Introduction
Supraventricular tachycardia (SVT) refers to a
diverse group of cardiac arrhythmias, characterized by abnormally
rapid supraventricular rhythms originating at or above the level of
the bundle of His (1). These rhythms
are defined by heart rates >100 bpm and involve mechanisms
arising from atrial tissue and the atrioventricular junction. This
group encompasses atrioventricular nodal reentrant tachycardia
(AVNRT), atrial tachycardia (AT) (both focal and multifocal forms),
several types of accessory pathway-related atrioventricular
reentrant tachycardias (AVRT), atrial flutter, atrial fibrillation
and sinus tachycardia (2). The
incidence of SVT is ~0.225 per 100 individuals, with a female
predominance, occurring almost twice as often in women across all
age groups (1). Thyroidal hormones
are essential for maintaining normal cardiac and vascular function
(3). Thyroid irregularities affect
~10 to 15% of adult women and a smaller proportion of adult men
(4). Thyroid disorders, including
both hypothyroidism and hyperthyroidism, are linked to a higher
risk of developing cardiovascular conditions.
Hyperthyroidism can cause both cardiac and
hemodynamic symptoms, including rapid heartbeat, palpitations,
atrial fibrillation, shortness of breath during physical activity,
and reduced exercise capacity. The symptoms of hypothyroidism on
the cardiovascular system are often more subtle and may include
bradycardia, reduced pulse pressure and diastolic hypertension
(5). SVT is commonly linked to
hyperthyroidism, while its occurrence due to hypothyroidism is
unusual (6). The present case report
presents a rare case of SVT following thyroidectomy in the setting
of biochemical hypothyroidism, as well as a brief literature
review.
Case report
Patient information
On July 1, 2025, a 50-year-old female patient
presented to Smart Health Tower (Sulaymaniyah, Iraq) with
palpitations and a sensation of chest tightness that began ~1 h
prior to presentation. She denied having chest pain, shortness of
breath, orthopnea or other associated symptoms. Her medical history
included a total thyroidectomy performed 3 years prior, and was
receiving levothyroxine 100 mcg daily. She had also undergone
axillary lymph node dissection and chemotherapy 12 years earlier;
however, the specific treatment details were unavailable. She had
previously been prescribed metoprolol at 50 mg empirically for
intermittent palpitations, without a prior confirmed diagnosis of
arrhythmia or structural heart disease. She had no history of
hypertension, diabetes mellitus, asthma, or known cardiac disease.
No known drug allergies were reported.
Clinical findings
The patient appeared anxious but alert, with no
signs of respiratory distress. Vital signs revealed a rapid,
regular heart rate of ~200 bpm. Cardiac auscultation demonstrated
normal first and second heart sounds (S1 and S2), with no murmurs,
gallops, or additional heart sounds. Peripheral pulses were weak in
volume.
The assessment for heart failure revealed mildly
elevated jugular venous pressure, clear lung fields bilaterally on
auscultation and no hepatomegaly. A lower extremity examination
revealed mild peripheral edema that was subtle and not prominent,
with no signs of significant fluid overload.
As regards hypothyroid-related features, the patient
reported mild weight gain and cold intolerance. A physical
examination revealed dry skin, with no facial puffiness. Deep
tendon reflexes were normal, without delayed relaxation.
Overall, the findings of the physical examination
were consistent with SVT in the absence of overt heart failure,
accompanied by mild clinical features suggestive of
hypothyroidism.
Diagnostic approach
A 12-lead electrocardiogram (ECG) demonstrated a
regular, narrow QRS complex tachycardia at approximately 200 bpm,
with absent visible P-waves and a short RP interval, findings
consistent with typical AVNRT (Fig.
1). Laboratory investigations revealed a complete blood count
within normal limits, with a white blood cell count of
9.6x109/l, hemoglobin level of 14.9 g/dl, hematocrit of
44.0%, red blood cell count of 5.04x1012/l, a mean
corpuscular volume of 87.3 fl, mean corpuscular hemoglobin of 29.7
pg, mean corpuscular hemoglobin concentration of 34.0 g/dl, and a
platelet count of 230x109/l. The differential count
revealed lymphocytes at 37.1%, granulocytes at 58.0%, and mid-sized
cells at 4.9%, all within normal reference ranges. There were no
notable findings in the levels of inflammatory markers, with a
C-reactive protein level of 2.66 mg/l (reference range, <5.0
mg/l). Serum electrolytes were within normal limits, including
sodium 143.1 mmol/l (reference range, 135-145 mmol/l), potassium
3.87 mmol/l (reference range, 3.5-5.1 mmol/l) and chloride 103.4
mmol/l (96-106 mmol/l). Thyroid function testing revealed an
elevated thyroid-stimulating hormone (TSH) level of 17.7 µIU/ml,
while free thyroxine (T4) remained within the normal range at 14.5
pmol/l. Transthoracic echocardiography demonstrated (images are not
available; the institutional system is not directly integrated with
the Picture Archiving and Communication System; therefore, the
echocardiography images for this patient were not archived and
could not be retrieved) normal cardiac chamber dimensions,
preserved left ventricular systolic function and no structural or
valvular abnormalities.
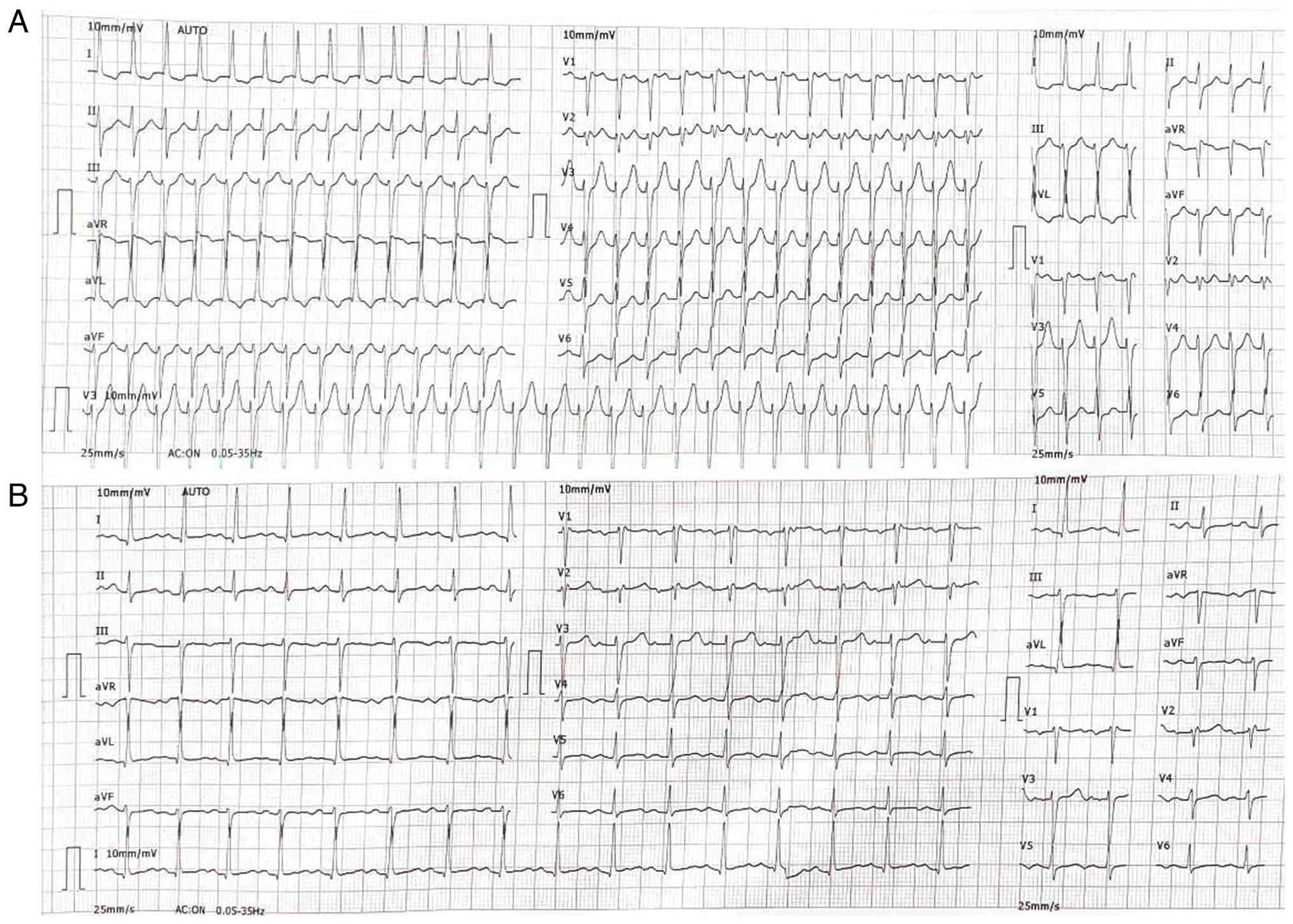 | Figure 1ECG results. (A) Upon administration,
the ECG revealed a regular, narrow-complex tachycardia with a heart
rate of ~160-180 bpm. P-waves are not clearly visible, likely
hidden within or just after the QRS complexes. The QRS duration is
narrow (<120 msec). These findings are consistent with
paroxysmal supraventricular tachycardia, most likely
atrioventricular nodal reentrant tachycardia, given the regular
rhythm, narrow QRS complexes, and absent or retrograde P-waves. (B)
Following the administration of 6 mg adenosine, the ECG revealed a
normal sinus rhythm with a heart rate of ~75-85 bpm. P-waves are
clearly visible and upright in lead II, consistent with sinus
rhythm, and the QRS duration remains normal. ECG,
electrocardiogram. |
Therapeutic intervention
Given her history of neck surgery and concerns about
the effectiveness of vagal maneuvers, 6 mg of adenosine was
administered as a rapid intravenous bolus. Successful rhythm
conversion was achieved, with the prompt resolution of symptoms.
The patient was discharged with an adjusted levothyroxine regimen
based on the elevated TSH level, aimed at achieving biochemical
euthyroidism, consisting of 100 mcg daily with an additional 50 mcg
twice weekly.
Follow-up and outcome
At the 2-month follow-up, the patient remained
asymptomatic with no recurrence of symptoms. She was
hemodynamically stable throughout follow-up period, and no episodes
of arrhythmia were reported.
Discussion
Ventricular and supraventricular arrhythmias are
rarely associated with hypothyroidism, such as SVT and Torsades de
Pointes. Hypothyroidism presents with a range of cardiovascular
effects, which vary according to the severity and duration of the
condition. These effects can range from mild changes to clearly
noticeable symptoms. Common symptoms of SVT include palpitations,
dizziness, chest discomfort, a pounding sensation in the neck or
chest, and dyspnea. The primary electrophysiological mechanism
underlying SVT is re-entry, whereas less frequent mechanisms
include abnormal automaticity and triggered activity (4). Paroxysmal SVT, which encompasses
arrhythmias such as AVRT, AVNRT and AT refers to a specific group
of SVTs characterized by sudden initiation and termination
(2). SVT may contribute to increased
morbidity, particularly with persistent or frequent symptoms. In
rare cases involving concomitant atrial fibrillation and
ventricular pre-excitation, the condition may be potentially
life-threatening (1).
Several similar cases of SVT occurring in the
setting of hypothyroidism were reviewed (Table I) (4,6-8).
The review included 4 cases, all of whom were female, with only 1
patient being >40 years of age. Palpitations were reported in
all cases, while dyspnea was observed in 3 cases. An ECG was used
in all cases to establish the diagnosis. Of note, 2 patients were
receiving treatment for hypothyroidism at the time of SVT
diagnosis, and 2 patients were treated with intravenous adenosine,
similar to the present case. Notably, predisposing cardiac history
was not consistently reported in the reviewed cases, which limiting
the assessment of underlying cardiac susceptibility to SVT. The
occurrence of tachyarrhythmias in hypothyroid states has been
attributed to several proposed mechanisms, such as changes in genes
specific to cardiac muscle cells, interstitial fluid accumulation,
swelling of myofibrils with loss of normal striations, increased
arterial rigidity, dysfunction of the endothelium, early onset of
atherosclerosis, imbalances in autonomic regulation, with a shift
toward heightened sympathetic activity, and autoimmunity. In
general, hypothyroidism is deemed to cause an imbalance in
autonomic nervous system control, marked by reduced modulation from
both sympathetic and parasympathetic pathways, with a relative
predominance of sympathetic activity (4).
 | Table IReview of some cases of
supraventricular tachycardia with hypothyroidism identified in the
literature. |
Table I
Review of some cases of
supraventricular tachycardia with hypothyroidism identified in the
literature.
| Authors, year of
publication | Age | Sex | Clinical
findings | On medication | Thyroid function
test | Electrocardiogram
findings | Treatment | Outcome | (Refs.) |
|---|
| Maznun et al,
2024 | 28 | F | Palpitations, dyspnea
and underlying hypothyroidism. | Levothyroxine. | Revealed
hypothyroidism. | Revealed SVT. | Carotid massage and
levothyroxine. | In a stable
condition. | (6) |
| Mak et al,
2018 | 26 | F | Palpitations, profuse
sweating and presyncopal attack. | None. | Severe
hypothyroidism, free T4: 0.3 pmol/l, TSH: 100 mIU/ml TPO IgG: 101
IU/ml. | Revealed SVT. | IV adenosine and
thyroxine replacement therapy. | In a stable
condition. | (4) |
| Tomar et al,
2015 | 32 | F | Palpitations and
dyspnea associated with diaphoresis. | Oral
levothyroxine. | TSH: 44.3 µU/ml, free
T3: 2.3 pg/ml, free T4: 0.3 ng/ml, TPO IgG: +ve. | Revealed paroxysmal
SVT. | Carotid massage
initially, IV adenosine 12 mg due to persistent tachyarrhythmia,
thyroxine and diltiazem. | In a stable
condition. | (7) |
| Olarescu et
al, 2009 | 47 | F | Palpitation, dyspnea,
dizziness and anxiety. | Not mentioned. | Free T4: 11.25
pmol/l, TSH=26.37 µUI/ml, TPO IgG: 1/640. | Revealed paroxysmal
SVT. | Thyroxin replacement
therapy. | In a stable
condition. | (8) |
Electrocardiographic abnormalities associated with
hypothyroidism commonly include sinus bradycardia, low voltage QRS
complexes, delayed electrical conduction, atrioventricular or
bundle branch blocks, and, less commonly, a prolonged QT interval
and Torsades de Pointes (7,9). The mechanisms underlying QT
prolongation and Torsades de Pointes in hypothyroid patients may
also provide insight into the development of paroxysmal SVT in this
condition. During phase one of the cardiac action potential,
depolarization occurs as a result of rapid sodium and calcium
influx. In hypothyroidism, the slow inward current is reduced,
particularly during phases two and three, predisposing to single or
repetitive depolarizations known as early afterdepolarizations
(10). These may manifest as
abnormal U-waves on the ECG, and if they reach a certain threshold,
they can trigger various forms of tachyarrhythmia. Such phenomena
are more prevalent in the deep endocardium and mid-myocardial
M-cell layers due to reduced delayed rectifier potassium currents
(9). A previous study evaluating the
effect of thyroid hormone replacement on benign atrial and
ventricular arrhythmias found that thyroxine therapy was associated
with a higher occurrence of atrial premature complexes in patients
who already had existing arrhythmia. However, it did not lead to
the development of new supraventricular or ventricular
tachyarrhythmias. Nevertheless, the potential contribution of
thyroxine therapy to tachyarrhythmogenesis cannot be entirely
excluded (11).
Palpitations are commonly experienced by individuals
at some point; however, not all palpitations are caused by
arrhythmias, and not all arrhythmias result in palpitations. In
some cases, arrhythmias can be diagnosed using ECG, whereas in
others, diagnosis is based primarily on reported symptoms. In such
situations, electrophysiological studies may help confirm the
presence and elucidate the underlying mechanism of the abnormal
cardiac rhythm (12). Thyroid
dysfunction, particularly hyperthyroidism, is a recognized cause of
palpitations. The association between atrial fibrillation and
thyroid abnormalities is well established. By contrast, the
association between thyroid dysfunction and other supraventricular
tachyarrhythmias (excluding atrial fibrillation) is less clearly
defined. Current guidelines recommend evaluation for
hyperthyroidism in cases of inappropriate sinus tachycardia or
frequent premature beats (13).
The clinical significance of SVT is not limited to
adults, as it can also occur in the fetal and pediatric
populations, where it may lead to serious complications such as
fetal heart failure and hydrops fetalis, a potentially
life-threatening condition. In children, SVT is primarily caused by
three electrophysiological mechanisms, with re-entry circuits being
the most common, followed by triggered activity and abnormal
automaticity, all of these mechanisms may produce similar ECG
patterns. In addition, SVT may be associated with structural heart
defects, electrolyte disturbances and genetic factors (14).
Careful analysis of the surface ECG can identify
features suggestive of the underlying mechanism in ~80% of cases of
AVRT and AVNRT, although comparison with a sinus rhythm ECG is
often helpful. AVNRT is the most common form of SVT in the general
population, representing >60% of cases evaluated by invasive
cardiac electrophysiological studies. This arrhythmia is caused by
the presence of two functionally distinct conduction pathways
within the atrioventricular node, one fast and one slow, that
differ in conduction velocity and refractory period. AVNRT is
typically initiated by an atrial premature beat, and less commonly
by a ventricular premature beat, which establishes a sustained
re-entrant circuit between these pathways. On a surface ECG, this
manifests as a narrow complex tachycardia without signs of bundle
branch block (1).
When the initiating premature impulse conducts
antegradely through the slow pathway, a prolonged PR interval is
observed the first beat of the tachycardia. During the re-entrant
circuit, simultaneous activation of the atria and ventricles
occurs, causing the P-wave and QRS complex to appear almost
simultaneously. This leads to the absence of a visible RP interval
or the presence of a very short RP interval, characteristic of
typical AVNRT. The P-wave typically appears inverted (negative) in
leads II, III, and augmented vector foot (aVF) due to retrograde
atrial activation from the lower to the upper atrium. In addition,
the P-waves are narrow, reflecting septal atrial activation
(2).
The acute management of regular narrow complex
tachycardia focuses on terminating the arrhythmia and identifying
the underlying mechanism. A 12-lead ECG is essential for diagnosis
and for guiding treatment decisions. In hemodynamically stable
patients, vagal maneuvers may be attempted as an initial management
strategy, with reported success rates of 19-54% when performed
using a modified Valsalva technique (1,15), with
improved results in a semi-recumbent position as per the REVERT
trial (15). In the event that vagal
maneuvers are unsuccessful or cannot be performed, adenosine may be
administered as a rapid intravenous bolus through a large vein,
followed immediately by a 10-ml saline flush. Due to its short
half-life (<10 sec), rapid delivery is crucial. Adenosine
functions by transiently slowing or blocking AV nodal conduction
through activation of A1 receptors. Continuous ECG monitoring is
essential during administration. If there is no response, the
adenosine dose may be insufficient, or the rhythm may be
ventricular tachycardia, which doesn't involve the AV node. The
abrupt termination of the tachycardia following adenosine
administration suggests AVNRT or AVRT, typically requiring ~6 mg.
The presence of visible P-waves with AV dissociation is more
consistent with AT. Adenosine rarely terminates AT; however, if it
does, a focal origin is more likely than a re-entrant one. In
patients who are hemodynamically unstable, immediate direct-current
cardioversion is indicated, immediate direct current cardioversion
is indicated, though adenosine may be attempted during preparation
(1).
The present case report has several key
considerations. First, collecting data from multiple patients with
post-thyroidectomy biochemical hypothyroidism and AVNRT is
challenging, which limits the feasibility of larger studies.
Second, although the patient had been receiving metoprolol for
several years, her arrhythmic signs and symptoms developed only
recently, suggesting the presence of additional contributing
factors, such as hormonal fluctuations. Third, the prior years of
hypothyroidism treatment of the patient were reviewed as part of
the data collection in order to better understand long-term thyroid
management. Finally, the primary focus of the present report was
the association between levothyroxine dose adjustment and
arrhythmia, as the condition of the patient improved the 6 six
months following the modification of thyroid hormone therapy,
highlighting the potential impact of optimized dosing on arrhythmia
control.
In conclusion, the occurrence of SVT in patients
with hypothyroidism is rare, but should still be considered by
clinicians. ECG plays a crucial role in both the diagnosis and
management of this condition.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
FHK and BJR were major contributors to the
conception of the study, as well as to the literature search for
related studies. ANQ, TOS, AOH and ZHA contributed to the clinical
management of the patient, assisted with data acquisition and
interpretation, and participated in the literature review and
manuscript preparation. DTQ, BAA, SFA and FJA contributed to the
conception and design of the study, the literature review, the
critical revision of the manuscript, and the processing of the
table. FHK and BJR confirm the authenticity of all the raw data.
All authors have read and approved the final manuscript.
Ethics approval and consent to
participate
Written informed consent was obtained from the
patient for their participation in the present case report.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of the present case report and any
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kotadia ID, Williams SE and O'Neill M:
Supraventricular tachycardia: An overview of diagnosis and
management. Clin Med. 20:43–47. 2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Mahtani AU and Nair DG: Supraventricular
tachycardia. Med Clin. 103:863–879. 2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Udovcic M, Pena RH, Patham B, Tabatabai L
and Kansara A: Hypothyroidism and the heart. Methodist Debakey
Cardiovasc J. 13:55–59. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Mak WW, Nurazni RR and Badrulnizam LM:
Severe hypothyroidism presenting with supraventricular tachycardia.
Med J Malaysia. 73:349–350. 2018.PubMed/NCBI
|
|
5
|
Yamakawa H, Kato TS, Noh JY, Yuasa S,
Kawamura A, Fukuda K and Aizawa Y: Thyroid hormone plays an
important role in cardiac function: From bench to bedside. Front
Physiol. 12(606931)2021.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Maznun MJ, Fatin NM, Sakinah MR and Najmi
NM: Case report: A rare case of supraventricular tachycardia in
pregnancy with hypothyroidism. Malaysian Family Physician.
19(36)2024.
|
|
7
|
Tomar LR, Gopalakrishnan ST and Aggarwal
A: Paroxysmal supraventricular tachycardia in Hypothyroidism: A
case report. J Cardiovascular Dis Res. 6:156–158. 2015.
|
|
8
|
Olarescu C, Ghervan C, Hazi G and Duncea
I: New clinical feature in hypothyroidism: Paroxysmal
supraventricular tachycardia: Case report. In Endocrine Abstracts.
Vol 20. Bioscientifica, 2009.
|
|
9
|
Klein I and Ojamaa K: Thyroid hormone and
the cardiovascular system. N Engl J Med. 344:501–509.
2001.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Kahaly GJ and Dillmann WH: Thyroid hormone
action in the heart. Endocr Rev. 26:704–728. 2005.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Polikar R, Feld GK, Dittrich HC, Smith J
and Nicod P: Effect of thyroid replacement therapy on the frequency
of benign atrial and ventricular arrhythmias. J Am Coll Cardiol.
14:999–1002. 1989.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Zimetbaum P and Josephson ME: Evaluation
of patients with palpitations. N Engl J Med. 338:1369–1373.
1998.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Gwag HB, Jun JE, Park Y, Lee SS, Park SJ,
Kim JS, Park KM and On YK: Thyroid dysfunction in patients with
suspected or documented supraventricular tachyarrhythmia. Int J
Arrhythmia. 20:1–7. 2019.
|
|
14
|
Nizami Z, Garcia P, Ahuja P, Nipper AJ,
Patel S, Sheth H, Gajendran N and Dhillon R: Supraventricular
tachycardia in children. Progr Pediatr Cardiol. 76(101771)2024.
|
|
15
|
Appelboam A, Reuben A, Mann C, Gagg J,
Ewings P, Barton A, Lobban T, Dayer M, Vickery J, Benger J, et al:
Postural modification to the standard Valsalva manoeuvre for
emergency treatment of supraventricular tachycardias (REVERT): A
randomised controlled trial. Lancet. 386:1747–1753. 2015.PubMed/NCBI View Article : Google Scholar
|














