Introduction
Angiosarcoma is a rare and highly aggressive cancer
originating from the endothelial cells of blood and lymphatic
vessels, comprising <1% of sarcoma cases (1-3).
This malignancy can affect any part of the body, but pulmonary
involvement is particularly rare (4). Although the majority of cases occur
spontaneously, risk factors such as radiation, chronic lymphedema,
exposure to vinyl chloride and genetic syndromes have been
documented in the literature (3).
Primary pulmonary angiosarcoma is an aggressive but rare cancer of
the pulmonary arteries that is malignant in nature. Secondary
pulmonary angiosarcoma where lung metastasis from some other
origin, such as the heart or breast occurs more often (4,5).
Metastatic pulmonary angiosarcoma often presents with non-specific
symptoms, complicating and delaying the diagnosis (4,6). Given
the clinical and pathological similarities between primary and
metastatic pulmonary angiosarcoma, excluding other tumor sites is
often necessary for diagnosing primary pulmonary angiosarcoma
(5). Angiosarcoma is the most common
malignancy affecting the heart, and the lungs are the most common
site of malignancy (7). Early
detection plays a critical role in the workup and management of
pulmonary angiosarcoma and having a high clinical suspicion
augments early detection (4).
In pulmonary angiosarcoma, hemoptysis is a critical
and alarming symptom indicative of tumor invasion into the
pulmonary vasculature (8-11).
Hemoptysis as an initial presentation is rare and is often
accompanied by other symptoms related to other metastatic sites or
systemic involvement (8-10).
The non-specific presentation of primary angiosarcoma is even more
complex in patients with other underlying comorbidities. In
immunocompromised patients, hemoptysis can occur due to
opportunistic infections (~80%), or other malignancies related to
immunodeficiency, such as Kaposi's sarcoma (12,13).
This overlapping symptomatology between pulmonary angiosarcoma,
infections, and other malignancies can further delay diagnosis and
appropriate treatment, further complicating the clinical picture.
In terms of radiographic evidence, the review compiled by Yogi
et al (14) indicated that
the halo sign was observed in 58% of patients on a computed
tomography (CT) scan of the chest. Among the patients of 28 cases
of primary pulmonary angiosarcoma summarized in the study by Yogi
et al (14), 50% of patients
(14/28) had multiple nodules (14).
Solitary lesions appeared in 39.3% of patients (11/28). They also
noted that patients with multiple nodules had more aggressive
courses and poorer prognosis compared to their single-lesioned
counterparts (14).
The present study describes the case a case of
metastatic pulmonary angiosarcoma in an human immunodeficiency
virus (HIV)-positive patient presenting with hemoptysis and
multisystem involvement. This serves to highlight the diagnostic
challenges associated with this condition and the importance of
considering rare malignancies in differential diagnoses,
particularly in patients with complex medical histories.
Case report
A 36-year-old African American male patient with HIV
on highly active antiretroviral therapy who initially presented to
the HCA Florida North Florida Hospital Emergency Department with 3
weeks of progressive hemoptysis (day 1). He reported recent
exposure to mold following flooding and renovations in his
apartment. His symptoms began as a mild, intermittent cough with
clear sputum, which progressed to hemoptysis, shortness of breath,
fatigue, post-tussive chest and back pain, and palpitations. Upon
his arrival, he was alert but frail, with conjunctival pallor,
borderline tachycardia and coarse breath sounds.
Initial laboratory tests revealed microcytic anemia
(Hgb, 8.4 g/dl), thrombocytopenia (platelets, 52 K/µl) and markedly
elevated D-dimer levels (19,119 ng/ml). The CD4 count was 447, and
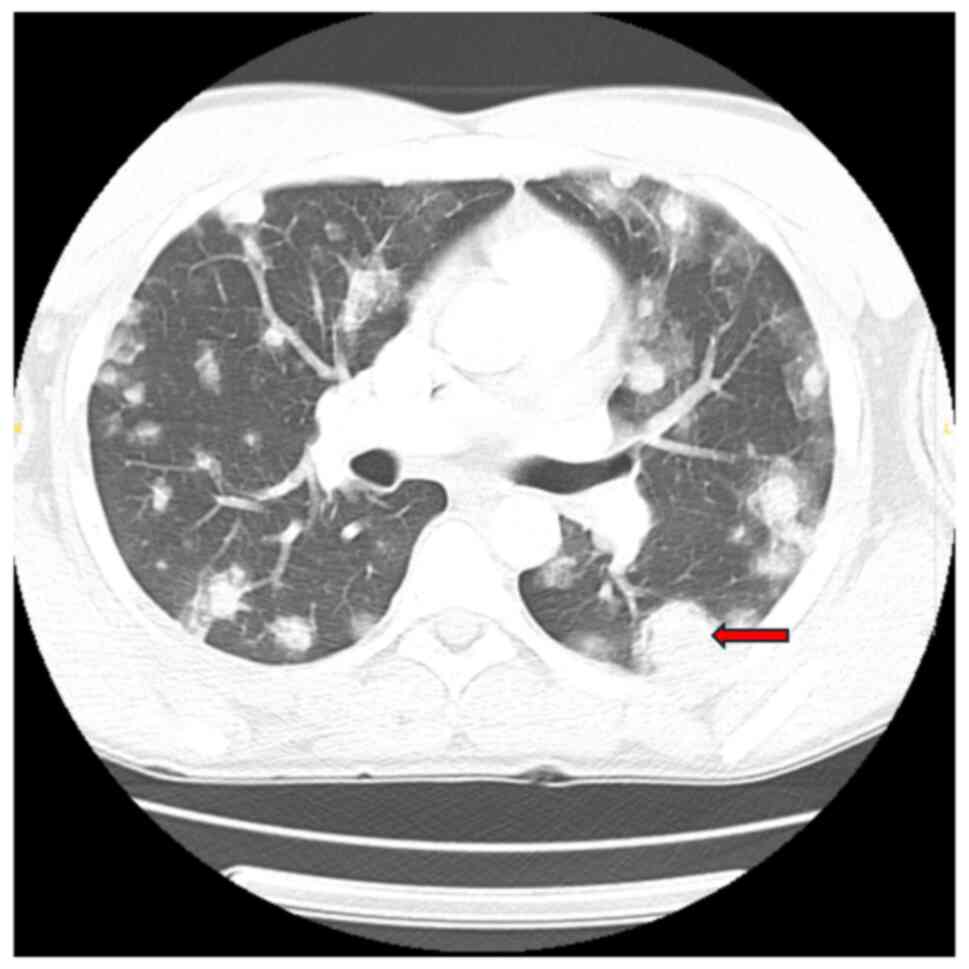
the HIV viral load was undetectable. Imaging upon admission
revealed innumerable bilateral pulmonary nodules with peripheral
ground-glass halos, the largest measuring 29x24 mm in the left
lower lobe, along with enlarged hilar lymph nodes (up to 14x15 mm
on the left and 14x21 mm on the right), hepatic lesions and lytic
bone lesions, all suggestive of metastatic disease (Fig. 1). Given his immunocompromised state,
mold exposure history and imaging findings, initial concerns
included opportunistic fungal infections, Kaposi's sarcoma and
metastatic malignancy.
A robotic-assisted bronchoscopy with transbronchial
biopsy and bronchoalveolar lavage (BAL) was performed on day 3.
Blood was noted throughout the tracheobronchial tree, although no
focal bleeding source was identified. The BAL fluid culture grew
Haemophilus influenzae, and he was commenced on ceftriaxone
2 g daily for 5 days (day 6). Fungal, Acid-fast bacillus and
tuberculosis workups were negative. Transthoracic echocardiography
on day 8 revealed a large (7.4x3.3 cm) mobile mass on the atrial
side of the tricuspid valve, initially raising concern for
culture-negative endocarditis. In the setting of HIV, this prompted
empiric treatment with continuation of ceftriaxone 2 g daily and
vancomycin 1 g every 8 h, and serological testing for
Bartonella, Q fever and Brucella was ordered. A
dental evaluation was also pursued to assess for potential
infectious sources. Blood cultures remained negative throughout his
hospitalization periods.
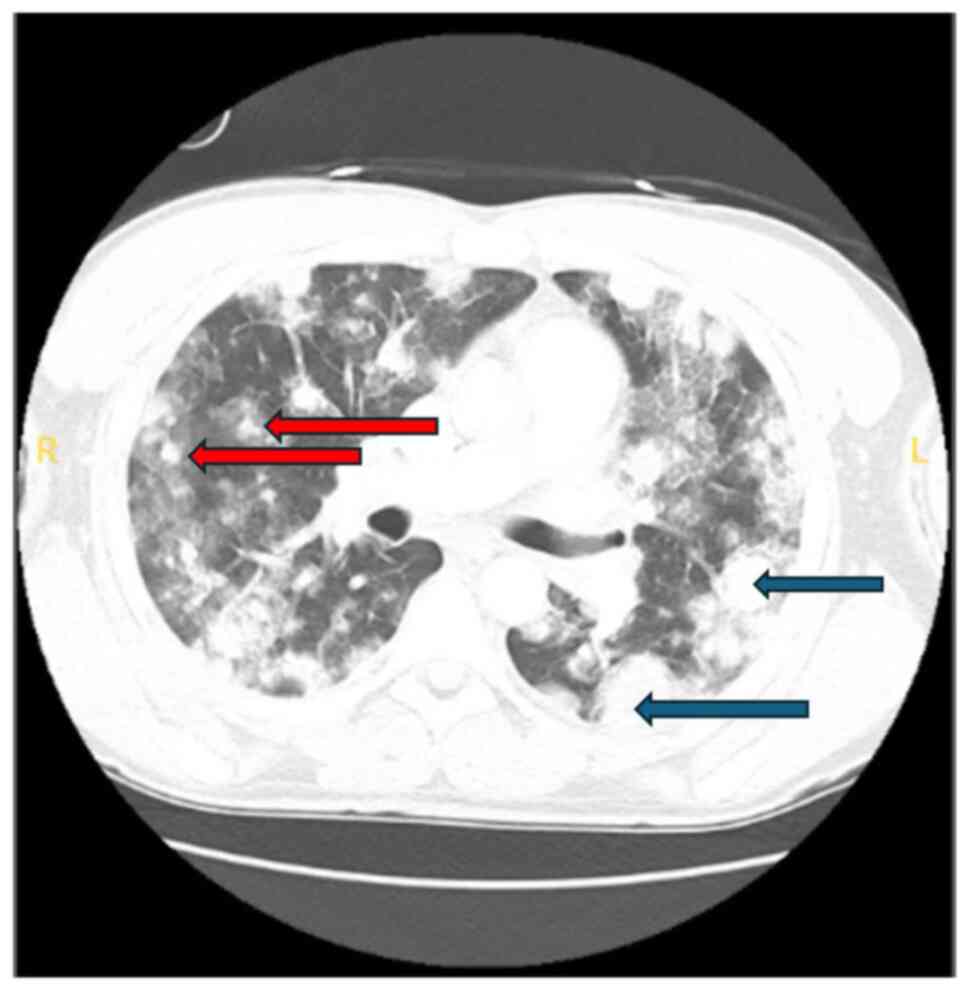
A CT scan on day 14 revealed an interval increase in
the size and number of nodules, with the largest left-sided mass
now measuring 4.2x3.1 cm, and a right-sided mass along the major
fissure measuring 2.9x1.8 cm, along with new right hilar adenopathy
measuring up to 2.3x1.6 cm (Fig.
2).
The patient departed from the hospital day 16,
against medical advice (AMA), prior to the biopsy results, citing
fatigue with the prolonged workup. He returned 5 days later (day
21) with worsening hemoptysis and dyspnea. Laboratory tests
revealed a hemoglobin level of 6.6 g/dl and a platelet count of 37
K/µl. He was transfused and stabilized. The pathological analysis
of the initial biopsy sample, reviewed at a tertiary center,
confirmed stage IV pulmonary angiosarcoma with immunohistochemistry
positivity for ERG, CD31, CD34 and CD117, and negativity for STAT6,
HHV8 and ALK (Fig. 3). These results
excluded more common HIV-associated malignancies, such as Kaposi's
sarcoma and ruled out inflammatory myofibroblastic tumor and
solitary fibrous tumor.
The Oncology Department initiated weekly paclitaxel
therapy, 160 mg once weekly (3 weeks on, 1 week off) on day 24, a
first-line agent with demonstrated efficacy in angiosarcoma. He
initially tolerated the first dose, but again departed from the
hospital, AMA, on day 29 before receiving subsequent treatment. He
returned several days later (day 39) with severe dyspnea and was
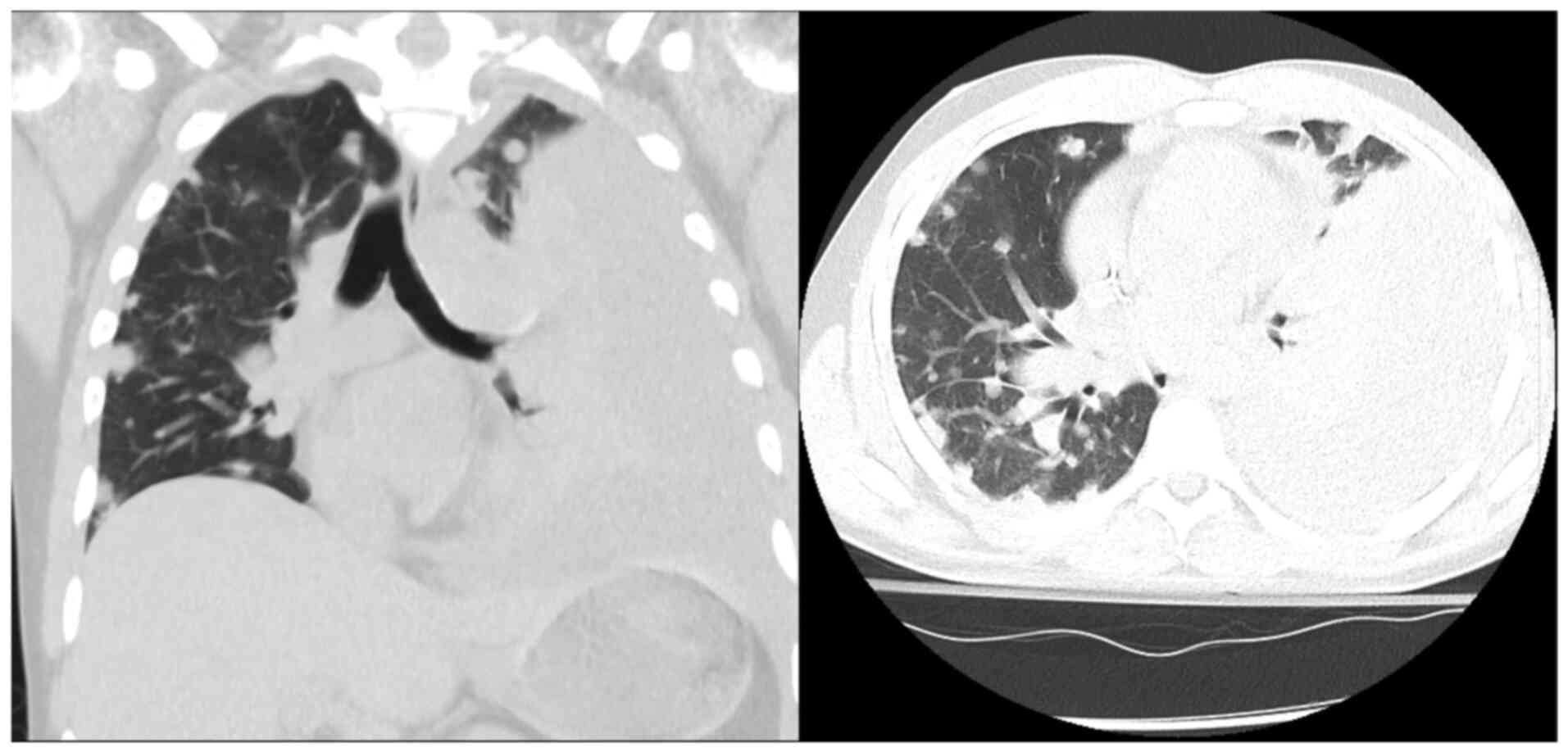
found to have a large left pleural effusion. Chest tube placement
on day 45 drained 1.35 liters of bloody fluid, consistent with
hemothorax, a common complication of angiosarcoma due to
tumor-induced vascular fragility. Cytology from both the pleural
and later pericardial effusions observed on the CT scan was
negative for malignancy, with no malignant cells identified
(Fig. 4).
During his second attempt at paclitaxel treatment on
day 41, he experienced a grade 2 infusion reaction characterized by
dyspnea and hypoxia, necessitating the discontinuation of
treatment. Given the reaction severity and limited access to close
outpatient monitoring, he was transitioned to doxorubicin 60
mg/m2. He received his first dose of doxorubicin on day
50 and tolerated it well. He continued with a second cycle on day
64 without major complications. Repeat CT imaging following two
cycles of doxorubicin (day 70) demonstrated a marked improvement in
pulmonary and hepatic metastases (Fig.
5), supporting a degree of chemotherapeutic responsiveness.
Despite early signs of treatment benefits, his
course was complicated by a progressive pericardial effusion. On
day 106 of hospitalization, shortly after using the bathroom, he
experienced acute abdominal pain, diaphoresis, hypotension and
oxygen desaturation. A rapid response was called, and a bedside
echocardiogram revealed cardiac tamponade with right ventricular
collapse. He was urgently transferred to the cardiovascular
intensive care unit, where emergent pericardiocentesis was
performed, draining 800 ml hemorrhagic fluid. He was stabilized
with supportive care and was commenced on colchicine 0.6 mg twice
daily, and ibuprofen 800 mg every 8 h for pericardial inflammation.
Both medications were continued for 14 days while admitted, and he
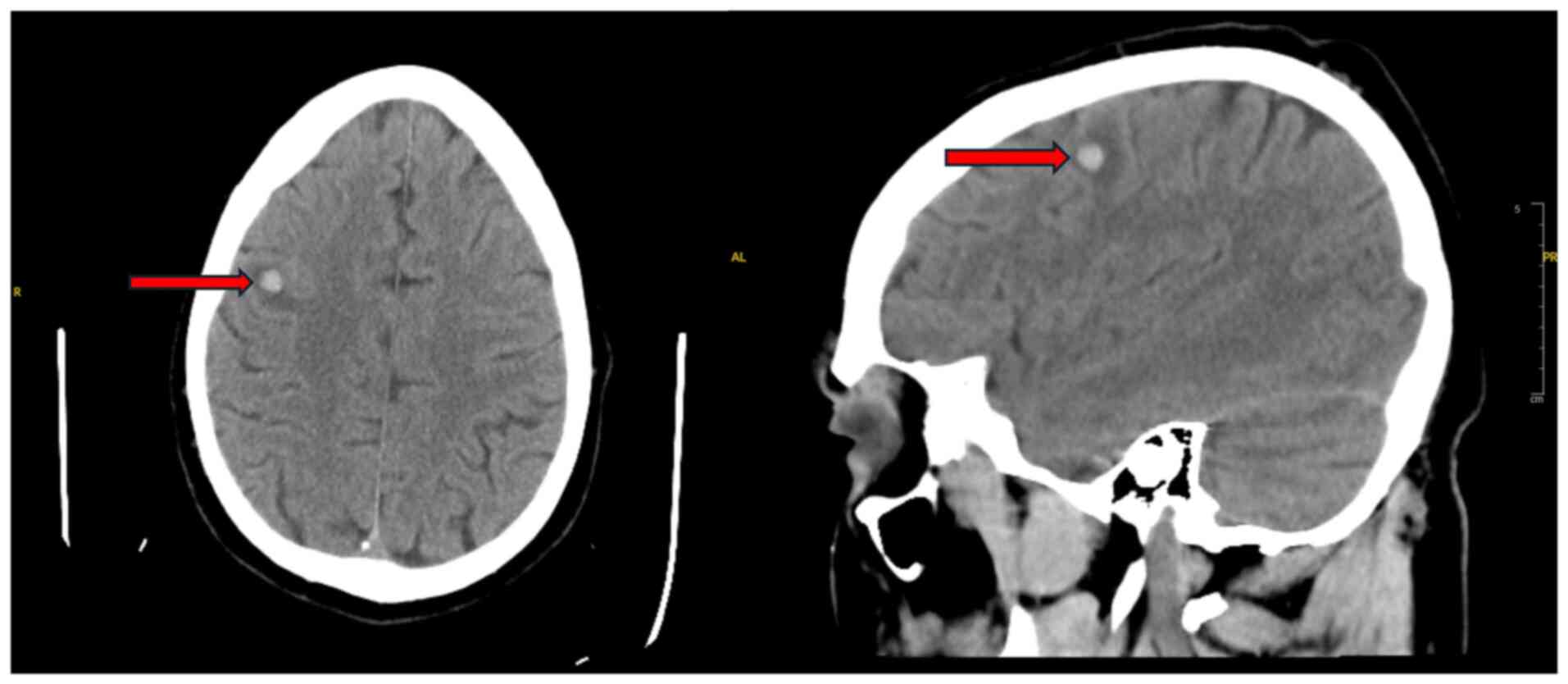
was discharged with the same regimen. A CT head scan performed
during this admission revealed a right frontal hemorrhagic
metastasis with surrounding edema (Fig.
6).
Although discharged home, he returned repeatedly
over the following weeks with hemoptysis, shortness of breath and
refractory metastatic pain. He was readmitted for fluid
reaccumulation (day 85), requiring a second pericardiocentesis (day
90). Over time, his performance status declined. He initially
enrolled in hospice care, but later revoked his do-not-resuscitate
order (DNR) status and pursued further treatment following
perceived clinical improvement. Despite this, the disease continued
to progress, and he again decompensated. He and his family engaged
in comprehensive goals-of-care discussions with the palliative care
team. Expressing concern about suffering and being a burden to his
loved ones, he opted for comfort-centered care and formally signed
a DNR (day 109). He was discharged to hospice care on hospital day
135, where he later passed away peacefully. The clinical timeline
is summarized in Table I.
 | Table ITimeline of clinical events. |
Table I
Timeline of clinical events.
| Time point | Clinical events |
|---|
| Day 1 | Presentation with 3
weeks of hemoptysis. CT chest scan revealed bilateral nodules with
halo sign. Placed in isolation. Initial labs show anemia,
thrombocytopenia, high D-dimer levels. |
| Day 3 | Robotic bronchoscopy
with biopsy and BAL. Blood in airways noted. BAL sent for cytology
and cultures. |
| Day 6 | BAL culture grows
Haemophilus influenzae. Ceftriaxone started. Fungal and TB
workup negative. |
| Day 8 | TTE revealed 7.4x3.3
cm mass on atrial side of tricuspid valve. Empiric vancomycin
commenced for possible culture-negative endocarditis. |
| Day 13 | Biopsy suggestive of
spindle cell sarcoma. Sent for external review. |
| Day 16 | Patient left
AMA. |
| Day 21 | Returned with
worsening hemoptysis. Hgb 6.6, platelets, 37 K. Transfused. Biopsy
confirmed angiosarcoma (ERG+, CD31+,
CD34+, CD117+). |
| Day 24-25 | Paclitaxel commenced.
Port placed. |
| Day 29 | Left AMA again,
missed outpatient oncology follow-up. |
| Day 39 | Returned with
dyspnea. Imaging stable. Planned to resume chemotherapy
inpatient. |
| Day 41 | Grade 2 reaction to
second dose of paclitaxel. Transitioned to doxorubicin. |
| Day 45 | Became more
hypoxemic. CT scan revealed large pleural effusion. Chest tube
placed, drains 1.35 liters bloody fluid. |
| Day 54 | Second cycle of
doxorubicin administered. Imaging revealed a partial response. |
| Day 61 | Discharged home. |
| Day 69 | Returned with
shoulder pain and dyspnea. CT scan revealed ~50% reduction in tumor
burden. Scheduled for outpatient chemotherapy, discharged with pain
medications. |
| Day 73 | Returned for pain
control due to a lack of outpatient medications, given another
prescription and instructed to follow-up outpatient. |
| Day 85 | Admitted with
intractable nausea. Echocardiogram revealed moderate pericardial
effusion. |
| Day 90 | Pericardiocentesis
performed; 800 ml hemorrhagic fluid removed. |
| Day 94 | Discharged on
colchicine and NSAIDs. |
| Day 106 | Returned with another
pericardial effusion and tamponade physiology. Emergent
pericardiocentesis performed. Head CT scan revealed hemorrhagic
brain metastasis. |
| Day 109 | Signs DNR. Discharged
to hospice. |
| Day 131 | Returned with
hemoptysis. Interventional pulmonology deemed bleeding
non-localizable. Referred to hospice again. |
| Day 135 | Returned once more
with chest pain and hemoptysis. No further interventions pursued.
Final discharge to hospice. |
Discussion
Pulmonary angiosarcoma is a malignant, yet rare
disease that has non-specific lung symptoms that lead to delay in
diagnosis and attributability to more usual conditions (15-17).
The case in the present study depicts the diagnostic and
therapeutic challenges of the disease. The non-specificity of
symptoms of hemoptysis, cough and dyspnea renders pulmonary
angiosarcoma a clinical imitator that frequently imitates
infectious pneumonia, tuberculosis and other malignancies (18,19). In
immunocompromised patients, such as in patients with HIV, the
initial suspicion tends to lean toward infectious disease rather
than uncommon primary pulmonary malignancy.
Radiologically, pulmonary angiosarcoma tends to
exhibit numerous pulmonary nodules in 50% of cases that possess
characteristics of nodules, ground-glass opacities, or halo signs,
a presentation that is typically associated with cases of fungal or
hemorrhagic metastases (20,21). Tricuspid valve mass in this context
was yet another clue for the differential diagnoses of cardiac
angiosarcoma or metastatic disease. Primary pulmonary angiosarcoma
could also be a possibility, as it has been shown to manifest as
either single or multiple pulmonary nodules (22).
Histopathologic confirmation remained the gold
standard, with strong positivity for CD31, ERG and CD34 supporting
the diagnosis of angiosarcoma. These vascular markers are commonly
expressed in endothelial malignancies and help distinguish
angiosarcoma from other sarcomas and primary lung tumors. Negative
staining for STAT6, ALK and HHV8 effectively excluded solitary
fibrous tumors, inflammatory myofibroblastic tumors and Kaposi's
sarcoma, respectively (23-27).
CD117 (c-KIT), while also positive in this case, is less specific
and can be expressed in a range of neoplasms, including
gastrointestinal stromal tumors, seminomas and some melanomas. In
angiosarcoma, CD117 expression has been reported but is considered
supportive rather than definitive. Therefore, its diagnostic
utility lies in being interpreted alongside more
endothelial-specific markers like CD31 and ERG (28,29).
Pulmonary angiosarcoma is associated with a poor
prognosis, particularly in patients with more than one pulmonary
mass, who have much poorer outcomes than patients with a solitary
mass (15). Accelerated disease
course and poor responsiveness to chemotherapy account for poor
survival in these patients (22).
Paclitaxel remains a first-line chemotherapeutic agent with
demonstrated efficacy in angiosarcoma; however, the patient
described herein was unable to tolerate it, necessitating a switch
to doxorubicin (22). While no
standardized treatment regimen has been established, therapy
selection is often guided more by patient tolerability than by
effectiveness (22).
A unique characteristic of this case was the
presence of a tricuspid valve mass that manifested either by direct
invasion of the heart or by seeding from the primary tumor.
Although primary cardiac angiosarcomas have their characteristic
localization in the right atrium, secondary cardiac disease is
generally more appreciated in the context of disseminated disease
(30). This presentation provides an
element of complexity to treatment as cardiac metastases have
greater thrombotic potential and hemodynamic impairment (31). Hemorrhagic features of the effusions
in angiosarcoma are in accordance with tumor-caused vascular
fragility that leads to intrapulmonary and pericardial hemorrhage
(32).
In conclusion, pulmonary angiosarcoma is an
exceedingly rare and aggressive malignancy that presents
significant diagnostic and therapeutic challenges, often mimicking
infectious or other malignant processes. The present case report
illustrates the diagnostic complexity of pulmonary angiosarcoma in
the setting of HIV, where extensive pulmonary and cardiac
involvement contributes to a poor prognosis, and highlights the
importance of maintaining a high index of suspicion for
angiosarcoma in immunocompromised patients presenting with
unexplained pulmonary nodules, hemoptysis and cardiac
abnormalities.
Acknowledgements
The authors would like to express their gratitude
sincere appreciation to the HCA North Florida Hospital for their
support and assistance towards the completion of this project with
mentorship and access patient charts. The resources and support
provided by the hospital was invaluable in facilitating this
study.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
All authors (GM, SP, HH, MK, AR and LJ) were
responsible for the clinical workup, literature review and drafting
of the manuscript. All authors (GM, SP, HH, MK, AR and LJ)
contributed to the case interpretation and manuscript revision. All
authors have read and approved the final version of the manuscript
to be published. All authors (GM, SP, HH, MK, AR and LJ) confirm
the authenticity of all the raw data.
Ethics approval and consent to
participate
The present case report was conducted in accordance
with institutional guidelines. Consent was obtained from the
patient for described herein for the presentation of his case.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of this case report and any
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
Use of artificial intelligence tools
During the preparation of this work, AI tools were
used to improve the readability and language of the manuscript or
to generate images, and subsequently, the authors revised and
edited the content produced by the AI tools as necessary, taking
full responsibility for the ultimate content of the present
manuscript.
References
|
1
|
Young RJ, Brown NJ, Reed MW, Hughes D and
Woll PJ: Angiosarcoma. Lancet Oncol. 11:983–991. 2010.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Zhang J, Gong H, Wang Y, Zhang G and Hou
P: Angiosarcoma of the visceral organs: A morphological,
immunohistochemical, and C-MYC status analysis. Pathol Res Pract.
238(154118)2022.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Florou V and Wilky BA: Current management
of angiosarcoma: Recent advances and lessons from the past. Curr
Treat Options Oncol. 22(61)2021.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Khalid K, Khan A, Lomiguen CM and Chin J:
Clinical detection of primary pulmonary angiosarcoma. Cureus.
13(e17059)2021.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Obeso Carillo GA, García Fontán EM,
Cañizares Carretero MÁ and Pérez Pedrosa A: Primary pulmonary
angiosarcoma, an exceptional neoplasm with a poor prognosis:
Reports of two cases and review of the literature. Gen Thorac
Cardiovasc Surg. 61:643–647. 2013.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Darawsha F, Kramer R, Raanani E and Saute
M: Angiosarcoma of the main pulmonary artery-hand-made conduit
reconstruction. Interact Cardiovasc Thorac Surg.
35(35)2022.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Jain G, Mukhopadhyay S, Kurien S, Yusuf J,
Tyagi S and Jain R: Ruptured cardiac angiosarcoma with pulmonary
metastases: A rare disease with a common (mis)diagnosis! Indian
Heart. J. 64:603–606. 2012.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Shimabukuro I, Yatera K, Noguchi S,
Kawanami Y, Iwanami T, Nishida C, Yamasaki K, Kawanami T, Ishimoto
H, So T, et al: Primary pulmonary angiosarcoma presenting with
hemoptysis and Ground-glass opacity: A case report and literature
review. Tohoku J Exp Med. 237:273–278. 2015.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Piechuta A, Przybyłowski T, Szołkowska M
and Krenke R: Hemoptysis in a patient with multifocal primary
pulmonary angiosarcoma. Pneumonol Alergol Pol. 84:283–289.
2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Pan Z, An Z, Li Y and Zhou J: Diffuse
alveolar hemorrhage due to metastatic angiosarcoma of the lung: A
case report. Oncol Lett. 10:3853–3855. 2015.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Chen J, Li C, Tian Y and He Y: 18F-FDG
PET/CT findings in a rare case of primary pulmonary angiosarcoma.
Japanese J Clin Oncol. 52:286–287. 2022.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Nelson JE and Forman M: Hemoptysis in
HIV-infected patients. Chest. 110:737–743. 1996.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Aboulafia DM: The Epidemiologic,
pathologic, and clinical features of AIDS-associated pulmonary
Kaposi's sarcoma. Chest. 117:1128–1145. 2000.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Yogi A, Miyara T, Ogawa K, Iraha S, Matori
S, Haranaga S and Murayama S: Pulmonary metastases from
angiosarcoma: A spectrum of CT findings. Acta Radiol. 57:41–46.
2016.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Sofia J, Moreira N, Ferreira MJ and
Antunes M: Angiosarcoma arising from the main pulmonary artery
mimicking pulmonary thromboembolism. Arq Bras Cardiol. 109:90–91.
2017.PubMed/NCBI View Article : Google Scholar : (In English,
Portuguese).
|
|
16
|
Kim JB, Kim SH, Lim SY, Roh SY, Cho G,
Song HJ, Park S, Lee J and Kim SJ: Primary angiosarcoma of the
pulmonary trunk mimicking pulmonary thromboembolism.
Echocardiography. 27:E23–E26. 2010.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Hsing JM, Thakkar SG, Borden EC and Budd
GT: Intimal pulmonary artery sarcoma presenting as dyspnea. Case
report. Int Semin Surg Oncol. 4(14)2007.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Scheffel H, Stolzmann P, Plass A, Weber A,
Prêtre R, Marincek B and Alkadhi H: Primary intimal pulmonary
artery sarcoma: A diagnostic challenge. J Thorac Cardiovasc Surg.
135:949–950. 2008.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Lakmal Samarasinghe, Manoharan A, Dinusha
Dharmaratna, Nathani Z and Cedeno H: Angiosarcoma of lung: A
diagnostic challenge. CHEST J. 164:A4525–6. 2023.
|
|
20
|
Saito M, Saraya T, Oda M, Minamishima T,
Kongoji K, Isomura A, Fujiwara M, Soejima K and Ishii H: Rapidly
progressive respiratory failure with multiple halo signs on
computed tomography in a patient with primary cardiac angiosarcoma
derived from the right atrium: A case report. BMC Pulm Med.
20(321)2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Luan T, Hao J, Gu Y, He P, Li Y, Wang L,
Deng H, Guan W, Lin X, Xie X, et al: A clinical analysis and
literature review of eleven cases with primary pulmonary
angiosarcoma. BMC Cancer. 24(1597)2024.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Miettinen M, Wang Z, Sarlomo-Rikala M,
Abdullaev Z, Pack SD and Fetsch JF: ERG expression in epithelioid
sarcoma. Am J Surg Pathol. 37:1580–1585. 2013.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Sullivan HC, Edgar MA, Cohen C, Kovach CK,
HooKim K and Reid MD: The utility of ERG, CD31 and CD34 in the
cytological diagnosis of angiosarcoma: An analysis of 25 cases. J
Clin Pathol. 68:44–50. 2014.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Yoshida A, Tsuta K, Ohno M, Yoshida M,
Narita Y, Kawai A, Asamura H and Kushima R: STAT6
Immunohistochemistry is helpful in the diagnosis of solitary
fibrous tumors. Am J Surg Pathol. 38:552–559. 2014.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Lobato F: Mesenchymal tumors of the
digestive system. https://atlasgeneticsoncology.org/solid-tumor/209310.
Accessed March 22, 2025.
|
|
26
|
Miettinen M: Immunohistochemistry of soft
tissue tumours-review with emphasis on 10 markers. Histopathology.
64:101–118. 2014.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Ren Y, Zhu M, Liu Y, Diao X and Zhang Y:
Primary pulmonary angiosarcoma: Three case reports and literature
review. Thoracic Cancer. 7:607–613. 2016.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Miettinen M and Lasota J: KIT (CD117): A
review on expression in normal and neoplastic tissues, and
mutations and their clinicopathologic correlation. Appl
Immunohistochem Mol Morphol. 13:205–220. 2005.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Darre T, Djiwa T, N'Timon B, Simgban P,
Tchaou M and Napo-Koura G: Breast primary angiosarcoma: A
clinicopathologic and imaging study of a series cases. Breast
Cancer (Auckl). 16(11782234221086726)2022.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Yamashita H, Higashida T, Huchioka A,
Asakawa Y, Nambu A, Ohyatsu S, Kohyama T, Takahashi M, Hayashi T
and Tago M: Cardiac angiosarcoma with metastatic to lung, brain,
and bone. Radiol Case Rep. 19:473–478. 2023.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Le AN, Nguyen AV, Nguyen TN, Kirkpatrick
JN, Nguyen HT and Thu T: Cardiac metastasis mimicking STEMI-impact
of point-of-care ultrasound on clinical decision-making: A case
report. Front Cardiovasc Med. 10(1098154)2013.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Chen FF, Jiang SF, Dong C, Che Y, Du LY,
Li ZY, Yang ZQ, Zhao YC and Liu Y: Case Report: Thromboembolism and
hemorrhagic pericardial Effusion-The Janus face of primary
pericardial angiosarcoma. Front Cardiovasc Med.
7(618146)2021.PubMed/NCBI View Article : Google Scholar
|