Introduction
Based on GLOBOCAN 2022 data, breast cancer accounted
for 2.3 million new cases and 666,000 deaths globally, remaining
the most frequently diagnosed cancer and the leading cause of
cancer-related mortality among women (1). A notable proportion, ~3-10%, of cases
are diagnosed with distant metastases at the time of initial
diagnosi (2-4).
The disease comprises a heterogeneous group of subtypes, each with
distinct molecular features, clinical behavior, and prognostic
implications. Among these, hormone receptor-positive
(HR+) and human epidermal growth factor receptor 2
(HER2)-negative (HER2-) BC accounts for nearly 70% of
all BC cases (5).
In the metastatic setting, systemic therapy remains
the cornerstone of treatment, as recommended by current
international guidelines. For patients with metastatic
HR+/HER2- disease, the combination of
endocrine therapy and cyclin-dependent kinase 4/6 (CDK4/6)
inhibitors has emerged as the standard first-line approach,
supported by multiple large-scale clinical trials demonstrating
significant improvements in both progression-free and overall
survival (6-8).
The potential role of locoregional surgery in
patients with de novo stage IV BC remains a matter of
ongoing investigation. Several retrospective studies and a few
prospective randomized trials have assessed whether resection of
the primary tumor offers a survival advantage in this setting.
However, the results have been inconclusive; some studies report
improved outcomes in selected patient populations, whereas others
have failed to demonstrate a clear benefit (4,9-11).
BC exhibits significant biological diversity not
only between individuals but also within a single tumor.
Intratumoral heterogeneity (ITH), characterized by the coexistence
of genetically and phenotypically distinct subclones, has emerged
as a major challenge in oncology practice (12). This diversity within tumors
contributes to diagnostic uncertainty, therapeutic resistance and
disease recurrence (13).
Subpopulations with resistant features may persist and drive tumor
progression (14). A deeper
understanding of ITH is therefore essential for optimizing clinical
management and developing more effective, personalized therapeutic
approaches in BC.
In the present case report, two cases of de
novo metastatic HR+, HER2- BC in which an
initial favorable response was achieved with standard first-line
systemic therapy, were presented. Despite this apparent clinical
benefit, subsequent resection of the primary tumor revealed the
emergence of HER2-positive (HER2+) tumor clones that had
not been detected in baseline diagnostic samples. These findings
prompted a change in systemic treatment strategy and illustrate how
limited initial sampling may fail to capture clinically actionable
subclonal populations or to fully reflect tumor biology under
therapeutic pressure, as it remains uncertain whether these
HER2+ clones were pre-existing or arose as a result of
treatment-driven clonal selection.
Although intratumoral and intertumoral heterogeneity
and receptor discordance are well recognized in BC, most prior
studies have focused on receptor changes occurring after disease
progression or metastatic relapse. By contrast, the present cases
demonstrate that biologically relevant HER2+ clones may
be present or emerge even in patients with HR+,
HER2- metastatic disease who show an early and favorable
response to systemic therapy. These observations underscore the
potential clinical consequences of ITH and highlight the need for
individualized and dynamic treatment strategies, even in patients
with initial treatment sensitivity.
Materials and methods
Pathology assessment
Initial diagnostic core needle biopsy specimens were
considered adequate for histopathological evaluation in both cases
and included multiple tumor-containing cores. Tissue samples were
fixed in 10% neutral buffered formalin at room temperature for 6-24
h, routinely processed, and embedded in paraffin. Sections of 4-µm
thickness were prepared for hematoxylin-eosin staining and
immunohistochemical (IHC) analyses.
IHC staining was performed using validated primary
antibodies and standard automated staining protocols in the
institutional pathology laboratory. Visualization was achieved
using a horseradish peroxidase-based detection system with
diaminobenzidine (DAB) as the chromogen. Slides were evaluated
under a light microscope by experienced breast pathologists. HER2
status was evaluated by IHC and, when indicated, by silver in
situ hybridization (SISH), and interpreted according to the
2018 ASCO/CAP guidelines (15) and
subsequent updates applicable at the time of diagnosis (16).
Surgical specimens were sampled according to routine
pathological protocols, with multiple representative
tumor-containing blocks obtained from different areas of the
residual primary tumor. HER2 IHC was performed on selected blocks
showing viable invasive carcinoma, and HER2 status was further
evaluated by SISH in areas of interest. HER2 assessment was
conducted in two independent pathology laboratories to confirm the
findings.
Estrogen receptor (ER) and progesterone receptor
(PR) status were assessed by IHC and interpreted according to
ASCO/CAP guidelines, with tumors considered positive when ≥1% of
tumor cell nuclei showed immunoreactivity (17). Ki-67 proliferation index was
evaluated by IHC and reported as the percentage of positively
stained tumor cell nuclei in areas of highest labeling (hot spots),
using standard scoring practice.
IHC analysis was performed on formalin-fixed,
paraffin-embedded tissue sections using validated monoclonal
antibodies according to standardized protocols. HER2 IHC was
conducted on automated staining platforms with appropriate
controls. HER2 expression was scored as 0, 1+, 2+, or 3+ based on
the intensity and completeness of circumferential membranous
staining in invasive tumor cells, in accordance with ASCO/CAP
guidelines. A score of 3+ (>10% of tumor cells with strong,
complete membranous staining) was considered positive, whereas
scores of 0 and 1+ were considered negative. Cases with equivocal
HER2 expression (2+) underwent reflex evaluation by in situ
hybridization.
Assessment of metastatic disease
In both cases, bone metastases were defined based on
imaging findings, without histopathological confirmation. No biopsy
of bone lesions was performed, and the diagnosis of metastatic
disease was established through radiologic, clinical
correlation.
Case report
Case 1
A 41-year-old premenopausal woman presented with a
palpable left breast mass. Imaging and biopsy confirmed invasive
ductal carcinoma (IDC), grade 3, ER-positive (95%), PR-positive
(90%), HER2- (score 0), with a Ki-67 index of 45%.
PET/CT showed metastatic bone involvement in C5 and C7 vertebrae.
She received systemic therapy with ribociclib (600 mg/day, D1-21),
letrozole (2.5 mg/day), goserelin (3.6 mg/month) and denosumab (120
mg/month). PET/CT showed partial regression of breast and axillary
lesions and near-complete resolution of vertebral metastases.
Following 18 months of disease control, the tumor board recommended
surgery for the residual breast tumor.
The patient underwent left breast-conserving surgery
(BCS) and sentinel lymph node biopsy (SLNB). The tumor measured 7
mm and was identified as grade 3 IDC. IHC evaluation showed ER
positivity of 70%, PR negativity (0%) and strong HER2
overexpression (score 3+). Only 1 of the 3 sentinel lymph nodes was
tumor positive. HER2 status was assessed in two independent
pathology laboratories and consistently reported as 3+. Further
confirmation with SISH demonstrated HER2 gene amplification
(SISH-positive).
To address potential ITH, the surgical specimen was
extensively sampled, with multiple representative tumor-containing
blocks obtained from spatially distinct areas. HER2 IHC was
performed on several blocks showing viable invasive carcinoma, with
consistent HER2 positivity across sampled regions; areas of strong
membranous staining were further evaluated by SISH. Re-evaluation
of the initial core needle biopsy confirmed HER2 negativity (score
0), consistent with the original diagnostic report. Representative
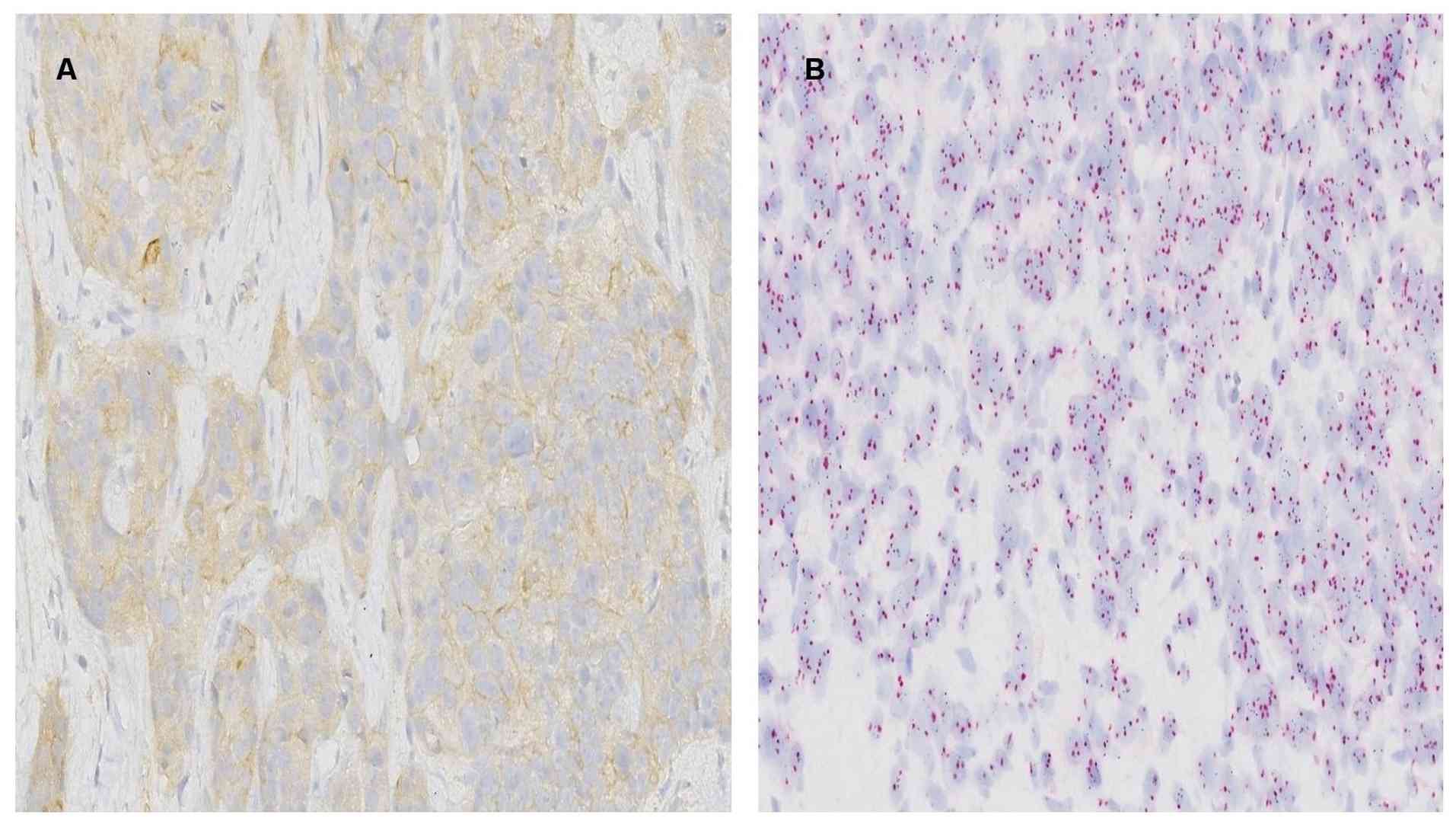
images of IHC and SISH analyses from the initial biopsy and
postoperative surgical specimen are shown in Fig. 1A-D.
 | Figure 1HER2 evaluation in the initial core
needle biopsy and postoperative surgical specimen in Case 1.
Representative HER2 IHC and SISH images from the initial core
needle biopsy and the postoperative surgical specimen. (A) HER2 IHC
showing negative staining in the initial core needle biopsy
(original magnification, x400). (B) HER2 IHC demonstrating strong
membranous positivity (score 3+) in the postoperative surgical
specimen (original magnification, x400). (C) SISH analysis showing
no HER2 amplification in the initial core needle biopsy (original
magnification, x1,000, oil immersion). (D) SISH analysis
demonstrating HER2 amplification in the postoperative surgical
specimen (original magnification, 1,000, oil immersion). HER2,
human epidermal growth factor receptor 2; IHC,
immunohistochemistry; SISH, silver in situ
hybridization. |
Following multidisciplinary team (MDT) discussion,
it was decided to continue trastuzumab therapy until disease
progression or unacceptable toxicity. Concurrently, goserelin and
letrozole were maintained as part of the endocrine treatment
regimen. The patient had no radiologic evidence of active disease
at the last follow-up (28 months) and remains under active
surveillance.
Case 2
A 51-year-old perimenopausal woman with low back
pain. Lumbar MRI was performed and revealed pathological signal
changes in the L2, L3, S1 and S3 vertebral bodies, consistent with
bone metastases. Breast ultrasound revealed a 1.5-cm solid lesion
in the right breast and a 10-mm right axillary lymph node. Biopsy
confirmed IDC, grade 2, with ER 100%, PR 85%, HER2 score 0 and
Ki-67 42%. Staging PET/CT revealed skeletal metastases, a right
breast primary lesion, and metastatic lymph nodes in the right
axilla and internal mammary chain. The patient received
radiotherapy to the involved bone sites and was started on systemic
therapy with ribociclib (600 mg/day), letrozole (2.5 mg/day),
leuprolide (3.75 mg/month) and denosumab (120 mg/month). PET/CT
demonstrated partial regression of the primary breast lesion and
axillary lymph nodes, along with near-complete regression of bone
metastases after 3 months. Ater 22 months of treatment, PET/CT
showed a stable 6-mm lesion in the right breast and inactive
skeletal metastases. Given the sustained response without
progression, the case was discussed in the MDT, and surgery was
recommended and the patient underwent right BCS with SLNB.
Postoperative pathology revealed multifocal grade 3
IDC with neuroendocrine differentiation, with tumor foci ranging
from 0.1-0.5 cm. IHC showed ER 70%, PR 0%, HER2 score 2+, Ki-67 4%,
and positivity for synaptophysin and chromogranin. HER2 status was
further evaluated by SISH in two independent pathology centers,
both confirming HER2 amplification. Postoperative histopathological
images were not available for this case, as the surgical specimen
was evaluated externally.
Due to HER2 discordance, MDT opted to continue the
CDK4/6-based regimen. After 7 months, PET/CT showed new liver and
vertebral metastases. Liver biopsy confirmed IDC with
neuroendocrine differentiation, ER 60%, HER2 IHC 1+, and
SISH-negative findings. According to current ASCO/CAP guidelines,
this profile was considered HER2- (HER2-low) (16). Despite this finding, the case was
included in the present series because HER2 amplification was
detected in the postoperative primary tumor specimen, indicating
discordant HER2 status between the initial biopsy and the resected
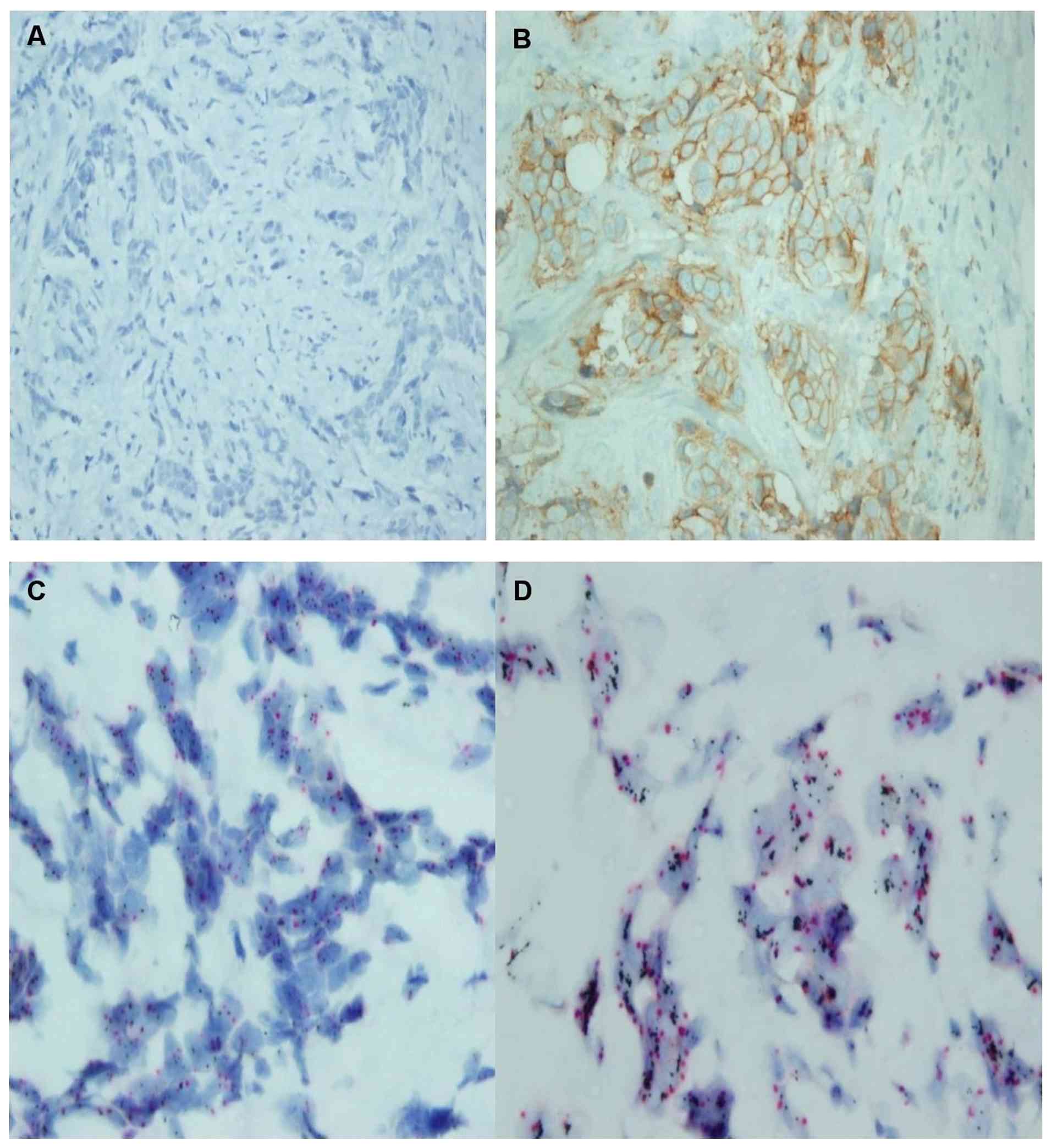
tumor. IHC and SISH images from the liver metastasis biopsy are
shown in Fig. 2A and B.
Although the liver biopsy demonstrated a HER2-low
phenotype (IHC 1+, SISH-negative), docetaxel, trastuzumab and
pertuzumab were initiated, along with selective internal radiation
therapy, based on the presence of a HER2 3+ amplified clone
identified in the postoperative primary tumor specimen, following
MDT discussion. Following eight cycles, partial hepatic response
was achieved. Docetaxel was discontinued due to toxicity, and
treatment continued with trastuzumab, pertuzumab and fulvestrant.
Despite this, central nervous system CNS and liver progression
occurred.
Carboplatin/gemcitabine was initiated after cranial
radiotherapy and resulted in a partial hepatic response; however,
disease progression with new liver lesions occurred after six
cycles. In the context of disease progression under dual HER2
blockade and limited benefit from platinum-based chemotherapy, and
based on the HER2-low status (IHC 1+), trastuzumab deruxtecan
(T-DXd) was initiated in line with evidence from the
DESTINY-Breast04(18) and
DESTINY-Breast06(19) trials.
Liver function subsequently improved, and follow-up PET/CT is
pending. The key clinical milestones and treatment sequences of the
two reported cases are summarized in Table I.
 | Table ISimplified clinical timeline of the
two cases. |
Table I
Simplified clinical timeline of the
two cases.
| Timeline step | Case 1 | Case 2 |
|---|
| Diagnosis |
HR+/HER2- breast
cancer with bone-only metastases |
HR+/HER2- breast
cancer with bone-only metastases |
| First-line systemic
therapy | CDK4/6 inhibitor +
endocrine therapy | CDK4/6 inhibitor +
endocrine therapy |
| Best response | Sustained disease
control | Sustained disease
control |
| Surgery | Performed after
response | Performed after
response |
| Postoperative
pathology | HER2-positive
subclone identified | HER2-positive
subclone identified |
| Initial post-surgical
management | Anti-HER2 therapy
added | CDK4/6-based therapy
continued |
| Disease
progression/reassessment | - | Liver metastasis →
liver biopsy (HER2-low) |
| Subsequent systemic
therapy | - | Dual HER2 blockade
(THP) |
| Further
treatment | - | Chemotherapy |
| Later-line
therapy | - | Trastuzumab
deruxtecan (T-DXd) |
| Follow-up | No radiologic
evidence of active disease | Ongoing
follow-up |
Discussion
The role of locoregional surgery in de novo
stage IV BC remains controversial. While retrospective studies have
suggested a potential survival benefit in selected patients with
low tumor burden, these findings are limited by inherent selection
bias (20). By contrast, most
randomized controlled trials have failed to demonstrate a
significant survival advantage associated with surgery (21-23).
However, a recent meta-analysis suggested that patients with
hormone receptor-positive, HER2- tumors in selected
clinical scenarios may derive benefit from locoregional treatment,
supporting a hypothesis-generating role for surgery rather than a
general treatment strategy (4).
Additionally, the prospective BOMET MF 14-01 study demonstrated a
significant survival benefit from locoregional surgery in patients
with de novo stage IV BC presenting with bone-only
metastases, a finding that further informs discussion in selected
patient populations (10). In this
context, locoregional surgery was performed in two patients with
de novo metastatic hormone receptor-positive,
HER2- BC with bone-only metastases who had achieved a
favorable response to first-line systemic therapy. In these cases,
surgery provided local control and enabled a more detailed
pathological assessment of the primary tumor.
BC is widely recognized for its pronounced
heterogeneity, which plays a pivotal role in tumor progression,
therapeutic response and clinical outcomes. This heterogeneity
manifests at two distinct levels: Intertumoral heterogeneity, which
refers to the biological differences between tumors of different
patients or between primary and metastatic lesions; and ITH, which
denotes the coexistence of diverse subclonal populations within a
single tumor (24). Both forms of
heterogeneity contribute to the complexity of disease management
and highlight the need for individualized treatment strategies.
In clinical practice, the significance of this
biological complexity becomes particularly evident in metastatic
BC. When disease progression occurs, repeat biopsy is typically
recommended to assess intertumoral heterogeneity, such as receptor
status discordance between primary and metastatic sites (25). However, identifying ITH is
considerably more challenging (26). While broader tumor sampling may
provide additional biological information, surgical resection is
not routinely performed in metastatic disease and is not intended
as a tool to reveal ITH; rather, it may be feasible only in
selected cases. In the present study, HER2+ subclones
were identified only after surgical resection in both cases.
Two cases of hormone receptor-positive,
HER2- de novo metastatic BC with bone metastases,
were presented. After a favorable response to first-line systemic
treatment with endocrine therapy and CDK4/6 inhibitors, both
patients had persistent residual primary breast tumors. To achieve
local control and obtain a more comprehensive pathological
assessment, surgical resection of the primary lesions was
performed. Postoperative histopathological analysis revealed
unexpected ITH, specifically the presence of HER2+
subclones that had not been detected in the initial diagnostic
biopsies. These findings prompted a change in therapeutic
strategy.
In the first case, although the patient had shown a
favorable systemic response to CDK4/6 inhibitor therapy, it was
decided to continue trastuzumab in addition to endocrine therapy to
target the HER2+ component identified in the surgical
specimen. The patient has no radiologic evidence of active disease
and remains under follow-up.
In the second case, CDK4/6 inhibitor therapy was
initially continued due to the favorable clinical response.
However, the patient later developed progressive disease with new
liver metastases. A biopsy of the liver lesion revealed a HER2-low
phenotype (IHC score 1+). Despite this, based on the
HER2+ clone found in the breast tumor, dual HER2
blockade with trastuzumab and pertuzumab was initiated.
Unfortunately, the patient did not respond to this approach. Local
therapy was required to control the liver lesion, and systemic
chemotherapy was resumed as the main treatment strategy.
Subsequently, considering the HER2-low phenotype in the liver
metastasis, treatment was continued with T-DXd, a novel option for
HER2-low disease. In this setting, identification of a HER2-low
phenotype in the metastatic lesion provided a rationale for
considering trastuzumab deruxtecan, in line with emerging evidence
supporting the role of antibody-drug conjugates in HER2-low
metastatic BC (17,18). Overall, this treatment sequence
illustrates that, in cases with HER2 discordance, therapeutic
decisions may be guided by reassessment of tumor biology.
An important consideration in interpreting these
findings is whether the observed HER2+ subclones reflect
true biological evolution under systemic therapy or sampling
limitations of the initial core needle biopsy. In both cases, HER2
positivity was identified only in the surgical specimen and not in
the initial biopsy, precluding a definitive distinction between
these mechanisms.
This issue is particularly evident in Case 2, where
HER2 amplification detected in the surgical specimen was followed
by a HER2-low profile in a subsequent liver biopsy, together with
limited clinical benefit from anti-HER2 therapy. This pattern may
reflect spatial heterogeneity, temporal changes in tumor biology
under treatment-related selective pressure, or technical
variability in HER2 assessment across different tissue samples.
Given the case-based nature of this report, it remains unclear
which mechanism predominated; however, these findings underscore
the dynamic and context-dependent nature of HER2 expression in
metastatic BC.
These two cases highlight two important aspects:
First, the decision to perform surgery in metastatic BC following a
favorable response to initial systemic treatment; and second, the
unexpected identification of ITH, specifically HER2+
subclones, through pathological evaluation of the surgical
specimens. To the best of our knowledge, no previous studies have
described the emergence of HER2+ subclones revealed
solely by surgery after systemic therapy in
HR+/HER2- de novo metastatic BC.
Although ITH is a well-recognized biological phenomenon, the
emergence of HER2+ subclones after an initial favorable
response to endocrine-based therapy in metastatic
HR+/HER2- BC, identified following surgery,
presents a therapeutic challenge. The present cases emphasize how
such findings, revealed only through more comprehensive tumor
assessment, may complicate treatment decisions and underscore the
dynamic nature of tumor biology in HR+/HER2-
de novo metastatic BC.
In conclusion, these two cases highlight the
potential clinical impact of ITH in de novo metastatic
HR-positive/HER2- BC. While limited by their case-based
nature, they serve as a practical reminder that tumor biology may
be underestimated by initial diagnostic sampling. Reassessment of
tumor characteristics, when feasible, may offer additional
clinically relevant information and should be considered in
selected scenarios where it may help inform treatment
decisions.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
ZB and ZHT contributed to the conception, design and
supervision of the study. ZB and EÇ collected and analyzed the
clinical data. CSW performed and interpreted the pathological
analysis. ZB and ZHT confirm the authenticity of all the raw data.
All authors read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patients for publication of their clinical details and associated
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Laversanne M, Sung H, Ferlay J,
Siegel RL, Soerjomataram I and Jemal A: Global cancer statistics
2022: GLOBOCAN estimates of incidence and mortality worldwide for
36 cancers in 185 countries. CA Cancer J Clin. 74:229–263.
2024.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Lobbezoo DJ, van Kampen RJ, Voogd AC,
Dercksen MW, van den Berkmortel F, Smilde TJ, van de Wouw AJ,
Peters FP, van Riel JM, Peters NA, et al: Prognosis of metastatic
breast cancer subtypes: The hormone receptor/HER2-positive subtype
is associated with the most favorable outcome. Breast Cancer Res
Treat. 141:507–514. 2013.PubMed/NCBI View Article : Google Scholar
|
|
3
|
den Brok WD, Speers CH, Gondara L, Baxter
E, Tyldesley SK and Lohrisch CA: Survival with metastatic breast
cancer based on initial presentation, de novo versus relapsed.
Breast Cancer Res Treat. 161:549–556. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Zhou W, Yue Y, Xiong J, Li W and Zeng X:
The role of locoregional surgery in de novo stage IV breast cancer:
A meta-analysis of randomized controlled trials. Cancer Treat Rev.
129(102784)2024.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Giaquinto AN, Sung H, Newman LA, Freedman
RA, Smith RA, Star J, Jemal A and Siegel RL: Breast cancer
statistics 2024. CA Cancer J Clin. 74:477–495. 2024.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Lu YS, Im SA, Colleoni M, Franke F, Bardia
A, Cardoso F, Harbeck N, Hurvitz S, Chow L, Sohn J, et al: Updated
overall survival of ribociclib plus endocrine therapy versus
endocrine therapy alone in pre- and perimenopausal patients with
HR+/HER2- advanced breast cancer in MONALEESA-7: A phase III
Randomized clinical trial. Clin Cancer Res. 28:851–859.
2022.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Sledge GW Jr, Toi M, Neven P, Sohn J,
Inoue K, Pivot X, Burdaeva O, Okera M, Masuda N, Kaufman PA, et al:
The effect of abemaciclib plus fulvestrant on overall survival in
hormone receptor-positive, ERBB2-Negative breast cancer that
progressed on endocrine therapy-MONARCH 2: A Randomized clinical
trial. JAMA Oncol. 6:116–124. 2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Cristofanilli M, Rugo HS, Im SA, Slamon
DJ, Harbeck N, Bondarenko I, Masuda N, Colleoni M, DeMichele A, Loi
S, et al: Overall survival with palbociclib and fulvestrant in
women with HR+/HER2- ABC: Updated exploratory analyses of PALOMA-3,
a double-blind, phase III Randomized study. Clin Cancer Res.
28:3433–3442. 2022.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Huang Z, Zhou X, Tong Y, Zhu L, Zhao R and
Huang X: Surgery for primary tumor benefits survival for breast
cancer patients with bone metastases: A large cohort retrospective
study. BMC Cancer. 21(222)2021.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Soran A, Dogan L, Isik A, Ozbas S,
Trabulus DC, Demirci U, Karanlik H, Soyder A, Dag A, Bilici A, et
al: The effect of primary surgery in patients with de novo stage IV
breast cancer with bone metastasis only (Protocol BOMET MF 14-01):
A multi-center, prospective registry study. Ann Surg Oncol.
28:5048–5057. 2021.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Tinterri C, Sagona A, Barbieri E, Di Maria
Grimaldi S, Jacobs F, Zambelli A, Trimboli RM, Bernardi D, Vinci V
and Gentile D: Loco-regional treatment of the primary tumor in de
novo metastatic breast cancer patients undergoing front-line
chemotherapy. Cancers (Basel). 14(6237)2022.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Zardavas D, Irrthum A, Swanton C and
Piccart M: Clinical management of breast cancer heterogeneity. Nat
Rev Clin Oncol. 12:381–394. 2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Vitale I, Shema E, Loi S and Galluzzi L:
Intratumoral heterogeneity in cancer progression and response to
immunotherapy. Nat Med. 27:212–224. 2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Gu TQ, Xiao YL and Shao ZM: Intratumor
heterogeneity in breast cancer: Tracing its origins and translating
findings into clinical practice. Precision Medicine and
Engineering. 1(100006)2024.
|
|
15
|
Wolff AC, Hammond MEH, Allison KH, Harvey
BE, Mangu PB, Bartlett JMS, Bartlett JMS, Bilous M, Ellis IO,
Fitzgibbons P, et al: Human epidermal growth factor receptor 2
testing in breast cancer: American society of clinical
oncology/college of American pathologists clinical practice
guideline focused update. J Clin Oncol. 36:2105–2122.
2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Wolff AC, Somerfield MR, Dowsett M,
Hammond MEH, Hayes DF, McShane LM, Saphner TJ, Spears PA and
Allison KH: Human epidermal growth factor receptor 2 testing in
breast cancer: ASCO-College of American pathologists guideline
update. J Clin Oncol. 41:3867–3872. 2023.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Allison KH, Hammond MEH, Dowsett M,
McKernin SE, Carey LA, Fitzgibbons PL, Hayes DF, Lakhani SR,
Chavez-MacGregor M, Perlmutter J, et al: Estrogen and progesterone
receptor testing in breast cancer: ASCO/CAP guideline update. J
Clin Oncol. 38:1346–1366. 2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Modi S, Jacot W, Yamashita T, Sohn J,
Vidal M, Tokunaga E, Tsurutani J, Ueno NT, Prat A, Chae YS, et al:
Trastuzumab deruxtecan in previously treated HER2-Low advanced
breast cancer. N Engl J Med. 387:9–20. 2022.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Bardia A, Hu X, Dent R, Yonemori K,
Barrios CH, O'Shaughnessy JA, Wildiers H, Pierga JY, Zhang Q, Saura
C, et al: Trastuzumab deruxtecan after endocrine therapy in
metastatic breast cancer. N Engl J Med. 391:2110–2122.
2024.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Lu S, Wu J, Fang Y, Wang W, Zong Y, Chen
X, Huang O, He JR, Chen W, Li Y, et al: The impact of surgical
excision of the primary tumor in stage IV breast cancer on
survival: a meta-analysis. Oncotarget. 9:11816–11823.
2017.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Badwe R, Hawaldar R, Nair N, Kaushik R,
Parmar V, Siddique S, Budrukkar A, Mittra I and Gupta S:
Locoregional treatment versus no treatment of the primary tumour in
metastatic breast cancer: An open-label randomised controlled
trial. Lancet Oncol. 16:1380–1288. 2015.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Khan SA, Zhao F, Goldstein LJ, Cella D,
Basik M, Golshan M, Julian TB, Pockaj BA, Lee CA, Razaq W, et al:
Early local therapy for the primary site in de novo stage IV breast
cancer: Results of a Randomized clinical trial (EA2108). J Clin
Oncol. 40:978–987. 2022.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Fitzal F, Bjelic-Radisic V, Knauer M,
Steger G, Hubalek M, Balic M, Singer C, Bartsch R, Schrenk P,
Soelkner L, et al: Impact of breast surgery in primary metastasized
breast cancer: outcomes of the prospective Randomized phase III
ABCSG-28 POSYTIVE trial. Ann Surg. 269:1163–1169. 2019.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Visvader JE: Cells of origin in cancer.
Nature. 469:314–322. 2011.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Holdaway IM and Bowditch JV: Variation in
receptor status between primary and metastatic breast cancer.
Cancer. 52:479–485. 1983.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Ramón Y, Cajal S, Sesé M, Capdevila C,
Aasen T, De Mattos-Arruda L, Diaz-Cano SJ, Hernández-Losa J and
Castellví J: Clinical implications of intratumor heterogeneity:
Challenges and opportunities. J Mol Med (Berl). 98:161–177.
2020.PubMed/NCBI View Article : Google Scholar
|