Introduction
Immune checkpoint inhibitors (ICIs) have emerged as
a promising therapeutic modality for patients with triple-negative
breast cancer (TNBC), a subtype characterized by the absence of
estrogen receptor (ER), progesterone receptor (PgR) and human
epidermal growth factor receptor 2 (HER2) expression and associated
with an aggressive clinical course and limited treatment options.
TNBC accounts for approximately 15-20% of all breast cancers
worldwide and is associated with a higher risk of early recurrence
and poorer overall survival compared with other subtypes (1,2). The
introduction of ICIs has partially improved outcomes in this
population, particularly following the KEYNOTE-355 trial, which
established pembrolizumab (Pembro) combined with chemotherapy as a
standard treatment option for advanced or recurrent TNBC (3). Despite their clinical benefit, ICIs
are associated with various immune-related adverse events (irAEs),
including dermatologic, gastrointestinal, hepatic, endocrine, and
pulmonary toxicities, which may necessitate treatment interruption
or discontinuation (4,5). Furthermore, predictive biomarkers for
response remain incompletely understood, particularly in breast
cancer, which generally exhibits a relatively low tumor mutational
burden (TMB) compared with other solid tumors such as melanoma or
lung cancer (6). This biological
feature may partly explain the variable efficacy of ICIs in breast
cancer and highlights the need for further clinical evidence,
especially in rare clinical settings.
Occult breast cancer (OBC), defined as axillary or
distant lymph node metastasis without an identifiable primary tumor
in the breast, is a rare clinical entity, accounting for less than
1% of all breast cancers (7-9).
Due to its low incidence, the clinicopathological characteristics
and optimal systemic treatment strategies for OBC remain poorly
defined. In particular, evidence regarding the efficacy of
ICI-containing regimens in OBC is extremely limited, and most
available data are extrapolated from studies in non-occult
TNBC.
Herein, we report a case of OBC with distant lymph
node metastases that exhibited a sustained and marked response to
Pembro combined with gemcitabine (GEM) and carboplatin (CBDCA).
Although immune-related colitis developed during treatment, the
Pembro-containing regimen was discontinued and treatment was
switched to eribulin, the patient subsequently maintained long-term
disease control under eribulin therapy. This case underscores the
potential efficacy and management considerations of ICI-based
therapy in rare breast cancer subtypes.
Case report
A 71-year-old woman presented with swelling of the
left cervical region, which she first noticed several weeks before
their initial visit to the Department of General Medicine, Saitama
Medical University Hospital (Moroyama-machi, Japan) in July 2023.
Contrast-enhanced computed tomography (CT) scans of the neck and
chest revealed enlargement of multiple lymph nodes in the left
axillary and supraclavicular regions. Fine-needle aspiration
cytology of the left cervical lymph node revealed carcinoma.
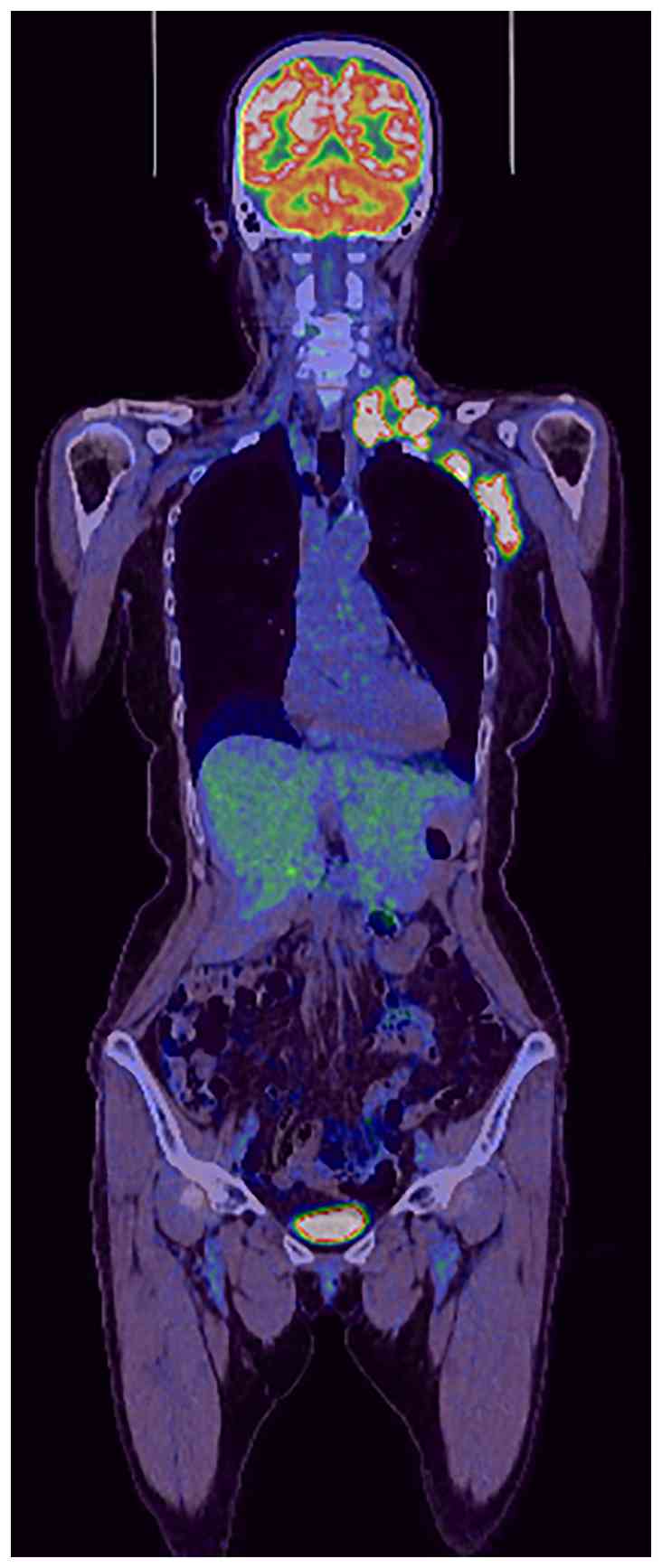
Positron emission tomography-CT using
18F-fluorodeoxyglucose (FDG) demonstrated enlarged lymph
nodes from the left cervical to axillary regions with increased FDG
uptake (Fig. 1); however, no
obvious primary lesion was detected. Breast ultrasonography was
subsequently performed under the suspicion of axillary lymph node
metastasis; however, no mass lesion was identified within the
breast.
As an OBC was suspected, the patient was referred to
the Department of Breast Oncology at our hospital for further
evaluation. She had no significant past medical history and was
taking only fexofenadine for seasonal allergic rhinitis. Regarding
notable family history, their brother had gastric and colorectal
cancers. The patient had no history of smoking or alcohol
consumption, and had a known allergy to penicillin antibiotics.
Upon referral, a core needle biopsy of the axillary
lymph node was performed. Histologically, the tumor cells showed
marked nuclear atypia with pleomorphism. Immunohistochemistry (IHC)
was performed using formalin-fixed, paraffin-embedded tissue
sections (4 µm thick), and the primary antibodies, antigen
retrieval methods and staining conditions are summarized in
Table I. Immunostaining was
performed using an automated immunostainer (BenchMark ULTRA PLUS;
Roche Diagnostics) with a polymer-based detection system according
to the manufacturer's protocol. The tumor cells were positive for
mammaglobin, GATA-binding protein 3 and cytokeratin 7, and negative
for gross cystic disease fluid protein-15 (GCDFP-15). ER and PgR
expression rates were 0% and HER2 score was 0, supporting the
diagnosis of metastatic TNBC of the axillary lymph node. Ki67
labeling index was 80% (Fig. 2).
Based on these findings, the patient was diagnosed with OBC in the
left breast, T0N3cM1(LYM), Stage IV TNBC. Programmed death-ligand 1
IHC demonstrated a combined positive score >10 with the 22C3
antibody, while the SP142 was IC0 (Fig. 2). Breast magnetic resonance imaging
(MRI) was not performed because systemic therapy was prioritized in
the setting of stage IV disease, and MRI could not be scheduled
immediately.
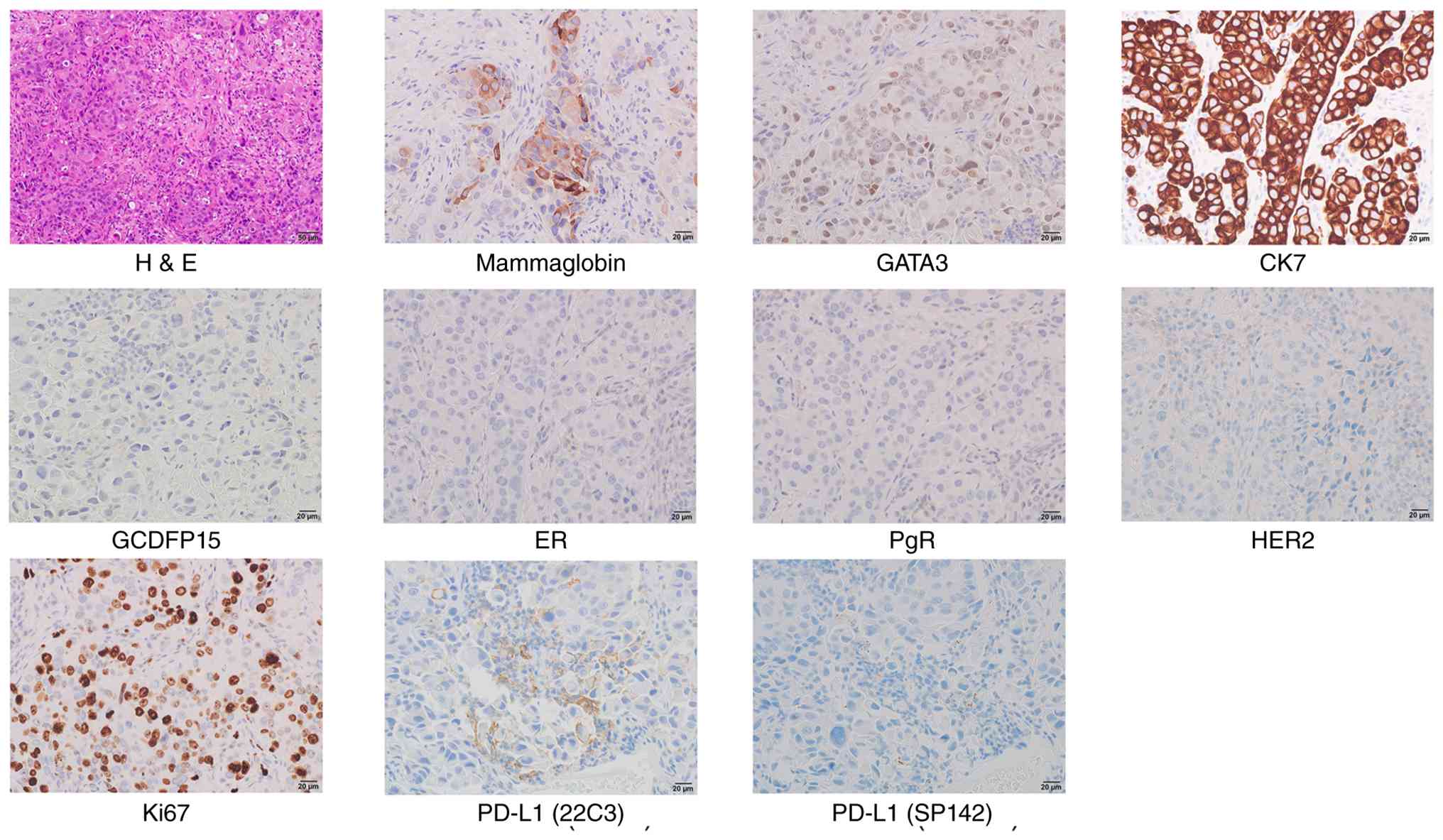 | Figure 2Histopathology and
immunohistochemistry of the axillary lymph node metastasis.
Representative images of the axillary lymph node core biopsy.
H&E staining shows tumor cells with marked nuclear atypia and
pleomorphism (magnification, x200; scale bar, 50 µm).
Immunohistochemistry demonstrates positivity for mammaglobin,
GATA3, and CK7, and negativity for GCDFP-15. Tumor cells are
negative for ER, PgR and HER2 (triple-negative breast cancer
profile), with a high Ki67 labeling index (80%), PD-L1 expression
(22C3, CPS >10; SP142, IC0) (magnification, x400; scale bar, 20
µm). H&E, hematoxylin and eosin; GATA3, GATA-binding protein 3;
CK7, cytokeratin 7; GCDFP15, gross cystic disease fluid protein-15;
ER, estrogen receptor; PgR, progesterone receptor; HER2, human
epidermal growth factor 2; PD-L1, programmed death-ligand 1. |
 | Table IPrimary antibodies and staining
conditions used for immunohistochemistry. |
Table I
Primary antibodies and staining
conditions used for immunohistochemistry.
| Name | Manufacturer | Cat. no. | Dilution | Antigen
retrieval | Incubation
temperature and time |
|---|
| GATA3 | Nichirei Biosciences,
Inc. | 418201 | Prediluted | pH 8.5, 95˚C, 64
min | 36˚C, 32 min |
| GCDFP15 | Leica Biosystems | NCL-L-GCDFP15 | 1:40 | pH 8.5, 95˚C, 36
min | 36˚C, 32 min |
| CK7 | Agilent Technologies,
Inc. | M7018 | 1:100 | pH 8.5, 95˚C, 36
min | 36˚C, 32 min |
| ER | Roche
Diagnostics | 790-4324 | Prediluted | pH 8.5, 95˚C, 64
min | 36˚C, 32 min |
| PgR | Roche
Diagnostics | 790-2223 | Prediluted | pH 8.5, 95˚C, 64
min | 36˚C, 32 min |
| HER2 | Roche
Diagnostics | 790-2991 | Prediluted | pH 8.5, 95˚C, 64
min | 36˚C, 12 min |
| PD-L1 (22C3) | Dako; Agilent
Technologies, Inc. | SK006 | Ready-to-use | EnVision FLEX TRS low
pH, 97˚C, 20 min | Room temperature, 30
min |
| PD-L1 (SP142) | Roche Tissue
Diagnostics; Roche Diagnostics, Ltd. | 744-7257 | Prediluted | Cell Conditioning 1
(CC1; Roche Diagnostics) on the Ventana BenchMark ULTRA system | 36˚C, 16 min |
Treatment with Pembro + GEM + CBDCA was initiated
shortly after referral. The patient's height, weight, and body
surface area were 150 cm, 43 kg, and 1.34 m2,
respectively. The administered doses were Pembro 200 mg, GEM 1,000
mg/m2 (1,340 mg total dose), and CBDCA AUC 4 (165 mg,
calculated using the Calvert formula). Even if the present case
were classified as carcinoma of unknown primary site (CUP), this
regimen was selected because GEM + CBDCA has been reported to be
effective in CUP (10), and the
KEYNOTE-355 trial demonstrated the clinical benefit of Pembro in
combination with several standard chemotherapy regimens, including
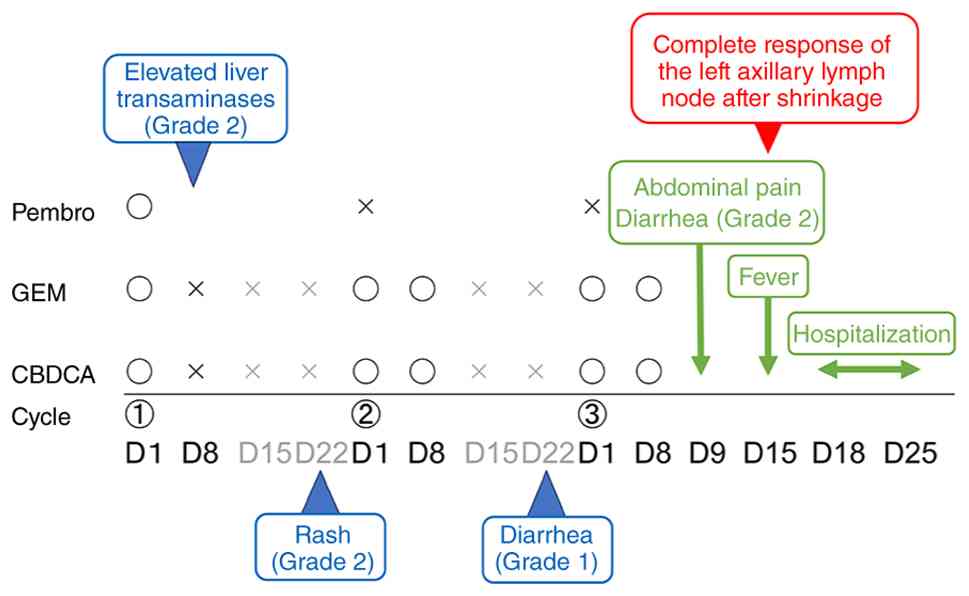
GEM + CBDCA, irrespective of chemotherapy partner (3). The chemotherapy course, including
dose modifications, adverse events, and treatment responses, is
summarized in Fig. 3. During the
first cycle, the patient received Pembro + GEM + CBDCA on Day 1. On
Day 8, the patient presented with elevated liver enzymes (AST 113
U/l; ALT 119 U/l, CTCAE Grade 2-3). Although immune-related
hepatitis was considered, the abnormalities were primarily
attributed to chemotherapy-induced toxicity, and the planned GEM +
CBDCA was withheld for monitoring. On Day 15, the patient's liver
function remained elevated (AST 64 U/l; ALT 82 U/l, Grade 1-2);
thus, treatment was again postponed. In the second cycle, on Day 1,
the treatment was delayed owing to a Grade 2 rash involving the
neck, both sides of the forearms, and the dorsal and palmar
surfaces of the hands. The patient was evaluated by a
dermatologist; after considering differential diagnoses, including
chemotherapy-induced reaction, drug eruption, infection, and
contact dermatitis, the patient was treated with oral
antihistamines and topical steroids. As the rash had improved to
Grade 1 but persisted, Pembro was withheld as a precaution, whereas
GEM + CBDCA were administered as scheduled. On Day 8, GEM + CBDCA
were administered again as planned.
In the third cycle, on Day 1, the treatment was
delayed owing to diarrhea (Grade 1). After improvement in the
following week, Pembro was withheld due to concern for irAEs,
whereas GEM + CBDCA were administered. On Day 8, GEM + CBDCA were
also administered. However, from Day 9, the patient developed
abdominal pain and Grade 2 diarrhea. By Day 15, she also presented
with fever and was evaluated in our Department of Breast Oncology.
Infectious enteritis was suspected; accordingly, the patient was
initially managed as an outpatient and received symptomatic
treatment, empiric levofloxacin (LVFX), and oral probiotics.
However, as abdominal pain and diarrhea persisted, re-evaluation
was performed on Day 18. Laboratory findings revealed white blood
cell count of 6,610/µl and C-reactive protein level of 6.484 mg/dl.
CT imaging demonstrated increased pericolic fat attenuation around
the sigmoid and descending colon, indicative of colitis.
Differential diagnoses included Clostridioides difficile
(CD) colitis, other bacterial or viral enteritis, and other
inflammatory bowel diseases. CMV antigen and stool tests, including
CD antigen and CD toxin, yielded negative results.
Considering the possibility of irAE colitis, the
patient was admitted on Day 18. During hospitalization, the patient
continued oral LVFX and probiotics and was managed with bowel rest
and intravenous fluids. Their symptoms improved by Day 21 (Day 3 of
hospitalization); no systemic steroid therapy was required, and
oral intake was resumed. The patient was discharged on Day 25 (Day
8 of hospitalization) after resolution of symptoms and stable oral
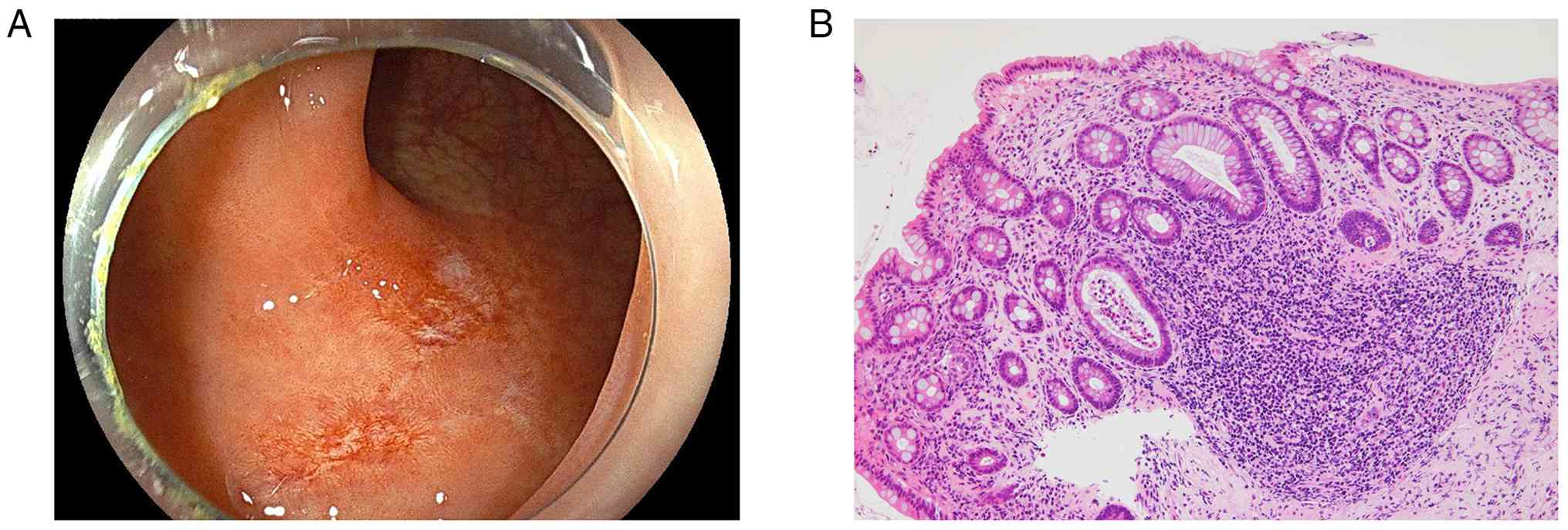
intake. Colonoscopy performed 1 week after discharge revealed
erosions in the transverse and sigmoid colon (Fig. 4A), and biopsy samples were
obtained. Histopathology showed chronic inflammatory cell
infiltration in the stroma and microcrypt abscesses (Fig. 4B), consistent with the diagnosis of
ICI-related colitis.
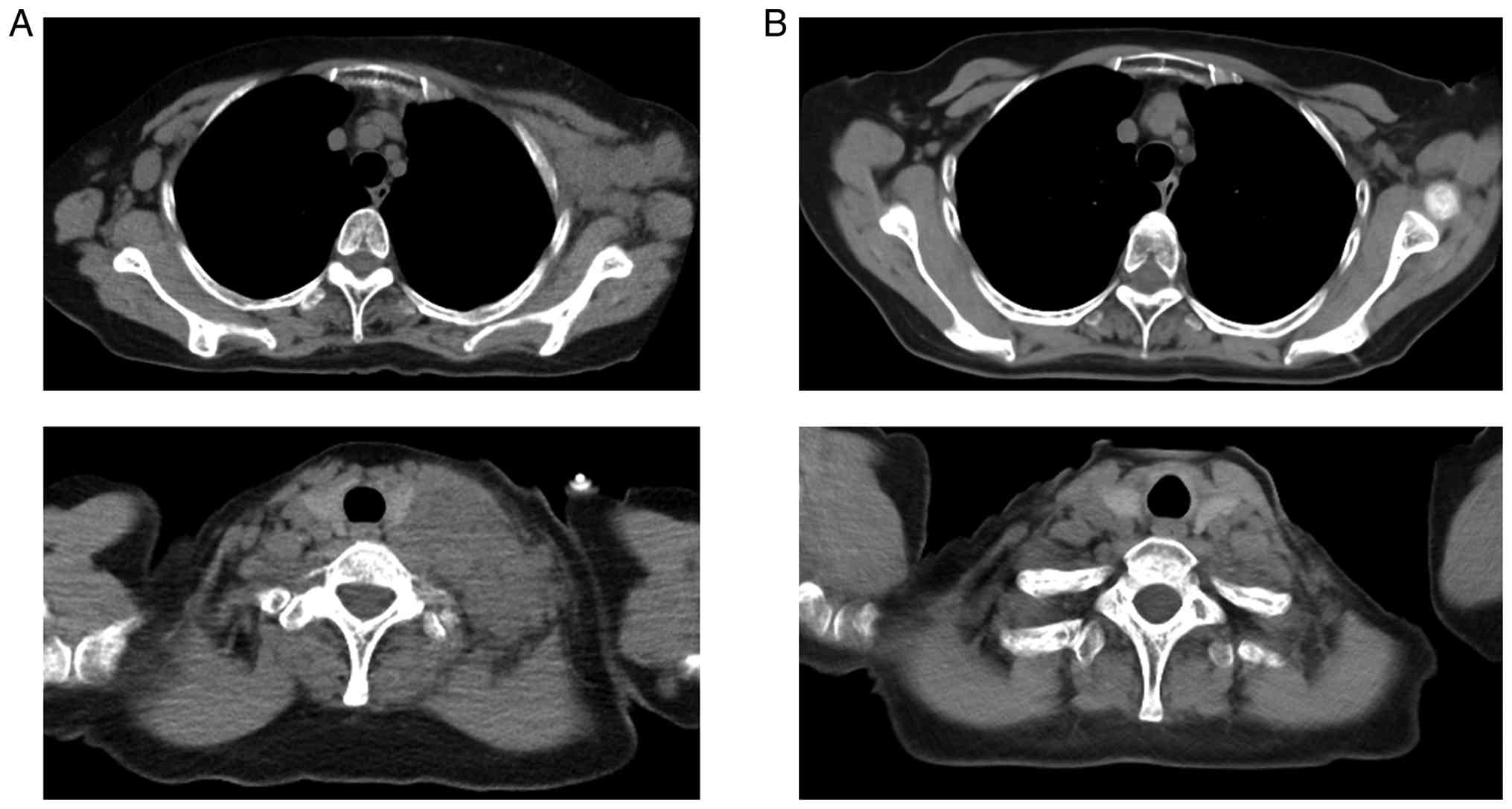
Notably, CT performed during the third treatment
cycle revealed marked shrinkage of the left axillary lymph node
metastases, which decreased from 26 and 21 mm at baseline to 0 mm
after treatment, as well as resolution of the left cervical lymph
node metastasis, which decreased from 25 mm at baseline to 0 mm.
According to RECIST criteria, both regions achieved a complete
response (CR) to Pembro + GEM + CBDCA regimen (Fig. 5). The Pembro + GEM + CBDCA regimen
was discontinued, and treatment was switched to eribulin 1 week
after colonoscopy. Among the available options, including taxanes,
eribulin, and oral fluoropyrimidines, we selected eribulin owing to
its short infusion time and relatively low risk of gastrointestinal
toxicity. Evidence guiding treatment after CR in this setting is
limited, and data supporting a switch to maintenance systemic
therapy remain scarce (11). The
patient has continued regular follow-up visits at the time of each
eribulin administration. Radiological evaluation using CT has been
performed every 2-3 months to monitor disease status. The patient
has maintained a CR on eribulin monotherapy for over 1 year as of
February, 2026, the date of the most recent CT evaluation. Although
breast MRI has not yet been performed, follow-up CT imaging has not
demonstrated any detectable breast lesion.
Discussion
OBC is a rare clinical entity, accounting for less
than 1% of all breast cancers. It is defined as axillary lymph node
metastasis without an identifiable primary tumor in the breast on
clinical and radiological examination (9). Originally, OBC was defined as
axillary lymph node metastasis consistent with breast carcinoma
without a clinically or radiologically detectable primary breast
lesion. More recently, the definition has evolved with advances in
imaging. For example, Ofri and Moore (9) proposed distinguishing clinical OBC
from pathological OBC. They define clinical OBC as no lesion
detectable on clinical examination, mammography, or
ultrasonography, whereas pathological OBC additionally requires a
negative breast MRI and, when performed, a pathologically negative
mastectomy specimen. Given the absence of an apparent breast
lesion, the differential diagnosis should include other primary
malignancies known to metastasize to axillary lymph nodes, such as
malignant melanoma, lung cancer, thyroid cancer, gastric cancer,
colorectal cancer, pancreatic cancer, and ovarian cancer (12,13).
Notably, accurate diagnosis relies on thorough imaging and IHC
evaluation of axillary lymph node metastases. IHC analysis of
biomarkers, including ER, PgR, GCDFP-15, and mammaglobin, has
proven useful in confirming that the tumor originates from breast
tissue (14,15).
In the KEYNOTE-355 trial, irAEs occurred in
approximately 26% of patients receiving Pembro in combination with
chemotherapy. The most commonly reported irAEs included
hypothyroidism, hyperthyroidism, pneumonitis, and colitis. Grade 3
or higher irAEs were relatively infrequent, occurring in
approximately 5% of patients, with colitis reported in less than 1%
(3). Regarding onset, patients
receiving PD-1 monotherapy reportedly develop colitis at a median
of 25.4 weeks (range: 0.6-119.9 weeks) after treatment initiation
(16). The onset in the present
case was relatively early compared with this previously reported
median but was within the reported range, thereby indicating the
possibility of early-onset cases. Therefore, when diarrhea occurs
even after a limited number of Pembro administrations,
immune-related colitis should be considered a differential
diagnosis. In patients receiving combination therapy with ICIs and
cytotoxic chemotherapy, alternative etiologies such as
chemotherapy-induced mucosal injury, bacterial or viral infection,
and pre-existing inflammatory bowel disease should also be
considered (17). Systematic
reviews have underscored the importance of timely colonoscopic
evaluation in suspected ICI-induced colitis. Colonoscopy is
generally recommended within 7 days of the onset of moderate to
severe diarrhea (grade ≥2), enabling direct mucosal assessment and
biopsy to confirm diagnosis and exclude infections or other
etiologies (5,18). Early colonoscopy facilitates
accurate grading of inflammation, which guides treatment decisions.
In cases with grade 2 or higher colitis, systemic corticosteroids
are initiated promptly at doses of 1-2 mg/kg/day of prednisone or
equivalent (4). Patients with
severe symptoms (grade 3 or higher) or those unable to tolerate
oral medications frequently require hospitalization for intravenous
steroid administration and close monitoring (19). Steroid tapering over 4-6 weeks is
recommended to reduce recurrence risk. In our case, infectious
causes were excluded, and the patient's symptoms improved rapidly
with bowel rest and hospitalization, allowing us to defer
corticosteroid therapy. Colonoscopy and histopathological
examination performed within 5 days of symptom onset confirmed the
diagnosis of irAE colitis, highlighting the value of early
endoscopic evaluation even in mild clinical courses.
Several studies have reported a positive association
between irAE occurrence and ICI efficacy, including overall
survival (OS). A meta-analysis published in 2021 demonstrated that
patients who experienced irAEs had significantly higher response
rates and improved OS than those who did not (20). These findings indicate that irAEs
may serve as a surrogate marker for effective immune activation and
therapeutic benefit. In our case, the emergence of irAEs may
similarly reflect an active antitumor immune response, contributing
to the favorable clinical outcome.
To the best of our knowledge, only few case reports
have described a dramatic response to Pembro-containing
chemotherapy in patients with metastatic or recurrent breast cancer
(21). Given that breast cancer
generally exhibits a low TMB, the efficacy of clinical ICIs in this
setting has been considered limited (6). Preclinical studies suggest that
tumor-draining lymph nodes play a central role in the antitumor
activity of immune checkpoint blockade, serving as key sites for
antigen presentation and T-cell priming (22,23).
Consistent with this concept, clinical observations in gastric
cancer have reported that nivolumab may be more effective in
patients with lymphatic metastases (24). Similarly, in the present case, the
predominant tumor burden consisted of lymph node metastases.
Therefore, the lymph node-dominant disease distribution may have
contributed to the favorable response to ICI therapy. However,
evidence supporting this hypothesis in OBC is currently limited.
Further studies are warranted to identify predictive biomarkers and
clinical contexts where ICIs could provide meaningful benefit for
patients with breast cancer.
This case has some limitations regarding diagnosis
evaluation and treatment decision-making. In the present case,
breast cancer was diagnosed based on ultrasonography, PET imaging,
and pathological confirmation of metastatic breast carcinoma in the
axillary lymph nodes. Mammography was not performed as the patient
declined the procedure, and breast MRI could not be performed
promptly owing to scheduling limitations. Therefore, this case did
not fully meet the strict contemporary diagnostic criteria for OBC,
as breast MRI is recommended by current guidelines (7,8) when
conventional imaging is negative was not performed. The possibility
of a small primary lesion detectable only by MRI cannot be
completely excluded. Nevertheless, systemic therapy was prioritized
because the patient had stage IV disease with lymph node
metastases. Furthermore, repeated CT imaging during the clinical
course did not demonstrate any breast lesions. Regarding irAEs,
guidelines indicate that ICI therapy can generally be continued in
patients with Grade 1 diarrhea (25-27).
In the present case, Pembro was temporarily withheld after
improvement of a preceding Grade 2 rash when Grade 1 diarrhea
subsequently developed. Although the diarrhea was mild, the
treatment was deferred owing to concerns of potential progression
to immune-related colitis, prioritizing patient safety.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
WI and MO conceptualized and designed the study, and
confirm the authenticity of all the raw data. KM, HI, TH, AO and TS
contributed to the clinical management of the patient, participated
in data acquisition and interpretation, and critically revised the
manuscript. EM, TK, ANa, AS, AF, YI, ANu, AA, HS and HY performed
the actual clinical treatments, and contributed to data collection
and interpretation. YM performed pathological evaluations and
contributed to data interpretation. All authors contributed to
drafting the manuscript or critically revised it for important
intellectual content, and read and approved the final version.
Ethics approval and consent to
participate
The Institutional Review Board Saitama Medical
University International Medical Center waived the ethical review
of the current case report for which patient consent for
publication was obtained.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this case report and accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
Use of artificial intelligence tools
During the preparation of this work, AI tools were
used to assist in literature search, and to identify relevant
terminology and phrasing, and subsequently, the authors revised and
edited the content produced by the AI tools as necessary, taking
full responsibility for the ultimate content of the present
manuscript.
References
|
1
|
Anders CK, Abramson V, Tan T and Dent R:
The evolution of triple-negative breast cancer: From biology to
novel therapeutics. Am Soc Clin Oncol Educ Book. 35:34–42.
2016.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Bianchini G, Balko JM, Mayer IA, Sanders
ME and Gianni L: Triple-negative breast cancer: Challenges and
opportunities of a heterogeneous disease. Nat Rev Clin Oncol.
13:674–690. 2016.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Cortes J, Cescon DW, Rugo HS, Nowecki Z,
Im SA, Yusof MM, Gallardo C, Lipatov O, Barrios CH, Holgado E, et
al: Pembrolizumab plus chemotherapy versus placebo plus
chemotherapy for previously untreated locally recurrent inoperable
or metastatic triple-negative breast cancer (KEYNOTE-355): A
randomised, placebo-controlled, double-blind, phase 3 clinical
trial. Lancet. 396:1817–1828. 2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Brahmer JR, Lacchetti C, Schneider BJ,
Atkins MB, Brassil KJ, Caterino JM, Chau I, Ernstoff MS, Gardner
JM, Ginex P, et al: Management of immune-related adverse events in
patients treated with immune checkpoint inhibitor therapy: American
Society of Clinical Oncology clinical practice guideline. J Clin
Oncol. 36:1714–1768. 2018.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Haanen JBAG, Carbonnel F, Robert C, Kerr
KM, Peters S, Larkin J and Jordan K: ESMO Guidelines Committee.
Management of toxicities from immunotherapy: ESMO Clinical Practice
Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 28
(suppl 4):iv119–iv142. 2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
O'Meara TA and Tolaney SM: Tumor
mutational burden as a predictor of immunotherapy response in
breast cancer. Oncotarget. 12:394–400. 2021.PubMed/NCBI View Article : Google Scholar
|
|
7
|
National Comprehensive Cancer Network:
NCCN Clinical Practice Guidelines in Oncology: Breast Cancer.
Version 4.2025. https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf.
Accessed August 1, 2025.
|
|
8
|
Loibl S, André F, Bachelot T, Barrios CH,
Bergh J, Burstein HJ, Cardoso MJ, Carey LA, Dawood S, Del Mastro L,
et al: Early breast cancer: ESMO clinical practice guideline for
diagnosis, treatment and follow-up. Ann Oncol. 35:159–182.
2024.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Ofri A and Moore K: Occult breast cancer:
Where are we at? Breast. 54:211–215. 2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Pittman KB, Olver IN, Koczwara B, Kotasek
D, Patterson WK, Keefe DM, Karapetis CS, Parnis FX, Moldovan S,
Yeend SJ, et al: Gemcitabine and carboplatin in carcinoma of
unknown primary site: A phase 2 Adelaide cancer trials and
education collaborative study. Br J Cancer. 95:1309–1313.
2006.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Inoue K, Ninomiya J, Saito T, Kimizuka K
and Kurosumi M: Induction therapy with paclitaxel and bevacizumab
followed by switch maintenance therapy with eribulin in Japanese
patients with HER2-negative metastatic breast cancer: A
multicenter, collaborative, open-label, phase II clinical study for
the SBCCSG 35 investigators. BMC Cancer. 18(671)2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Fizazi K, Greco FA, Pavlidis N, Daugaard
G, Oien K and Pentheroudakis G: ESMO Guidelines Committee: Cancers
of unknown primary site: ESMO clinical practice guidelines for
diagnosis, treatment and follow-up. Ann Oncol. 26 (Suppl
5):v133–v138. 2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Ettinger DS, Agulnik M, Cates JM, Cristea
M, Denlinger CS, Eaton KD, Fidias PM, Gierada D, Gockerman JP,
Handorf CR, et al: NCCN clinical practice guidelines Occult
primary. J Natl Compr Canc Netw. 9:1358–1395. 2011.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Bhatia SK, Saclarides TJ, Witt TR, Bonomi
PD, Anderson KM and Economou SG: Hormone receptor studies in
axillary metastases from occult breast cancers. Cancer.
59:1170–1172. 1987.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Kaufmann O, Deidesheimer T, Muehlenberg M,
Deicke P and Dietel M: Immunohistochemical differentiation of
metastatic breast carcinomas from metastatic adenocarcinomas of
other common primary sites. Histopathology. 29:233–240.
1996.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Wang DY, Mooradian MJ, Kim D, Shah NJ,
Fenton SE, Conry RM, Mehta R, Silk AW, Zhou A, Compton ML, et al:
Clinical characterization of colitis arising from anti-PD-1 based
therapy. Oncoimmunology. 8(e1524695)2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Weber JS, Kähler KC and Hauschild A:
Management of immune-related adverse events and kinetics of
response with ipilimumab. J Clin Oncol. 30:2691–2697.
2012.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Collins M, Soularue E, Marthey L and
Carbonnel F: Management of patients with immune checkpoint
inhibitor–induced enterocolitis: A systematic review. Clin
Gastroenterol Hepatol. 18:1393–1403.e1. 2020.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Marthey L, Mateus C, Mussini C, Nachury M,
Nancey S, Grange F, Zallot C, Peyrin-Biroulet L, Rahier JF,
Bourdier de Beauregard M, et al: Cancer immunotherapy with
anti-CTLA-4 monoclonal antibodies induces an inflammatory bowel
disease. J Crohns Colitis. 10:395–401. 2016.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Fan Y, Xie W, Huang H, Wang Y, Li G, Geng
Y, Hao Y and Zhang Z: Association of immune related adverse events
with efficacy of immune checkpoint inhibitors and overall survival
in cancers: A systemic review and meta-analysis. Front Oncol.
11(633032)2021.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Koi Y, Tajiri W, Kawasaki J, Akiyoshi S,
Ijichi H, Nakamura Y, Koga C, Koga Y, Taguchi K and Tokunaga E: A
dramatic response to an immune checkpoint inhibitor plus
chemotherapy in a patient with metastatic metaplastic carcinoma of
the breast: A case report. Thorac Cancer. 15:2073–2076.
2024.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Fransen MF, Schoonderwoerd M, Knopf P,
Camps MG, Hawinkels LJ, Kneilling M, van Hall T and Ossendorp F:
Tumor-draining lymph nodes are pivotal in PD-1/PD-L1 checkpoint
therapy. JCI Insight. 3(e124507)2018.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Mishima S, Kawazoe A, Nakamura Y, Sasaki
A, Kotani D, Kuboki Y, Bando H, Kojima T, Doi T, Ohtsu A, et al:
Clinicopathological and molecular features of responders to
nivolumab for patients with advanced gastric cancer. J Immunother
Cancer. 7(24)2019.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Oya S, Sato Y, Asaoka R, Sugawara K,
Okamoto A, Miwa Y, Yajima S, Yagi K, Yamashita H, Baba Y and Seto
Y: Lymphatic metastasis predicts better response to nivolumab in
recurrent or metastatic gastric cancer: Insights from
tumor-draining lymph node immunity and long-term outcomes.
Oncology. 1-9:2025.PubMed/NCBI View Article : Google Scholar : (Epub ahead of
print).
|
|
25
|
Schneider BJ, Naidoo J, Santomasso BD,
Lacchetti C, Adkins S, Anadkat M, Atkins MB, Brassil KJ, Caterino
JM, Chau I, et al: Management of immune-related adverse events in
patients treated with immune checkpoint inhibitor therapy: ASCO
guideline update. J Clin Oncol. 39:4073–4126. 2021.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Haanen J, Obeid M, Spain L, Carbonnel F,
Wang Y, Robert C, Lyon AR, Wick W, Kostine M, Peters S, et al:
Management of toxicities from immunotherapy: ESMO clinical practice
guideline for diagnosis, treatment and follow-up. Ann Oncol.
33:1217–1238. 2022.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Thompson JA, Schneider BJ, Brahmer J, Zaid
MA, Achufusi A, Armand P, Berkenstock MK, Bermas B, Braaten T,
Budde LE, et al: NCCN Guidelines® Insights: Management of
immunotherapy-related toxicities, version 2.2024. J Natl Compr Canc
Netw. 22:582–592. 2024.PubMed/NCBI View Article : Google Scholar
|