Introduction
Massive ovarian edema is a rare gynecological entity
resembling a solid ovarian tumor due to the accumulation of
edematous fluid within the ovarian stroma, first described by
Kalstone et al in 1969(1) and
defined by the World Health Organization as an accumulation of
edematous fluid within the ovarian stroma separating normal
follicular structures. Massive edema of the ovary is a rare
condition affecting mainly young women (mean age, 20 years);
however, premenarcheal (2) or
menopausal women (3) have been
reported to be affected as well. Massive ovarian edema is
characterized by a build-up of interstitial fluid without
neoplastic changes, and it is mainly considered to be the
consequence of torsion of the ovary, despite the fact that there
are several reported cases without torsion observed during surgery
(4-7).
However, this condition can be easily mistaken for a neoplasm,
resulting in overtreatment by the removal of the whole affected
ovary. Conservative treatment is recommended for this entity,
particularly when preservation of fertility is important.
Therefore, the accuracy of preoperative diagnosis should be
improved by taking massive ovarian edema into consideration when
solid enlargement of the ovary is detected.
The present study describes the case of a
28-year-old woman who presented with massive ovarian edema with
paraovarian cyst torsion and was successfully treated with
conservative laparoscopic surgery owing to the accurate
preoperative diagnosis.
Case report
A 28-year-old woman (gravida 1, para 1) visited a
local clinic due to mild left lower abdominal pain lasting for 1
week. The patient's medical history and family history did not
reveal any abnormalities. Her menstrual cycle was regular at 28
days, and she had experienced menarche at the age of 12 years. An
ultrasonographic examination revealed two loculated left ovarian
masses and the patient was referred to the Osaka City University
Hospital (Osaka, Japan) for further evaluation.
The patient did not suffer from abdominal pain when
she visited the hospital. Upon a physical examination, the uterus
was found to be anteverted, anteflexed and resembled a hen's egg in
size; a slightly painful left adnexal mass was palpated, whereas
the right adnexa was not palpable during a bimanual examination.
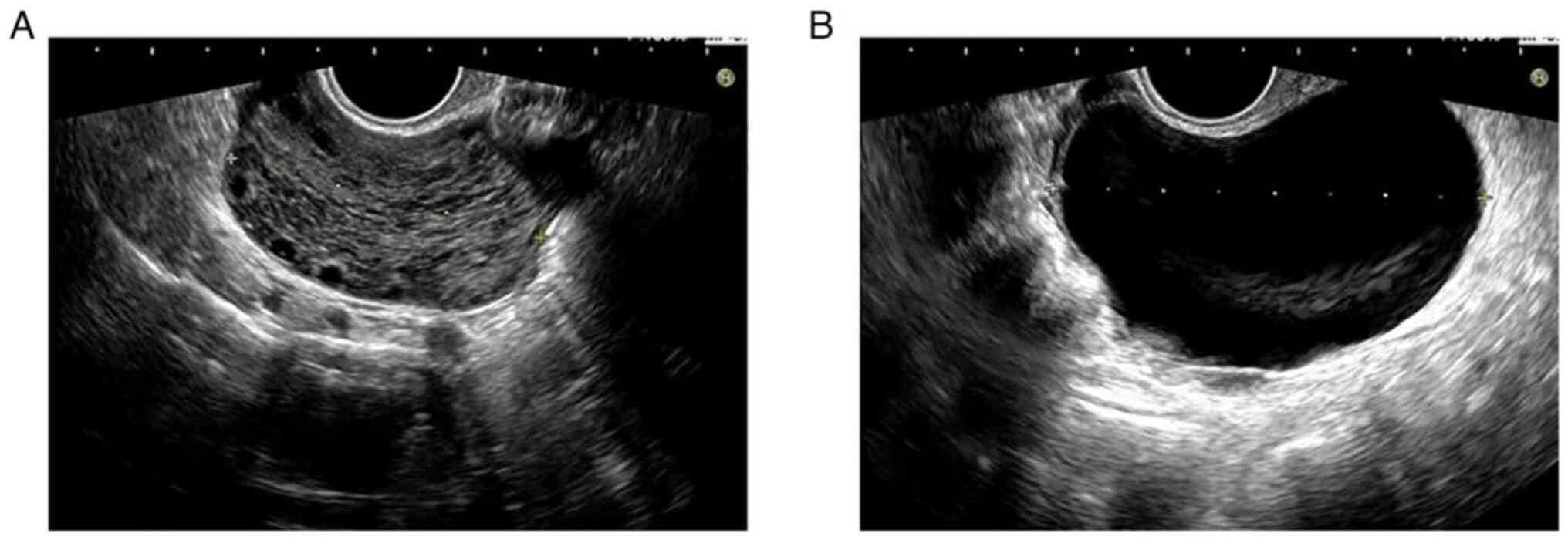
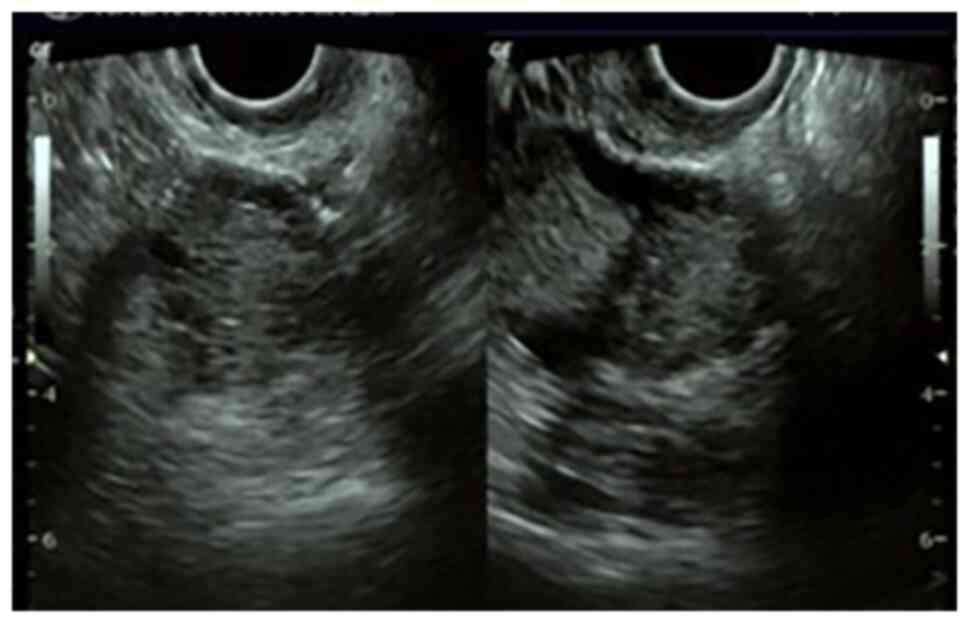
There was no hirsutism or signs of virilization. The transvaginal
ultrasonographic examination performed at the hospital revealed a
77.9-mm cystic lesion and a 57.7-mm solid lesion with multiple
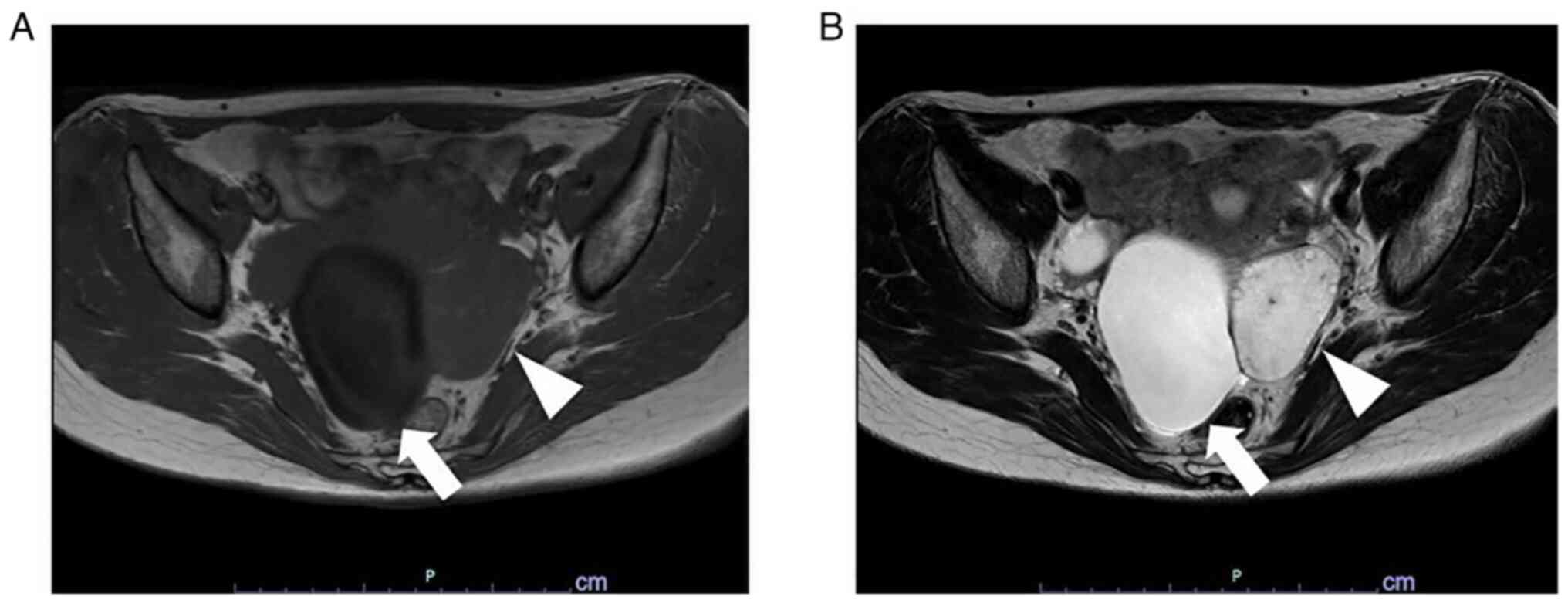
peripheral ovarian follicles in the left adnexa (Fig. 1). The magnetic resonance imaging
(MRI) examination revealed a 55-mm lesion with multiple peripheral
ovarian follicles, which was isointense on T1-weighted images and
hyperintense on T2-weighted images, and a 75-mm cystic lesion
without a solid component, which was hypointense on T1-weighted
images and hyperintense on T2-weighted images in the left adnexa
(Fig. 2). The right ovary was
normal, exhibiting only a small functional cyst. There were no
observed abnormalities of the right adnexa or the uterus. A
laboratory examination revealed normal complete blood count,
electrolyte levels, liver and renal function tests, C-reactive
protein and lactate dehydrogenase levels; the serum level of
carbohydrate antigen (CA) 125 was 13 U/ml (normal limits, ≤35 U/ml)
(8), while that of CA19-9 was <2
U/ml (normal limits, ≤37 U/ml) (9),
that of carcinoembryonic antigen was 1.3 ng/ml (normal limits,
<5 ng/ml) (10) and that of
Sialyl-Tn was 20.6 U/ml (normal limits, ≤45 U/ml) (11), which were all within normal
limits.
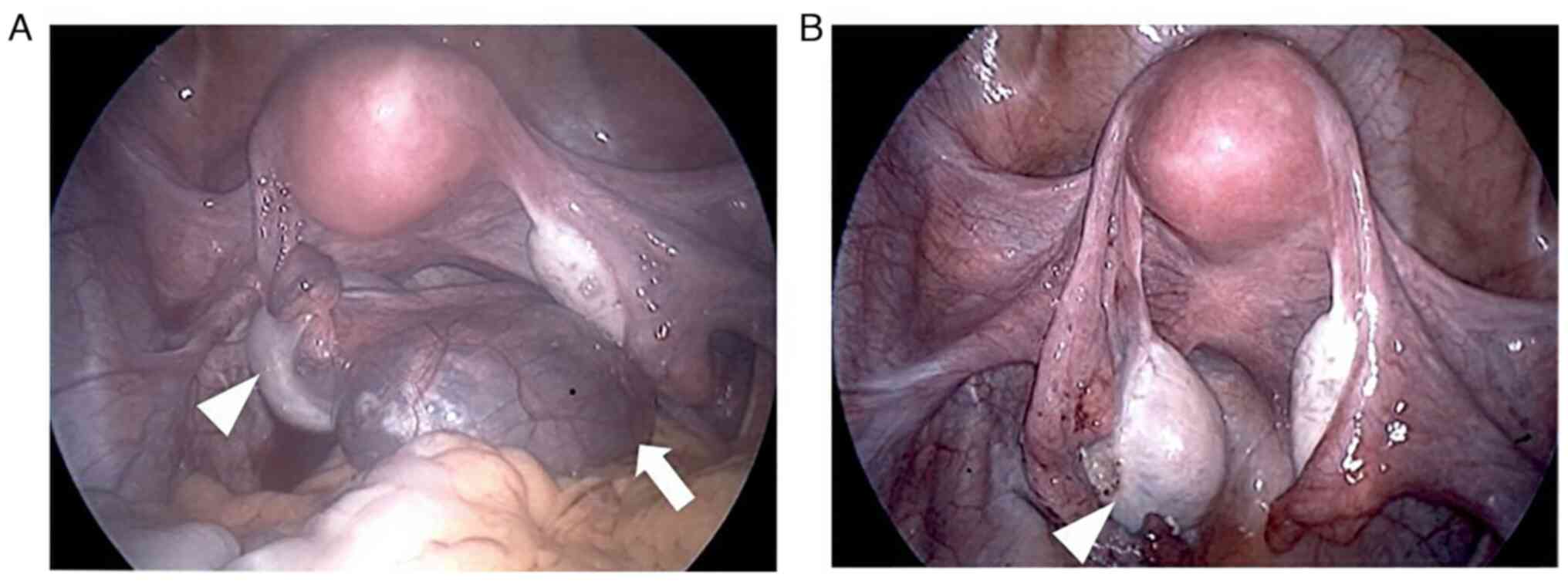
Laparoscopic surgery was performed based on the
clinical suspicion of a massive ovarian edema with paraovarian cyst
torsion. A paraovarian cyst was identified in the left adnexa; the
left adnexa was twisted 360˚, and the left ovary appeared enlarged,
with a white and opaque external surface (Fig. 3A). The right adnexa and uterus were
normal in appearance and there was no ascites. Following detorsion
of the left adnexa, the size of the enlarged left ovary gradually
returned to almost normal (Fig. 3B).
The diagnosis of a massive ovarian edema was considered likely, due
to the shrinkage in size following detorsion and the findings of
the pre-operative ultrasonographic and MRI examinations. A
substantial amount of paraovarian cyst fluid was drained using the
SAND balloon catheter (Hakko Shoji Co., Ltd.), as previously
described by Yagihashi et al (12) without spillage of the cyst contents;
the paraovarian cyst was resected, resulting in the successful
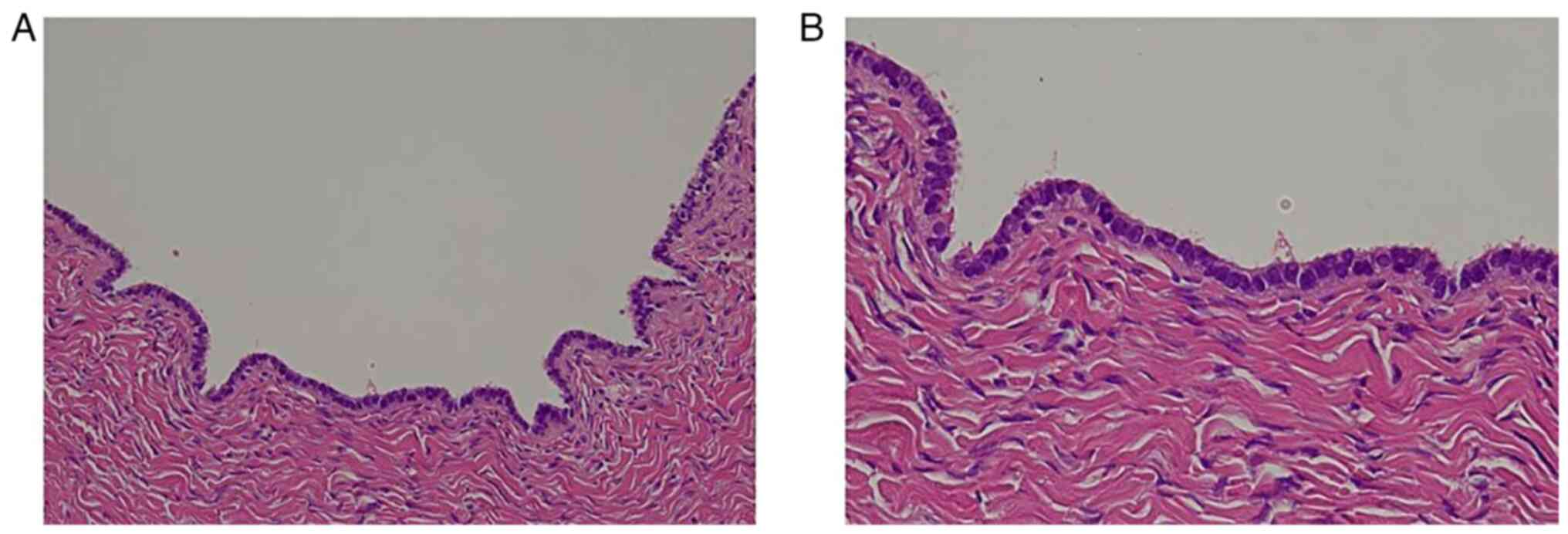
preservation of the whole left ovary. Following surgery, the
pathological examination using hematoxylin and eosin staining
(performed by the Department of Pathology, Osaka City University
Graduate School of Medicine, Osaka, Japan) as routine clinical work
of the paraovarian cyst revealed a serous cystadenoma without any
malignant characteristics (Fig. 4).
At the 1-month post-operative follow-up visit at the hospital, an
ultrasonographic examination confirmed normal-sized bilateral
ovaries and uterus (Fig. 5).
In the case presented herein, the diagnosis of
massive ovarian edema was not confirmed by a pathological
examination; however, the diagnosis of a massive ovarian edema was
based on the other available evidence, including the identification
of multiple ovarian follicles at the periphery of the enlarged
ovary, which shrank following detorsion.
Discussion
Massive ovarian edema was first described in 1969 by
Kalstone et al (1) as a
‘massive, solid enlargement of the ovary associated with
interstitial edema, without neoplastic changes’. The etiology is
unknown; however, it may result from the partial intermittent
torsion of the ovary causing venous and lymphatic obstruction, to
the extent that it interferes with venous and lymphatic drainage,
but is not sufficient to cause necrosis. The removal of
high-molecular-weight proteins from the interstitium of the ovary
can be hindered by any degree of compression at the ovarian hilum,
which is followed by an increase in the osmotic pressure, resulting
in edema formation. This causes the shutdown of the lymphatic
capillary pores and results in a vicious cycle of accumulation of
increased amounts of fluid in the interstitium of the ovary.
According to this mechanism, lymphatic blockage may occur even in
the absence of complete torsion (13). Massive ovarian edema is a rare entity
affecting mainly young women. Therefore, it is crucial to recognize
this entity, as it is often misdiagnosed as a malignant ovarian
tumor, placing the young patient at risk of overtreatment and
resulting in the loss of hormonal function and fertility. The most
common presenting symptoms include recurrent intermittent abdominal
pain, abdominal distension or an abdominal mass, menstrual
abnormalities, infertility and, in some cases, virilization and
precocious puberty (14). The excess
amounts of androgen secreted by luteinized stromal cells in the
edematous ovary are considered to cause androgenic manifestations
(4). In cases in which the torsion
is acute, the most common symptom is acute abdominal pain that may
mimic an acute abdomen. In the cases in which the torsion is
gradual, a provoked stromal luteinization may cause virilization in
the patient (15).
There are two types of massive ovarian edema,
depending on the presence or absence of concomitant pathological
findings predisposing to the partial torsion of the mesovarium.
Primary massive ovarian edema is an entity without a concomitant
pathology, whereas secondary massive ovarian edema is an entity
superimposed on already diseased ovaries (16). The most favored hypothesis for the
etiology is obstructed venous and lymphatic circulation, but not
arterial blood flow, due to the complete or partial torsion of the
ovary, leading to the development of a massive ovarian edema
(13). As a result, stromal cell
luteinization is induced, due to the response of the edematous
ovary to torsion and subsequent ischemia, which causes hormone
production (17). There are estrogen
and progesterone receptors in stromal cells, and mechanical
stimulation due to stretching of the stroma by the edematous fluid
may lead to hormone-related symptoms (13,14,18).
Another explanation for the hormone-related changes is the
deregulated expression of a local paracrine factor, such as
epidermal growth factor, insulin-like growth factor or cytokines
(18). Secondary massive ovarian
edema occurs in diseased ovaries, such as those with an ovarian
mass or cyst-like ovarian capillary hemangioma (19), serous and mucinous cyst adenomas
(6), mature cystic teratoma
(20), ovarian fibrothecoma
(21), polycystic ovary syndrome
(22) and Meigs syndrome (23), and may also occur as a consequence of
drug treatment for ovulation induction (24) and in some malignancies (25,26).
Malignancies reported to cause ovarian lymphatic vessel obstruction
by metastatic carcinoma cells include gastric carcinoma (26), uterine cervical cancer (25) and lymphangitis carcinomatosa
(27).
Although there are no diagnostic imaging criteria,
ultrasonography and MRI have been reported to be the most useful
modalities for diagnosing this entity. Umesaki et al
(28) reported that a solid ovarian
tumor with multiple peripheral ovarian follicles on
ultrasonographic examination may indicate a possible preoperative
diagnosis of massive ovarian edema. Furthermore, another report by
Umesaki et al (29) using MRI
demonstrated that the main indicator of massive ovarian edema is an
enlarged ovary with edematous stroma exhibiting high intensity on
T2-weighted images, with multiple ovarian follicles pressed towards
the peripheral cortical area of the ovary by the edematous fluid
accumulated within the ovarian stroma. Similarly, Hall et al
(30) also reported that the
presence of multiple ovarian follicles situated around the
periphery of the cortex of the enlarged ovary on MRI is a crucial
sign that indicates massive ovarian edema. Therefore, the finding
of multiple ovarian follicles located at the peripheral cortex of
an enlarged ovary is considered to be a crucial diagnostic evidence
of massive ovarian edema.
The morphological characteristics of massive ovarian
edema are as follows: The external surface of the ovary is usually
white and opaque, or grayish and glistening; on cross section the
internal surface is grey in color and typically watery fluid oozes
out from the cut surface due to the edematous pressure; and, in the
majority of cases, the ovary has a rubbery consistency (13,15).
Histologically, the ovarian architecture is
preserved, but with an edematous and hypocellular ovarian stroma,
and a thickened and fibrotic outer cortex. In cases with endocrine
symptoms, a cluster of luteinized stromal cells is occasionally
observed (31). There is diffuse
edema confined to the medullary stroma and the spared cortex. Small
subcortical follicular cysts, and uniformly dilated blood and
lymphatic vessels are observed (15). Necrosis and hemorrhage are unusual,
as the torsion commonly causes venous and lymphatic obstruction,
but not arterial occlusion (31).
Focal stromal luteinization has been noted in some of the studied
cases, and it is considered to be a mechanical stimulation of
proliferation and luteinization of stromal cells induced by
stretching of the stroma due to lymphedema (14). Nogales et al (15) reported no histopathological evidence
of a proliferative process, such as fibromatosis, and concluded
that massive edema of the ovary is a reactive, non-proliferative
state of specific stromal cells due to torsion of the ovary.
In the case present herein, the MRI findings were
typical of a massive ovarian edema, demonstrating an enlarged ovary
with edematous stroma that appeared hyperintense on T2-weighted
images, with multiple ovarian follicles pressed towards the
peripheral cortical area of the ovary. Based on the characteristic
MRI images and prior knowledge of this entity, the condition was
diagnosed pre-operatively as a massive ovarian edema. The fact that
the size of the enlarged ovary returned to almost normal following
detorsion of the adnexa intraoperatively further confirmed the
suspected clinical diagnosis, and the affected adnexa was preserved
by simply removing the paraovarian cyst.
Due to the lack of awareness of this entity and its
resemblance to a neoplastic disease, more aggressive treatment than
necessary is often undertaken, with a resultant loss of fertility
and hormonal function. The differential diagnosis of massive
ovarian edema should be taken into consideration in young women
presenting with a complex solid ovarian mass with multiple
peripheral ovarian follicles, particularly in cases with a history
of recurrent abdominal pain. An accurate pre-operative evaluation,
with careful inspection of the ovary and other organs or tissues in
the abdominal cavity, may prevent unnecessary surgery, including
oophorectomy, particularly in young women with massive ovarian
edema.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
TF and TS conceived and designed the study. TF, KI,
MY, MK, TI and TY acquired, examined and interpreted the data of
the patient. TF and TS drafted and revised the manuscript. TF and
TS confirm the authenticity of all the raw data. All the authors
have read and approved the final manuscript.
Ethics approval and consent to
participate
Written informed consent was obtained from the
patient depicted in the present case report.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of the case details and any
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kalstone CE, Jaffe RB and Abell MR:
Massive edema of the ovary simulating fibroma. Obstet Gynecol.
34:564–571. 1969.PubMed/NCBI
|
|
2
|
Heiss KF, Zwiren GT and Winn K: Massive
ovarian edema in the pediatric patient: A rare solid tumor. J
Pediatr Surg. 29:1392–1394. 1994.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Shirk JO, Copas PR and Kattine AA: Massive
ovarian edema in a menopausal woman. A case report. J Reprod Med.
41:359–362. 1996.PubMed/NCBI
|
|
4
|
Thomas RL, Carr BR, Ziadie MS and Wilson
EE: Bilateral mucinous cystadenomas and massive edema of the
ovaries in a virilized adolescent girl. Obstet Gynecol.
120:473–476. 2012.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Peters FH, Brunell C and Benjamin E:
Massive ovarian edema and contralateral mature cystic teratoma:
Asymptomatic presentation in a premenarchal female. J Pediatr
Adolesc Gynecol. 22:e118–e120. 2009.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Khalbuss WE and Dipasquale B: Massive
ovarian edema associated with ovarian serous cystadenoma: A case
report and review of the literature. Int J Gynecol Cancer. 16
(Suppl 1):S326–S330. 2006.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Harke AB, Sigamani K, Thukkaram C,
Ramamurthy M and Sekar M: Massive ovarian oedema-a case report. J
Clin Diagn Res. 10:Ed03–Ed04. 2016.
|
|
8
|
Alagoz T, Buller RE, Berman M, Anderson B,
Manetta A and DiSaia P: What is a normal CA125 level? Gynecol
Oncol. 53:93–97. 1994.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Luo G, Jin K, Guo M, Cheng H, Liu Z, Xiao
Z, Lu Y, Long J, Liu L, Xu J, et al: Patients with normal-range
CA19-9 levels represent a distinct subgroup of pancreatic cancer
patients. Oncol Lett. 13:881–886. 2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Flamini E, Mercatali L, Nanni O, Calistri
D, Nunziatini R, Zoli W, Rosetti P, Gardini N, Lattuneddu A,
Verdecchia GM and Amadori D: Free DNA and carcinoembryonic antigen
serum levels: An important combination for diagnosis of colorectal
cancer. Clin Cancer Res. 12:6985–6988. 2006.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Hashiguchi Y, Kasai M, Fukuda T, Ichimura
T, Yasui T and Sumi T: Serum sialyl-Tn (STN) as a tumor marker in
patients with endometrial cancer. Pathol Oncol Res. 22:501–504.
2016.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Yagihashi Y, Kato K, Nagahama K, Yamamoto
M and Kanamaru H: A case of laparoscopic excision of a huge
retroperitoneal cystic lymphangioma. Case Rep Urol.
2011(712520)2011.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Geist RR, Rabinowitz R, Zuckerman B, Shen
O, Reinus C, Beller U and Lara-Torre E: Massive edema of the ovary:
A case report and review of the pertinent literature. J Pediatr
Adolesc Gynecol. 18:281–284. 2005.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Natarajan A, Wales JK, Marven SS and
Wright NP: Precocious puberty secondary to massive ovarian oedema
in a 6-month-old girl. Eur J Endocrinol. 150:119–123.
2004.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Nogales FF, Martin-Sances L,
Mendoza-Garcia E, Salamanca A, González-Nuñez MA and Pardo Mindán
FJ: Massive ovarian oedema. Histopathology. 28:229–234.
1996.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Bychkov V and Kijek M: Massive ovarian
edema. Four cases and some pathogenetic considerations. Acta Obstet
Gynecol Scand. 66:397–399. 1987.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Chervenak FA, Castadot MJ, Wiederman J and
Sedlis A: Massive ovarian edema: Review of world literature and
report of two cases. Obstet Gynecol Surv. 35:677–684.
1980.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Eden JA: Massive ovarian oedema. Br J
Obstet Gynaecol. 101:456–458. 1994.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Gehrig PA, Fowler WC Jr and Lininger RA:
Ovarian capillary hemangioma presenting as an adnexal mass with
massive ascites and elevated CA-125. Gynecol Oncol. 76:130–132.
2000.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Lakhey M, Upreti D, Kulshrestha R and Rani
S: Massive ovarian edema with contralateral mature cystic
teratoma-a case report of an uncommon combination. Indian J Pathol
Microbiol. 46:219–221. 2003.PubMed/NCBI
|
|
21
|
Sakaki M, Hirokawa M, Horiguchi H,
Wakatsuki S, Sano T and Izumi Y: Ovarian fibrothecoma with massive
edema. J Med Invest. 47:148–151. 2000.PubMed/NCBI
|
|
22
|
Guvenal T, Cetin A and Tasyurt A:
Unilateral massive ovarian edema in a woman with polycystic
ovaries. Eur J Obstet Gynecol Reprod Biol. 99:129–130.
2001.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Spurrell EL, Yeo YC, Rollason TP and
Judson IR: A case of ovarian fibromatosis and massive ovarian
oedema associated with intra-abdominal fibromatosis, sclerosing
peritonitis and Meig's syndrome. Sarcoma. 8:113–121.
2004.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Kawaguchi R, Ueda S, Tsuji Y, Haruta S,
Kanayama S, Yamada Y, Ooi H and Kobayashi H: Massive ovarian edema
in pregnancy after ovulation induction using clomiphene citrate.
Arch Gynecol Obstet. 277:375–378. 2008.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Krasević M, Haller H, Rupcić S and Behrem
S: Massive edema of the ovary: A report of two cases due to
lymphatic permeation by metastatic carcinoma from the uterine
cervix. Gynecol Oncol. 93:564–567. 2004.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Bazot M, Detchev R, Cortez A, Uzan S and
Darai E: Massive ovarian edema revealing gastric carcinoma: A case
report. Gynecol Oncol. 91:648–650. 2003.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Wong SY: Bilateral massive ovarian
oedema-report of a case due to lymphangiitis carcinomatosa.
Virchows Arch A Pathol Anat Histopathol. 414:355–358.
1989.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Umesaki N, Tanaka T, Miyama M and Kawamura
N: Sonographic characteristics of massive ovarian edema. Ultrasound
Obstet Gynecol. 16:479–481. 2000.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Umesaki N, Tanaka T, Miyama M, Nishimura
S, Kawamura N and Ogita S: Successful preoperative diagnosis of
massive ovarian edema aided by comparative imaging study using
magnetic resonance and ultrasound. Eur J Obstet Gynecol Reprod
Biol. 89:97–99. 2000.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Hall BP, Printz DA and Roth J: Massive
ovarian edema: Ultrasound and MR characteristics. J Comput Assist
Tomogr. 17:477–479. 1993.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Young RH and Scully RE: Fibromatosis and
massive edema of the ovary, possibly related entities: A report of
14 cases of fibromatosis and 11 cases of massive edema. Int J
Gynecol Pathol. 3:153–178. 1984.PubMed/NCBI View Article : Google Scholar
|