Introduction
Breast cancer (BC) is the most common malignancy among women worldwide, with an estimated 2.3 million new cases diagnosed annually, accounting for one in four cancer cases among women. Despite advances in diagnosis and treatment, it remains a leading cause of cancer-related mortality and a major global public health challenge (1-3). Various reproductive and obstetric factors have been investigated to understand their association with BC risk (4), among which mode of delivery has recently garnered significant attention (5).
Cesarean section (CS) has become one of the most frequently performed surgical procedures worldwide, with rates rising far above the World Health Organization's recommended threshold of 10-15% in numerous regions. In 2021, global estimates indicated that >21% of all deliveries occurred by CS, a figure projected to reach nearly one-third of all births by 2030(6). The convergence of these two major health concerns-rising CS prevalence and persistent BC burden- underscores the importance of investigating whether delivery mode may influence long-term maternal cancer risk.
The potential link between cesarean delivery and BC risk is grounded in several biological and epidemiological hypotheses. One proposed mechanism is the difference in hormonal milieu between vaginal delivery (VD) and CS. Studies have indicated that levels of oxytocin, known to have antiproliferative effects on BC cells, are significantly lower during CS compared with VD (7,8). Additionally, fetal microchimeric cells (FMc)-fetal-derived cells that can persist in maternal tissues and circulation for decades after pregnancy-are transferred at higher levels during CS. These cells have been implicated in both protective and adverse outcomes regarding maternal malignancies (5).
Despite accumulating evidence on the association between CS and increased risk of malignancies, particularly uterine cancer (5), the link between CS and BC remains inconclusive. Some studies have reported a higher incidence of BC in women with a history of CS, while others have not found significant associations. For example, a study analyzing a large cohort found an increased risk of BC in women with CS, particularly in those diagnosed within one year postpartum (9). By contrast, another study failed to demonstrate a significant difference in BC risk between women who delivered vaginally and those who had a CS (5).
Moreover, CS has been associated with adverse prognostic factors in BC, such as increased rates of lymphovascular invasion and extracapsular extension, which are markers of more aggressive disease (7). CS association with adverse prognostic factors in BC is particularly evident in estrogen receptor-positive (ER+) cases, where patients with a history of CS were found to have a poorer prognosis compared with those without (10).
Given the rising prevalence of CS worldwide and the potential implications for long-term maternal health, it is crucial to comprehensively assess its relationship with BC. Accordingly, the present systematic review had two distinct aims: i) to evaluate whether a history of CS is associated with an increased incidence of BC, and ii) to investigate whether CS correlates with specific tumor characteristics or features of biological aggressiveness in affected women.
Materials and methods
Study design
The study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (11). The present systematic review has been registered in the International Prospective Register of Systematic Reviews (PROSPERO) with ID number CRD420251017783.
Search strategy and data sources
A comprehensive literature search was performed in PubMed (https://pubmed.ncbi.nlm.nih.gov/), Scopus (https://www.scopus.com/home.uri?zone=header&origin=sbrowse), Web of Science (https://clarivate.com/), Cochrane Library (https://www.cochranelibrary.com/) and Google Scholar (https://scholar.google.com/) from their inception to June 30, 2024. The search was limited to peer-reviewed articles published in English. No restrictions were applied regarding study population age or geographic location. The following Boolean search strategy was used in PubMed and adapted for other databases: (‘BC’ OR ‘breast neoplasm’ OR ‘mammary carcinoma’) AND (‘CS’ OR ‘caesarean section’ OR ‘C-section’ OR ‘mode of delivery’) AND (‘risk’ OR ‘incidence’ OR ‘prognosis’ OR ‘tumor characteristics’). Medical Subject Headings and equivalent controlled vocabulary terms were used where available. Reference lists of all included studies and relevant reviews were also manually searched to identify additional eligible articles.
Inclusion and exclusion criteria
Studies were considered eligible if they met the following criteria: i) Peer-reviewed original research articles published in English; ii) observational studies (cohort, case-control, or cross-sectional) that assessed the association between CS and BC; and iii) studies reporting outcomes related to BC incidence, risk factors, or prognosis among women with a history of CS.
Studies were excluded if they met any of the following criteria: i) Reviews, meta-analyses, case reports, or editorial articles; ii) studies that did not clearly differentiate between cesarean delivery and VD; iii) studies focusing solely on cancers other than BC; iv) studies with incomplete or unclear reporting of methodology or outcomes; v) non-human or preclinical studies; vi) studies with insufficient primary data or inaccessible full texts; vii) non-English language publications; and viii) studies with extremely small sample sizes, which limited statistical power.
PRISMA process. Identification
The initial search yielded 276 articles. After removing 76 duplicates, 200 unique records remained for screening.
Screening. The titles and abstracts of the 200 articles were independently screened by two reviewers (AD and FS) to assess relevance to the research question. After the initial screening, 138 articles were excluded for the following reasons: i) Not related to the association between CS and BC (n=89); ii) reviews, editorials, or meta-analyses (n=24); and iii) irrelevant study designs (for example, animal studies) (n=25). This resulted in 62 full-text articles being assessed for eligibility.
Eligibility. The 62 full-text articles were assessed based on predefined inclusion criteria. During this phase, 58 articles were excluded for the following reasons: i) Insufficient differentiation between delivery modes (n=19); ii) incomplete reporting of BC outcomes (n=26); and iii) low-quality studies (n=13).
Inclusion. Finally, 4 studies were deemed eligible and included in the systematic review. The flowchart of the study selection process is illustrated in Fig. 1.
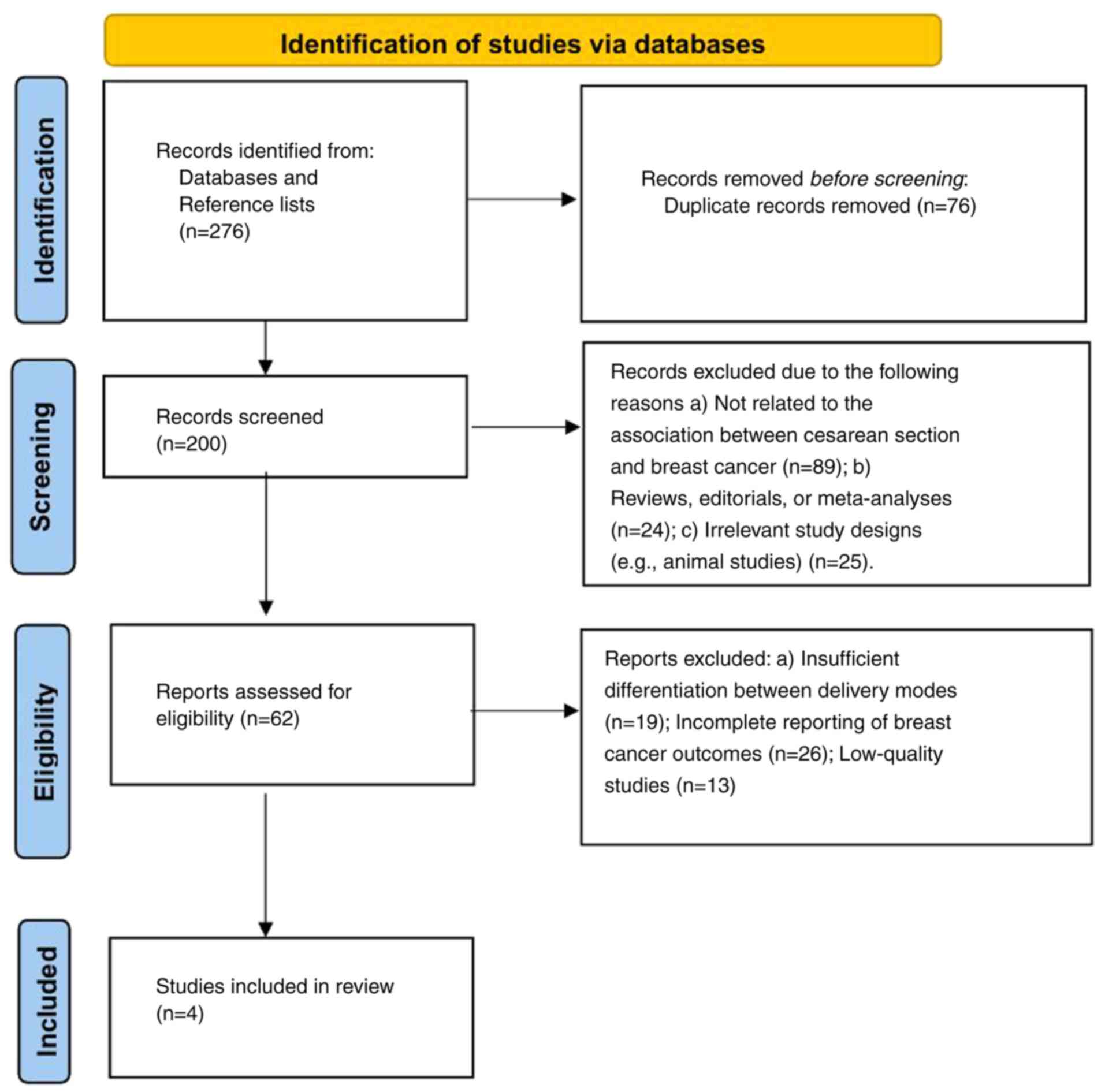 |
Figure 1
Flowchart of the study selection process.
|
Quality assessment
The quality of the included studies was assessed using the Newcastle-Ottawa Scale (NOS) (12) for cohort and case-control studies. Studies scoring ≥7 were considered high quality. The methodological quality of the four included studies ranged from 7 to 9 stars, indicating high quality overall (Table I). Detailed domain-level assessments are provided in Data S1.
 |
Table I
Quality assessment of the included studies.
|
Table I
Quality assessment of the included studies.
| First author/s, year |
Country |
Study design |
Selection (max 4) |
Comparability (max 2) |
Outcome (max 3) |
Total NOS score |
Quality rating |
(Refs.) |
| Schwarzman et al, 2023 |
Israel |
Population-based cohort |
4 |
2 |
3 |
9/9 |
High |
(5) |
| Kang et al, 2016 |
Korea |
Nation-wide cohort |
4 |
2 |
3 |
9/9 |
High |
(9) |
| Oğuz et al, 2021 |
Turkey |
Retrospective cohort |
3 |
2 |
2 |
7/9 |
High |
(7) |
| Kalan et al, (2010) |
Turkey |
Retrospective cohort |
3 |
1 |
2 |
7/9 |
High |
(10) |
Data extraction. Two independent reviewers (AD and FS) performed data extraction using a standardized data extraction form. The extracted data included study characteristics, such as the first author, year of publication, country, study design and sample size. Exposure and comparators were also noted, specifically the comparison between CS and VD or no CS. Outcome measures were recorded, including the incidence of BC, prognostic factors such as age at diagnosis and tumor characteristics, and risk estimates with odds ratios (ORs) and confidence intervals (CIs). Key findings, including numerical data related to incidence and risk and the statistical significance of associations, were carefully documented.
Statistical analysis
Meta-analyses were performed using Review Manager (RevMan, version 5.4; Cochrane Collaboration). Effect sizes were expressed as ORs with 95% CIs. Associations between CS and BC incidence, extracapsular extension and lymphovascular invasion were evaluated. All pooled analyses were conducted using a random-effects model to account for potential heterogeneity between studies. Statistical heterogeneity was assessed with Cochran's Q test (P<0.10 considered significant) and quantified using the I² statistic. Given the small number of included studies, publication bias could not be formally assessed using funnel plots. P<0.05 was considered to indicate a statistically significant difference.
Results
The present systematic review included 4 studies that investigated the association between CS and BC risk and prognosis. These studies were conducted in three countries: Israel, Turkey and Korea. The study designs comprised cohort studies, including one population-based cohort conducted in Israel, one nationwide cohort conducted in Korea, and two retrospective cohort studies conducted in Turkey.
The total sample size across the four studies was 1,492,962 women, with individual study populations ranging from 434 to 1,384,551 women. All studies compared the outcomes between women who underwent CS and those who had VD or no CS. Characteristics of the included studies are displayed in Table II. The systematic review evaluated the association between CS and BC risk by synthesizing data from various studies. The findings regarding the relationship between CS and BC were inconsistent across the studies.
|
Table II
Characteristics of the included studies.
|
Table II
Characteristics of the included studies.
| First author/s, year |
Country |
Study design |
Study sample |
Comparators |
Measurement regarding BC risk |
Key finding with numerical data |
(Refs.) |
| Schwarzman et al, 2023 |
Israel |
Population-based cohort |
105,992 women (14,150 CS only, 91,842 VD only) |
CS vs. VD |
Incidence of BC |
No significant association between CS and BC (0.64 per 1,000 patient-years for CS vs. 0.54 per 1,000 patient-years for VD; P=0.072) |
(5) |
| Kalan et al, 2010 |
Turkey |
Retrospective cohort |
985 women (90 CS, 895 no CS) |
CS vs. no CS |
Prognosis of BC |
Higher risk of lymphovascular invasion (70.3% vs. 48.2%, P=0.01) and extracapsular extension (45.9% vs. 25.1%, P=0.006) in CS group. CS history identified as an independent risk factor for lymphovascular invasion (OR: 2.28, 95% CI: 1.09-4.79, P=0.029) and extracapsular extension (OR: 1.45, 95% CI: 0.98-2.16, P=0.013). |
(10) |
| Oğuz et al, 2021 |
Turkey |
Retrospective cohort |
434 women (75 CS, 359 no CS) |
CS vs. no CS |
Prognosis of BC |
History of CS associated with younger age at diagnosis (42.8±8.7 years vs. 50.4±10.6 years, P<0.001), higher risk of extracapsular invasion in ER+ patients (p=0.023), and shorter time interval between last parity and BC diagnosis (11 vs. 23 years, P<0.001). |
(7) |
| Kang et al, 2016 |
Korea |
Nationwide cohort |
Group 1: 1,384,551 deliveries (317 BC), Group 2: 457,92 deliveries (655 BC) |
CS vs. no CS |
Incidence and risk of postpartum BC |
CS associated with increased risk of postpartum BC (Group 1: OR 1.237, 95% CI 0.986-1.553; Group 2: OR 1.211, 95% CI 1.034-1.418); older age (≥35 years) also significantly increased risk (Group 1: OR 2.003, 95% CI 1.567-2.560; Group 2: OR 2.777, 95% CI 2.356-3.274). |
(9) |
Some studies reported a slight increase in the risk of BC following CS. A nationwide cohort study conducted in Korea by Kang et al (9) observed a higher risk of postpartum BC among women who had undergone CS compared with those who had vaginal deliveries. The ORs reported were 1.237 [95% CI: 0.986-1.553] and 1.211 (95% CI :1.034-1.418) for different population groups. The study also highlighted that older maternal age (≥35 years) significantly increased the risk of postpartum BC, with an OR of 2.003 (95% CI 1.567-2.560). By contrast, a large population-based cohort study from Israel, conducted by Schwarzman et al (5), found no statistically significant association between CS and BC incidence, reporting similar rates between CS and VD groups (0.64 vs. 0.54 per 1,000 patient-years, P=0.072).
In addition to the variable risk association, some studies identified a link between CS and more aggressive BC features. A retrospective cohort study from Turkey by Oğuz et al (7) reported that women with a history of CS were diagnosed with BC at a younger age and had a higher risk of extracapsular invasion, particularly among patients with estrogen receptor-positive BC. Furthermore, they observed a shorter time interval between the last childbirth and the diagnosis of BC in women with a CS history. Another retrospective cohort study by Kalan et al (10) also demonstrated that CS was associated with a higher risk of lymphovascular invasion and extracapsular extension, identifying CS history as an independent risk factor for both conditions.
Meta-analysis. BC incidence
The present meta-analysis included two cohorts (5,9) and assessed the risk of BC incidence following CS vs. VD. The pooled analysis revealed a modest but statistically significant increased risk among women with a history of CS (OR=1.26, 95% CI: 1.07-1.47, P=0.004). Heterogeneity was negligible (I²=0%), indicating consistency between the two large studies (Fig. 2).
 |
Figure 2
Meta-analysis of the association between CS and BC incidence. Forest plot presenting pooled ORs with 95% CIs comparing women with a history of CS vs. vaginal delivery. The pooled estimate (OR=1.26, 95% CI: 1.07-1.47, P=0.004) indicates a modest but statistically significant increased risk of BC among women with a history of CS. Heterogeneity was negligible (I²=0%). CS, cesarean section; BC, breast cancer; OR, odds ratio; CI, confidence interval.
|
Extracapsular extension. The current meta-analysis combined two studies (7,10) assessing the association between mode of delivery and extracapsular extension in BC. The pooled OR demonstrated a significant association, with women who had undergone CS exhibiting higher odds of extracapsular extension compared with those with VD (OR=2.11, 95% CI: 1.42-3.15, P=0.0002). Heterogeneity was low (I²=20%), suggesting consistency across the included studies. These findings support the hypothesis that cesarean delivery may be linked to more aggressive BC features (Fig. 3).
 |
Figure 3
Meta-analysis of the association between CS and extracapsular extension in BC. Forest plot presenting pooled ORs with 95% CIs comparing women with a history of CS vs. vaginal delivery. The pooled estimate (OR=2.11, 95% CI: 1.42-3.15, P=0.0002) indicates that CS is significantly associated with increased odds of extracapsular extension in BC. Heterogeneity was low (I²=20%). CS, cesarean section; BC, breast cancer; OR, odds ratio; CI, confidence interval.
|
Lymphovascular invasion. The present meta-analysis evaluated the relationship between cesarean delivery and lymphovascular invasion. Again, the analysis was based on two studies (7,10). The pooled OR did not show a statistically significant association (OR=1.63, 95% CI: 0.69-3.89, P=0.27). Notably, heterogeneity was high (I²=82%, P=0.02), reflecting inconsistency between the two studies (Fig. 4).
 |
Figure 4
Meta-analysis of the association between CS and lymphovascular invasion in breast cancer. Forest plot presenting pooled ORs with 95% CIs comparing women with a history of CS vs. vaginal delivery. The pooled estimate (OR=1.63, 95% CI: 0.69-3.89, P=0.27) did not demonstrate a statistically significant association between CS and lymphovascular invasion. Heterogeneity was high (I²=82%), reflecting inconsistency between the included studies. CS, cesarean section; OR, odds ratio; CI, confidence interval.
|
Discussion
The present systematic review and meta-analysis provides the first pooled evidence on the potential association between CS and BC. Our results indicate a modest but statistically significant increased risk of BC incidence among women with a history of CS (OR=1.26, 95% CI: 1.07-1.47). In addition, the pooled analysis demonstrated more than a twofold increased risk of extracapsular extension (OR=2.11, 95% CI: 1.42-3.15), suggesting that CS may be linked not only to incidence but also to more aggressive tumor phenotypes. By contrast, no statistically significant association was observed between CS and lymphovascular invasion (OR=1.63, 95% CI: 0.69-3.89), and this analysis showed substantial heterogeneity.
The biological mechanisms linking CS with BC remain largely theoretical, as none of the four included studies directly evaluated mechanistic pathways. The retrospective cohorts from Turkey reported that women with a history of CS were diagnosed at a younger age and had more aggressive tumor characteristics, such as extracapsular extension and lymphovascular invasion (7,10). These findings suggest that CS could be associated with unfavorable tumor biology, although causality cannot be established. By contrast, the large population-based cohorts from Israel and Korea primarily assessed incidence rather than biological correlates, providing no mechanistic insight (5,9).
Several mechanisms could explain the potential link between CS and an increased risk of BC, as well as the association with more aggressive tumor characteristics. One of the most extensively discussed hypotheses is the role of fetal microchimerism, which refers to the persistence of fetal cells in the maternal bloodstream and tissues long after delivery. It has been observed that the concentration of FMc is significantly higher following CS than VD. These cells can persist in maternal tissues for decades, potentially exerting both protective and harmful effects. While FMc has been shown to participate in tissue repair and immune modulation, it may also promote carcinogenesis through immune evasion and aberrant cellular proliferation. Some studies have linked higher concentrations of FMc with breast and uterine cancers, although the evidence remains inconsistent (5,13-16).
Another potential mechanism is the alteration of hormonal profiles induced by CS. Unlike VD, which triggers a surge of oxytocin and stress hormones, elective CS may result in lower oxytocin levels. Oxytocin has been shown to exhibit antiproliferative effects on BC cells, reducing cell viability and inhibiting tumor growth. The absence of this hormonal boost during CS might reduce the protective effect against BC development (89). Furthermore, higher rates of postpartum lactation failure in women who undergo CS may reduce the long-term protective effects of breastfeeding against BC (17,18).
CS is associated with increased inflammatory responses, which may predispose women to carcinogenesis. The surgical trauma involved in CS triggers a cascade of pro-inflammatory cytokines, such as interleukins and tumor necrosis factors, which could contribute to tumor initiation or progression. Chronic low-grade inflammation has been linked to increased cancer risk and may play a role in BC development among women who undergo CS (19,20).
CS has been associated with a higher prevalence of obesity and metabolic syndrome in later life. Obesity itself is an established risk factor for BC, particularly in postmenopausal women. Increased adipose tissue contributes to elevated estrogen levels and chronic inflammation, creating a favorable environment for tumorigenesis. It is plausible that women who undergo CS are more likely to develop metabolic abnormalities, indirectly increasing their BC risk (21-23).
Women who undergo CS are often of advanced maternal age, have higher parity, or have pregnancy complications, all of which may indirectly influence cancer risk (24,25). Socioeconomic factors and healthcare access may also play a role in the association, as women opting for elective CS may differ systematically from those delivering vaginally (26).
However, these hypotheses remain speculative in the context of the present review. None of the included studies provided molecular or biomarker data to substantiate these pathways. Thus, while biological plausibility exists, the current evidence base does not allow definitive conclusions about causal mechanisms. Future prospective studies integrating epidemiological, clinical and molecular data are essential to clarify whether the observed associations reflect true biological effects or residual confounding. The mechanistic hypotheses linking CS to BC risk are demonstrated in Fig. 5.
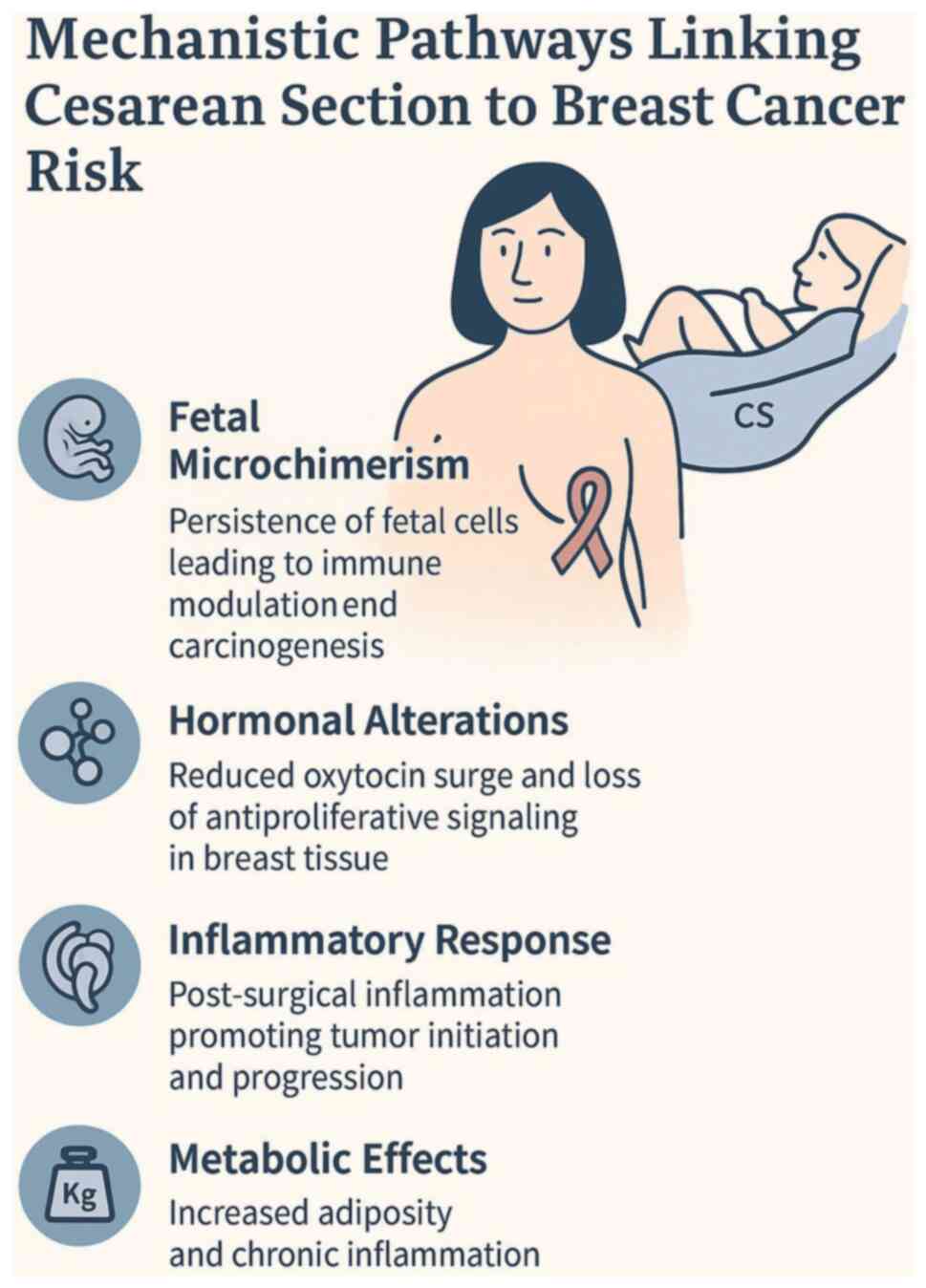 |
Figure 5
Mechanistic hypotheses linking cesarean section to breast cancer risk. CS, cesarean section.
|
Implications for clinical practice
Although the evidence remains inconclusive, the present review suggests that certain subgroups of women-particularly those of advanced maternal age and those with estrogen receptor-positive BC-may exhibit stronger associations between CS history and aggressive tumor features. For practicing clinicians, these findings underscore the importance of incorporating detailed obstetric history, including mode of delivery, into BC risk assessment and patient records. While cesarean delivery should not currently influence obstetric decision-making, clinicians managing women with BC may consider a history of CS as one of several contextual factors when evaluating prognosis, especially in the presence of lymphovascular invasion or extracapsular extension. At a broader level, the findings highlight the need for vigilance in long-term follow-up of women who undergo cesarean delivery, particularly when additional risk factors such as obesity, advanced maternal age, or family history of BC are present.
Limitations and future directions
The present review is limited by the small number of eligible studies, as only four met our predefined inclusion criteria despite a comprehensive search across multiple databases. This reflects the scarcity of high-quality research specifically addressing the association between CS and BC. Moreover, two of the included studies were relatively small retrospective cohorts from Turkey, which restricts statistical power and generalizability. Nonetheless, their findings provide valuable insights into tumor aggressiveness that complement the larger population-based cohorts. Taken together, the limited evidence highlights an important gap in the literature and underscores the urgent need for large, well-designed prospective studies to clarify this association. Future research should focus on mechanistic studies that elucidate the role of fetal microchimerism, hormonal changes and inflammatory responses following CS. Investigating the interaction between genetic predisposition and obstetric factors could also provide insight into the pathophysiological basis of the observed associations.
In conclusion, the association between CS and BC remains uncertain, but the present review highlights emerging evidence of a modest increase in BC incidence and possible links with more aggressive tumor phenotypes, particularly extracapsular extension. These associations appear more pronounced among women of advanced maternal age and in estrogen receptor-positive disease. While obstetric decision-making should continue to prioritize maternal and neonatal safety, clinicians should also recognize that a history of cesarean delivery may carry potential long-term oncological implications. Incorporating obstetric history into routine cancer risk assessment and ensuring vigilant postnatal surveillance in higher-risk populations, such as older women undergoing CS, may represent pragmatic steps while awaiting definitive prospective evidence. Future large-scale cohort and mechanistic studies are needed to clarify causality and determine whether CS history could be integrated into individualized BC risk stratification models.
Supplementary Material
Newcastle-Ottawa Scale (NOS) Assessment
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
FS and AD conceptualized the study. FS, AD, GK, AB and DAS made a substantial contribution to data interpretation and analysis and wrote and prepared the draft of the manuscript. FS and AD analyzed the data and provided critical revisions. FS and AD confirm the authenticity of all the raw data. All authors contributed to manuscript revision, read and approved the final version of the manuscript.
Ethics approval and consent to participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Use of artificial intelligence tools
During the preparation of this work, artificial intelligence tools were used to improve the readability and language of the manuscript, and subsequently, the authors revised and edited the content produced by the artificial intelligence tools as necessary, taking full responsibility for the ultimate content of the present manuscript.
References
|
1
|
Papalexis P, Georgakopoulou VE, Drossos PV, Thymara E, Nonni A, Lazaris AC, Zografos GC, Spandidos DA, Kavantzas N and Thomopoulou GE: Precision medicine in breast cancer (Review). Mol Clin Oncol. 21(78)2024.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Papalexis P, Georgakopoulou VE, Keramydas D, Vogiatzis R, Taskou C, Anagnostopoulou FA, Nonni A, Lazaris AC, Zografos GC, Kavantzas N and Thomopoulou GE: Clinical, histopathological, and immunohistochemical characteristics of predictive biomarkers of breast cancer: A retrospective study. Cancer Diagn Progn. 4:340–351. 2024.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Damaskos C, Garmpis N, Garmpi A, Nikolettos K, Sarantis P, Georgakopoulou VE, Nonni A, Schizas D, Antoniou EA, Karamouzis MV, et al: Investigational drug treatments for triple-negative breast cancer. J Pers Med. 11(652)2021.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Xie F, Liu L, Yang H, Liu M, Wang S, Guo J, Yu L, Zhou F, Wang F, Xiang Y, et al: The impact of reproductive factors on the risk of breast cancer by ER/PR and HER2: A multicenter case-control study in Northern and Eastern China. Oncologist. 27:e1–e8. 2022.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Schwarzman P, Sheiner E, Sergienko R and Kessous R: A history of cesarean section and future maternal long-term risk for neoplasms: A population-based cohort study. Arch Gynecol Obstet. 308:499–505. 2023.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Betran AP, Ye J, Moller AB, Souza JP and Zhang J: Trends and projections of caesarean section rates: Global and regional estimates. BMJ Glob Health. 6(e005671)2021.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Oguz SH and Utkan G: Reproductive factors and breast cancer prognosis: The possible role of cesarean delivery. Acta Medica. 52:29–36. 2021.
|
|
8
|
Lerman B, Harricharran T and Ogunwobi OO: Oxytocin and cancer: An emerging link. World J Clin Oncol. 9:74–82. 2018.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Kang EJ, Seo JH, Kim LY, Park GU, Oh MJ, Park PJ and Cho GJ: Pregnancy-associated risk factors of postpartum breast cancer in Korea: A nationwide health insurance database study. PLoS One. 11(e0168469)2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Kalan I, Turgut D, Aksoy S, Dede DS, Dizdar O, Ozisik Y and Altundag K: Clinical and pathological characteristics of breast cancer patients with history of cesarean delivery. Breast. 19:67–68. 2010.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al: The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 372(n71)2021.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Wells GA, Shea BJ, O'Connell D, Peterson J, Welch V, Losos M and Tugwell P: The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses.
|
|
13
|
Gadi VK and Nelson JL: Fetal microchimerism in women with breast cancer. Cancer Res. 67:9035–9038. 2007.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Fugazzola L, Cirello V and Beck-Peccoz P: Fetal cell microchimerism in human cancers. Cancer Lett. 287:136–141. 2010.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Dubernard G, Aractingi S, Oster M, Rouzier R, Mathieu MC, Uzan S and Khosrotehrani K: Breast cancer stroma frequently recruits fetal derived cells during pregnancy. Breast Cancer Res. 10(R14)2008.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Hromadnikova I, Kotlabova K, Pirkova P, Libalova P, Vernerova Z, Svoboda B and Kucera E: The occurrence of fetal microchimeric cells in endometrial tissues is a very common phenomenon in benign uterine disorders, and the lower prevalence of fetal microchimerism is associated with better uterine cancer prognoses. DNA Cell Biol. 33:40–48. 2014.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and breastfeeding: Collaborative reanalysis of individual data from 47 epidemiological studies in 30 countries, including 50302 women with breast cancer and 96973 women without the disease. Lancet. 360:187–195. 2002.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Hobbs AJ, Mannion CA, McDonald SW, Brockway M and Tough SC: The impact of caesarean section on breastfeeding initiation, duration and difficulties in the first four months postpartum. BMC Pregnancy Childbirth. 16(90)2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Cao Y, Nguyen LH, Tica S, Otegbeye E, Zong X, Roelstraete B, Chan AT, Warner BB, Stephansson O and Ludvigsson JF: Evaluation of birth by cesarean delivery and development of early-onset colorectal cancer. JAMA Netw Open. 6(e2310316)2023.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Hamidullah M, Cui H and Lei H: The role of chronic inflammation in the development of breast cancer. Cancers (Basel). 13(3918)2021.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Sogunle E, Masukume G and Nelson G: The association between caesarean section delivery and later life obesity in 21-24 year olds in an Urban South African birth cohort. PLoS One. 14(e0221379)2019.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Mohanty SS and Mohanty PK: Obesity as potential breast cancer risk factor for postmenopausal women. Genes Dis. 8:117–123. 2019.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Hurtado MD, Tama E, D'Andre S and Shufelt CL: The relation between excess adiposity and breast cancer in women: Clinical implications and management. Crit Rev Oncol Hematol. 193(104213)2024.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Cooke CM and Davidge ST: Advanced maternal age and the impact on maternal and offspring cardiovascular health. Am J Physiol Heart Circ Physiol. 317:H387–H394. 2019.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Hajiebrahimi M, Cnattingius S, Lambe M and Bahmanyar S: Pregnancy history and risk of premenopausal breast cancer-A nested case-control study. Int J Epidemiol. 45:816–824. 2016.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Hassan MM, Ameeq M, Fatima L, Naz S, Sikandar SM, Kargbo A and Abbas S: Assessing socio-ecological factors on caesarean section and vaginal delivery: An extended perspective among women of South-Punjab, Pakistan. J Psychosom Obstet Gynaecol. 44(2252983)2023.PubMed/NCBI View Article : Google Scholar
|














