Introduction
Colorectal cancer (CRC) represents a major global
health burden, ranking as the third most commonly diagnosed cancer
and the second leading cause of cancer-associated mortality
worldwide (1). In 2022, ~1.93
million new cases and 904,000 mortalities were attributed to CRC
globally, with incidence rates continuing to rise in numerous
developing countries and among younger populations in developed
nations (2). The 5-year survival
rate for patients with metastatic CRC (mCRC) remains low at 14-15%,
despite marked therapeutic advances across the past two decades
(3). This poor prognosis
highlights the need for optimized treatment strategies that improve
survival while maintaining quality of life.
The identification of RAS (including KRAS and NRAS)
mutational status has emerged as a key biomarker in the management
of mCRC, markedly impacting treatment strategies (4). In total, 40-45% of patients with mCRC
harbor RAS wild-type tumors, which are sensitive to anti-EGFR
monoclonal antibodies, such as cetuximab and panitumumab (5). This molecular stratification has
enabled personalized treatment approaches, as patients with RAS
wild-type tumors demonstrate improved outcomes when treated with
anti-EGFR therapies, compared with patients harboring RAS mutations
(6). The therapeutic landscape for
RAS wild-type mCRC has evolved notably, with numerous targeted
agents available for first-line treatment (7). Available options include anti-EGFR
antibodies, such as cetuximab and panitumumab, anti-VEGF agents,
such as bevacizumab and biosimilar agents, all of which may be
combined with standard chemotherapy backbones including
5-fluorouracil, leucovorin and oxaliplatin (FOLFOX) or
5-fluorouracil, leucovorin and irinotecan (FOLFIRI) (8). Previous clinical trials have also
explored UDP glucuronosyltransferase family 1 member A1
(UGT1A1)-guided dose escalation strategies and the addition of
adjuvant agents, such as vitamin C, to enhance therapeutic efficacy
(9,10).
Although these advances have expanded treatment
options, they have also increased complexity in clinical
decision-making. Patient heterogeneity, including differences in
performance status, comorbidities and prior adjuvant therapy
exposure, further complicates treatment selection (11). In addition, the financial burden
associated with biological therapies presents challenges for
healthcare systems and patients, emphasizing the need for
evidence-based treatment optimization (12).
A major limitation in current evidence is the lack
of comprehensive comparative effectiveness data across all
available treatment options. Although a number of randomized
controlled trials (RCTs) have evaluated individual regimens
(7,8,13-16),
numerous studies include only two or three treatment arms, limiting
direct comparisons across all available therapies (17). Traditional pairwise meta-analyses
cannot synthesize evidence in the absence of direct comparisons and
therefore fail to provide a comprehensive evaluation of relative
efficacy and safety (18).
However, network meta-analysis offers an effective approach by
enabling simultaneous comparison of numerous treatments using both
direct and indirect evidence (19). This methodology preserves the
benefits of randomization while allowing estimation of relative
treatment effects between interventions that have not been directly
compared in head-to-head trials (20). For clinicians managing RAS
wild-type mCRC, network meta-analysis can provide a treatment
hierarchy based on numerous efficacy endpoints, supporting
evidence-based clinical decision-making (21).
Therefore, the present network meta-analysis aimed
to comprehensively compare the efficacy and safety of available
first-line treatment options for patients with RAS wild-type mCRC.
By synthesizing evidence from RCTs, treatment rankings were
established based on overall survival (OS), progression-free
survival (PFS), objective response rate (ORR) and safety outcomes,
with the aim of providing evidence-based guidance for optimal
treatment selection in clinical practice.
Materials and methods
Study design
Firstly, the present network meta-analysis was
registered in the International Prospective Register of Systematic
Review (ID: CRD420251138090) and adhered to the Preferred Reporting
Items for Systematic Reviews and Meta-Analyses (PRISMA).
Inclusion and exclusion criteria
Studies were considered eligible for inclusion if
they met the following criteria: i) Population: Adult patients aged
≥18 years with histologically determined RAS wild-type MCRC,
including initially metastatic or recurrent disease; ii)
intervention: Any first-line systemic anticancer treatment,
including chemotherapy, targeted therapy, immunotherapy or
combination regimens; iii) comparison: No restrictions on
comparator arms; iv) outcomes: Reporting at least one primary
outcome, including OS or PFS; and v) study design: RCTs.
Studies were excluded if they met any of the
following criteria: i) Non-randomized study designs, including
observational studies, case series or case reports; ii) inclusion
of RAS-mutant patients without separately extractable data for RAS
wild-type subgroups; iii) focus on adjuvant or neoadjuvant
treatment settings; iv) inclusion of patients with resectable
metastatic disease; v) duplicate publications or overlapping
patient populations; vi) conference abstracts when full-text
publications of the same study were available; or vii) letters,
editorials, reviews or commentaries.
Search strategy
A comprehensive systematic literature search was
conducted across MEDLINE (https://www.nlm.nih.gov/medline/medline_home.html)/PubMed
(https://pubmed.ncbi.nlm.nih.gov/),
Embase (https://www.embase.com/), the Cochrane
Central Register of Controlled Trials through the Ovid platform
(https://ovidsp.ovid.com/) and Web of Science
(https://www.webofscience.com/) from
inception to September 1, 2025. The search strategy combined
Medical Subject Headings and free-text keywords associated with
CRC, RAS wild-type status, metastatic disease and first-line
treatment. No language restrictions were applied. In addition,
reference lists of included studies and relevant systematic reviews
were manually screened to identify additional eligible studies. The
complete search strategy is provided in Table SI.
Data extraction
Data was extracted from eligible studies by two
independent reviewers using a standardized data extraction form.
Discrepancies were resolved through discussion or consultation with
a third reviewer. The following information was extracted from each
study: i) Trial identification, including trial ID, publication
year and study region; ii) study characteristics, including trial
phase and sample size; iii) patient demographics, including mean
age and sex distribution; iv) tumor characteristics, including
primary tumor sidedness and metastatic status; v) interventions
compared; and vi) reported clinical outcomes. For efficacy
outcomes, OS, PFS, ORR and duration of response were extracted,
along with corresponding hazard ratios (HRs), odds ratios (ORs) and
95% CIs. Safety data, including incidence of grade ≥3
treatment-emergent adverse events (TEAEs), were also extracted when
available.
Risk of bias assessment
Methodological quality of included studies was
assessed using the Cochrane Collaboration Risk of Bias tool
(22). The two independent
reviewers evaluated each study across seven domains: Random
sequence generation, allocation concealment, blinding of
participants and personnel, blinding of outcome assessment,
incomplete outcome data, selective reporting and other potential
sources of bias. Each domain was classified as low risk, high risk
or unclear risk of bias. Disagreements were resolved through
consensus or consultation with a third reviewer. Risk of bias
summary figures and graphs were generated using Review Manager
(version 5.4; The Cochrane Collaboration).
Statistical analysis
A random-effects network meta-analysis was conducted
within a frequentist framework using the ‘netmeta’ package in R
(version 4.5.2; Posit Software, PBC) (23). This approach applied a
graph-theoretical model based on electrical network theory. Network
plots were generated to visualize the evidence base, where node
size was proportional to total sample size for each intervention
and line thickness corresponded to the number of trials for each
comparison. The statistical model accounted for associated
treatment effects and addressed zero-event studies by applying a
continuity correction to trials with zero events in a single arm,
while trials with zero events in both arms were excluded. Results
were presented as ORs or HRs with corresponding 95% CIs, depending
on the outcome.
Treatment rankings were determined using P-scores,
representing the frequentist equivalent of the surface under the
cumulative ranking curve, to estimate treatment superiority.
Consistency between direct and indirect evidence within closed
loops was assessed using the node-splitting method. Potential
small-study effects were evaluated through visual inspection of
funnel plots and formally tested using Egger's test. Heterogeneity
was assessed using the Cochran Q statistic, decomposed into
within-design and between-design components and quantified using
the I2 statistic. I2 values of 25-49, 50-74
and ≥75% were interpreted as low, moderate and high heterogeneity,
respectively. All statistical tests were two-sided, and P<0.05
was considered to indicate a statistically significant
difference.
Results
Characteristics of included
studies
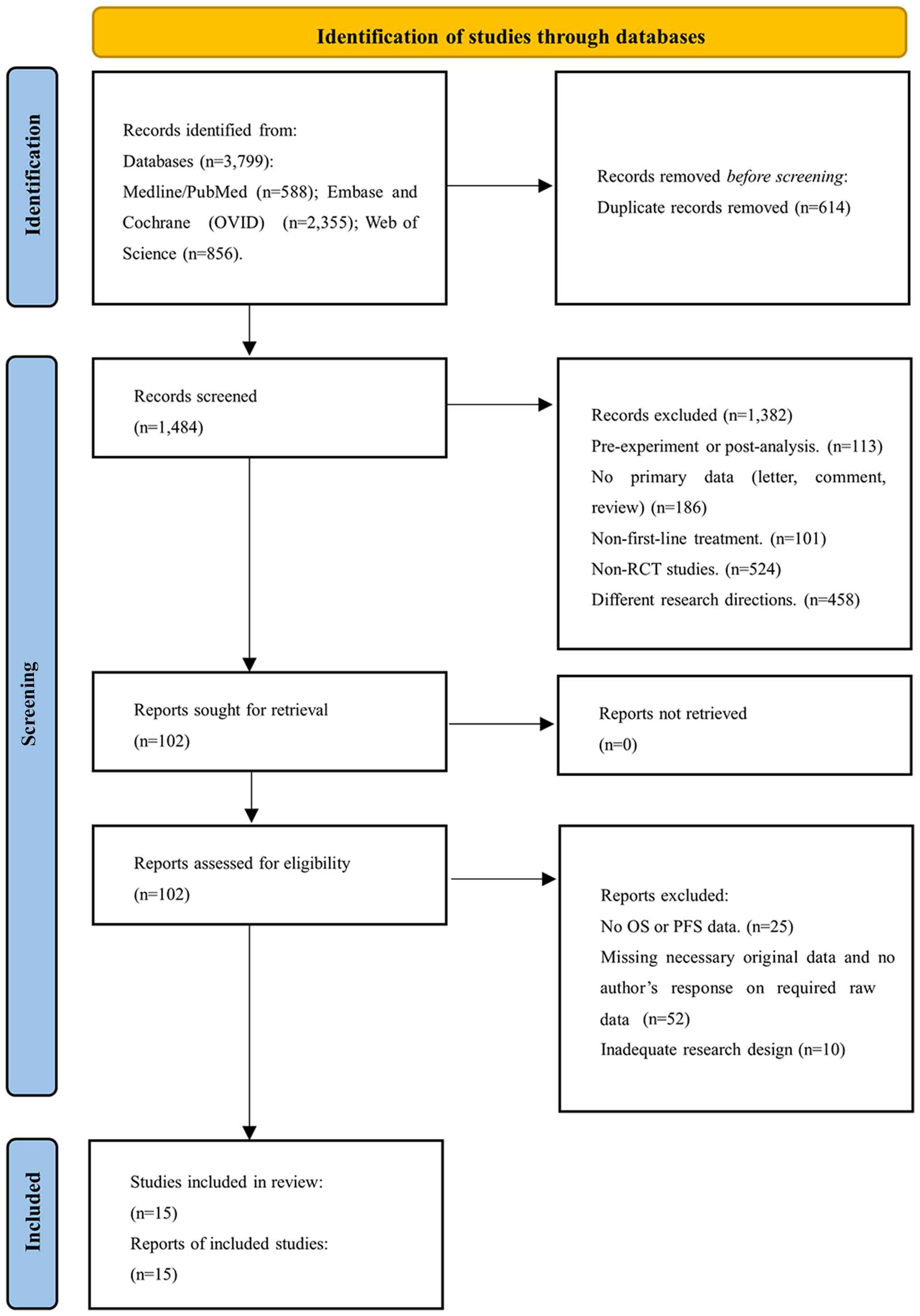
Study selection processes for the present analysis
are outlined in the PRISMA flow diagram (Fig. 1). The initial database search
identified 3,799 records. After removal of 614 duplicates, 1,484
records were screened, resulting in retrieval of 102 full-text
articles for eligibility assessment. Following detailed evaluation,
15 RCTs met the inclusion criteria and were included in the present
network meta-analysis (7-10,13-16,24-30).
Study characteristics are summarized in Table I. Collectively, the 15 trials
included 6,298 patients. Among the included studies, 10 were phase
III trials and 5 were phase II trials.
 | Table ICharacteristics of the included
randomized controlled trials. |
Table I
Characteristics of the included
randomized controlled trials.
| First author,
year | Trial ID
(region) | Phase | Sample size | Average age,
years | Sex | Interventions
compared | PTS | Metastatic
status | OS, months | PFS, months | ORR, months | DOR, months | Safety profile
(grade ≥3 TEAEs) | (Refs.) |
|---|
| Aranda et
al, 2018 | NCT01161316
(Spain) | II | 193 (129/64) | 60 | M: 64%, F: 36% | Cet vs. FOLFOX +
Cet | Left: 73%, Right:
22% | Single site 68.0%,
Multiple: 32.0% | 23/27 (HR=1.24; 95%
CI: 0.85-1.79) | 9/10 (HR=1.19; 95%
CI: 0.80-1.79) | 48.0/39.0%
(OR=1.44; 95% CI: 0.78-2.66) | NA | 70.0/68.0% | (26) |
| Tsai et al,
2020 | NCT02256800
(China) | III | 213 (107/106) | 61 | M: 67%, F: 33% | FOLFIRI + Bev
(UGT1A1- guided dose escalation) vs. Bev + standard FOLFIRI | Left: 81%, Right:
19% | NA | 30.0/22.0
(HR=0.693; 95% CI: 0.503-0.955) | 14.0/10.0
(HR=0.539; 95% CI: 0.398-0.730) | 71.9/41.5%
(OR=4.067; 95% CI: 2.240-7.384) | NA | 23.4/23.6% | (9) |
| Venook et
al, 2017 | NCT00265850
(USA) | III | 1137 (578/559) | 59 | M: 61%, F: 39% | Cet +
FOLFOX/FOLFIRI vs. Bev + FOLFOX/FOLFIRI | Left: 61%, Right:
25% | Liver: 74.0%; Lung:
33.0% | 30.0/29.0 (HR=0.88;
95% CI: 0.77-1.01) | 10.5/10.6 (HR=0.95;
95% CI: 0.84-1.08) | 59.6/55.2%
(NA) | NA | Overall incidence:
53.0% | (8) |
| Watanabe et
al, 2023 | NCT02394795
(Japan) | III | 823 (411/412) | 66 | M: 66%, F: 34% | Pan + FOLFOX vs.
Bev + mFOLFOX | Left: 75.3%, Right:
23.3% | Liver: 81.4% | 37.9/34.3 (HR=0.82;
95.8% CI: 0.68-0.99) | 13.1/11.9 (HR=1.00;
95% CI: 0.83-1.20) | 80.2/68.6%
(NA) | 13.1/11.2 (HR=0.86;
95% CI: 0.70-1.10) | NA | (13) |
| Qin et al,
2018 | NCT01228734
(China) | III | 393 (193/200) | 56 | M: 70%, F: 30% | Cet + FOLFOX vs.
FOLFOX | Left: 79.2 vs.
81.3%/Right: 15.2 vs. 15.4% | Liver:
79.2/84.6% | 20.7/17.8 (HR=0.76;
95% CI: 0.61-0.96) | 9.2/7.4 (HR=0.69;
95% CI: 0.54-0.89) | 61.1/39.5%
(OR=2.41; 95% CI: 1.61-3.61) | NA | 43.2/26.0% | (14) |
| Modest et
al, 2021 | NCT01991873
(Germany) | II | 248 (125/123) | 66 | M: 65%, F: 35% | Pan + FU/FA vs.
FU/FA | Left: 79.2 vs.
81.3%/Right: 15.2 vs. 15.4% | Liver: 79.2/84.6%;
Peritoneum: 10.4/17.9% | 28.7/25.7 (HR=0.84;
95% CI: 0.60-1.18) | 8.8/5.7 (HR=0.72;
80% CI: 0.60-0.85) | 40.8/26.0%
(OR=1.96; 95% CI: 1.14-3.36) | NA | 43.2/26.0% | (28) |
| Liu et al,
2025 | NCT04835142
(China) | III | 688 (341/347) | 59 | M: 65%, F: 35% | A140 + FOLFOX vs.
Cet + FOLFOX | Left: 87.7 vs.
87.0%/Right: 12.3 vs. 13.0% | Liver:
76.2/75.8% | 28.1/NR (HR=1.10;
95% CI: 0.84-1.42) | 10.9/10.8 (HR=1.03;
95% CI: 0.83-1.28) | 71.0/77.5% (ORR
Ratio= 0.93; 90% CI: 0.87-0.99) | 10.2/9.5 (HR=0.91;
95% CI: 0.70-1.18) | 66.6/68.3% | (29) |
| Shi et al,
2025 | NCT03206151
(China) | III | 505 (257/248) | 57 | M: 69%, F: 31% | Cet β + FOLFIRI vs.
FOLFIRI | Left: 85.6 vs.
85.9%/Right 13.2 vs. 12.5% | Liver:
69.6/76.2% | 28.3/23.1
(HR=0.729; 95% CI: 0.551-0.965) | 13.1/9.6 (HR=0.639;
95% CI: 0.468-0.872) | 69.1/42.3%
(OR=3.090; 95% CI: 2.280-4.189) | NA | 83.3/66.9% | (30) |
| Bond et al,
2023 | NCT02162563 (The
Netherlands) | III | 230 (114/116) | 62 | M: 62%, F: 38% | FOLFOX/FOLFIRI +
Bev vs. FOLFOX/FOLFIRI + Pan | Left: 100% | Liver: 12.0% | 39.9/38.3 (HR=0.95;
95% CI: 0.68-1.32) | 10.8/10.4 (HR=1.11;
95% CI: 0.84-1.48) | 53.0/80.0%
(OR=NA) | NA | 54.0/69.0% | (16) |
| Douillard et
al, 2014 | NA (global) | III | 656 (325/331) | 62 | M: 65%, F: 35% | Pan + FOLFOX vs.
FOLFOX | NA | Liver: 19.0/17.0%;
Other: 12.0/14.0% | 23.9/19.7 (HR=0.88;
95% CI: 0.73-1.06) | 10.0/8.6 (HR=0.80;
95% CI: 0.67-0.95) | 57.0/48.0%
(OR=1.47; 95% CI: 1.07-2.04) | NA | NA | (15) |
| Heinemann et
al, 2021 | NCT00433927
(Germany and Austria) | III | 352 (169/183) | 64 | M: 76%, F: 24% | FOLFIRI + Cet vs.
FOLFIRI + Bev | Left: 82%, Right:
18% | NA | 33.0/26.0 (HR=0.75;
95% CI: 0.59-0.94) | 10.0/11.0 (HR=0.99;
95% CI: 0.81-1.24) | 77.0/65.0%
(OR=1.84; 95% CI: 1.15-2.93) | NA | 64.0/51.0% | (7) |
| Wang et al,
2022 | NA (China) | III | 442 (221/221) | 55 | M: 61%, F: 39% | Vitamin C + FOLFOX
+ Bev vs. FOLFOX + Bev | Left: 72.9 vs.
71.5%/Right: 27.1 vs. 28.5% | NA | 20.7/19.7 (HR=1.04;
95% CI: 0.81-1.33) | 8.6/8.3 (HR=0.86;
95% CI: 0.70-1.05) | 44.3/42.1%
(OR=NA) | NA | 33.5/30.3% | (10) |
| Modest et
al, 2019 | NCT01328171
(Germany) | II | 96 (63/33) | 59 | M: 67%, F: 33% | FOLFOX + Pan vs.
FOLFOX | Left: 84.1 vs.
75.8%/Right: 15.9 vs. 24.2% | Liver: 92.1/78.8%;
Lung: 28.6/21.2%; Lymph nodes: 20.6/24.2% | 35.7/29.8 (HR=0.67;
95% CI: 0.41-1.11) | 9.7/9.7 (HR=1.07;
95% CI: 0.69-1.67) | 87.3/60.6%
(OR=4.469; 95% CI: 1.61-12.38) | NA | 81.3/66.7% | (27) |
| Boige et al,
2023 | NCT02404935
(France) | II | 139 (67/72) | 66 | M: 68%, F: 32% | FOLFIRI + Cet vs.
FOLFIRI | Left: 76.1 vs.
80.3%/Right: 23.9 vs. 18.3% | NA | 24.8/19.7 (HR=0.79;
95% CI: 0.50-1.25) | 5.3/2.0 (HR=0.36;
95% CI: 0.24-0.53) | 17.5/4.8%
(OR=NA) | NA | NA | (25) |
| Lonardi et
al, 2019 | NCT02904031
(Italy) | II | 183 (91/92) | 77 | M: 63%, F: 37% | FOLFOX + Pan vs.
5-FU/LV + Pan | Left: 77 vs.
79%/Right: 23 vs. 21% | Single site:
42.9/41.3%, Multiple: 51.7/58.7% | 23.5/22.0 (HR=1.00;
95% CI: 0.73-1.38) | 9.6/9.0 (HR=1.08;
95% CI: 0.80-1.46) | 69.0/52.0%
(OR=0.48; 95% CI: 0.26-0.89) | NA | 60.0/37.0% | (24) |
Patient characteristics were generally balanced
across studies. The mean age was 55-77 years, with a predominance
of male patients ranging from 61-76% across studies. Primary tumor
location was predominantly left-sided, accounting for 61-100% of
patients, consistent with the known favorable prognosis of
left-sided tumors in RAS wild-type disease (17,18).
The liver was the most common site of metastasis, reported in
12-92% of patients, followed by lung metastases in 21-33% and lymph
node involvement in 20-25% of patients (Table I).
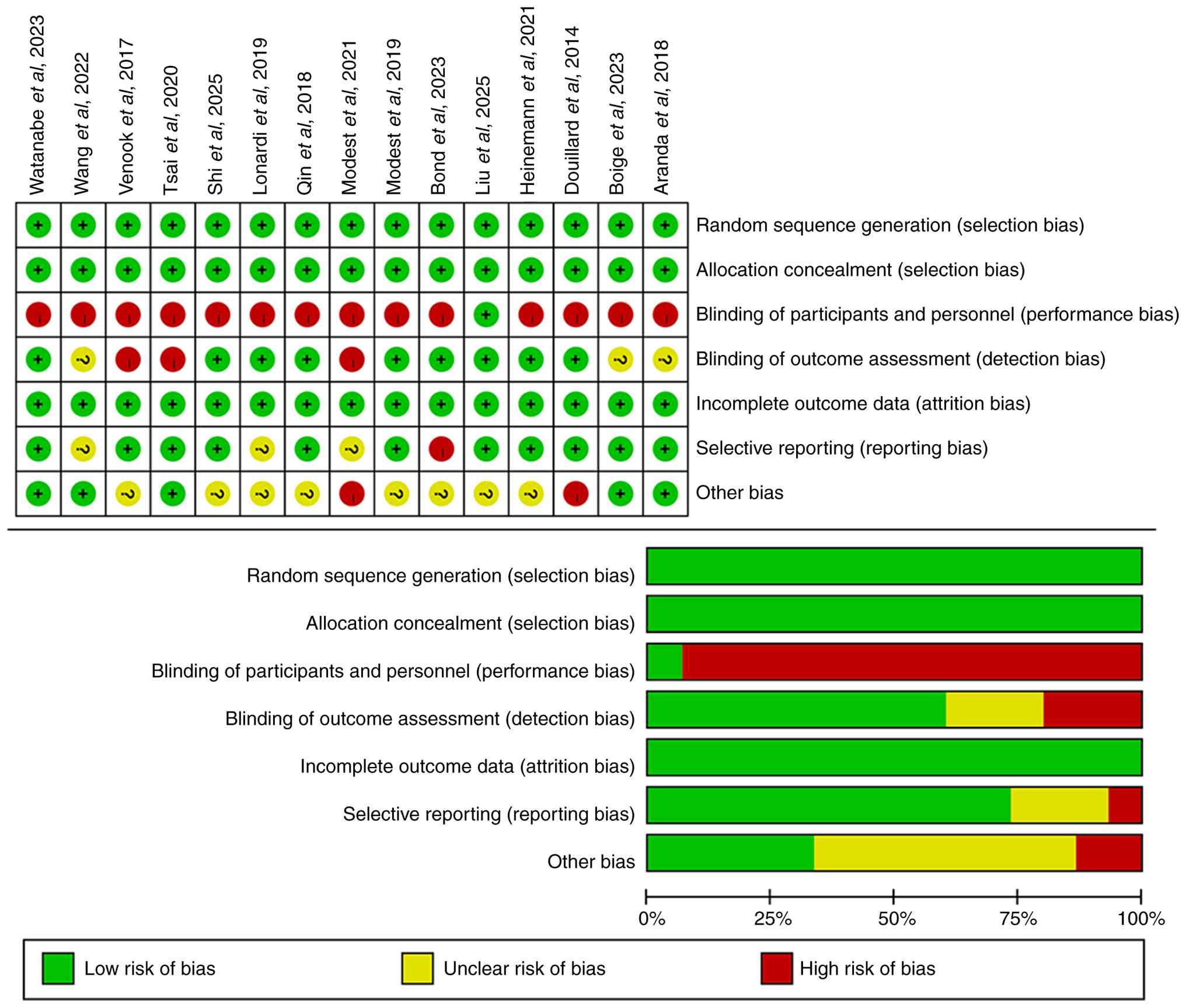
Risk of bias in studies
Overall methodological quality of the included
studies was satisfactory (Fig. 2).
All trials demonstrated low risk of bias for random sequence
generation and allocation concealment, indicating appropriate
randomization procedures. The majority of studies also exhibited
low risk of attrition bias and selective reporting bias, indicating
that outcome data were generally complete and that no major
selective outcome reporting was identified according to the
aforementioned prespecified risk-of-bias criteria.
The main methodological limitation was lack of
blinding of participants and personnel, with 93% of studies
classified as high risk for performance bias. This was largely due
to open-label study designs required when comparing treatments with
different administration schedules or toxicity profiles.
A notable proportion of studies (~67%) exhibited
unclear or high risk of other bias, primarily associated with
pharmaceutical industry funding or involvement of
industry-affiliated authors. Although industry sponsorship does not
necessarily compromise study validity, the potential for conflicts
of interest justified classification as unclear risk in the present
domain.
Network meta-analysis results
Evidence network for the primary analysis included
12 RCTs, seven treatment nodes and eight distinct pairwise
comparisons (Fig. S1).
UGT1A1-guided bevacizumab + FOLFIRI (trial ID: NCT02256800),
vitamin C + bevacizumab + FOLFOX (10) and A140 + FOLFOX (trial ID:
NCT04835142) were excluded because they were single-trial nodes
with small sample sizes. The primary analysis comprised the
following seven treatment nodes: Bevacizumab + chemotherapy (Bev +
Chemo), cetuximab + chemotherapy (Cet + Chemo), panitumumab +
chemotherapy (Pan + Chemo), FOLFOX, FOLFIRI,
5-fluorouracil/leucovorin (5-FU/LV) and cetuximab maintenance. The
network was fully connected, with Bev + Chemo serving as the most
frequently used comparator. In the network plot, node size reflects
cumulative sample size and edge thickness is proportional to the
number of contributing studies per comparison.
OS
Primary network meta-analysis for OS incorporated 12
RCTs. The network demonstrated excellent statistical consistency,
with no significant between-design inconsistency
(Qbetween=0.53; df=2; P=0.768), negligible overall
heterogeneity (Qtotal=2.67; df=6; P=0.849; τ²=0;
I2=0%) and no statistically significant disagreement
between direct and indirect evidence in node-splitting analysis for
any evaluable comparison (all P>0.05; Table SII). Forest plots presenting OS
HRs relative to Bev + Chemo under the random-effects model are
shown in Fig. 3A. A total of two
treatment regimens demonstrated statistically significant
superiority compared with Bev + Chemo: Cet + Chemo (HR=0.853; 95%
CI: 0.775-0.938; P=0.001) and Pan + Chemo (HR=0.855; 95% CI:
0.738-0.992; P=0.038). The remaining treatments, including
cetuximab maintenance, FOLFIRI, FOLFOX and 5-FU/LV, did not differ
significantly from Bev + Chemo. Complete pairwise comparisons
between all treatment nodes are provided in the league table
(Tables SIII and SIV). Treatment ranking based on P-scores
identified Cet + Chemo as the regimen most likely to provide the
highest OS (P-score=0.814), followed by Pan + Chemo (P-score=0.798)
and 5-FU/LV (P-score=0.735). Bev + Chemo ranked fourth
(P-score=0.420), followed by cetuximab maintenance (P-score=0.350),
FOLFIRI (P-score=0.225) and FOLFOX (P-score=0.158; Fig. 4A).
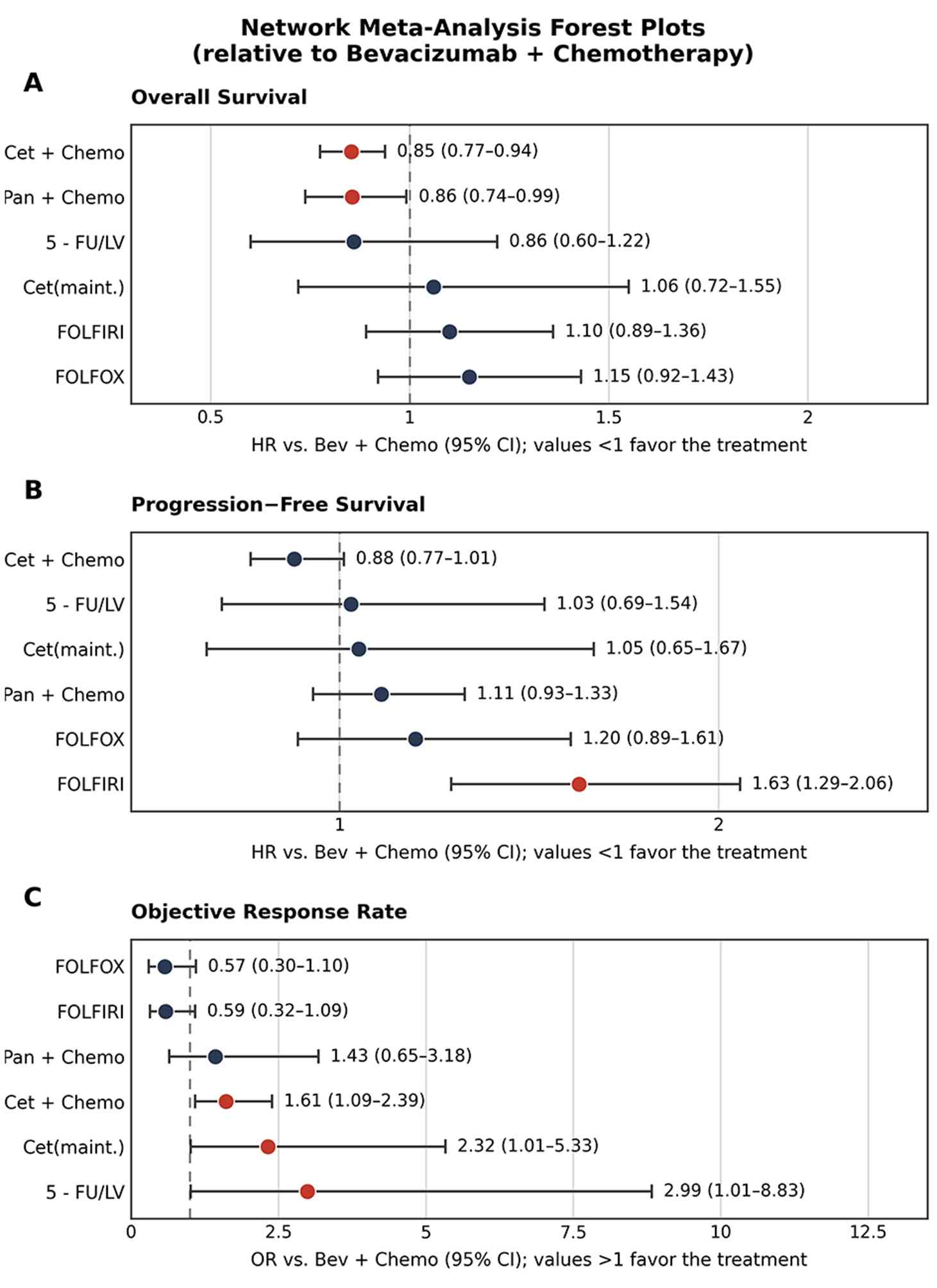 | Figure 3Network meta-analysis forest plots
comparing therapies for (A) overall survival, (B) progression-free
survival and (C) objective response rate. HR, hazard ratio;
5-FU/LV, 5-fluorouracil/leucovorin; FOLFOX, 5-fluorouracil,
leucovorin and oxaliplatin; FOLFIRI, 5-fluorouracil, leucovorin and
irinotecan; Cet, cetuximab; Cet(maint.), Cet maintenance; Chemo,
chemotherapy; Bev, bevacizumab. |
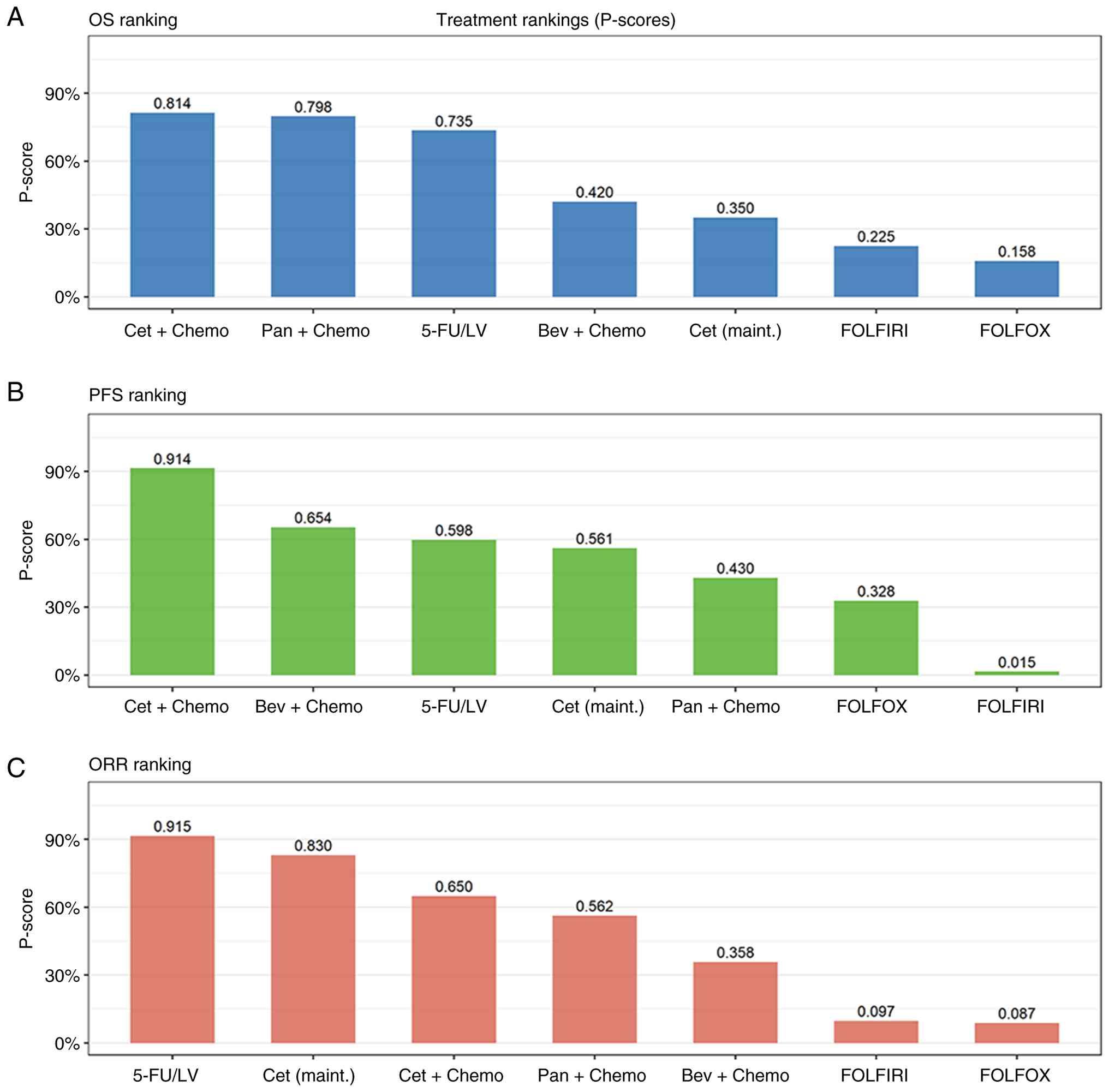 | Figure 4Treatment ranking by P-scores for (A)
OS, (B) PFS and (C) ORR. OS, overall survival; PFS,
progression-free survival; ORR, objective response rate; FOLFOX,
5-fluorouracil, leucovorin and oxaliplatin; FOLFIRI,
5-fluorouracil, leucovorin and irinotecan; 5-FU/LV,
5-fluorouracil/leucovorin; Cet, cetuximab; Cet(maint.), Cet
maintenance; Chemo, chemotherapy; Bev, bevacizumab. |
PFS
PFS analysis included the same 12 RCTs and 7
treatment nodes, with moderate between-study heterogeneity
(I2=44.8%; Qtotal=10.87; df=6; P=0.092).
Between-design inconsistency was not statistically significant
(Qbetween=1.308; P=0.520) and node-splitting determined
no statistically significant direct-indirect disagreement for any
evaluable comparison (all P>0.05; Tables SII and SV). Forest plots for PFS are presented
in Fig. 3B. Under the
random-effects model, Cet + Chemo showed a non-significant trend
toward PFS benefit over Bev + Chemo (HR=0.880; 95% CI: 0.766-1.011;
P=0.072). Notably, FOLFIRI alone was significantly inferior to Bev
+ Chemo for PFS (HR=1.631; 95% CI: 1.294-2.056; P<0.001),
reflecting the marked PFS benefit conferred by bevacizumab addition
to chemotherapy. No other treatment differed significantly from Bev
+ Chemo in PFS. P-score ranking placed Cet + Chemo as the
top-ranked treatment for PFS (P-score=0.914), followed by Bev +
Chemo (P-score=0.654), 5-FU/LV (P-score=0.598) and cetuximab
maintenance (P-score=0.561; Fig.
4B).
ORR
ORR analysis incorporated 8 RCTs and 7 treatment
nodes, with moderate heterogeneity (I2=40.9%) and
borderline between-design inconsistency (Qbetween=2.784;
P=0.095). Forest plots for ORR are presented in Fig. 3C, with estimates expressed as ORRs
relative to Bev + Chemo (OR >1 indicates higher ORR compared
with Bev + Chemo). A total of three regimens demonstrated
significantly higher ORR than Bev + Chemo under the random-effects
model: Cet + Chemo (OR=1.612; 95% CI: 1.087-2.390; P=0.017),
cetuximab maintenance (OR=2.321; 95% CI: 1.011-5.327; P=0.047) and
5-FU/LV (OR=2.989; 95% CI: 1.012-8.828; P=0.047). Pan + Chemo,
FOLFIRI and FOLFOX did not differ significantly from Bev + Chemo.
P-score ranking identified 5-FU/LV (P-score=0.915) and cetuximab
maintenance (P-score=0.830) as top-ranked, followed by Cet + Chemo
(P-score=0.650) and Pan + Chemo (P-score=0.562; Fig. 4C).
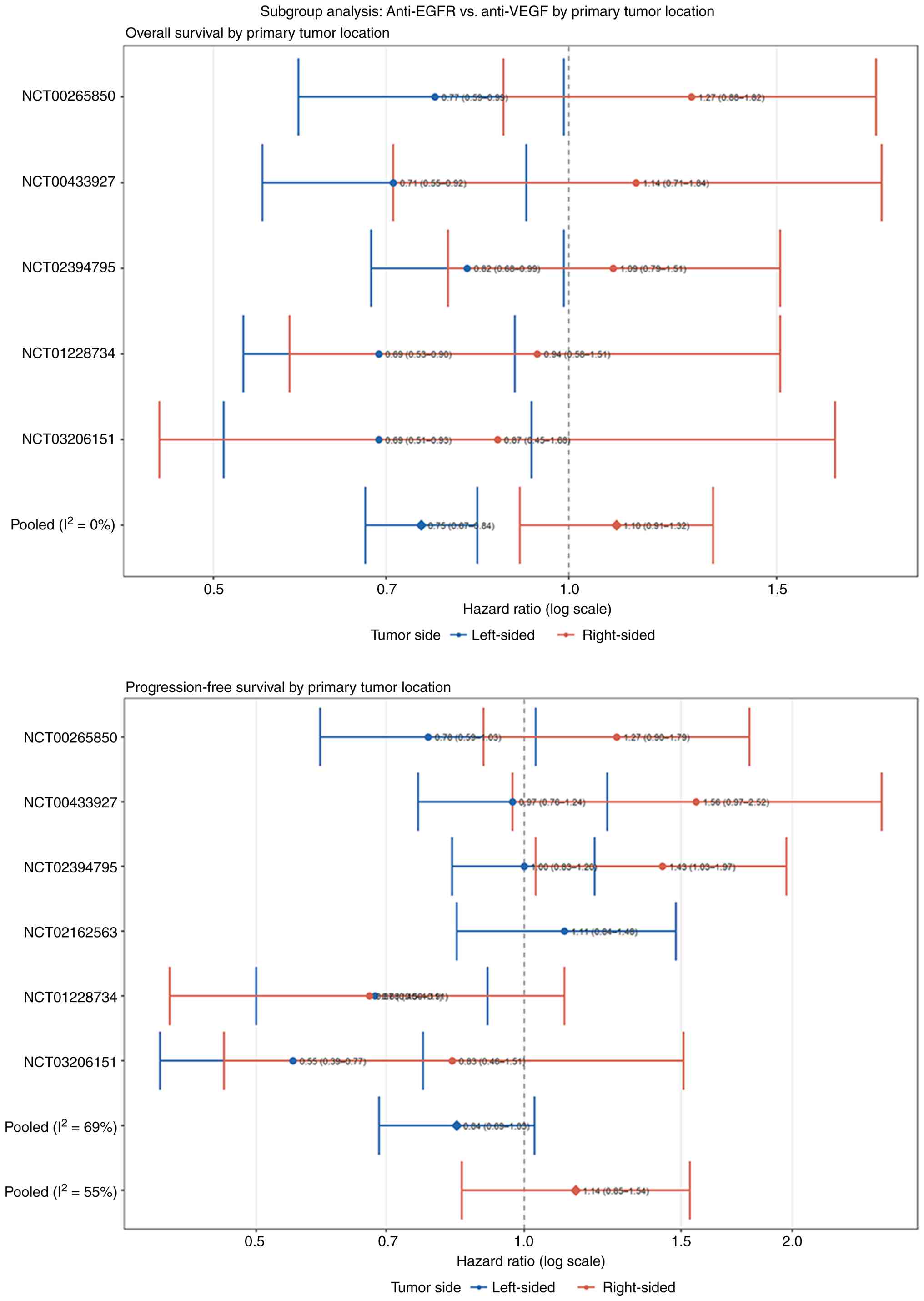
Subgroup analysis: Primary tumor
location
A pre-specified subgroup analysis was conducted
stratifying treatment effects by primary tumor sidedness
(left-sided vs. right-sided). Subgroup-specific HRs were
extractable from 5 trials for OS and 6 trials for PFS. Forest plots
are provided in Fig. 5. For OS,
anti-EGFR-containing regimens demonstrated consistent benefit in
left-sided tumors across all 5 contributing studies. The pooled HR
for anti-EGFR vs. control in left-sided tumors was 0.750 (95% CI:
0.672-0.836; I2=0%), representing a 25.0% mortality risk
reduction. In right-sided tumors, the corresponding pooled HR was
1.097 (95% CI: 0.909-1.325; I2=0%), indicating no OS
benefit from anti-EGFR therapy and a non-significant trend favoring
bevacizumab-based or chemotherapy-only approaches. For PFS, a
broadly consistent directional pattern was observed. In left-sided
tumors, the pooled PFS HR for anti-EGFR vs. control was 0.840 (95%
CI: 0.687-1.027; I2=68.6%), reflecting a non-significant
trend toward benefit. In right-sided tumors, the pooled PFS HR was
1.143 (95% CI: 0.851-1.536; I2=54.9%), suggesting no PFS
advantage and a non-significant numerical disadvantage, for
anti-EGFR agents. Notably, the PARADIGM trial reported a
statistically significant PFS detriment for panitumumab plus
mFOLFOX6 vs. bevacizumab + mFOLFOX6 in right-sided tumors (HR=1.43;
95% CI: 1.03-1.97) (13).
Safety analysis
Incidence of grade ≥3 TEAEs across included
treatments is summarized in Table
I. Rates ranged from 23.4-83.3% across treatment arms.
Anti-EGFR-based combinations were associated with the highest
toxicity burden: Cetuximab biosimilar plus FOLFIRI reported 83.3%
grade ≥3 TEAEs (trial no. NCT03206151) and panitumumab plus FOLFOX
81.3% (trial no. NCT01328171). Bevacizumab-containing regimens
demonstrated comparatively more favorable toxicity profiles (grade
≥3 TEAE rate: 23.4-68.3% across trials). FOLFIRI alone was
associated with grade ≥3 TEAEs in 66.9% of patients. Due to
heterogeneous adverse event reporting across trials, a formal
network meta-analysis of safety outcomes was not performed.
Descriptively, anti-EGFR agents were consistently associated with
skin toxicity, hypomagnesemia and infusion reactions, while
bevacizumab-based regimens were more commonly associated with
hypertension and thromboembolic events. Detailed adverse event data
are provided in Table SVI.
Sensitivity analysis and heterogeneity
assessment
A sensitivity analysis incorporating all 15 RCTs and
9 treatment nodes, including UGT1A1-guided bevacizumab + FOLFIRI,
vitamin C plus bevacizumab + FOLFOX and A140 + FOLFOX, was
conducted. The expanded evidence network is presented in Fig. S2, with full numerical results in
Tables SI and II.
The primary analysis conclusions were demonstrated
to be robust: Cet + Chemo and Pan + Chemo maintained statistically
significant OS benefits in comparison with Bev + Chemo. In the
nine-node sensitivity network, the UGT1A1-guided bevacizumab +
FOLFIRI node ranked highest for both OS (P-score=0.932) and PFS
(P-score=0.992), consistent with the favorable efficacy estimates
reported in the single PURE FIST trial (OS HR=0.693; 95% CI:
0.503-0.955; PFS HR=0.539; 95% CI: 0.398-0.730) (9). However, as these estimates derive
from a single study employing a non-genotyped control arm, their
comparability with other nodes is limited and they are reported as
supplementary findings. A140 + FOLFOX and vitamin C + bevacizumab +
FOLFOX showed no statistically significant benefit compared with
any comparator.
For PFS (I2=44.8%; τ²=0.010) and ORR
(I2=40.9%; τ²=0.041), where moderate between-study
heterogeneity was observed, meta-regression analyses were conducted
incorporating publication year, geographic region (Eastern vs.
Western), chemotherapy backbone (FOLFOX vs. FOLFIRI) and trial
phase (II vs. III) as study-level covariates.
For PFS, none of the examined moderators reached
statistical significance: Publication year (P=0.420), region
(P=0.523), trial phase (P=0.686) and chemotherapy backbone
(P=0.151). Chemotherapy backbone explained the largest, though
non-significant, proportion of PFS heterogeneity (R2 analog=9.9%),
with FOLFOX-based regimens showing a non-significant trend toward
higher HR in comparison with FOLFIRI-based regimens
(coefficient=0.128; P=0.151).
For ORR, geographic region was the strongest, though
non-significant, moderator (R2 analog=24.5%; P=0.150), with
Eastern-region trials showing higher pooled ORR for anti-EGFR
regimens compared with Western-region trials (coefficient=0.600).
Publication year (P=0.347), trial phase (P=0.359) and chemotherapy
backbone (P=0.610) did not explain ORR heterogeneity. Bubble and
dot plots illustrating the association between study-level
covariates and treatment effects for PFS and ORR are provided in
Fig. S3.
Publication bias
Comparison-adjusted funnel plots for OS, PFS and ORR
are presented in Fig. S4. The
funnel plots for all three outcomes demonstrated broadly symmetric
distributions around the null, with no consistent pattern
suggestive of small-study effects or publication bias. Formal
statistical asymmetry tests were not performed owing to the limited
number of studies per individual comparison (k<10 for the
majority of direct comparisons).
Discussion
Within the present comprehensive network
meta-analysis, evidence from 15 RCTs encompassing 6,298 patients
was synthesized to provide the most extensive comparative
assessment of first-line treatments for RAS wild-type mCRC to date.
In the primary analysis of 12 RCTs and seven treatment nodes,
anti-EGFR antibodies combined with chemotherapy demonstrated
statistically significant OS benefits compared with bevacizumab +
chemotherapy, with cetuximab + chemotherapy reducing mortality risk
by 14.7% (HR=0.853; 95% CI: 0.775-0.938) and panitumumab +
chemotherapy by 14.5% (HR=0.855; 95% CI: 0.738-0.992). Treatment
ranking consistently favored cetuximab plus chemotherapy, which
achieved the highest P-scores for both OS (0.814) and PFS (0.914).
Critically, the pre-specified subgroup analysis revealed that these
survival benefits were strongly modified by primary tumor
sidedness: Anti-EGFR therapy conferred a 25.0% OS risk reduction in
left-sided tumors (HR=0.750; I²=0%) but provided no benefit in
right-sided tumors (HR=1.097). Furthermore, anti-EGFR regimens were
associated with markedly higher rates of grade ≥3 adverse events
(up to 83.3%) compared with bevacizumab-based approaches
(23.4-68.3%), highlighting an important efficacy-toxicity trade-off
that must be weighed in clinical decision-making.
The mechanistic basis for the observed differential
efficacy between treatment regimens reflects the distinct
biological pathways targeted by anti-EGFR and anti-VEGF therapies
in RAS wild-type tumors (31). RAS
wild-type status preserves intact EGFR signaling, enabling
effective pathway blockade by cetuximab and panitumumab, which
competitively inhibit ligand binding and prevent receptor
dimerization, ultimately suppressing downstream RAF-MEK/ERK and
PI3K/Akt/mTOR cascades key in tumor cell proliferation and survival
(32). The superior performance of
UGT1A1-guided dosing, observed in a single exploratory phase II
trial (PURE FIST) rather than demonstrated by numerous phase III
trials, leverages pharmacogenomic optimization of irinotecan
metabolism, as patients with favorable UGT1A1 genotypes
(*1/*1 or *1/*28) can
tolerate higher irinotecan doses due to enhanced glucuronidation of
the active metabolite, SN-38, thereby achieving greater cytotoxic
exposure without proportional toxicity increases (33). The mechanism of bevacizumab
involves sequestration of circulating VEGF-A, disrupting tumor
angiogenesis and normalizing aberrant vasculature, which enhances
chemotherapy delivery while reducing interstitial pressure
(34).
The present findings were broadly consistent with
previous comparative effectiveness research while providing updated
and more comprehensive estimates. The FIRE-3 trial reported an OS
HR of 0.70 favoring cetuximab plus FOLFIRI compared with
bevacizumab + FOLFIRI in patients with the RAS wild-type (7); the pooled network estimate for
cetuximab + chemotherapy vs. bevacizumab + chemotherapy (HR=0.853;
95% CI: 0.775-0.938) showed a directionally concordant but
attenuated effect, likely reflecting the integration of more recent
trials, such as CALGB/SWOG 80405 and PARADIGM with heterogeneous
chemotherapy backbones and evolving subsequent therapy landscapes
(8,13). The PARADIGM trial demonstrated a
significant OS benefit for panitumumab plus mFOLFOX6 compared with
bevacizumab + mFOLFOX6 (HR=0.82), which aligns closely with the
pooled panitumumab estimate (HR=0.855; 95% CI: 0.738-0.992) and
further reinforces the OS advantage of anti-EGFR therapy (7,35).
However, unlike the OS findings, the PFS analysis showed only a
non-significant trend favoring cetuximab plus chemotherapy
(HR=0.880; P=0.072), consistent with the well-documented
dissociation between PFS and OS benefits observed in prior
individual trials and meta-analyses, potentially attributable to
differential post-progression treatment effects (36,37).
Regarding response outcomes, the analysis demonstrated higher ORR
with anti-EGFR combinations (OR=1.612; 95% CI: 1.087-2.390;
P=0.017), consistent with a prior meta-analysis reporting pooled
ORRs of 65-75% for anti-EGFR regimens, supporting their
preferential use when rapid tumor shrinkage is clinically
imperative (35).
The subgroup analysis stratified by primary tumor
sidedness may provide quantitative confirmation of a phenomenon
that has been increasingly recognized in the literature. The pooled
OS HR of 0.750 (95% CI: 0.672-0.836) favoring anti-EGFR therapy in
left-sided tumors, contrasted with the absence of benefit in
right-sided tumors (HR=1.097; 95% CI: 0.909-1.325), is consistent
with the landmark retrospective analyses of CRYSTAL and FIRE-3 by
Tejpar et al (37) which
first demonstrated the prognostic and predictive relevance of tumor
sidedness in anti-EGFR-treated patients. Arnold et al
(17) synthesized individual
patient data from six randomized trials and reported a similar
directional interaction, with anti-EGFR therapy conferring marked
OS and PFS benefits exclusively in left-sided tumors (17). The PARADIGM trial further
strengthened this evidence by prospectively stratifying patients by
tumor sidedness and demonstrating a statistically significant PFS
detriment for panitumumab in right-sided tumors (HR=1.43; 95% CI:
1.03-1.97), a finding corroborated in the pooled PFS analysis
(18). Holch et al
(18) conducted a meta-analysis of
first-line trials and concluded that primary tumor location was a
strong predictive factor for anti-EGFR efficacy, with a magnitude
of interaction effect comparable to that observed in the present
analysis (18). Notably, the
present study extends these prior observations by integrating data
from more recently published trials, including PARADIGM, PANDA and
CAIRO5 (13,16,24),
and by providing pooled estimates within a network meta-analysis
framework that allows simultaneous comparison across all available
treatment nodes. The negligible heterogeneity in the left-sided OS
analysis (I²=0%) reinforces the robustness and generalizability of
the sidedness-treatment interaction, supporting the incorporation
of tumor location as a mandatory stratification factor in future
RAS wild-type mCRC trial designs and clinical treatment
algorithms.
The clinical importance of these findings lies in
providing an integrated, evidence-based framework to guide
treatment selection based on primary tumor sidedness. The present
network meta-analysis demonstrated that anti-EGFR therapy conferred
a robust and statistically significant 25.0% OS reduction in
left-sided tumors (HR=0.750; I²=0%), supporting preferential use of
cetuximab or panitumumab + chemotherapy in this population.
Conversely, the absence of anti-EGFR benefit in right-sided tumors
(OS HR=1.097) and the non-significant trend toward PFS detriment
(HR=1.143) argue against anti-EGFR therapy in the present subset,
favoring bevacizumab-based combinations. The differential toxicity
profiles, with anti-EGFR regimens exhibiting higher rates of grade
≥3 adverse events, further reinforce this benefit-risk assessment.
Sensitivity analysis showing favorable results for UGT1A1-guided
bevacizumab + FOLFIRI (OS P-score=0.932; PFS P-score=0.992)
suggests that pharmacogenomic optimization may offer additional
personalization, though further demonstration in independent trials
is required (38,39).
Notably, the present study exhibits a number of
limitations. Firstly, despite including 15 trials, the network
remains sparse for certain comparisons, potentially limiting
precision. Secondly, the open-label design of 93% of trials
introduces potential performance bias, although objective endpoints
mitigate this concern. In addition, heterogeneity in response-based
endpoints suggests treatment effect modifiers that could not be
explored without individual patient data. The single trial
evaluating UGT1A1-guided therapy requires external validation and
subsequent therapies influencing OS could not be accounted for. In
addition, generalizability may be limited because several
clinically relevant molecular subgroups, such as BRAF V600E-mutant,
MSI-H/dMMR, HER2-amplified and rare gene fusion-positive tumors,
were underrepresented or could not be separately analyzed. Finally,
quality-of-life outcomes could not be synthesized due to
heterogeneous reporting.
In conclusion, anti-EGFR antibodies combined with
chemotherapy provide statistically significant OS benefits compared
with bevacizumab + chemotherapy as first-line treatment for RAS
wild-type mCRC, with cetuximab + chemotherapy consistently ranking
as the optimal regimen. The treatment benefit is strongly dependent
on primary tumor location, with a robust 25.0% mortality risk
reduction in left-sided tumors and no benefit in right-sided
tumors. These findings support a tumor sidedness-guided treatment
algorithm, favoring anti-EGFR therapy for left-sided disease and
bevacizumab-based regimens for right-sided disease, while
considering differential toxicity profiles in clinical
decision-making.
Supplementary Material
Network plot for the primary analysis
(seven-node network). mCRC, metastatic colorectal cancer. FOLFOX,
5-fluorouracil, leucovorin and oxaliplatin; FOLFIRI,
5-fluorouracil, leucovorin and irinotecan; 5-FU/LV,
5-fluorouracil/leucovorin; Cet, cetuximab; Cet(maint.), Cet
maintenance; Chemo, chemotherapy; Bev, bevacizumab.
Network plot for the sensitivity
analysis (nine-node network). FOLFOX, 5-fluorouracil, leucovorin
and oxaliplatin; FOLFIRI, 5-fluorouracil, leucovorin and
irinotecan; VitC, vitamin C; UGT1A1, UDP glucuronosyltransferase
family 1 member A1; 5-FU/LV, 5-fluorouracil/leucovorin; Cet,
cetuximab; Cet(maint.), Cet maintenance; Chemo, chemotherapy; Bev,
bevacizumab.
Bubble plots and dot plots. PFS,
progression-free survival; ORR, objective response rate; HR, hazard
ratio; OR, odds ratio; Chemo, chemotherapy; Bev, bevacizumab.
Comparison-adjusted funnel plots for
OS, PFS, and ORR. OS, overall survival; PFS, progression-free
survival; ORR, objective response rate. FOLFOX, 5-fluorouracil,
leucovorin and oxaliplatin; FOLFIRI, 5-fluorouracil, leucovorin and
irinotecan; Cet, cetuximab; Cet(maint.), Cet maintenance; 5-FU/LV,
5-fluorouracil/leucovorin; Chemo, chemotherapy; Bev,
bevacizumab.
Search strategy.
Sensitivity analysis league
table.
League table.
Node-splitting: Direct vs. indirect
evidence consistency.
Sensitivity analysis league table:
Objective response rate (nine nodes).
Safety profiles: Grade ≥3 TEAEs.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
SK and CS performed data collection, conducted
statistical analysis and wrote the manuscript. CS and SY confirm
the authenticity of all the raw data. SY designed the present study
and revised the manuscript. All authors critically reviewed the
manuscript. All authors read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Laversanne M, Sung H, Ferlay J,
Siegel RL, Soerjomataram I and Jemal A: Global cancer statistics
2022: GLOBOCAN estimates of incidence and mortality worldwide for
36 cancers in 185 countries. CA Cancer J Clin. 74:229–263.
2024.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Morgan E, Arnold M, Gini A, Lorenzoni V,
Cabasag CJ, Laversanne M, Vignat J, Ferlay J, Murphy N and Bray F:
Global burden of colorectal cancer in 2020 and 2040: Incidence and
mortality estimates from GLOBOCAN. Gut. 72:338–344. 2023.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Siegel RL, Wagle NS, Cercek A, Smith RA
and Jemal A: Colorectal cancer statistics, 2023. CA Cancer J Clin.
73:233–254. 2023.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Van Cutsem E, Cervantes A, Adam R, Sobrero
A, Van Krieken JH, Aderka D, Aranda Aguilar E, Bardelli A, Benson
A, Bodoky G, et al: ESMO consensus guidelines for the management of
patients with metastatic colorectal cancer. Ann Oncol.
27:1386–1422. 2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Douillard JY, Oliner KS, Siena S,
Tabernero J, Burkes R, Barugel M, Humblet Y, Bodoky G, Cunningham
D, Jassem J, et al: Panitumumab-FOLFOX4 treatment and RAS mutations
in colorectal cancer. N Engl J Med. 369:1023–1034. 2013.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Bokemeyer C, Köhne CH, Ciardiello F, Lenz
HJ, Heinemann V, Klinkhardt U, Beier F, Duecker K, van Krieken JH
and Tejpar S: FOLFOX4 plus cetuximab treatment and RAS mutations in
colorectal cancer. Eur J Cancer. 51:1243–1252. 2015.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Heinemann V, von Weikersthal LF, Decker T,
Kiani A, Vehling-Kaiser U, Al-Batran SE, Heintges T, Lerchenmüller
C, Kahl C, Seipelt G, et al: FOLFIRI plus cetuximab versus FOLFIRI
plus bevacizumab as first-line treatment for patients with
metastatic colorectal cancer (FIRE-3): A randomised, open-label,
phase 3 trial. Lancet Oncol. 15:1065–1075. 2014.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Venook AP, Niedzwiecki D, Lenz HJ,
Innocenti F, Fruth B, Meyerhardt JA, Schrag D, Greene C, O'Neil BH,
Atkins JN, et al: Effect of first-line chemotherapy combined with
cetuximab or bevacizumab on overall survival in patients with KRAS
wild-type advanced or metastatic colorectal cancer: A randomized
clinical trial. JAMA. 317:2392–2401. 2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Tsai HL, Huang CW, Lin YW, Wang JH, Wu CC,
Sung YC, Chen TL, Wang HM, Tang HC, Chen JB, et al: Determination
of the UGT1A1 polymorphism as guidance for irinotecan dose
escalation in metastatic colorectal cancer treated with first-line
bevacizumab and FOLFIRI (PURE FIST). Eur J Cancer. 138:19–29.
2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Wang F, He MM, Xiao J, Zhang YQ, Yuan XL,
Fang WJ, Zhang Y, Wang W, Hu XH, Ma ZG, et al: A Randomized,
open-label, multicenter, phase 3 study of high-dose vitamin C plus
FOLFOX ± bevacizumab versus FOLFOX ± bevacizumab in unresectable
untreated metastatic colorectal cancer (VITALITY study). Clin
Cancer Res. 28:4232–4239. 2022.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Cremolini C, Schirripa M, Antoniotti C,
Moretto R, Salvatore L, Masi G, Falcone A and Loupakis F:
First-line chemotherapy for mCRC-a review and evidence-based
algorithm. Nat Rev Clin Oncol. 12:607–619. 2015.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Goldstein DA, Chen Q, Ayer T, Howard DH,
Lipscomb J, El-Rayes BF and Flowers CR: First- and second-line
bevacizumab in addition to chemotherapy for metastatic colorectal
cancer: A United States-based cost-effectiveness analysis. J Clin
Oncol. 33:1112–1118. 2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Watanabe J, Muro K, Shitara K, Yamazaki K,
Shiozawa M, Ohori H, Takashima A, Yokota M, Makiyama A, Akazawa N,
et al: Panitumumab vs bevacizumab added to standard first-line
chemotherapy and overall survival among patients with RAS
Wild-type, left-sided metastatic colorectal cancer: A randomized
clinical trial. JAMA. 329:1271–1282. 2023.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Qin S, Li J, Wang L, Xu J, Cheng Y, Bai Y,
Li W, Xu N, Lin LZ, Wu Q, et al: Efficacy and tolerability of
first-line cetuximab plus leucovorin, fluorouracil, and oxaliplatin
(FOLFOX-4) versus FOLFOX-4 in patients with RAS wild-type
metastatic colorectal cancer: The open-label, randomized, phase III
TAILOR trial. J Clin Oncol. 36:3031–3039. 2018.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Douillard JY, Siena S, Cassidy J,
Tabernero J, Burkes R, Barugel M, Humblet Y, Bodoky G, Cunningham
D, Jassem J, et al: Final results from PRIME: Randomized phase III
study of panitumumab with FOLFOX4 for first-line treatment of
metastatic colorectal cancer. Ann Oncol. 25:1346–1355.
2014.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Bond MJG, Bolhuis K, Loosveld OJL, de
Groot JWB, Droogendijk H, Helgason HH, Hendriks MP, Klaase JM,
Kazemier G, Liem MSL, et al: First-line systemic treatment
strategies in patients with initially unresectable colorectal
cancer liver metastases (CAIRO5): An open-label, multicentre,
randomised, controlled, phase 3 study from the Dutch colorectal
cancer group. Lancet Oncol. 24:757–771. 2023.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Arnold D, Lueza B, Douillard JY, Peeters
M, Lenz HJ, Venook A, Heinemann V, Van Cutsem E, Pignon JP,
Tabernero J, et al: Prognostic and predictive value of primary
tumour side in patients with RAS wild-type metastatic colorectal
cancer treated with chemotherapy and EGFR directed antibodies in
six randomized trials. Ann Oncol. 28:1713–1729. 2017.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Holch JW, Ricard I, Stintzing S, Modest DP
and Heinemann V: The relevance of primary tumour location in
patients with metastatic colorectal cancer: A meta-analysis of
first-line clinical trials. Eur J Cancer. 70:87–98. 2017.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Mills EJ, Thorlund K and Ioannidis JPA:
Demystifying trial networks and network meta-analysis. BMJ.
346(f2914)2013.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Lumley T: Network meta-analysis for
indirect treatment comparisons. Stat Med. 21:2313–2324.
2002.PubMed/NCBI View
Article : Google Scholar
|
|
21
|
Jansen JP, Trikalinos T, Cappelleri JC,
Daw J, Andes S, Eldessouki R and Salanti G: Indirect treatment
comparison/network meta-analysis study questionnaire to assess
relevance and credibility to inform health care decision making: An
ISPOR-AMCP-NPC good practice Task Force report. Value Health.
17:157–173. 2014.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Higgins JP, Altman DG, Gøtzsche PC, Jüni
P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA, et
al: The Cochrane Collaboration's tool for assessing risk of bias in
randomised trials. BMJ. 343(d5928)2011.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Balduzzi S, Rücker G, Nikolakopoulou A,
Papakonstantinou T, Salanti G, Efthimiou O and Schwarzer G:
netmeta: An R package for network meta-analysis using frequentist
methods. J Stat Softw. 106:1–40. 2023.
|
|
24
|
Lonardi S, Rasola C, Lobefaro R, Rossini
D, Formica V, Scartozzi M, Frassineti GL, Boscolo G, Cinieri S, Di
Donato S, et al: Initial panitumumab plus fluorouracil, leucovorin,
and oxaliplatin or plus fluorouracil and leucovorin in elderly
patients with RAS and BRAF wild-type metastatic colorectal cancer:
The PANDA trial by the GONO foundation. J Clin Oncol. 41:5263–5273.
2023.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Boige V, Blons H, François E, Ben
Abdelghani M, Phelip JM, Le Brun-Ly V, Mineur L, Galais MP, Villing
AL, Hautefeuille V, et al: Maintenance therapy with cetuximab after
FOLFIRI plus cetuximab for RAS wild-type metastatic colorectal
cancer: A phase 2 randomized clinical trial. JAMA Netw Open.
6(e2333533)2023.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Aranda E, García-Alfonso P, Benavides M,
Sánchez Ruiz A, Guillén-Ponce C, Safont MJ, Alcaide J, Gómez A,
López R, Manzano JL, et al: First-line mFOLFOX plus cetuximab
followed by mFOLFOX plus cetuximab or single-agent cetuximab as
maintenance therapy in patients with metastatic colorectal cancer:
Phase II randomised MACRO2 TTD study. Eur J Cancer. 101:263–272.
2018.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Modest DP, Martens UM, Riera-Knorrenschild
J, Greeve J, Florschütz A, Wessendorf S, Ettrich T, Kanzler S,
Nörenberg D, Ricke J, et al: FOLFOXIRI plus panitumumab as
first-line treatment of RAS wild-type metastatic colorectal cancer:
The randomized, open-label, phase II VOLFI study (AIO KRK0109). J
Clin Oncol. 37:3401–3411. 2019.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Modest DP, Karthaus M, Fruehauf S, Graeven
U, Müller L, König AO, Fischer von Weikersthal L, Caca K,
Kretzschmar A, Goekkurt E, et al: Panitumumab plus fluorouracil and
folinic acid versus fluorouracil and folinic acid alone as
maintenance therapy in RAS wild-type metastatic colorectal cancer:
The randomized PANAMA trial (AIO KRK 0212). J Clin Oncol. 40:72–82.
2022.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Liu R, Yin X, Bai Y, Zhong H, Ye F, Wang
Q, Liu M, Li N, Deng Y, Wang Y, et al: A140 plus mFOLFOX6 compared
with cetuximab plus mFOLFOX6 for first-line RAS wild-type
metastatic colorectal cancer: A randomized clinical trial. Eur J
Cancer. 226(115566)2025.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Shi Y, Ba Y, Wang J, Xiong J, Gu K, Chen
Y, Zheng Z, Wang Z, Guo W, Cheng Y, et al: First-line treatment of
anti-EGFR monoclonal antibody cetuximab β plus FOLFIRI versus
FOLFIRI alone in Chinese patients with RAS/BRAF wild-type
metastatic colorectal cancer: A randomized, phase 3 trial. Signal
Transduct Target Ther. 10(147)2025.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Misale S, Di Nicolantonio F,
Sartore-Bianchi A, Siena S and Bardelli A: Resistance to anti-EGFR
therapy in colorectal cancer: From heterogeneity to convergent
evolution. Cancer Discov. 4:1269–1280. 2014.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Parseghian CM, Napolitano S, Loree JM and
Kopetz S: Mechanisms of innate and acquired resistance to anti-EGFR
therapy: A review of current knowledge with a focus on rechallenge
therapies. Clin Cancer Res. 25:6899–6908. 2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Innocenti F, Schilsky RL, Ramírez J,
Janisch L, Undevia S, House LK, Das S, Wu K, Turcich M, Marsh R, et
al: Dose-finding and pharmacokinetic study to optimize the dosing
of irinotecan according to the UGT1A1 genotype of patients with
cancer. J Clin Oncol. 32:2328–2334. 2014.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Jain RK: Normalization of tumor
vasculature: An emerging concept in antiangiogenic therapy.
Science. 307:58–62. 2005.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Pietrantonio F, Cremolini C, Petrelli F,
Di Bartolomeo M, Loupakis F, Maggi C, Antoniotti C, de Braud F,
Falcone A and Iacovelli R: First-line anti-EGFR monoclonal
antibodies in panRAS wild-type metastatic colorectal cancer: A
systematic review and meta-analysis. Crit Rev Oncol Hematol.
96:156–166. 2015.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Toffoli G, Sharma MR, Marangon E, Posocco
B, Gray E, Mai Q, Buonadonna A, Polite BN, Miolo G, Tabaro G and
Innocenti F: Genotype-guided dosing study of FOLFIRI plus
bevacizumab in patients with metastatic colorectal cancer. Clin
Cancer Res. 23:918–924. 2017.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Tejpar S, Stintzing S, Ciardiello F,
Tabernero J, Van Cutsem E, Beier F, Esser R, Lenz HJ and Heinemann
V: Prognostic and predictive relevance of primary tumor location in
patients with RAS wild-type metastatic colorectal cancer:
Retrospective analyses of the CRYSTAL and FIRE-3 trials. JAMA
Oncol. 3:194–201. 2017.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Franke AJ, Skelton WP, Starr JS, Parekh H,
Lee JJ, Overman MJ, Allegra C and George TJ: Immunotherapy for
colorectal cancer: A review of current and novel therapeutic
approaches. J Natl Cancer Inst. 111:1131–1141. 2019.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Tabernero J, Vyas M, Giuliani R, Arnold D,
Cardoso F, Casali PG, Cervantes A, Eggermont AMM, Eniu A, Jassem J,
et al: Biosimilars: A position paper of the European society for
medical oncology, with particular reference to oncology
prescribers. ESMO Open. 1(e000142)2017.PubMed/NCBI View Article : Google Scholar
|