1. Introduction
The field of oncology is currently experiencing an
unprecedented expansion in the development and clinical adoption of
antibody-drug conjugates (ADCs). Following the foundational success
of ado-trastuzumab emtansine (T-DM1), multiple next-generation ADCs
targeting human epidermal growth factor receptor 2 (HER2),
trophoblast cell-surface antigen 2 (TROP2), Nectin-4 and MET have
received regulatory approval in recent years (1). These agents have rapidly become
integral components of standard-of-care treatment algorithms for
metastatic breast cancer, urothelial carcinoma and non-small cell
lung cancer (NSCLC).
This rapid expansion has introduced a novel and
clinically relevant dilemma. Historically, disease progression in
the metastatic setting prompted a switch between chemotherapy
classes (e.g., taxane to platinum). By contrast, contemporary
practice increasingly involves transitioning from one ADC to
another. This paradigm shift raises a fundamental question: Whether
the ‘Trojan Horse’ delivery strategy remains effective following
prior ADC exposure, or whether shared resistance mechanisms render
subsequent agents ineffective (2).
The clinical implications of this uncertainty are
substantial. Inappropriate sequencing may expose patients to costly
and potentially toxic therapies with limited likelihood of benefit.
For example, in the event that resistance develops primarily
against the cytotoxic payload of an initial ADC, a subsequent agent
carrying a similar warhead may exhibit immediate cross-resistance,
regardless of its antigenic target (3). Accordingly, a more in-depth
understanding of resistance mechanisms is essential to guide
rational sequencing decisions.
In addition to breast and urothelial malignancies,
the present review also considers emerging sequencing challenges in
NSCLC and gastric cancer, where multiple ADCs are entering clinical
practice. As novel agents, such as trastuzumab deruxtecan,
telisotuzumab vedotin and datopotamab deruxtecan become integrated
into treatment algorithms, understanding payload-driven resistance
and rational ADC transition strategies across tumor types has
become increasingly important. Accordingly, the present review
adopts a tumor-agnostic framework focused on shared biological
mechanisms of resistance while incorporating disease-specific
clinical evidence where available (4,5).
The present narrative review discusses the
biological drivers of resistance to sequential ADC therapy, with a
focus on distinguishing target-mediated resistance (failure of
antigen recognition and internalization) from payload-mediated
resistance (failure of intracellular cytotoxic activity). This
framework is intended to provide clinicians with a practical
approach to navigating an increasingly complex therapeutic
landscape.
2. Mechanisms of resistance
Antigen downregulation
The efficacy of any ADC is contingent upon the
sufficient expression of its target antigen on the tumor cell
surface. A well-recognized mechanism of resistance is antigen
downregulation or loss, effectively preventing ADC binding and
internalization. In HER2-positive breast cancer, treatment with
trastuzumab deruxtecan (T-DXd) has been shown to select for
HER2-low or HER2-null tumor clones (6). When antigen expression falls below a
critical threshold, subsequent ADCs targeting the same antigen,
such as switching from T-DXd to trastuzumab emtansine (T-DM1) are
unlikely to be effective because the delivery vehicle can no longer
reliably engage the tumor cell (6).
Bystander effect and primary vs.
acquired resistance in ADC sequencing
An additional consideration in ADC sequencing is the
role of the bystander effect, particularly for ADCs carrying
membrane-permeable, high-potency payloads such as T-DXd. The
bystander effect may partially mitigate heterogeneous or reduced
antigen expression by allowing payload diffusion into adjacent
antigen-low or antigen-negative tumor cells. This property likely
contributes to the clinical activity of T-DXd in HER2-low tumors.
However, available data suggest that the bystander effect does not
fully overcome resistance once antigen expression falls below a
critical threshold or when resistance is driven predominantly by
payload-specific mechanisms such as drug efflux, altered
intracellular trafficking, or DNA (deoxyribonucleic acid) damage
response adaptation. In these contexts, the sequential use of ADCs
sharing the same payload class may still result in diminished
efficacy despite preserved bystander activity (7,8).
Notably, resistance to ADCs can be broadly
categorized as primary (intrinsic) or acquired. Primary resistance
reflects pre-existing tumor features, including absent or
heterogeneous antigen expression, intrinsic insensitivity to the
payload, or baseline efflux activity, and may limit the
effectiveness of any ADC targeting the same pathway. By contrast,
acquired resistance arises following ADC exposure and is frequently
driven by adaptive changes such as antigen downregulation,
payload-specific resistance mechanisms, or alterations in
intracellular processing. This distinction has practical
implications for sequencing: patients with acquired,
antigen-specific resistance may remain candidates for a rational
‘target swap’ or ‘payload swap’, whereas those with primary
payload-class resistance are less likely to benefit from sequential
ADCs carrying similar cytotoxic warheads (8). While the loss of HER2 represents the
most well-characterized example of target-mediated resistance,
antigen downregulation in non-HER2 targets, such as TROP2 and
Nectin-4 remains less clearly defined, and ongoing translational
and clinical studies are expected to further clarify its role in
ADC resistance and sequencing decisions.
Payload cross-resistance
Even when antigen binding and internalization remain
intact, resistance to the cytotoxic payload can lead to therapeutic
failure. A major concern in contemporary practice is the increasing
reliance on camptothecin-derived topoisomerase I inhibitors as ADC
payloads. Agents such as trastuzumab deruxtecan, sacituzumab
govitecan and datopotamab deruxtecan all share this mechanism of
action (9).
In the event that a tumor acquires resistance to one
topoisomerase I inhibitor through target enzyme mutations,
alterations in DNA damage response pathways, or enhanced drug
efflux it is biologically plausible that cross-resistance will
extend to other ADCs carrying similar payloads. In addition, cancer
cells may upregulate ATP-binding cassette transporters, including
multidrug resistance 1 (P-glycoprotein), which actively export
cytotoxic agents from the cytoplasm before they can induce lethal
DNA damage or microtubule disruption (10). Such mechanisms can confer broad
resistance across multiple ADCs, irrespective of target
antigen.
Linker and intracellular processing
defects
Resistance may also arise from the impaired
intracellular processing of the ADC. Following internalization,
linker cleavage within the lysosome is required to release the
active payload. Lysosomal dysfunction, such as increased lysosomal
pH or reduced expression of proteolytic enzymes (e.g., cathepsin B)
can prevent effective payload release (11). In this context, tumor cells
internalize the ADC, but fail to liberate the cytotoxic component,
resulting in resistance that may extend across ADCs utilizing
similar linker technologies. Although linker instability and
intracellular processing defects represent biologically plausible
mechanisms of resistance, current evidence supporting their role is
derived largely from preclinical and translational studies, and
their relative clinical impact appears less well established
compared with antigen downregulation or payload-mediated
resistance.
3. Clinical evidence
Sequencing in breast cancer
Breast cancer provides the most robust clinical data
regarding ADC sequencing and highlights the importance of payload
diversity. The sequence of T-DM1 followed by T-DXd (topoisomerase I
inhibitor payload) has demonstrated substantial clinical benefit.
The phase III DESTINY-Breast03 trial established the superiority of
T-DXd over T-DM1 in patients with previously treated HER2-positive
metastatic breast cancer, demonstrating significantly prolonged
progression-free survival and higher response rates (12). The superiority of T-DXd over T-DM1
has been demonstrated, and real-world data confirm its continued
efficacy following T-DM1 failure (8). This success is likely attributable to
both a ‘payload swap’ and the higher drug-to-antibody ratio of
T-DXd.
By contrast, sequencing T-DXd (HER2-targeted)
followed by sacituzumab govitecan (TROP2-targeted) represents a
‘target swap’ without a ‘payload swap’, as both ADCs deliver
topoisomerase I inhibitors. Emerging retrospective and real-world
cohort data, including the multi-institutional analysis by Mai
et al, suggest diminished efficacy when a topoisomerase
I-based ADC is administered after progression on a prior agent with
the same payload class (13). These
findings are hypothesis-generating and require prospective
validation. A recent multi-institutional retrospective analysis
reported shorter progression-free survival among patients receiving
a topoisomerase I-based ADC after progression on a prior agent with
the same payload class, compared with payload-naïve patients
(13). These findings strongly
support the clinical relevance of payload-mediated
cross-resistance. It is important to note that these observational
sequencing data are retrospective in nature and inherently subject
to selection bias and confounding, and therefore should be
interpreted as complementary to, rather than a replacement for,
evidence derived from prospective randomized clinical trials.
Sequencing in urothelial cancer
In metastatic urothelial carcinoma, the standard
sequencing paradigm typically involves enfortumab vedotin (EV),
which carries a monomethyl auristatin E (MMAE)
microtubule-disrupting payload, followed by sacituzumab govitecan
in subsequent lines of systemic therapy (14,15).
This sequence generally preserves clinical activity, likely as the
payloads disrupt distinct cellular processes. The relative absence
of cross-resistance in this setting further supports the hypothesis
that switching cytotoxic mechanisms rather than targets alone is
critical for maintaining efficacy in sequential ADC therapy
(14,15). However, it should be emphasized that
sequencing data in metastatic urothelial carcinoma remain evolving,
with additional ADCs and combination strategies currently under
investigation, and therefore current conclusions should be
interpreted within the context of a rapidly developing therapeutic
landscape.
Sequencing considerations in NSCLC and
gastric cancer
Emerging data from NSCLC and gastric cancer further
support the importance of payload class in determining clinical
benefit. In HER2-mutant and HER2-overexpressing NSCLC, T-DXd, a
topoisomerase I inhibitor-based ADC, has demonstrated substantial
activity and is currently an established therapeutic option.
However, as additional ADCs enter clinical practice, such as
telisotuzumab vedotin (MET-directed, MMAE payload) and datopotamab
deruxtecan (TROP2-directed, topoisomerase I payload) sequencing
considerations analogous to those observed in breast cancer are
emerging. Early-phase clinical trials and emerging clinical data in
NSCLC, including the LUMINOSITY study (telisotuzumab vedotin) and
the phase III TROPION-Lung01 trial (datopotamab deruxtecan),
suggest that preserved efficacy may be more likely when
transitioning between ADCs with distinct cytotoxic payload classes,
whereas sequential exposure to ADCs sharing topoisomerase I
inhibitor payloads may be associated with reduced benefit due to
payload-driven cross-resistance (4,16).
Similar principles may apply to gastric cancer, where trastuzumab
deruxtecan demonstrated improved overall survival and response
rates compared with chemotherapy in previously treated
HER2-positive metastatic gastric cancer in the phase II
DESTINY-Gastric01 trial, underscoring the broader relevance of
payload diversification rather than target substitution alone in
rational ADC sequencing strategies (5).
4. Strategic considerations for the
clinician
The ‘payload swap’ strategy
Emerging clinical and translational data, as
summarized in a recent review, suggest that prioritizing a change
in payload class may represent a rational sequencing approach
(6). When progression occurs on an
ADC, subsequent therapy should ideally employ a cytotoxic mechanism
distinct from the first. For example, transitioning from a
microtubule inhibitor-based ADC (e.g., T-DM1 or EV) to a
topoisomerase I inhibitor-based ADC (e.g., T-DXd or sacituzumab
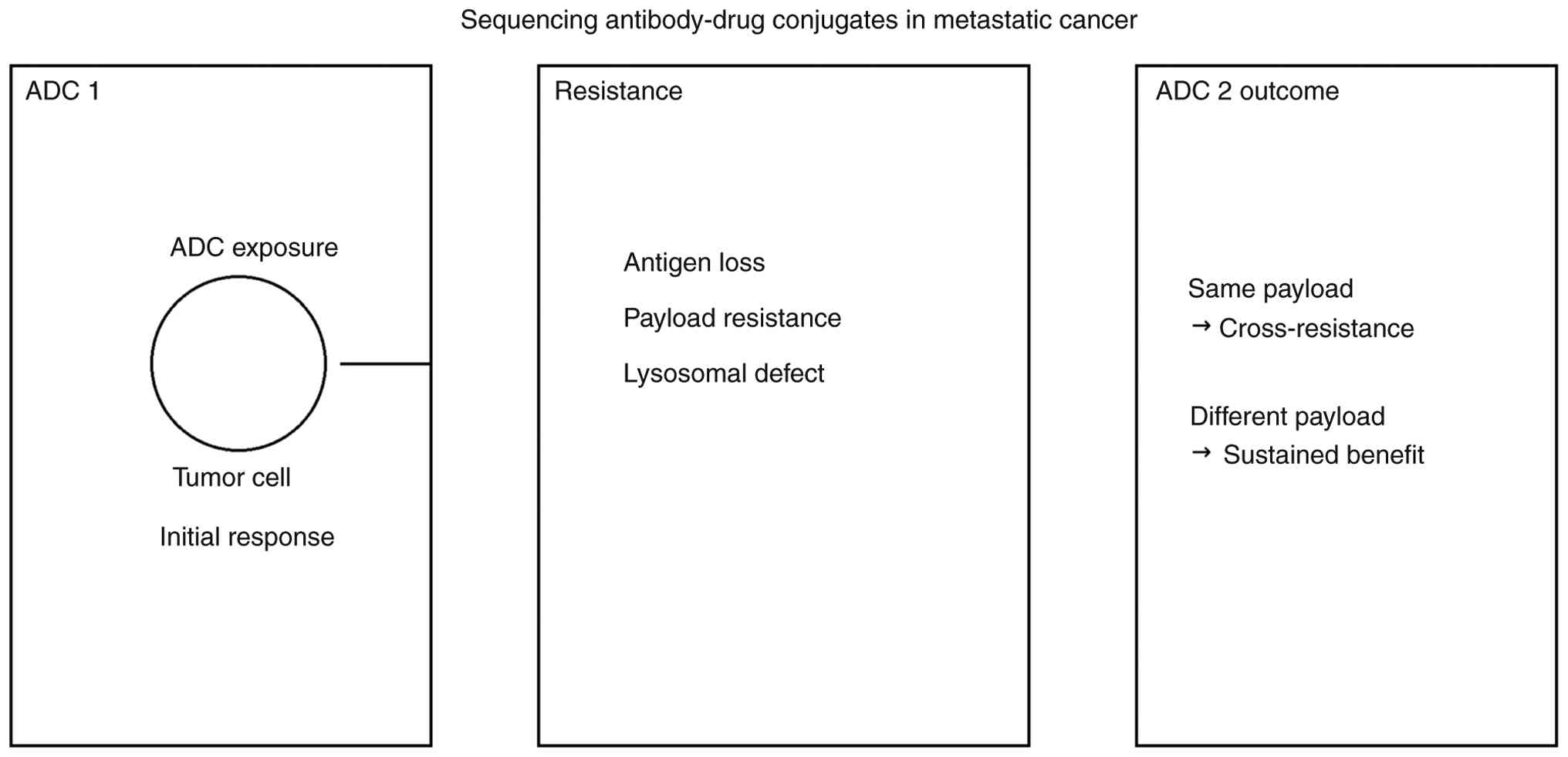
govitecan) appears to reduce the risk of cross-resistance (Table I) (13). These mechanisms collectively
illustrate how resistance acquired during initial ADC exposure can
influence the efficacy of subsequent ADCs, highlighting the
importance of payload selection in sequencing strategies (Fig. 1). It should be emphasized that this
proposed ‘payload swap’ strategy is supported primarily by indirect
and retrospective clinical evidence and is intended to guide
mechanistic clinical reasoning rather than serve as a definitive
treatment guideline, pending validation in prospective sequencing
trials.
 | Table IAntibody-drug conjugates by target and
payload class. |
Table I
Antibody-drug conjugates by target and
payload class.
| ADC | Target | Payload class | Toxicities |
|---|
| Trastuzumab emtansine
(T-DM1) | HER2 | Microtubule
inhibitor | Thrombocytopenia,
hepatotoxicity, peripheral neuropathy |
| Trastuzumab
deruxtecan | HER2 | Topoisomerase I
inhibitor | ILD/pneumonitis,
nausea |
| Sacituzumab
govitecan | TROP2 | Topoisomerase I
inhibitor | Neutropenia,
diarrhea |
| Enfortumab
vedotin | Nectin-4 | Microtubule
inhibitor | Peripheral
neuropathy, skin toxicity |
| Datopotamab
deruxtecan | TROP2 | Topoisomerase I
inhibitor | ILD/pneumonitis,
stomatitis |
Beyond efficacy considerations, overlapping
payload-associated toxicities represent an additional practical
constraint in ADC sequencing. For example, sequential use of
DXd-based ADCs (e.g., trastuzumab deruxtecan or datopotamab
deruxtecan) may increase clinical vigilance for interstitial lung
disease (ILD), whereas back-to-back exposure to MMAE-based ADCs
(e.g., trastuzumab emtansine or enfortumab vedotin) may compound
the risk of cumulative peripheral neuropathy. In this context, a
‘payload swap’ may not only mitigate biological cross-resistance
but also alter the toxicity profile, potentially improving
tolerability in selected patients. Therefore, sequencing decisions
should integrate both mechanistic resistance principles and
anticipated safety overlap (12,14,16).
The ‘target swap’ strategy
Switching antigen targets while retaining a similar
payload class (e.g., T-DXd to sacituzumab govitecan) carries a
higher risk of diminished efficacy. Although a new antigen may
permit cellular entry, intracellular resistance to the cytotoxic
warhead may limit the depth and duration of response (9). Clinicians should approach such
sequences cautiously and counsel patients regarding the potential
for reduced benefit. In general, a target swap strategy may be most
appropriate in patients with confirmed preservation of the new
target antigen on repeat biopsy, limited alternative treatment
options, adequate organ function, and no clear evidence of
payload-class resistance from prior therapy.
The role of re-biopsy
Given the prevalence of antigen downregulation,
obtaining a repeat biopsy prior to initiating a second ADC is
increasingly important. Confirming adequate expression of the
intended target antigen (e.g., HER2 or TROP2) can help avoid
target-mediated resistance and guide rational treatment selection
(6). However, re-biopsy may be
constrained by procedural risks, limited access in certain practice
settings, financial cost, and feasibility in heavily pre-treated
patients, and therefore should be pursued selectively when the
anticipated clinical benefit justifies these considerations.
5. Limitations
The present review has several critical limitations
that should be acknowledged. First, as a narrative review, the
manuscript does not follow a systematic review or meta-analytic
methodology. Consequently, the included studies were selected based
on clinical relevance and emerging impact rather than predefined
inclusion criteria, and the conclusions should be interpreted as
hypothesis-generating rather than definitive.
Second, much of the clinical evidence informing ADC
sequencing, particularly regarding payload cross-resistance, is
derived from retrospective analyses, real-world cohorts and
subgroup observations, which are inherently subject to selection
bias and confounding. While these data provide valuable insights
into real-world practice, they cannot fully substitute for
prospective, randomized sequencing trials, which remain limited or
unavailable in most tumor types.
Third, although the review emphasizes
payload-mediated resistance as a dominant driver of sequential ADC
failure, direct comparative data between different sequencing
strategies are scarce, and resistance mechanisms are often inferred
from translational or preclinical studies. The relative
contribution of antigen loss, payload resistance, linker
instability, and intracellular trafficking defects likely varies
across tumor types and individual patients, limiting the
generalizability of any single sequencing paradigm.
Finally, the rapidly evolving ADC landscape
represents an inherent limitation. New ADCs, novel payload classes,
and emerging clinical trial data (including conference abstracts)
continue to reshape sequencing considerations, and recommendations
discussed here may require refinement as prospective evidence
matures.
6. Future directions and conclusion
Next-generation ADC strategies are currently under
active investigation and aim to overcome limitations observed with
existing sequencing paradigms. Bispecific ADCs targeting two
antigens simultaneously (e.g., HER2 and EGFR) are being developed
to address tumor heterogeneity and potential antigen loss. In
addition, novel payload classes, including immunostimulatory agents
such as stimulator of interferon genes agonists, as well as
dual-payload constructs, are being explored to circumvent
established resistance pathways.
Notably, these approaches remain investigational and
are largely supported by preclinical data or early-phase clinical
studies. While conceptually promising, their safety, durability of
response, and optimal integration into existing sequencing
strategies have yet to be defined. Accordingly, the clinical
utility of these next-generation ADC platforms remains to be
established through prospective clinical trials.
In conclusion, sequential ADC therapy has become a
cornerstone of modern metastatic cancer management, but carries a
substantial risk of futility if cross-resistance is not carefully
considered. Accumulating evidence indicates that resistance is more
commonly driven by the cytotoxic payload than by the target
antigen. Consequently, successful sequencing often depends on
prioritizing a ‘payload swap’ rather than merely changing targets.
Incorporating this mechanistic approach into clinical
decision-making is essential to maximize therapeutic benefit while
minimizing unnecessary toxicity in the evolving ADC era.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
BAA conceived the study, and performed the
literature search for related studies and the critical revision of
the manuscript. BAA was also involved in the literature review, in
the design of the study and in the writing of the manuscript, as
well as in the acquisition and interpretation of data from the
literature. The author has read and approved the final manuscript.
Data authentication is not applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The author declares that he has no competing
interests.
References
|
1
|
Drago JZ, Modi S and Chandarlapaty S:
Unlocking the potential of antibody-drug conjugates for cancer
therapy. Nat Rev Clin Oncol. 18:327–344. 2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Coates JT, Sun S, Leshchiner I, Thimmiah
N, Martin EE, McLoughlin D, Danysh BP, Slowik K, Jacobs RA,
Rhrissorrakrai K, et al: Parallel genomic alterations of antigen
and payload targets mediate therapeutic failure of multiple
antibody-drug conjugates. Cancer Discov. 11:2436–2445. 2021.
|
|
3
|
Hao Y and Song Z: Mechanisms of resistance
to antibody-drug conjugates in cancer therapy: Molecular basis and
therapeutic strategies. Cancer Drug Resist. 8(59)2025.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Camidge DR, Bar J, Horinouchi H, Goldman
J, Moiseenko F, Filippova E, Cicin I, Ciuleanu T, Daaboul N, Liu C,
et al: Telisotuzumab vedotin monotherapy in patients with
previously treated c-Met protein-overexpressing advanced
nonsquamous EGFR-wildtype non-small cell lung cancer in the phase
II LUMINOSITY trial. J Clin Oncol. 42:3000–3011. 2024.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Shitara K, Bang YJ, Iwasa S, Sugimoto N,
Ryu MH, Sakai D, Chung HC, Kawakami H, Yabusaki H, Lee J, et al:
Trastuzumab deruxtecan in previously treated HER2-positive gastric
cancer. N Engl J Med. 382:2419–2430. 2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Fenton MA, Tarantino P and Graff SL:
Sequencing antibody drug conjugates in breast cancer: exploring
future roles. Curr Oncol. 30:10211–10223. 2022.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Ogitani Y, Aida T, Hagihara K, Yamaguchi
J, Ishii C, Harada N, Soma M, Okamoto H, Oitate M, Arakawa S, et
al: DS-8201a, a novel HER2-targeting ADC with a novel DNA
topoisomerase I inhibitor, demonstrates a promising antitumor
efficacy with differentiation from T-DM1. Clin Cancer Res.
22:5097–5108. 2016.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Loganzo F, Sung M and Gerber HP:
Mechanisms of resistance to antibody-drug conjugates. Mol Cancer
Ther. 15:2825–2834. 2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Bardia A, Hurvitz S, Tolaney SM, Loirat D,
Punie K, Oliveira M, Brufsky A, Sardesai SD, Kalinsky K, Zelnak AB,
et al: Sacituzumab govitecan in metastatic triple-negative breast
cancer. N Engl J Med. 384:1529–1541. 2021.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Kovtun YV, Audette CA, Mayo MF, Jones GE,
Doherty H, Maloney EK, Erickson HK, Sun X, Wilhelm S, Ab O, et al:
Antibody-drug conjugates designed to eradicate tumors with
multidrug resistance. Cancer Res. 70:2528–2537. 2010.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Hamblett KJ, Senter PD, Chace DF, Sun MM,
Lenox J, Cerveny CG, Kissler KM, Bernhardt SX, Kopcha AK, Zabinski
RF, et al: Effects of drug loading on the antitumor activity of a
monoclonal antibody drug conjugate. Clin Cancer Res. 10:7063–7070.
2004.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Cortés J, Kim SB, Chung WP, Im SA, Park
YH, Hegg R, Kim MH, Tseng LM, Petry V, Chung CF, et al: Trastuzumab
deruxtecan versus trastuzumab emtansine for breast cancer. N Engl J
Med. 386:1143–1154. 2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Mai N, Klar Lieberman MM, Ferraro E,
Bromberg M, Chen Y, Razavi P, Modi S, Chandarlapaty S, Walsh EM and
Drago JZ: Sequential antibody-drug conjugate therapy in patients
with metastatic breast cancer treated with sacituzumab govitecan
and trastuzumab deruxtecan. JCO Precis Oncol.
9(e2400898)2025.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Powles T, Rosenberg JE, Sonpavde GP,
Loriot Y, Durán I, Lee JL, Matsubara N, Vulsteke C, Castellano D,
Wu C, et al: Enfortumab vedotin in previously treated advanced
urothelial carcinoma. N Engl J Med. 384:1125–1135. 2021.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Tagawa ST, Balar AV, Petrylak DP,
Kalebasty AR, Loriot Y, Fléchon A, Jain RK, Agarwal N, Bupathi M,
Barthelemy P, et al: TROPHY-U-01: A phase II open-label study of
sacituzumab govitecan in patients with metastatic urothelial
carcinoma progressing after platinum-based chemotherapy and
checkpoint inhibitors. J Clin Oncol. 39:2474–2485. 2021.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Ahn MJ, Tanaka K, Paz-Ares L, Cornelissen
R, Girard N, Pons-Tostivint E, Vicente Baz D, Sugawara S, Cobo M,
Pérol M, et al: Datopotamab deruxtecan versus docetaxel for
previously treated advanced or metastatic non-small cell lung
cancer: The randomized, open-label phase III TROPION-Lung01 study.
J Clin Oncol. 43:260–272. 2025.PubMed/NCBI View Article : Google Scholar
|