Introduction
Lung cancer (LC) remains the leading cause of
cancer-related mortality worldwide (1). Small cell LC (SCLC), accounting for
~15% of all LCs (2), is classified
into limited-stage and extensive-stage (ES-SCLC) according to the
VALSG staging system. The five-year relative survival rate for SCLC
is ~6.4% (3), most patients are
diagnosed at the extensive stage (4). For over 30 years, platinum plus
etoposide has been the standard first-line treatment (5). In the latest NCCN guidelines
(6), atezolizumab and durvalumab,
as immune checkpoint inhibitors (ICIs) combined with
platinum-etoposide, have been officially established as the
preferred first-line treatment options for ES-SCLC.
During chemotherapy for patients with LC, various
adverse reactions often occur. Glucocorticoids, such as
dexamethasone, have anti-inflammatory, immunosuppression and
anti-allergic effects (7) and may
help reduce chemotherapy-related adverse reactions, thus being
widely used in chemotherapy regimens for patients with LC (8). Although dexamethasone is routinely
used for antiemesis, the optimal timing-prophylactic versus
symptom-triggered-remains undefined. In clinical practice, there
are two main strategies: One is prophylactic use, where
dexamethasone is routinely administered before the initiation of
chemotherapy or prior to the onset of adverse reactions, with the
expectation that early intervention will reduce the incidence and
severity of adverse reactions; the other is episodic use, where
symptomatic treatment is only provided after patients develop clear
symptoms of adverse reactions (such as severe nausea and vomiting
and drug allergic reactions). Each of these strategies has its own
considerations: Prophylactic use may reduce the suffering caused by
adverse reactions, but long-term or excessive use may increase the
risk of infections, blood glucose fluctuations and other side
effects; while episodic use can avoid unnecessary drug exposure, it
may lead to the aggravation of adverse reactions due to delayed
intervention, and even affect the progress of chemotherapy. It is
precisely due to the uncertainty in the timing of dexamethasone
administration and the controversies surrounding the balance
between efficacy and safety of different administration strategies
(8,9) that the present study intended to
adopt the prophylactic dexamethasone administration regimen. By
systematically observing its efficacy in controlling adverse
reactions, patient tolerance and related safety indicators during
platinum-etoposide chemotherapy, the present study aimed to provide
clinical evidence for clarifying the optimal timing of
dexamethasone administration in LC chemotherapy.
Materials and methods
General data
The present study retrospectively collected data of
289 patients with SCLC admitted to the First Affiliated Hospital of
Anhui Medical University (Hefei, China) from August 2022 to
December 2024. After excluding 116 cases not meeting the inclusion
criteria, 57 cases meeting the exclusion criteria and 13 cases lost
to follow-up, 103 patients were finally included. Among them, 63
patients who received glucocorticoids during chemotherapy were
assigned to the hormone group and 40 patients who did not receive
glucocorticoids were assigned to the control group. The present
study aimed to compare the differences in treatment outcomes,
adverse reaction rates and quality of life between the two
groups.
Inclusion criteria were as follows: i) Patients aged
>18 years; ii) newly diagnosed ES-SCLC confirmed by histology or
cytology; iii) Eastern Cooperative Oncology Group (ECOG) score ≤2;
iv) expected survival >2 months; v) first-line treatment drugs
containing etoposide plus platinum.
Exclusion criteria were as follows: i) Previous
surgery or radiotherapy; ii) allergy to glucocorticoids or
contraindications for glucocorticoid use; iii) concurrent other
malignancies; iv) severe liver or kidney dysfunction; v) pregnant
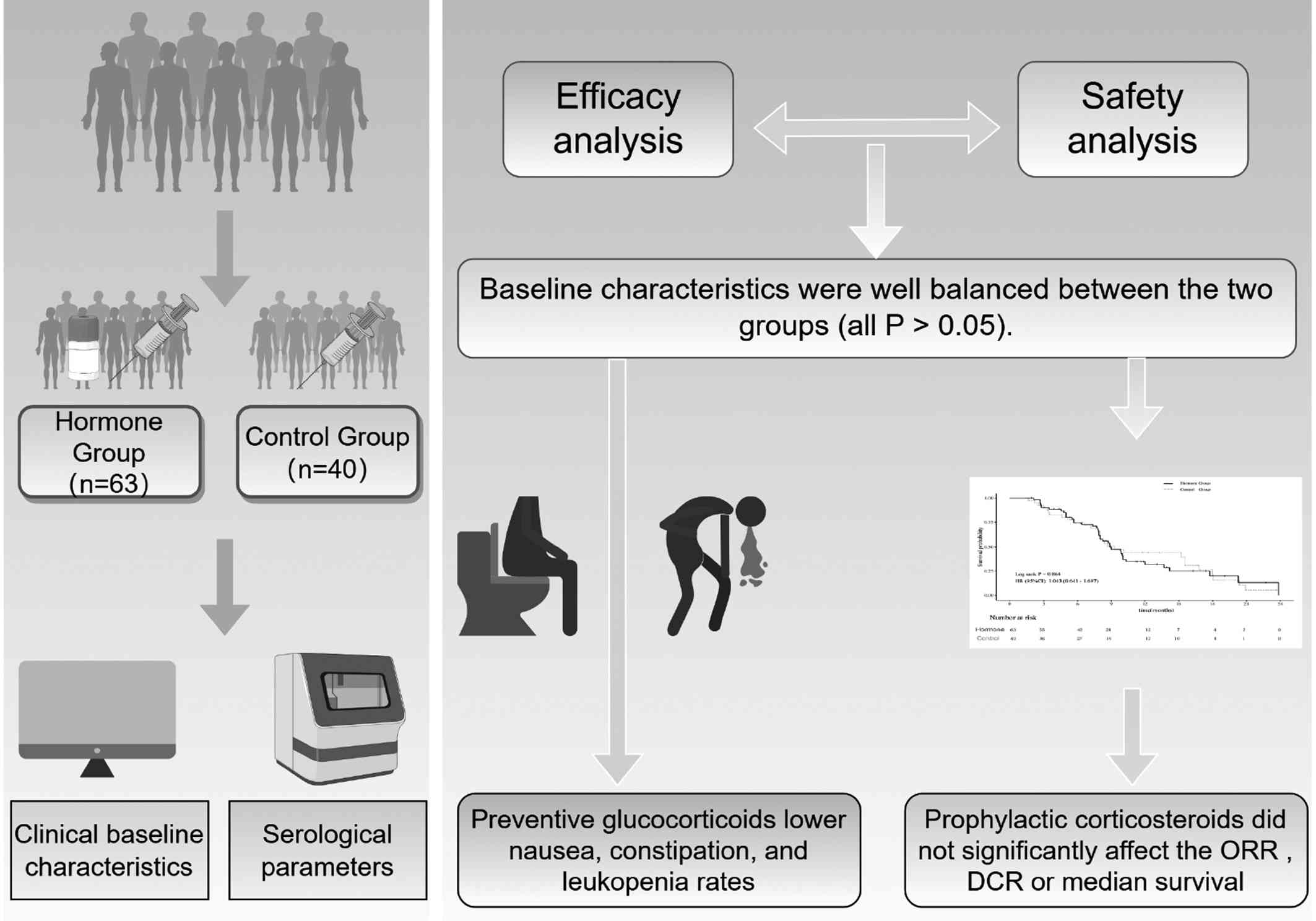
or breastfeeding women. To provide a comprehensive visual overview
of the present study's design, a detailed technical road-map was
constructed, which is presented in the graphical abstract (Fig. 1).
Treatment methods
All patients received etoposide plus platinum
combination chemotherapy, repeated every 3 weeks. ICIs could be
combined and all were administered one day before chemotherapy in
the present study. Hormone group: Dexamethasone tablets 4.5 mg
(Tianjin Xinyi Jinjin Pharmaceutical Co., Ltd., specification 0.75
mg, cat. no. H31020793) were orally administered 30 min before
intravenous (i.v.) etoposide daily, once a day. Control Group: No
routine prophylactic oral administration of dexamethasone acetate
tablets was given before or during chemotherapy. If patients
developed definite chemotherapy-related adverse reactions (such as
grade Ⅱ or higher nausea/vomiting, drug allergic reactions and
infusion-related reactions), symptomatic treatment was provided
according to clinical guidelines, including i.v. or oral
glucocorticoid therapy with dexamethasone when necessary. Pro re
nata (PRN) dexamethasone was administered immediately upon
meeting any of the following per-specified criteria: i)
Breakthrough CINV (≥ grade 2 despite prophylaxis): 8-12 mg
i.v./per os (p.o.), repeatable once per 24 h; discontinued
when symptoms ≤ grade 1, no taper. ii) Acute
infusion/hypersensitivity reaction: 10 mg i.v. bolus, chemotherapy
paused; infusion resumed at 50% rate after complete resolution. No
further dose administered in absence of recurrence within 1 h. iii)
Other transient toxicities (fatigue, anorexia, mild transaminitis)
requiring rapid symptom relief: iv) 4 mg p.o. each morning for ≤5
days; withheld if glucose >13.9 mmol/l or active infection. Stop
without tapering once symptoms improve (9). Among the 40 control patients, 11
received PRN dexamethasone after breakthrough nausea/vomiting or
hypersensitivity reactions.
Etoposide injection (Qilu Pharmaceutical Co., Ltd.;
specification 5 ml: 0.1 g, cat. no. H20143143), 100 mg/m², i.v.
infusion, days 1-3; Cisplatin injection (Jiangsu Hosen
Pharmaceutical Co., Ltd.; specification 30 mg: 6 ml, cat. no.
H20040813), 25 mg/m², i.v. infusion, days 1-3; Carboplatin
injection (Qilu Pharmaceutical Co., Ltd., specification 50 mg: 10
ml, cat. no. H20020181), AUC=5, i.v. infusion, day 1; Lobaplatin
for injection (Hainan Chang'an International Pharmaceutical Co.,
Ltd.; specification 50 mg, cat. no. H20050308), 30 mg/m², i.v.
infusion, day 1. ICIs included: Atezolizumab 1,200 mg per dose,
Durvalumab 1,500 mg per dose, Adebrelimab 20 mg/kg per dose and
Serplulimab 4.5 mg/kg per dose. Symptomatic treatments such as
antiemetic and gastric protection were provided during
chemotherapy.
Study endpoints
Primary endpoint: Incidence of nausea or vomiting
during the first chemotherapy cycle (cycle 1).
Secondary endpoints: Incidence of other adverse
events (constipation, leukopenia, anemia, thrombocytopenia and
renal dysfunction), objective response rate (ORR), disease control
rate (DCR) and median overall survival (OS).
Observation indicators
Adverse reactions were assessed according to the
Common Terminology Criteria for Adverse Events (CTCAE) version
5.0(10). Various adverse
reactions during chemotherapy, such as hypertension, hyperglycemia,
nausea/vomiting, constipation, leukopenia, anemia, hypoalbuminemia,
ALT elevation, AST elevation, renal dysfunction, hypokalemia,
hyponatremia and hypocalcemia, were observed and recorded, with
their incidence and severity graded as I, II, III and IV. Renal
dysfunction was defined as eGFR <60 ml/min/1.73 m²
(corresponding to CTCAE v5.0 grade ≥2: 30-<60 ml/min/1.73 m² for
grade 2, 15-<30 for grade 3, and <15 for grade 4).
Clinical efficacy was evaluated based on the
Response Evaluation Criteria in Solid Tumors version 1.1(11). Contrast-enhanced computed
tomography or magnetic resonance imaging was repeated 2-4 weeks
after every two cycles of chemotherapy, with positron emission
tomography reserved for inconclusive cases and baseline imaging was
performed within 14 days before treatment initiation. Complete
response (CR) was defined as the disappearance of all target
lesions; partial response (PR) as ≥30% reduction in the sum of
target lesion diameters; stable disease (SD) as neither sufficient
shrinkage to qualify for PR nor sufficient increase to qualify for
progressive disease and progressive disease (PD) as ≥20% increase
in the sum of target lesion diameters or the appearance of new
lesions. ORR and DCR were calculated as follows: ORR=(CR+PR)/total
number of cases x100%, DCR=(CR + PR + SD)/total number of cases
x100%.
Statistical methods
SPSS 27.0 (IBM Corp.) software was used to process
the collected case data. Chi-square tests were conducted for
statistical analysis. For every 2x2 comparison of categorical
outcomes, the expected cell frequency (E) was evaluated first. If
all E≥5, the standard Pearson χ² test was applied. Whenever any E
fell below 5, the analysis was switched to two-tailed Fisher's
exact test. Group comparisons were made with the two-sample t-test.
Kaplan-Meier survival curves were used to assess the cumulative
risk of endpoint events; the 95% confidence interval for each
median survival time was calculated with the log-log (Greenwood)
method with Log-rank tests to examine intergroup differences. A
significance level of P<0.05 was set for all observed
indicators. For numerical variables [for example, age, body mass
index (BMI) and laboratory indices] missing values (range 0.5-9.2%
per variable) were imputed once using mean imputation.
Results
Baseline differences
A total of 103 subjects were finally included and
divided into the hormone group (n=63) and the control group (n=40).
Baseline data were analyzed for differences. Statistical analysis
showed no significant differences between the two groups in sex,
age, smoking history, ECOG performance status, or BMI (P>0.05),
indicating favorable comparability (Table I).
 | Table IClinical characteristics of patients
in two groups. |
Table I
Clinical characteristics of patients
in two groups.
| | Total (n=103) | Hormone group
(n=63) | Control group
(n=40) | x2 | P-value |
|---|
| Sex | | | | 2.06 | 0.151 |
|
Male | 94 (91.26) | 60 (95.24) | 34 (85.00) | | |
|
Female | 9 (8.74) | 3 (4.76) | 6 (15.00) | | |
| Age | | | | 1.90 | 0.168 |
|
≥60
years | 34 (33.01) | 24 (38.10) | 10 (25.00) | | |
|
<60
years | 69 (66.99) | 39 (61.90) | 30 (75.00) | | |
| Smoking history | | | | 1.91 | 0.167 |
|
Yes | 50 (48.54) | 34 (53.97) | 16 (40.00) | | |
|
No | 53 (51.46) | 29 (46.03) | 24 (60.00) | | |
| Eastern Cooperative
Oncology Group | | | | | 0.215 |
|
0 | 6 (5.83) | 3 (4.76) | 3 (7.50) | | |
|
1 | 74 (71.84) | 49 (77.78) | 25 (62.50) | | |
|
2 | 23 (22.33) | 11 (17.46) | 12 (30.00) | | |
| Body mass index | | | | | 0.482 |
|
<18.5 | 7 (6.80) | 5 (7.94) | 2 (5.00) | | |
|
18.5-24 | 67 (65.05) | 43 (68.25) | 24 (60.00) | | |
|
>24 | 29 (28.16) | 15 (23.81) | 14 (35.00) | | |
| eGFR | 69.46 | 69.45 (±16.36) | 69.42 (±15.14) | | 0.993 |
Clinical efficacy
As shown in Table
II, the hormone group had 37 cases (58.73%) of PR, 10 cases
(15.87%) of SD and 16 cases (25.40%) of PD. The control group had
19 cases (47.50%) of PR, 10 cases (25.00%) of SD, and 11 cases
(27.50%) of PD. The ORR and DCR were similar between the two groups
(ORR: 58.73 vs. 47.50%, P=0.265; DCR: 74.60 vs. 72.50%, P=0.813).
Further analysis showed no statistical significance in ORR and DCR
between the glucocorticoid and control groups, whether in patients
treated with etoposide plus platinum alone or in combination with
ICIs (P>0.05, data not shown).
| Table IIClinical efficacy of all patients. |
Table II
Clinical efficacy of all patients.
| | Total (n=103) | Hormone group
(n=63) | Control group
(n=40) | x2 | P-value |
|---|
| Complete
response | 0 | 0 | 0 | | |
| Partial
response | 56 (54.37) | 37 (58.73) | 19 (47.50) | | |
| Stable disease | 20 (19.42) | 10 (15.87) | 10 (25.00) | | |
| Progressive
disease | 27 (26.21) | 16 (25.40) | 11 (27.50) | | |
| Objective response
rate | 54.37% | 58.73% | 47.50% | 1.24 | 0.265 |
| Disease control
rate | 73.79% | 74.60% | 72.50% | 0.06 | 0.813 |
Adverse reactions
As shown in Table
III, compared with the control group, the hormone group had
lower incidences of grade II-IV nausea/vomiting (19.05 vs. 45.00%,
χ²=7.98, P=0.005), constipation (3.17 vs. 25.00%, χ²=9.3, P=0.002)
and leukopenia (20.63 vs. 45.00%, χ²=6.9, P=0.009). These results
indicate that glucocorticoids can effectively alleviate
chemotherapy-induced nausea/vomiting, constipation and leukopenia.
However, there were no significant differences between the two
groups in the incidence of grade II-IV anemia, thrombocytopenia,
hypoalbuminemia, ALT elevation, AST elevation, renal dysfunction,
hypokalemia, hyponatremia, hypocalcemia, or thyroid dysfunction,
suggesting that glucocorticoids have no significant effect on
improving these conditions.
| Table IIIIncidence of grade II-IV adverse
reactions in all patients. |
Table III
Incidence of grade II-IV adverse
reactions in all patients.
| | Hormone group
(n=63) | Control group
(n=40) | x2 | P-value |
|---|
| Nausea and
vomiting | 12 (19.05) | 18 (45.00) | 7.98 | 0.005 |
| Constipation | 2(3.17) | 10 (25.00) | 9.30 | 0.002 |
| Hypertension | 28 (44.44) | 13 (32.50) | 1.46 | 0.227 |
| Hyperglycemia | 9 (14.29) | 5 (12.50) | 0.07 | 0.797 |
| Leukopenia | 13 (20.63) | 18 (45.00) | 6.90 | 0.009 |
| Anemia | 8 (12.70) | 10 (25.00) | 2.57 | 0.109 |
|
Thrombocytopenia | 2 (3.17) | 1 (2.50) | <0.001 | 0.999 |
|
Hypoproteinemia | 3 (4.76) | 2 (5.00) | <0.001 | 0.999 |
| ALT elevation | 2 (3.17) | 1 (2.50) | <0.001 | 0.999 |
| AST elevation | 1 (1.59) | 2 (5.00) | 0.16 | 0.687 |
| Renal
dysfunction | 2 (3.17) | 6 (15.00) | 3.27 | 0.071 |
| Hypokalemia | 0 (0.00) | 3 (7.50) | | 0.999 |
| Hyponatremia | 6(9.52) | 3 (7.50) | <0.001 | 0.999 |
| Hypocalcemia | 7 (11.11) | 3 (7.50) | 0.07 | 0.793 |
| Hypothyroidism | 1 (1.59) | 4 (10.00) | 2.15 | 0.143 |
In patients treated with etoposide plus platinum,
the hormone group had significantly lower incidences of grade I-III
nausea/vomiting (54.84 vs. 87.50%, χ²=5.01, P=0.025) and
constipation (9.68 vs. 43.75%, χ²=5.42, P=0.02) compared with the
control group (Table IV).
However, there were no significant differences between the two
groups in the incidence of grade I-III leukopenia, anemia,
thrombocytopenia, hypoalbuminemia, ALT elevation, AST elevation,
renal dysfunction, hypokalemia, hyponatremia, hypocalcemia, or
thyroid dysfunction.
| Table IVIncidence of grade I-III adverse
reactions in etoposide plus platinum. |
Table IV
Incidence of grade I-III adverse
reactions in etoposide plus platinum.
| | Hormone group
(n=31) | Control group
(n=16) | x2 | P-value |
|---|
| Nausea and
vomiting | 17 (54.84) | 14 (87.50) | 5.01 | 0.025 |
| Constipation | 3 (9.68) | 7 (43.75) | 5.42 | 0.020 |
| Hypertension | 20 (64.52) | 7 (43.75) | 1.86 | 0.172 |
| Hyperglycemia | 10 (32.26) | 5 (31.25) | 0.001 | 0.999 |
| Leukopenia | 18 (58.06) | 11 (68.75) | 0.51 | 0.475 |
| Anemia | 24 (77.42) | 12 (75.00) | 0.001 | 0.999 |
|
Thrombocytopenia | 3 (9.68) | 0 | | 0.512 |
|
Hypoproteinemia | 6(19.35) | 5 (31.25) | 0.30 | 0.583 |
| ALT elevation | 10 (32.26) | 4 (25.00) | 0.03 | 0.858 |
| AST elevation | 5 (16.13) | 1 (6.25) | 0.25 | 0.617 |
| Renal
dysfunction | 12 (38.71) | 4 (25.00) | 0.88 | 0.347 |
| Hypokalemia | 3 (9.68) | 1 (6.25) | <0.001 | 0.999 |
| Hyponatremia | 9 (29.03) | 4 (25.00) | <0.001 | 0.999 |
| Hypocalcemia | 13 (41.94) | 5 (31.25) | 0.51 | 0.475 |
In patients treated with etoposide plus platinum
combined with ICIs, the hormone group had significantly lower
incidences of grade II-IV nausea/vomiting (9.38 vs. 37.50%,
χ²=6.44, P=0.011) and leukopenia (18.75 vs. 54.17%, χ²=7.67,
P=0.006) compared with the control group (Table V). Notably, grade ≥2 renal
dysfunction occurred in 0% of the hormone group versus 20.83% of
controls (P=0.026); this difference was not observed in the overall
cohort or the chemotherapy-alone subgroup. No significant
differences were observed between the two groups in the incidence
of grade II-IV constipation, anemia, thrombocytopenia,
hypoalbuminemia, ALT elevation, AST elevation, hypokalemia,
hyponatremia, hypocalcemia, or thyroid dysfunction.
| Table VIncidence of Grade II-IV adverse
reactions in etoposide plus platinum combine with immune checkpoint
inhibitors. |
Table V
Incidence of Grade II-IV adverse
reactions in etoposide plus platinum combine with immune checkpoint
inhibitors.
| | Hormone group
(n=32) | Control group
(n=24) | x2 | P-value |
|---|
| Nausea and
vomiting | 3 (9.38) | 9 (37.50) | 6.44 | 0.011 |
| Constipation | 1 (3.12) | 5 (20.83) | 2.83 | 0.092 |
| Hypertension | 14 (43.75) | 8 (33.33) | 0.62 | 0.430 |
| Hyperglycemia | 3 (9.38) | 3 (12.50) | <0.001 | 0.999 |
| Leukopenia | 6 (18.75) | 13 (54.17) | 7.67 | 0.006 |
| Anemia | 2 (6.25) | 7 (29.17) | 3.78 | 0.052 |
|
Thrombocytopenia | 0 | 1 (4.17) | | 0.429 |
|
Hypoproteinemia | 3 (9.38) | 1 (4.17) | 0.05 | 0.822 |
| ALT elevation | 1 (3.12) | 1 (4.17) | | 0.999 |
| AST elevation | 0 | 1 (4.17) | | 0.429 |
| Renal
dysfunction | 0 | 5 (20.83) | | 0.026 |
| Hypokalemia | 0 | 2 (8.33) | | 0.179 |
| Hyponatremia | 4 (12.50) | 1 (4.17) | 0.37 | 0.543 |
| Hypocalcemia | 3 (9.38) | 1 (4.17) | 0.05 | 0.822 |
| Hypothyroidism | 1 (3.12) | 4 (16.67) | 1.65 | 0.199 |
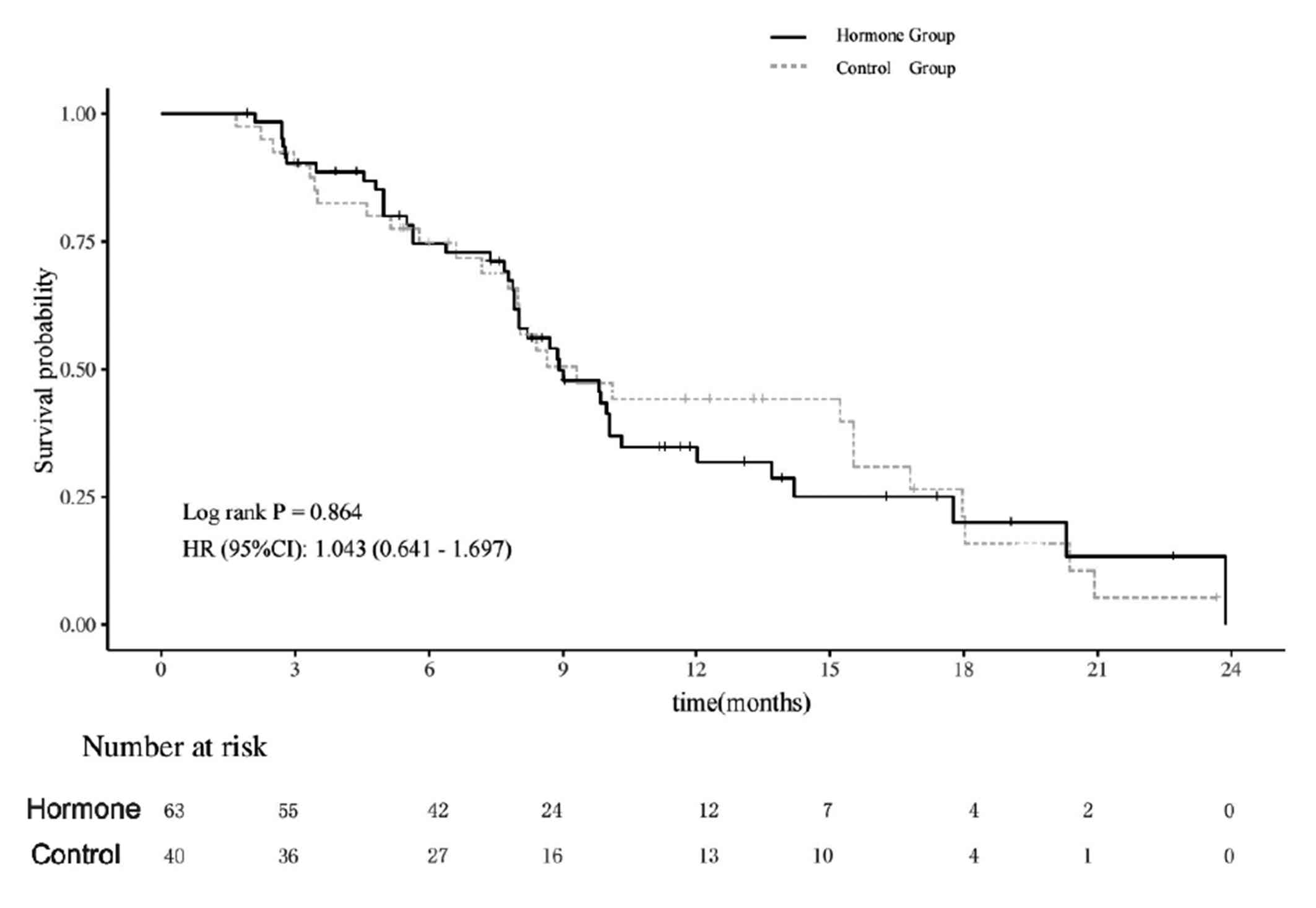
Survival analysis
Kaplan-Meier analysis (Fig. 2) showed that the median survival
time was 8.9 months [95% confidence interval (CI): 8.00-12.03] in
the hormone group and 9.3 months (95% CI: 7.97-16.80) in the
control group, with no significant difference between the two
groups (Log-rank P=0.864, hazard ratio=1.043, 95% CI: 0.641-1.697).
Further analysis showed no significant differences in median
survival time between the glucocorticoid and control groups,
whether in patients treated with etoposide plus platinum alone or
in combination with ICIs (P>0.05, data not shown).
Discussion
Glucocorticoids can alleviate chemotherapy-induced
adverse reactions through various mechanisms (12). Their anti-inflammatory effects can
inhibit the release of inflammatory mediators, reducing tissue
inflammation and relieving symptoms such as vomiting and
constipation (13). Additionally,
they can stabilize mast cell and lysosomal membranes, reducing the
occurrence of allergic and toxic reactions (14), which may have a positive impact on
preventing severe adverse reactions. However, long-term use of
glucocorticoids may lead to a series of side effects, such as
metabolic disorders (15). This
dilemma places clinicians in the challenging position of
continuously weighing therapeutic benefit against potential harm.
In the context of LC chemotherapy, a pivotal and still unresolved
question is whether dexamethasone should be administered only after
adverse events have manifested, or whether prophylactic use is more
likely to maximize net clinical benefit. Consequently, optimizing
the strategic deployment of dexamethasone remains an urgent unmet
need.
To address this central controversy, the present
study specifically interrogates the prophylactic dexamethasone
paradigm. The results showed that compared with the control group,
the hormone group had a significantly lower incidence of
nausea/vomiting, confirming the effectiveness of prophylactic
glucocorticoid use in reducing chemotherapy-related nausea/vomiting
and after adjusting for age, sex and ECOG performance status in a
multivariable logistic regression model, the incidence of vomiting
remained significantly lower in the prophylactic dexamethasone
group than in the non-prophylactic group (Table SII), consistent with the
pharmacological actions of glucocorticoids (7). Nausea/vomiting is a common adverse
reaction to chemotherapy and glucocorticoids can alleviate vomiting
symptoms by inhibiting neurotransmitter release and regulating
gastrointestinal function (16).
In patients treated with etoposide plus platinum and all patients,
the hormone group had a significantly lower incidence of
constipation. Glucocorticoids can improve intestinal motility,
promote water absorption in the intestines and make stools softer
and easier to pass (17). In
patients treated with etoposide plus platinum combined with ICIs
and all patients, the hormone group had a significantly lower
incidence of leukopenia. Glucocorticoids may regulate the immune
system and hematopoietic function of the body, reducing the
inhibitory effects of chemotherapy drugs on bone marrow
hematopoietic cells and thereby lowering the risk of leukopenia
(18). Moreover, in patients
receiving etoposide plus platinum combined with ICIs, the hormone
group had significantly less renal dysfunction, suggesting a
potential kidney-protective effect of prophylactic dexamethasone in
this chemo-immunotherapy subset (19). Glucocorticoids can reduce renal
tubular injury, inflammation and improve renal microcirculation
caused by chemotherapy drugs, thus reducing the risk of renal
dysfunction (20), which is of
significant clinical importance for patients with ES-SCLC receiving
chemotherapy. Renal dysfunction not only affects the quality of
life of patients but may also limit the dosage and course of
subsequent chemotherapy drugs (21). Although this renal benefit is
intriguing, it was observed exclusively in the chemo-immunotherapy
subgroup and needs prospective validation. Notably, all analyses
adhered to the intention-to-treat principle, rescue dexamethasone
was administered only after documented nausea/vomiting or other
breakthrough toxicities and therefore could not bias the primary
endpoint assessment (incidence of nausea/vomiting). Nevertheless,
such rescue therapy constitutes a potential confounder in survival
analyses. To address this, both univariate and multivariate Cox
regression analyses were performed after excluding patients who
received any systemic glucocorticoid. The results remained
consistent, showing that prophylactic versus no prophylactic
dexamethasone did not significantly affect overall survival either
before or after this exclusion (Table
SI).
Concerns have been raised that sustained systemic
glucocorticoids (≥10 mg prednisone-equivalent daily) can attenuate
the efficacy of immune-checkpoint inhibitors (22). In the present cohort study,
however, short-term chemotherapy-linked dexamethasone (4.5 mg
orally for 3 days) did not adversely affect ORR, DCR or OS in
patients receiving ICIs. These findings align with prospective data
showing that brief steroid pulses for anti-emesis do not
significantly diminish efficacy of ICIs (23). Until further randomized evidence is
available, the lowest effective dose and shortest feasible duration
of dexamethasone should be preferred.
However, in terms of hypertension, the hormone group
showed a higher incidence compared with the control group, although
the difference was not statistically significant. This trend
suggests that prophylactic glucocorticoid use may increase the risk
of hypertension, possibly related to the physiological effects of
glucocorticoids in promoting sodium and water retention (24). However, due to limitations such as
sample size, no significant difference was observed. For patients
with a history of hypertension or other cardiovascular risk
factors, it is recommended to closely monitor blood pressure
changes during treatment and take appropriate measures to avoid
potential adverse effects, such as administering antihypertensive
therapy if necessary. Additionally, glucocorticoids can lead to
increased blood glucose levels by promoting gluconeogenesis and
reducing peripheral tissue glucose uptake (25). Although there was no direct data
supporting this in the present study, based on previous research
(26,27), long-term or high-dose use of
glucocorticoids may increase the risk of hyperglycemia. In the
present study, glucocorticoids were used prophylactically for a
short term, therefore no hyperglycemia events were observed.
However, based on previous research results, patients with diabetes
or abnormal glucose regulation should have their blood glucose
monitored during treatment, and any abnormalities should be
promptly addressed. Regarding other adverse reactions, such as
anemia, thrombocytopenia, hypoalbuminemia, AST elevation, ALT
elevation and electrolyte disturbances, no significant differences
were observed between the two groups. It should be noted that,
although subgroup analyzes were attempted, the limited sample size
rendered most of these subgroups underpowered. Residual confounding
cannot be fully excluded and needs to be validated in larger-scale
or pooled datasets. In conclusion, prophylactic glucocorticoid use
has certain benefits for patients with ES-SCLC on platinum-based
doublet therapy. It can alleviate nausea and vomiting, reduce the
risk of leukopenia, and decrease the incidence of constipation,
thereby improving patients' treatment experience and boosting
adherence. The present study found no significant adverse events
linked to prophylactic glucocorticoid use. Additionally, no
significant differences in ORR, DCR, or median survival were
observed between the two groups, indicating that prophylactic
glucocorticoid use does not affect treatment efficacy. In clinical
practice, recognizing the dual-edged nature of glucocorticoids and
using them appropriately can optimize treatment and enhance
patients' quality of life.
Supplementary Material
Cox regression analysis of overall
survival.
Multivariate logistic regression
analysis of nausea/vomiting.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the Beijing Science
and Technology Innovation Medical Development Foundation (grant no.
KC2025-JX-0102ZSC-11), the Beijing Medical and Health Public
Welfare Foundation Medical Science Research Fund (grant no.
YWJKJJHKYJJ-ZH25033), the Natural Science Research Projects in
Anhui Universities (grant no. KJ2021A0279) and the Anhui Province
Traditional Chinese Medicine Inheritance and Innovation Research
Project Funding (grant no. 2025CCCX063).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
WQ and YX designed the study. WQ, WD and ZY were
responsible for data collection and statistical analysis. WQ wrote
and plotted the manuscript. YX reviewed and revised the manuscript
and provided funding support. WQ and YX confirm the authenticity of
all the raw data. All authors read and approved the final version
of the manuscript.
Ethics approval and consent to
participate
The present study was approved (approval no. PJ
2025-04-98) by the Ethics Committee of the First Affiliated
Hospital of Anhui Medical University. As a retrospective study with
no additional risks to patients' treatment or personal information,
it was granted an informed consent exemption.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Kratzer TB, Giaquinto AN, Sung
H and Jemal A: Cancer statistics, 2025. CA Cancer J Clin. 75:10–45.
2025.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Goldman JW, Dvorkin M, Chen Y, Reinmuth N,
Hotta K, Trukhin D, Statsenko G, Hochmair MJ, Özgüroğlu M, Ji JH,
et al: Durvalumab, with or without tremelimumab, plus
platinum-etoposide versus platinum-etoposide alone in first-line
treatment of extensive-stage small-cell lung cancer (CASPIAN):
Updated results from a randomised, controlled, open-label, phase 3
trial. Lancet Oncol. 22:51–65. 2021.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Lee JH, Saxena A and Giaccone G:
Advancements in small cell lung cancer. Semin Cancer Biol.
93:123–128. 2023.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Zhu Y, Liu K, Zhu H, Cao H and Zhou Y:
Comparative efficacy and safety of novel immuno-chemotherapy for
extensive-stage small-cell lung cancer: A network meta-analysis of
randomized controlled trial. Ther Adv Med Oncol: Oct 14, 2023 (Epub
ahead of print).
|
|
5
|
Sabari JK, Lok BH, Laird JH, Poirier JT
and Rudin CM: Unravelling the biology of SCLC: Implications for
therapy. Nat Rev Clin Oncol. 14:549–561. 2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
National Comprehensive Cancer Network.
NCCN Clinical Practice Guidelines in Oncology: Small Cell Lung
Cancer.Version 2.2026. Accessed March 2026. https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1461.
|
|
7
|
Kapugi M and Cunningham K:
Corticosteroids. Orthop Nurs. 38:336–339. 2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Li N, Zheng X, Gan J, Zhuo T, Li X, Yang
C, Wu Y and Qin S: Effects of glucocorticoid use on survival of
advanced non-small-cell lung cancer patients treated with immune
checkpoint inhibitors. Chin Med J (Engl). 136:2562–2572.
2023.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Hesketh PJ, Kris MG, Basch E, Bohlke K,
Barbour SY, Clark-Snow RA, Danso MA, Dennis K, Dupuis LL, Dusetzina
SB, et al: Antiemetics: ASCO guideline update. J Clin Oncol.
38:2782–2797. 2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Freites-Martinez A, Santana N,
Arias-Santiago S and Viera A: Using the common terminology criteria
for adverse events (CTCAE-Version 5.0) to evaluate the severity of
adverse events of anticancer therapies. Actas Dermosifiliogr (Engl
Ed). 112:90–92. 2021.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Schwartz LH, Litiere S, de Vries E, Ford
R, Gwyther S, Mandrekar S, Shankar L, Bogaerts J, Chen A, Dancey J,
et al: RECIST 1.1-update and clarification: From the RECIST
committee. Eur J Cancer. 62:132–137. 2016.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Kalfeist L, Galland L, Ledys F,
Ghiringhelli F, Limagne E and Ladoire S: Impact of glucocorticoid
use in oncology in the immunotherapy era. Cells.
11(770)2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Cruz-Topete D and Cidlowski JA: One
hormone, two actions: Anti- and pro-inflammatory effects of
glucocorticoids. Neuroimmunomodulation. 22:20–32. 2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Busillo JM and Cidlowski JA: The five Rs
of glucocorticoid action during inflammation: Ready, reinforce,
repress, resolve, and restore. Trends Endocrinol Metab. 24:109–119.
2013.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Pofi R, Caratti G, Ray DW and Tomlinson
JW: Treating the side effects of exogenous glucocorticoids; can we
separate the good from the bad? Endocr Rev. 44:975–1011.
2023.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Zhong W, Shahbaz O, Teskey G, Beever A,
Kachour N, Venketaraman V and Darmani NA: Mechanisms of nausea and
vomiting: Current knowledge and recent advances in intracellular
emetic signaling systems. Int J Mol Sci. 22(5797)2021.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Reichardt SD, Amouret A, Muzzi C,
Vettorazzi S, Tuckermann JP, Luhder F and Reichardt HM: The role of
glucocorticoids in inflammatory diseases. Cells.
10(2921)2021.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Cain DW and Cidlowski JA: Immune
regulation by glucocorticoids. Nat Rev Immunol. 17:233–247.
2017.
|
|
19
|
Li D, Yang M, Zhang J, Zhong J, Ding H,
Chen W, Pan J and Liao J: Development and validation of nomogram
for predicting the risk of community-acquired pneumonia after
kidney transplantation of deceased donors. Life Conflux.
1(e115)2025.
|
|
20
|
Choi HM, Jo SK, Kim SH, Lee JW, Cho E,
Hyun YY, Cha JJ, Kang YS, Cha DR, Cho WY and Kim HK:
Glucocorticoids attenuate septic acute kidney injury. Biochem
Biophys Res Commun. 435:678–684. 2013.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Horie S, Oya M, Nangaku M, Yasuda Y,
Komatsu Y, Yanagita M, Kitagawa Y, Kuwano H, Nishiyama H, Ishioka
C, et al: Guidelines for treatment of renal injury during cancer
chemotherapy 2016. Clin Exp Nephrol. 22:210–244. 2018.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Ricciuti B, Dahlberg SE, Adeni A, Sholl
LM, Nishino M and Awad MM: Immune checkpoint inhibitor outcomes for
patients with non-small-cell lung cancer receiving baseline
corticosteroids for palliative versus nonpalliative indications. J
Clin Oncol. 37:1927–1934. 2019.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Schneider BJ, Naidoo J, Santomasso BD,
Lacchetti C, Adkins S, Anadkat M, Atkins MB, Brassil KJ, Caterino
JM, Chau I, et al: Management of immune-related adverse events in
patients treated with immune checkpoint inhibitor therapy: ASCO
guideline update. J Clin Oncol. 39:4073–4126. 2021.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Goodwin JE and Geller DS:
Glucocorticoid-induced hypertension. Pediatr Nephrol. 27:1059–1066.
2012.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Hoes JN, van der Goes MC, van Raalte DH,
van der Zijl NJ, den Uyl D, Lems WF, Lafeber FP, Jacobs JWJ,
Welsing PMJ, Diamant M and Bijlsma JWJ: Glucose tolerance, insulin
sensitivity and beta-cell function in patients with rheumatoid
arthritis treated with or without low-to-medium dose
glucocorticoids. Ann Rheum Dis. 70:1887–1894. 2011.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Lakhani OJ, Kumar S, Tripathi S, Desai M
and Seth C: Comparison of two protocols in the management of
glucocorticoid-induced hyperglycemia among hospitalized patients.
Indian J Endocrinol Metab. 21:836–844. 2017.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Struja T, Nitritz N, Alexander I,
Kupferschmid K, Hafner JF, Spagnuolo CC, Schuetz P, Mueller B and
Blum CA: Treatment of glucocorticoid- induced hyperglycemia in
hospitalized patients-a systematic review and meta- analysis. Clin
Diabetes Endocrinol. 10(8)2024.PubMed/NCBI View Article : Google Scholar
|