Introduction
Acute coronary syndrome (ACS) may present with a
wide spectrum of symptoms, and the absence of chest pain is well
recognized, particularly among women and patients with diabetes.
Diabetic autonomic neuropathy can blunt the perception of ischemic
pain, leading to atypical manifestations, such as nausea, vomiting,
abdominal discomfort or generalized weakness, rather than classic
substernal chest pain. These atypical presentations are associated
with a delayed diagnosis, suboptimal treatment and worse clinical
outcomes, contributing to the higher mortality rates observed among
women with myocardial infarction (1-4).
Electrocardiography remains a cornerstone in the
evaluation of suspected ACS, and dynamic changes on serial
electrocardiograms (ECGs) are critical for detecting evolving
ischemia, particularly in non-ST-elevation presentations (5,6). Certain
ECG patterns, including diffuse ST-segment depressions and T wave
inversions with upright T waves in aVR and V1, have been shown to
be associated with severe multivessel or left-main equivalent
coronary artery disease and carry significant prognostic
implications (7).
Gabapentinoids, including pregabalin and gabapentin,
are commonly prescribed for diabetic neuropathy; however, their use
has been linked to adverse cardiovascular outcomes and may further
obscure the recognition of ischemic symptoms in high-risk patients
(8-10).
The present case report describes a case of atypical ACS in a
diabetic woman receiving pregabalin, ultimately found to have
severe multivessel coronary artery disease.
Case report
A 57-year-old woman with type 2 diabetes mellitus,
hypertension, hyperlipidemia, obesity, chronic obstructive
pulmonary disease, arthritis, migraines, and a 40-pack-year smoking
history presented to the Emergency Department of Wellstar Spalding
Medical Center (Griffin, GA, USA) on September 27, 2025 with
sudden-onset nausea and bilious vomiting without chest pain. She
reported constipation and generalized weakness. Her home
medications included pregabalin at 300 mg three times daily.
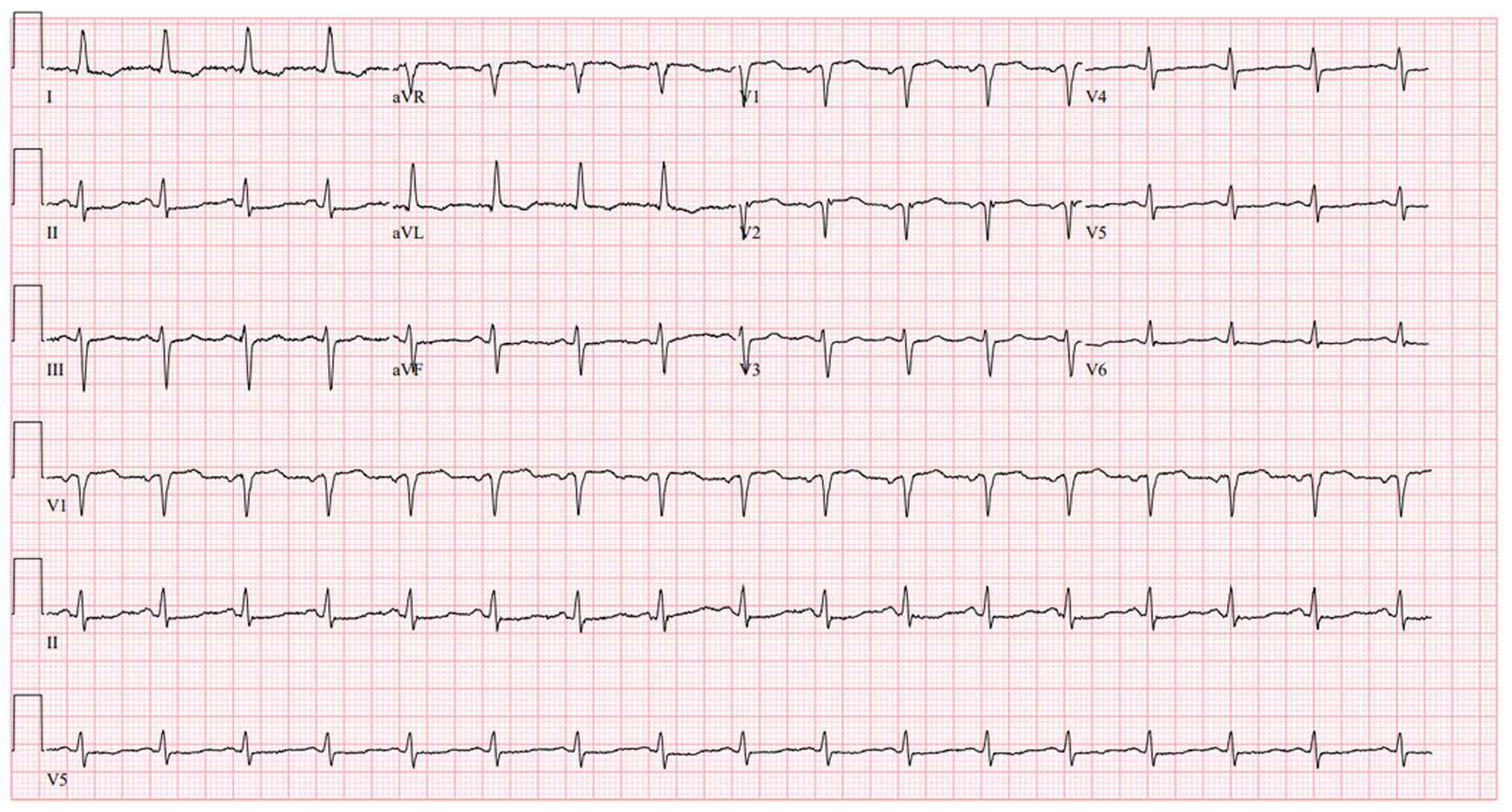
An initial evaluation revealed mildly elevated, yet
rising high sensitivity troponin T (103 → 129 → 161 ng/l),
non-specific ECG changes characterized by low-voltage QRS complexes
and T-wave flattening in V4-V6 (Fig.
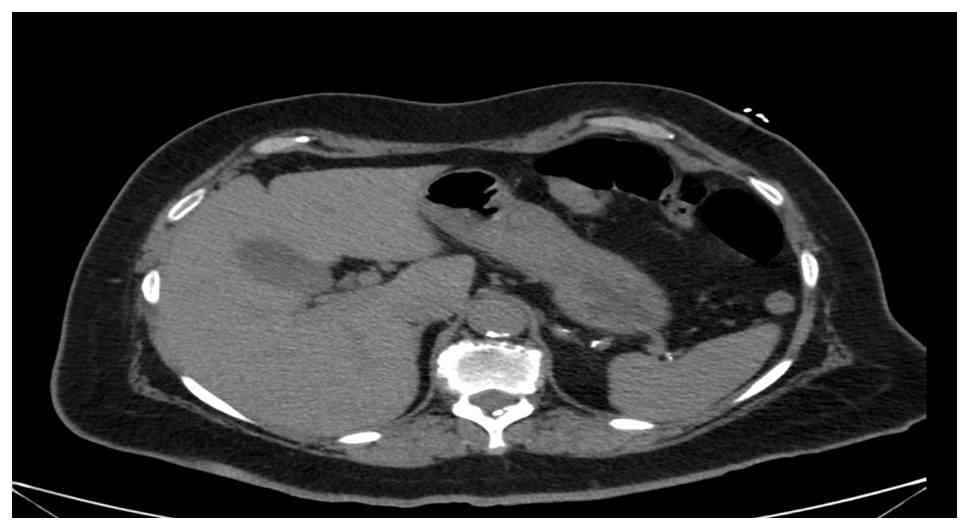
1) and a normal chest radiograph; an abdominal computed
tomography (CT) scan (Fig. 2) did
not reveal any notable findings. Despite the elevated levels of
cardiac biomarkers, the absence of chest pain and improving
gastrointestinal symptoms led to a working diagnosis of non-cardiac
etiology. She received aspirin (81 mg), statin therapy
(atorvastatin, 80 mg), β-blocker (metoprolol succinate, 100 mg) and
a heparin drip for 48 h and supportive care and was discharged
following presumed stabilization.
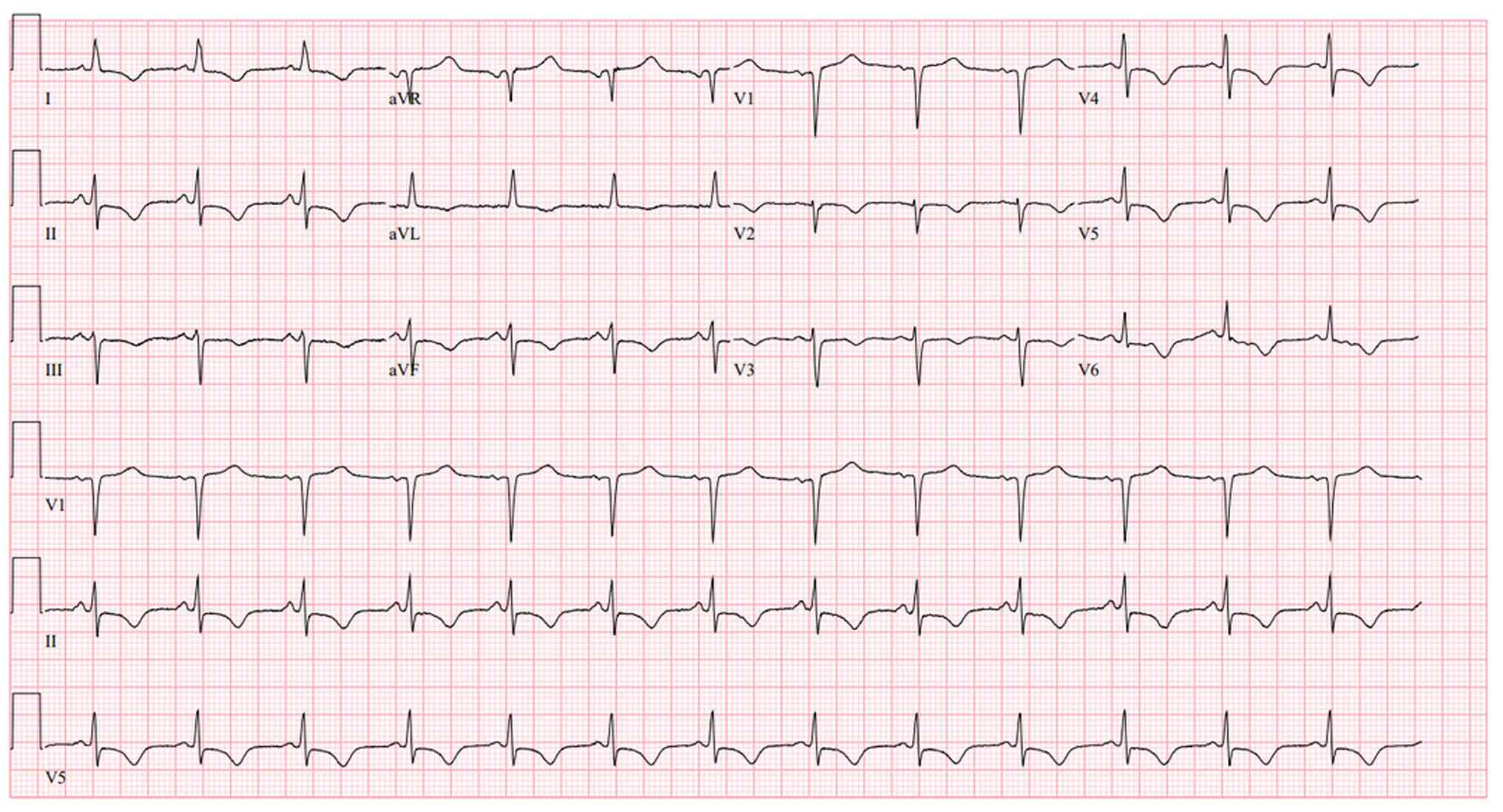
However, within 24 h, the patient returned with
persistent nausea, vomiting and new dull periumbilical pain. A
repeat ECG demonstrated diffuse ST-segment depressions with T-wave
inversions in inferior (II, III and aVF), lateral (I, aVL and
V5-V6) and anterior (V2-V4) leads, along with upright T waves in
aVR and V1 (Fig. 3). High
sensitivity troponin T was down-trending (~64 ng/l). Her
thrombolysis in myocardial infarction (TIMI) score was 5, and the
Global Registry of Acute Coronary Events (GRACE) score was 103.
Transthoracic echocardiography revealed a severely reduced left
ventricular ejection fraction (25-30%) and grade I diastolic
dysfunction.
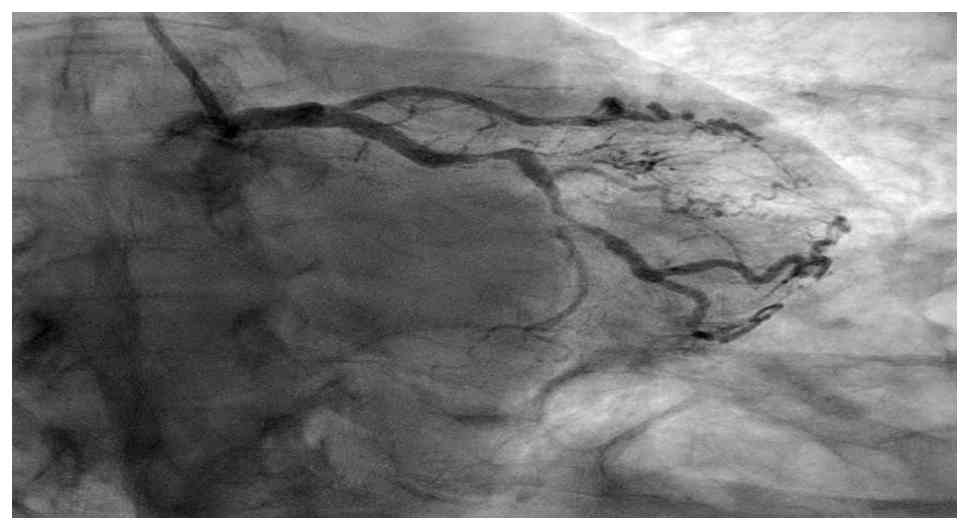
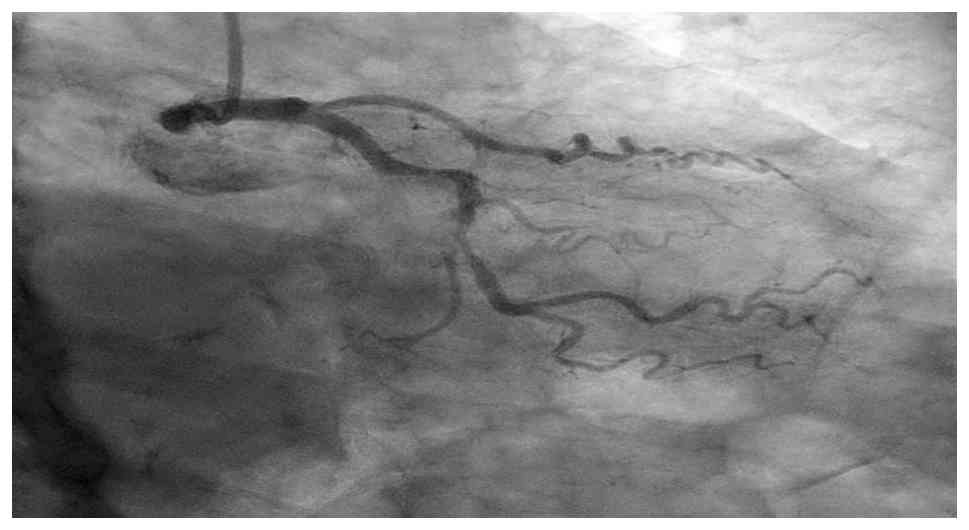
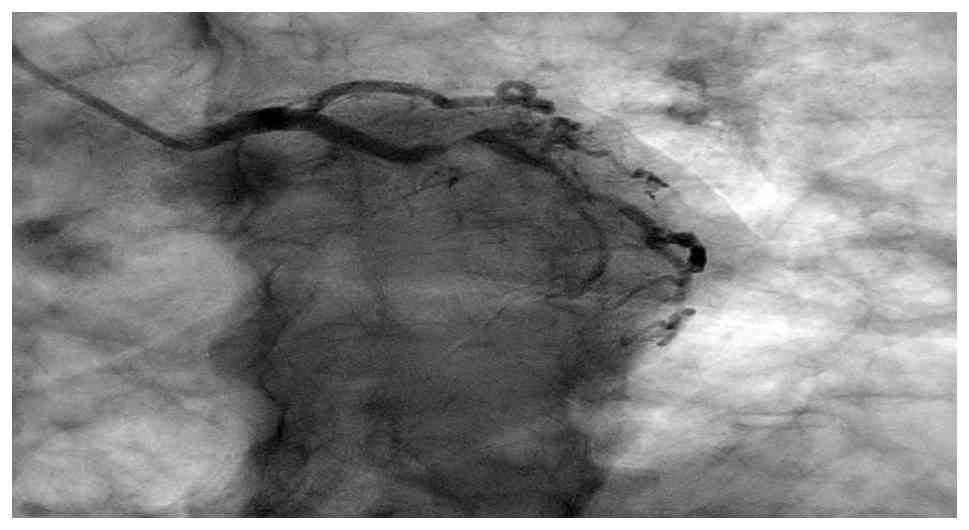
Coronary angiography confirmed severe multivessel
coronary artery disease, including the chronic total occlusion of
the left anterior descending artery with collateral flow from the
right coronary artery, severe mid-circumflex stenosis (80-90%) and
proximal right coronary artery stenosis (60-70%) with distal
posterolateral branch stenosis (90%) (Fig. 4, Fig.
5 and Fig. 6). Left ventricular
end-diastolic pressure measured at 12 mm Hg, and anterior wall
hypokinesis was noted. She was managed with guideline-directed
medical therapy, including aspirin, 81 mg; clopidogrel, 75 mg;
metoprolol succinate, 100 mg; atorvastatin, 80 mg; lisinopril, 40
mg; sublingual nitroglycerin, 0.4 mg; and a heparin drip for 24 h
and referred for cardiology evaluation and potential
revascularization. She underwent evaluation for coronary artery
bypass grafting and subsequently underwent coronary artery bypass
graft surgery. She was discharged on post-operative day 5. Her
pre-operative left ventricular ejection fraction improved from ~30%
to 41-45% post-operatively. At the 4-week follow-up, she was
clinically stable and cleared to begin cardiac rehabilitation and
return to work as tolerated.
Discussion
Women and patients with diabetes frequently exhibit
atypical symptoms during ACS, including nausea, vomiting, abdominal
discomfort, or generalized weakness, rather than the classic
substernal chest pain. Diabetic autonomic neuropathy may blunt the
perception of visceral pain, altering sympathetic and sensory
responses and contributing to atypical presentations (1-4).
These clinical variations often lead to delayed or missed
diagnoses, resulting in worse outcomes and higher mortality among
women compared with men (2,4).
In the case presented herein, the initial
presentation of the patient with gastrointestinal symptoms led to a
diagnostic focus on abdominal pathology, despite elevated troponins
and cardiovascular risk factors. The absence of chest pain, coupled
with apparent improvement following supportive therapy, created a
false sense of reassurance that contributed to her premature
discharge. This emphasizes a critical clinical lesson: In high-risk
individuals, particularly in diabetic women, a single ECG or
biomarker assessment is insufficient to exclude ACS. Instead,
serial ECGs and troponin trending are indispensable, even when
initial findings are non-diagnostic or symptoms transiently
improve, in alignment with consensus recommendations for non-ST
elevation ACS evaluation (5,6).
A critical turning point occurred during the return
visit of the patient, when a repeat ECG revealed diffuse ST-segment
depressions and T wave inversions, with upright T waves in aVR and
V1 (Fig. 3), a pattern strongly
associated with severe multivessel or left main equivalent ischemia
(7). Such global subendocardial
changes often indicate widespread coronary insufficiency and should
prompt urgent cardiologic evaluation. Notably, her troponin level
was declining at this point, underscoring that reliance solely on
biomarker trends may overlook evolving ischemia;
electrocardiographic monitoring, rather than biochemical data
alone, proved decisive in establishing the true severity of her
condition (5).
An additional consideration in the case described
herein involves the chronic use of pregabalin by the patient.
Diabetic autonomic neuropathy is a well-established and likely
primary mechanism underlying painless or atypical myocardial
infarction in patients with diabetes, due to blunted visceral pain
perception and altered autonomic signaling (1-4).
Gabapentinoids, such as pregabalin and gabapentin, are widely
prescribed for diabetic neuropathy and chronic pain, and have been
increasingly linked to adverse cardiovascular events, including
myocardial infarction and heart failure (8-10).
Proposed mechanisms include fluid retention, autonomic modulation
and effects on vascular tone, which may further elevate the
threshold for ischemic symptom perception. In this context,
pregabalin may have functioned as a contributory or exacerbating
factor, amplifying the blunting of symptoms already present due to
diabetic neuropathy, rather than serving as the sole cause of the
masked ischemic presentation. Clinicians should therefore remain
vigilant when evaluating atypical symptoms in high-risk patients
receiving these agents (8-10).
In conclusion, the present case report reinforces
several key diagnostic principles. First, the atypical
presentations of ACS, particularly in women with diabetes, should
not diminish clinical suspicion (1-4).
Second, symptomatic improvement should never preclude serial
cardiac evaluation when risk factors are present. Finally, repeat
ECGs, rather than a single initial tracing, may reveal dynamic,
high-risk patterns indicative of multivessel coronary disease. In
the patient in the present study, the diagnostic turning point was
not imaging or laboratory normalization, but rather the recognition
of evolving ischemic changes on serial ECG evaluation (5-7).
Maintaining a low threshold for ECG repetition and troponin
trending in high-risk populations, even in the absence of chest
pain, is therefore essential to avoid premature diagnostic closure
and prevent missed or delayed identification of life-threatening
coronary disease (5,6).
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated and/or analyzed during the
present study are available from the corresponding author on
request.
Authors' contributions
All authors (DD, TR, RA, PA and LB) contributed to
the conception of the study, the acquisition and interpretation of
the clinical data of the patient, and the drafting and critical
revision of the manuscript. All authors have read and approved the
final version of the manuscript and agree to be accountable for all
aspects of the work. DD and TR confirm the authenticity of all the
raw data.
Ethics approval and consent to
participate
The present study was conducted in accordance with
the ethical principles of the Declaration of Helsinki (1964) and
its subsequent amendments. Written informed consent was obtained
from the patient for her participation in the present case
report.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of the case information and any
accompanying images in the present case report. All personal
identifiers were removed to ensure confidentiality.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Canto JG, Shlipak MG, Rogers WJ, Malmgren
JA, Frederick PD, Lambrew CT, Ornato JP, Barron HV and Kiefe CI:
Prevalence, clinical characteristics, and mortality among patients
with myocardial infarction presenting without chest pain. JAMA.
283:3223–3229. 2000.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Mehta LS, Beckie TM, DeVon HA, Grines CL,
Krumholz HM, Johnson MN, Lindley KJ, Vaccarino V, Wang TY, Watson
KE, et al: Acute myocardial infarction in women: A scientific
statement from the American heart association. Circulation.
133:916–947. 2016.PubMed/NCBI View Article : Google Scholar
|
|
3
|
DeVon HA, Ryan CJ, Ochs AL and Shapiro M:
Symptoms across the continuum of acute coronary syndromes:
Differences between women and men. Am J Crit Care. 17:14–24.
2008.PubMed/NCBI
|
|
4
|
Haider A, Bengs S, Luu J, Osto E,
Siller-Matula JM, Muka T and Gebhard C: Sex and gender in
cardiovascular medicine: Presentation and outcomes of acute
coronary syndrome. Eur Heart J. 41:1328–1336. 2020.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Thygesen K, Alpert JS, Jaffe AS, Chaitman
BR, Bax JJ, Morrow DA and White HD: Executive Group on behalf of
the Joint European Society of Cardiology (ESC)/American College of
Cardiology (ACC)/American Heart Association (AHA)/World Heart
Federation (WHF) Task Force for the Universal Definition of
Myocardial Infarction. Fourth Universal definition of myocardial
infarction (2018). J Am Coll Cardiol. 72:2231–2264. 2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Amsterdam EA, Wenger NK, Brindis RG, Casey
DE Jr, Ganiats TG, Holmes DR Jr, Jaffe AS, Jneid H, Kelly RF,
Kontos MC, et al: 2014 AHA/ACC guideline for the management of
patients with non-ST-elevation acute coronary syndromes: A report
of the American College of Cardiology/american heart association
task force on practice guidelines. J Am Coll Cardiol. 64:e139–e228.
2014.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Wong CK, Gao W, Stewart RA, French JK,
Aylward PE and White HD: HERO-2 Investigators. The prognostic
meaning of the full spectrum of aVR ST-segment changes in acute
myocardial infarction. Eur Heart J. 33:384–392. 2012.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Pan Y, Davis PB, Kaebler DC, Blankfield RP
and Xu R: Cardiovascular risk of gabapentin and pregabalin in
patients with diabetic neuropathy. Cardiovasc Diabetol.
21(170)2022.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Corriere MA, Dickson AL, Daniel LL, Nepal
P, Hall K, Plummer WD, Dupont WD, Murray KT, Stein CM, Ray WA and
Chung CP: Duloxetine, gabapentin, and the risk for acute myocardial
infarction, stroke, and out-of-hospital death in medicare
beneficiaries with non-cancer pain. Clin J Pain. 39:203–208.
2023.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Dutta D, Mohindra R, Kumar M, Banerjee M,
Sharma M and Mukhopadhyay S: Cardiovascular safety of
gabapentinoids gabapentin & pregabalin: A systematic review.
Indian J Med Res. 161:363–374. 2025.PubMed/NCBI View Article : Google Scholar
|