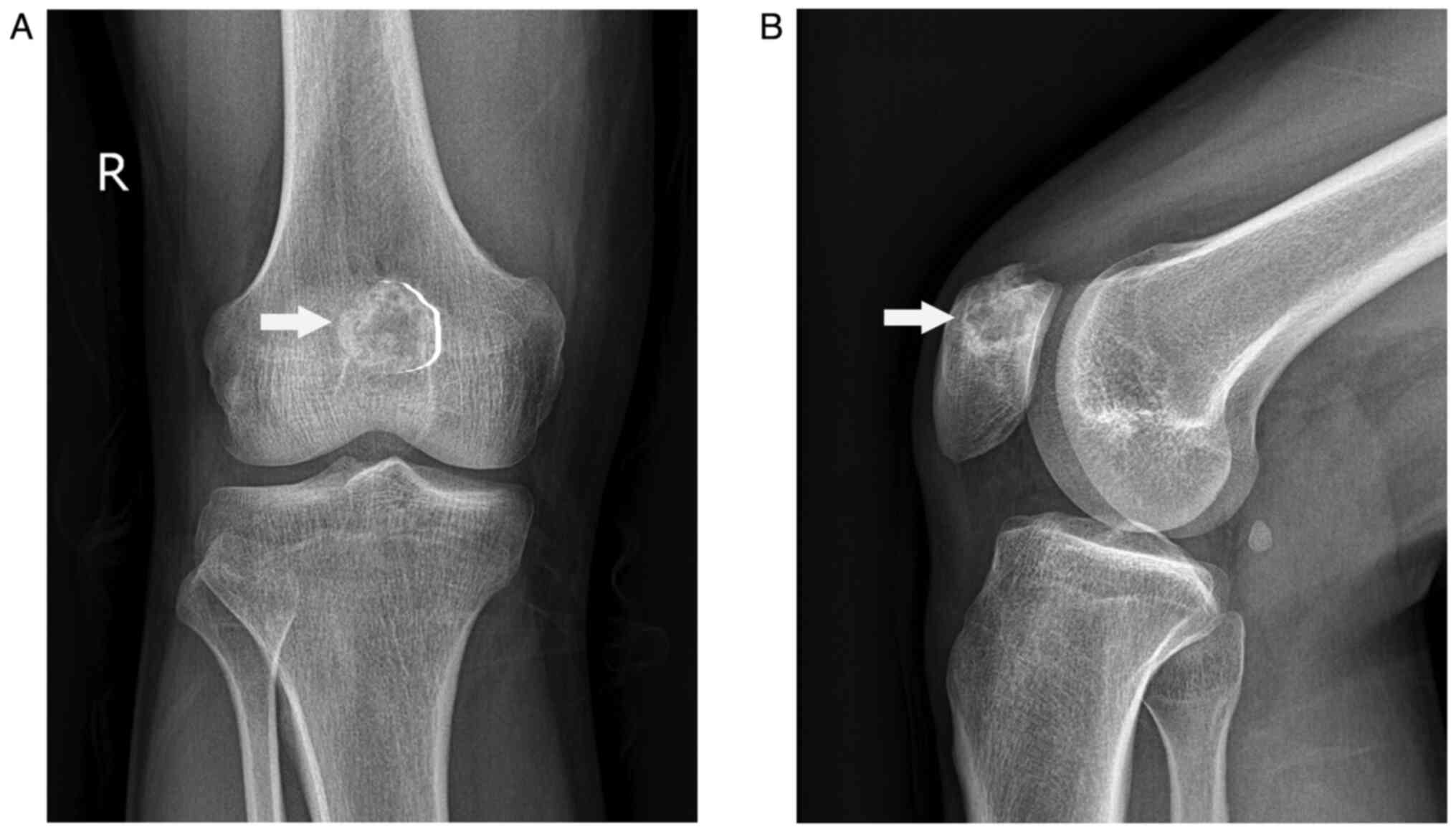
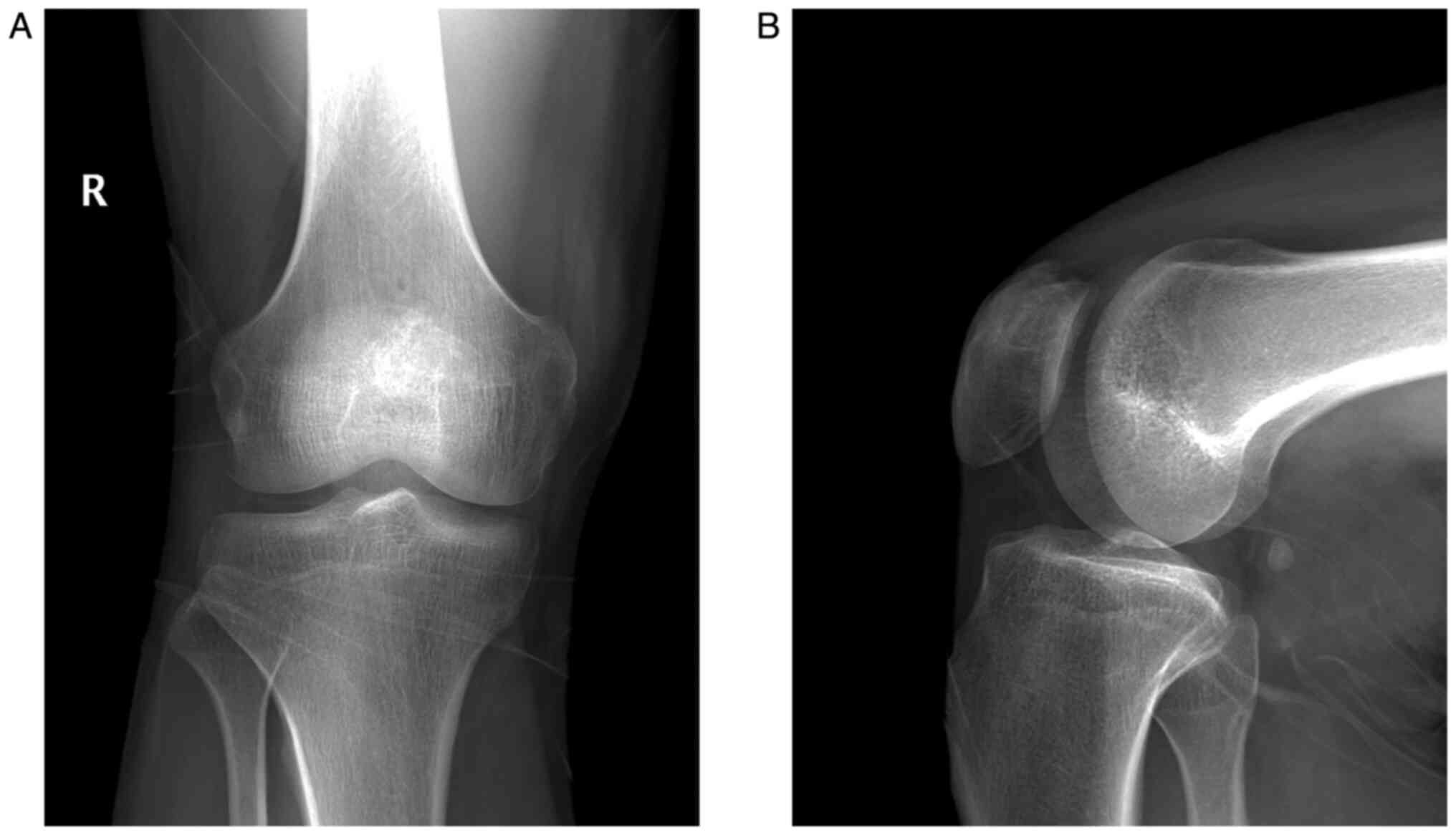
were within the normal range. Radiography of the knee showed an
osteolytic lesion at the medial superior quadrant of the right
patella surrounded by a sclerotic margin with high density
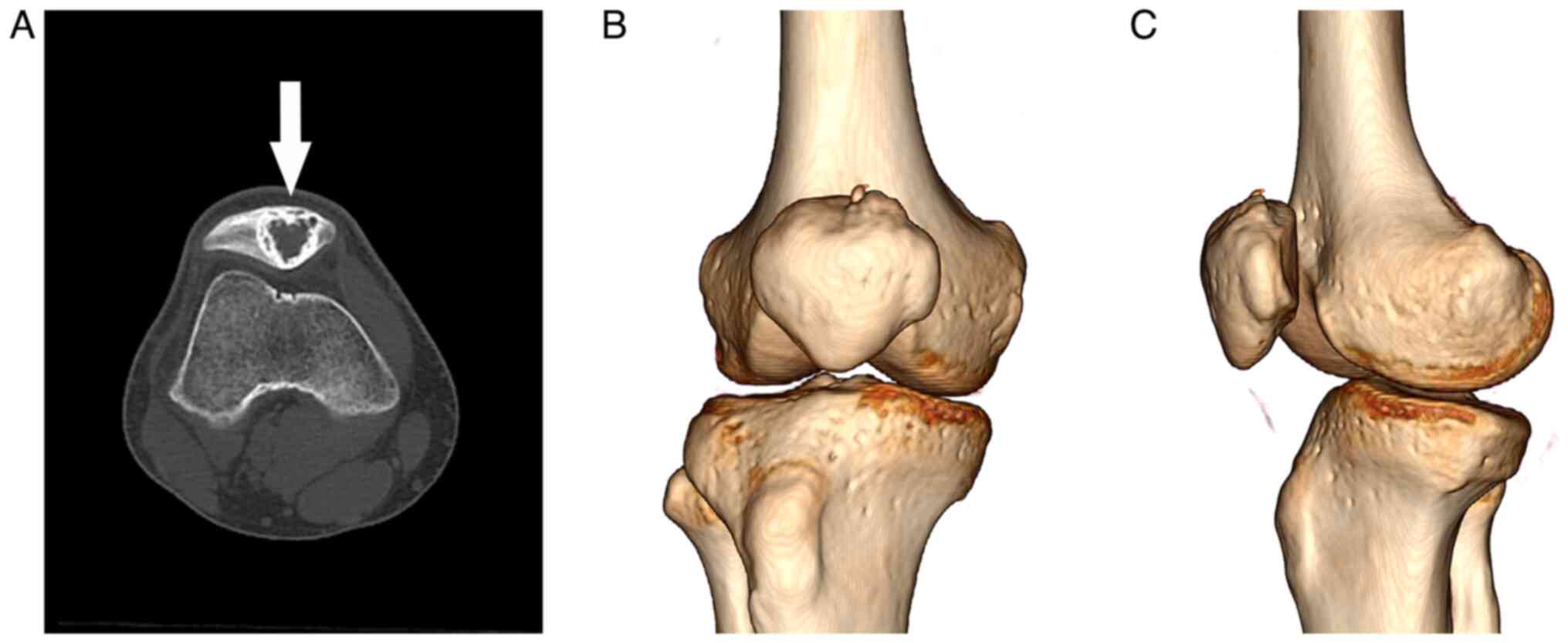
(Fig. 1). Computed tomography (CT)
scan revealed a circular mixed-density image of the right patella
that was surrounded by a thick sclerotic margin with high density
(Fig. 2A). Three-dimensional CT
showed no pathological fracture or cortical bone breakthrough
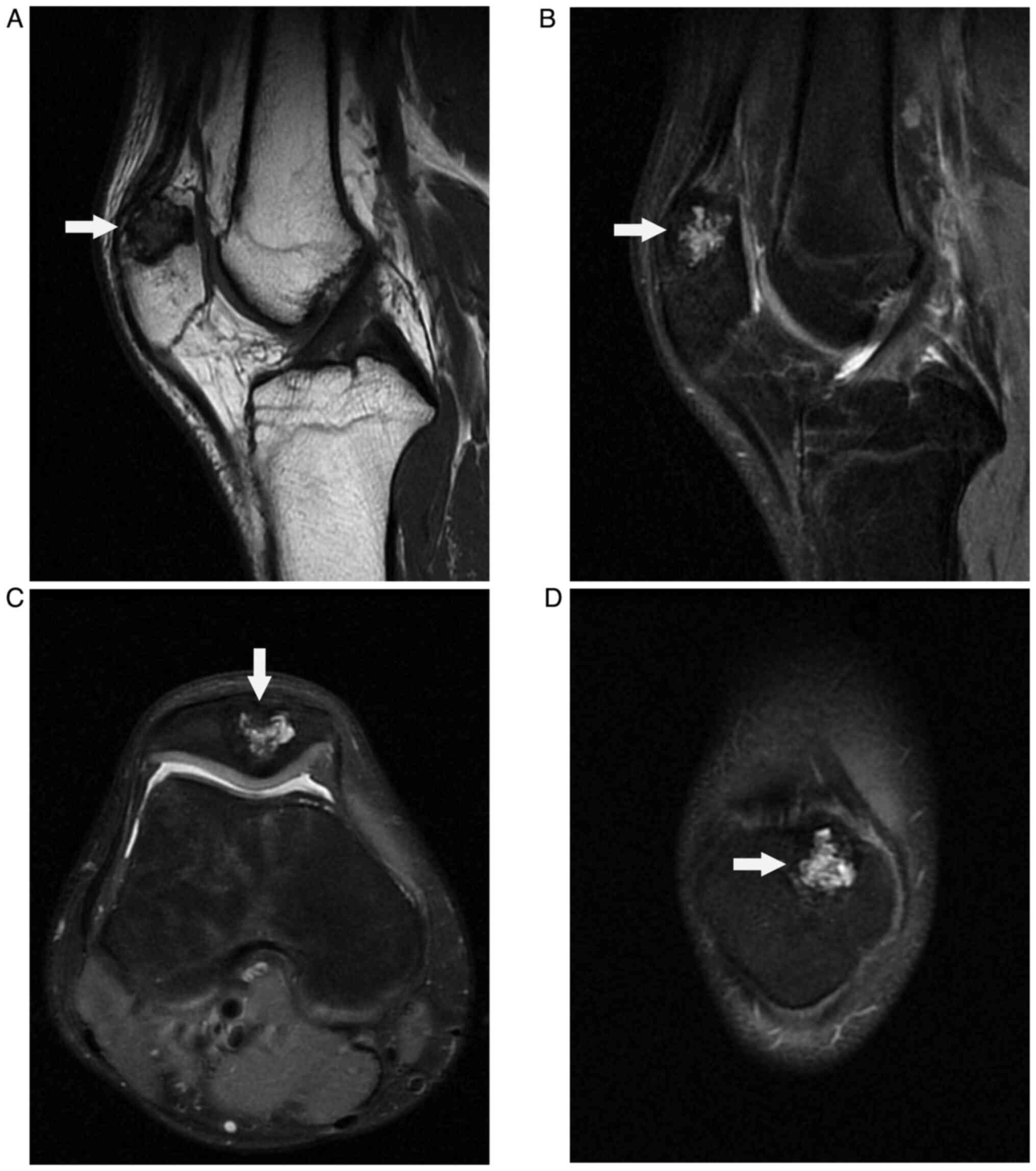
(Fig. 2B and C). Magnetic resonance imaging (MRI)
displayed a low-intensity signal mass on T1-weighted image
(Fig. 3A) and high-intensity
signal mass on T2-weighted image (Fig.
3B, C and D) with a well-defined lesion of the
patella. Considering the clinical and imaging manifestations of the
patient, benign bone lesions including chondroblastoma, osteoid
osteoma, osteoblastoma, and bone abscess, were considered as the
initial diagnosis.
The preoperative contraindications were excluded.
The patient was administered spinal anesthesia in the supine
position by applying an air pressure tourniquet on the right thigh
(pressure 35 kPa for 90 min). The right knee and homolateral iliac
region were routinely disinfected and draped. First, a 3-cm oblique
incision along the anterior superior iliac spine was made for
cutting the cancellous bone. In total, approximately 2
cm3 (2.0x1.0x1.0 cm) autologous iliac cancellous bone
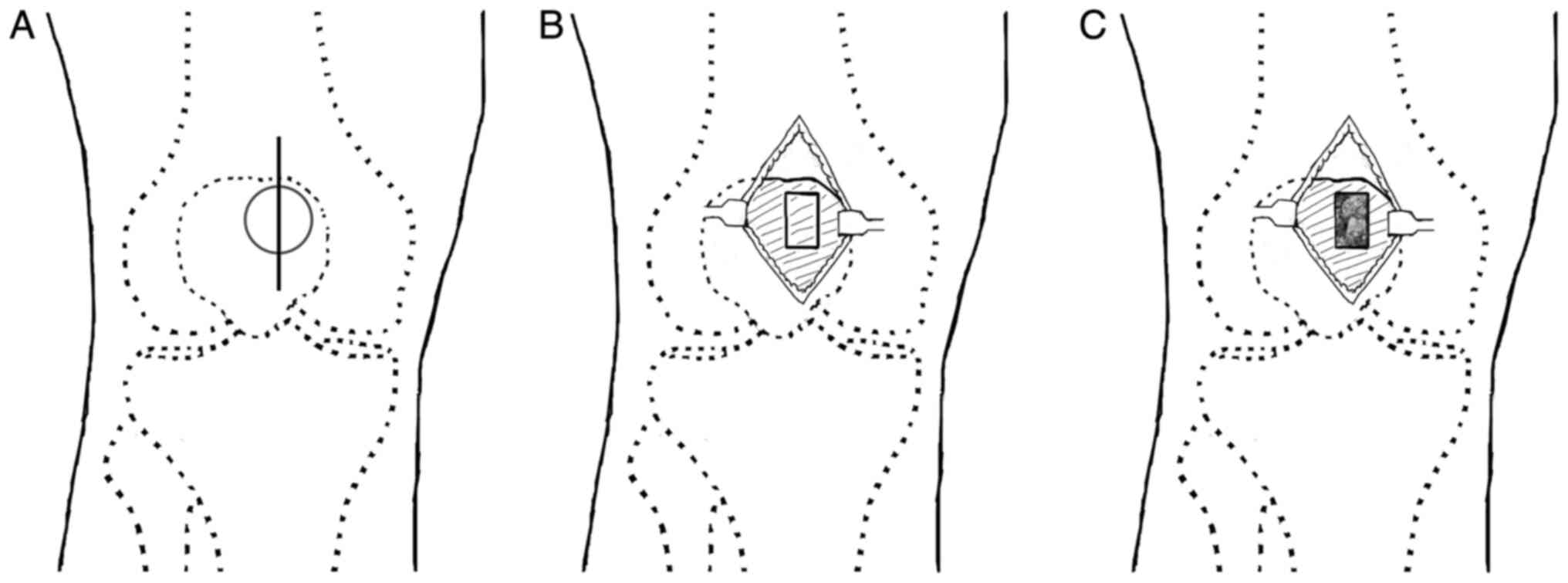
was removed for subsequent grafting. Then, to expose the right
patella, a 4-cm longitudinal anteromedial incision was made
(Fig. 4A), and the soft tissue was
not invaded by the bone tumor. The bone window (0.5x1 cm) was
located on the medial superior quadrant of the patella (Fig. 4B). Thorough intralesional curettage
of the bone tumor was performed. The specimen contained a mixture
of sand-like, pale-yellow substances. The tumor border was ground
by a high-speed burr and cauterized using a high-frequency
electrotome. The tumor cavity was inactivated by anhydrous ethanol
and washed with distilled water for 20 and 10 min, respectively. To
reconstruct bone defects, the tumor cavity of the patella was
subsequently filled with autogenous iliac cancellous bone (Fig. 4C). Finally, the intraoperative
specimen was submitted for histopathological examination.
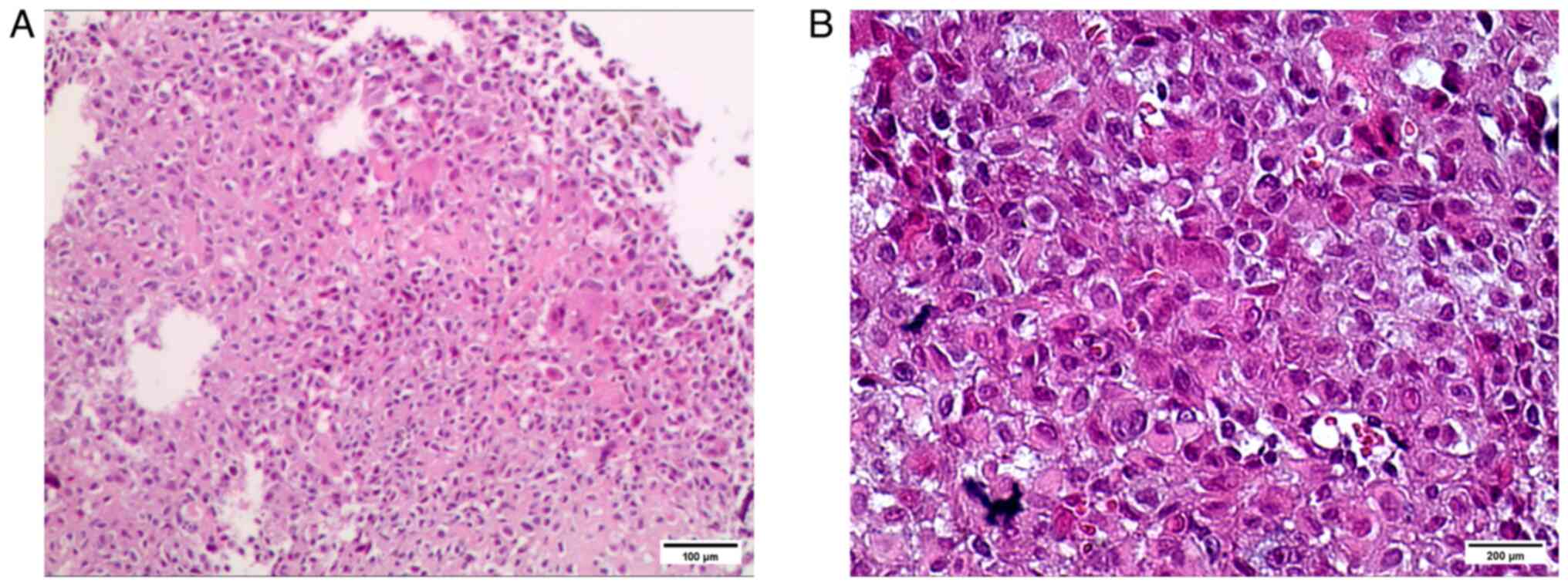
Pathologist conducted histopathological examination
through hematoxylin-eosin staining. The intraoperative specimen was
made into paraffin sections through the procedures of fixation,
washing, dehydration, transparency, wax penetration, embedding,
sectioning, and then underwent the procedures of dewaxing,
hydration, staining (hematoxylin, 15 min), washing,
differentiation, washing, re-staining (eosin, 3 min), dehydration,
transparency, and sealing before microscopy. The histopathological
examination findings showed that oval osteoblasts were distributed
in sheets, in which focal multinucleated giant cells were observed.
The histopathological findings were consistent with the diagnosis
of benign osteoblastoma (Fig.
5).
At the last follow-up 2 years postoperatively, no
clinical and radiological evidence of local recurrence was noted,
and the bone graft was blurred and fused (Fig. 6). The patient's sports and physical
functioning domain score was 100 points. In spite of satisfactory
outcome, we require a long-term regular follow-up in order to
perform an early detection and treatment for a possible
recurrence.
Discussion
The clinical presentations of osteoblastoma differ
depending on its location. Cranial osteoblastoma may present as an
enlarging mass with or without pain and neurological symptoms
(11). Osteoblastoma of the spine
can present with localized pain, night pain, extremity weakness,
and radicular pain (12,13). The aggressive variants of
osteoblastoma usually present with more intense pain, which can be
due to localized areas of destruction (14). The most common symptoms of
osteoblastoma of the patella are pain and swelling (7,8).
Local tenderness may be noted during physical examination (8).
The imaging manifestations of osteoblastoma differ
depending on its location, and the results lack specificity. The
most frequent X-ray manifestations of the osteoblastoma of the
patella are that of an osteolytic lesion, with or without matrix
mineralization and pathological fracture of the patella, surrounded
by a high-density sclerotic margin with no evidence of
extra-articular invasion (7,15).
Aggressive spinal osteoblastoma can break through the bony cortex
and invade the spinal canal and paravertebral soft tissue (16,17).
CT scans are superior to MRI in showing calcification of
osteoblastoma and thus are used to further confirm a well-defined
lesion with fine calcifications. However, the radiological
characteristics of CT are atypical. Tang P et al reported a
case of osteoblastoma of the rib that was misdiagnosed as
lymphomatous by CT and was confirmed by pathological examination
(18). MRI helps in evaluating
bone marrow edema and soft tissue component or extension of the
tumor; however, there is no significant specificity to this
finding.
The pathological examination findings of
osteoblastoma reveal that the lesion is composed of irregular
trabeculae of woven bone, lined by active osteoblasts within a
copious vascularized fibrous stroma containing focal multinucleated
giant cells (7,8). The cartilaginous matrix may be
present rarely (19).
Osteoblastoma is difficult to distinguish from osteoid osteoma due
to their similar imaging and histopathological patterns (20). Some of the histopathological
features suggesting the diagnosis of the aggressive variant
included surrounding soft tissue invasion, large and more irregular
trabeculae of woven bone, ace- or sheet-like osteoid production,
abundant large epithelioid osteoblasts, increased mitotic figures,
disordered osteoid matrix, less vascularized fibrous stroma
(3,21).
The treatment of osteoblastoma depends on the
location within the bone and the aggressiveness of the tumor
(20,22). In theory, the treatment options
available for osteoblastoma of the patella include intralesional
curettage followed by bone grafting or bone cement, en-bloc
resection of the lesion, and even patellectomy. To treat the
osteoblastoma of the patella, intralesional curettage with
subsequent allogeneic bone grafting has been previously performed
(7,8). Intralesional curettage can be
effective but is related to a recurrence rate of 15-25% (23). Patellectomy can be the used for a
failure after wide intralesional curettage (6). En-bloc resection is the preferred
treatment for osteoblastoma of some irregular bones due to its
propensity for local recurrence. Garvayo et al performed an
en-bloc resection to treat cranial osteoblastoma and observed no
recurrence at 3 years follow-up (11). Mohammadi et al performed
total surgical resection for treating maxillary osteoblastoma in a
10-month-old infant and found no recurrence during 10 months of
follow-up (24). The treatment of
unresectable or extensive osteoblastoma is difficult. Osteoblastoma
can respond to denosumab. Yamaga et al reported a case of
unresectable osteoblastoma of the cervical spine that was
controlled with denosumab (25).
Wong et al reported a case of aggressive osteoblastoma with
a secondary aneurysmal bone cyst that was effectively treated with
denosumab (22). If there is
evidence of persistent aggressive behavior of the tumor or
recurrence, radiotherapy should be considered. Long-term imaging
surveillance after surgical resection is essential due to the risk
of local recurrence.
However, there were several limitations in our case
that should be noted. First, a intraoperative image was not
captured during autogenous iliac cancellous bone grafting. Second,
the 2-year follow-up period is relatively short, so we need to
conduct long-term follow-up to confirm that our surgical procedures
can achieve long-term good outcomes. Third, case report lack
representativeness, and the research conclusion of our case cannot
be summarized as general conclusion. In order to further study this
rare bone tumor with an uncommon site, more case reports are
needed.
In summary, our patient underwent thorough
intralesional curettage of the patella with subsequent autogenous
iliac cancellous bone grafting. This treatment was found to be
effective as there was no clinical and radiological evidence of
recurrence after a follow-up of 2 years. The accurate diagnosis of
osteoblastoma of the patella is challenging and important in
determining the appropriate treatment modality and prognosis.
Acknowledgements
Not applicable.
Funding
Funding: This work was supported by grants from Youth Science
and Technology Foundation of Gansu Province (grant nos. 20JR5RA588
and 21JR7RA014), the Key Research and Development Program of Gansu
Province (grant no. 21YF5FA154) and Military Training Injury
Prevention Program (grant no. 21XLS24).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
HZ, FL, and YQ performed the operation together. FL
designed the study, collected data and drafted the manuscript. YQ
assisted with study design, data collection and in the editing of
the manuscript. FL and YQ contributed to this paper equally. SZ and
XS made substantial contributions to data acquisition and
manuscript revision. HZ assisted with study design and in the
editing and revising of the manuscript. All authors read and
approved the final manuscript. HZ and FL confirm the authenticity
of all the raw data.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of the patient's data and images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
McLeod RA, Dahlin DC and Beabout JW: The
spectrum of osteoblastoma. AJR Am J Roentgenol. 126:321–325.
1976.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Kroon HM and Schurmans JJR: Osteoblastoma:
Clinical and radiologic findings in 98 new cases. Radiology.
175:783–790. 1990.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Lucas DR, Unni KK, McLeod RA, O'Connor MI
and Sim FH: Osteoblastoma: Clinicopathologic study of 306 cases.
Hum Pathol. 25:117–134. 1994.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Mercuri M and Casadei R: Patellar tumors.
Clin Orthop Relat Res. 389:35–46. 2001.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Song M, Zhang Z, Wu Y, Ma K and Lu M:
Primary tumors of the patella. World J Surg Oncol.
13(163)2015.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Sicard A, Touzard RC and Squalli S:
Osteoblastoma of the patella (author's transl). J Chir (Paris).
116:47–50. 1979.PubMed/NCBI(In Frence).
|
|
7
|
De Coster E, Van Tiggelen R, Shahabpour M,
Charels K, Osteaux M and Opdecam P: Osteoblastoma of the patella.
Case report and review of the literature. Clin Orthop Relat Res.
243:216–219. 1989.PubMed/NCBI
|
|
8
|
Shen CI, Shih HN, Hsu RW and Hsueh S:
Osteoblastoma of the patella: Case report. Chang Gung Med J.
24:269–273. 2001.PubMed/NCBI
|
|
9
|
Bhagat S, Sharma H, Bansal M and Reid R:
Presentation and outcome of primary tumors of the patella. J Knee
Surg. 21:212–216. 2008.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Zhong JJ, Han DY, Guo TS, Wang MY, Yang W,
Dai MJ, Wang JL and Guo LD: A case report of giga-osteoblastoma of
patella. Zhongguo Gu Shang. 23:619–620. 2010.PubMed/NCBI(In Chinese).
|
|
11
|
Garvayo M, Cossu G, Broome M, Maeder P,
Renella R, Maduri R, Daniel RT and Messerer M: Pediatric cranial
osteoblastoma: Technical note of surgical treatment and review of
the literature. . 67:383–390. 2021.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Chen K, Tian C, Yang S, Han S, Jiang L,
Wei F, Yuan H, Liu X and Liu Z: Typical and atypical radiographic
features of symptomatic osteoblastoma in the Spine. World
Neurosurg. 145:e209–e215. 2021.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Cao S, Chen K, Jiang L, Wei F, Liu X and
Liu Z: Intralesional marginal resection for osteoblastoma in the
mobile Spine: Experience from a single center. Front Surg.
9(838235)2022.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Berry M, Mankin H, Gebhardt M, Rosenberg A
and Hornicek F: Osteoblastoma: A 30-year study of 99 cases. J Surg
Oncol. 98:179–183. 2008.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Casadei R, Kreshak J, Rinaldi R, Rimondi
E, Bianchi G, Alberghini M, Ruggieri P and Vanel D: Imaging tumors
of the patella. Eur J Radiol. 82:2140–2148. 2013.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Si Z and Meng W: Multimodal imaging
evaluation and clinical progress of spinal osteoblastoma: A
comprehensive review. World Neurosurg. 170:28–37. 2023.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Jiang L, Liu X, Wang C, Yang SM, Liu C,
Wei F, Wu FL, Zhou H, Dang L and Liu ZJ: Surgical treatment options
for aggressive osteoblastoma in the mobile spine. Eur Spine J.
24:1778–1785. 2015.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Tang P, Zhang Y, Tian R and Yang G:
Osteoblastoma of the Rib Mimicking lymphomatous involvement on
18F-FDG PET/CT Imaging. Clin Nucl Med. 47:456–457. 2022.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Bertoni F, Unni KK, Lucas DR and McLeod
RA: Osteoblastoma with cartilaginous matrix. An unusual morphologic
presentation in 18 cases. Am J Surg Pathol. 17:69–74.
1993.PubMed/NCBI
|
|
20
|
Sharma V, Chew FS and Hoch B: Periosteal
osteoblastoma: Multimodal imaging of a rare neoplasm. Radiol Case
Rep. 4(329)2015.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Sharma R, Mahajan S and Gupta D:
Aggressive cranial osteoblastoma of the parietotemporo-occipital
bone: A case report and review of literature with special emphasis
on recurrence/residue. World Neurosurg. 142:255–267.
2020.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Wong K, Chantharasamee J, Nelson S,
Eckardt MA, Motamedi K, Hornicek FJ and Singh AS: Aggressive
osteoblastoma with a secondary aneurysmal bone cyst treated with
denosumab. Rare Tumors. 13(20363613211034710)2021.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Lucas DR: Osteoblastoma. Arch Pathol Lab
Med. 134:1460–1466. 2010.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Mohammadi F, Derakhshan S, Shooshtarizadeh
T and Sobhaninejad S: A rare case of maxillary osteoblastoma in a
10-month-old infant. Dent Res J (Isfahan). 19(13)2022.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Yamaga K, Kuwamoto S, Tanishima S,
Yamashita H, Asano N, Matsushita M, Akahori K, Osaki M, Hisaoka M
and Nagashima H: An unresectable osteoblastoma of the axis
controlled with denosumab. J Orthop Sci: Apr 22, 2022 (Epub ahead
of print).
|