Introduction
Brain metastasis is considered a major complication
of the later stages of cancer. This is associated with various
signs and symptoms, including headaches, seizures, weakness in the
arms or legs, loss of balance, memory loss and speech disruptions
(1). The management of these
metastatic lesions has always been a challenge. There are different
approaches employed in treating metastatic brain tumours, including
the following:
Radiation therapy uses X-rays, protons and other
high-energy electron beams to eliminate cancer cells. The two most
known techniques are stereotactic radiosurgery (SRS) and
whole-brain radiation therapy (WBRT). SRS provides precise
radiation towards the cancerous cells and is performed in a few
sessions, whereas the radiation in WBRT is applied to the whole
brain and requires 10-15 sessions (2). Traditionally, SRS was limited to
patients with up to four brain metastases. However, it is
increasingly being considered a viable treatment option for those
with more numerous metastases, with a recent study demonstrating a
promising safety and efficacy profile in patients with ≥15 brain
metastases (3).
Chemotherapy is limited as the majority of
chemotherapeutic agents cannot cross the blood-brain barrier.
However, it is still considered a viable option. Extensive research
has been performed in an aim to improve drug delivery to the brain
(2).
Targeted therapy is one of the newest methods in the
treatment of cancer. The agents used in this type of therapy can
cross the blood-brain barrier and can identify cancerous cells with
minimal harm to normal cells. It is usually co-administered with
radiation therapy or administered following surgery to eliminate
the remaining cancerous cells (1).
Recently, neuroendoscopy has gained increasing
attention in the field of neurosurgery, being used for the
treatment of a wide range of conditions including hydrocephalus,
intracranial cysts, craniosynostosis, intraventricular tumours, and
skull base tumours (4,5). Due to its minimally invasive technique,
while maintaining effectiveness and comparative safety, it has
become the preferred surgical approach for the management of many
intracranial diseases (5). A recent
single-centre retrospective study surveying 318 neuroendoscopic
procedures for intracranial pathologies reported that only 5.4% of
cases were affected by an early surgical adverse event while 3.1%
were affected by a non-surgical adverse event (5).
The present systematic review aimed to summarise the
available literature surrounding neuroendoscopic procedures in
patients diagnosed with metastatic brain tumours. In particular,
the authors were interested in summarising the available evidence
regarding the characteristics of patients selected for this
technique, technical details regarding the procedure in this
patient population, and evaluating the evidence regarding the
outcomes of these neuroendoscopic procedures.
Data and methods
The present systematic review was undertaken using
the approach outlined by the Preferred Reporting Items for
Systematic Reviews and Meta-Analyses (PRISMA) method (6). Articles assessed as part of the present
systematic review were identified from a search of the PubMed
library electronic database performed on June 1, 2022. The search
string utilised was: ‘(Endoscop*[Title/Abstract] OR
Neuroendoscop*[Title/Abstract]) AND (Metast*[Title/Abstract]) AND
(Brain[Title/Abstract])’. Asterisks (‘*’) and Boolean operators
‘AND’ and ‘OR’ are established tools used to search the PubMed
library and were used to enhance search yield.
Studies were included or excluded from analysis in
the present systematic review in accordance with predefined
inclusion and exclusion criteria. Following a review of the
existing literature and discussions with an expert in this field,
the present systematic review decided to focus its search on the
use of endoscopic techniques in the management of metastatic brain
tumours.
The inclusion criteria were the following: i)
Studies involving only adult (≥18 years) participants; ii) studies
in which an endoscopic procedure was conducted on a metastatic
brain lesion; iii) studies that reported specific demographic,
procedural, or outcome parameters for those with metastatic brain
lesions who received endoscopic intervention(s).
The exclusion criteria were as follows: i) Studies
involving non-human participants; ii) studies not available in the
English language; iii) studies that did not report demographic,
procedural, or outcome parameters for those with metastatic brain
lesions who received an endoscopic intervention. Duplicate studies
were removed, and for instances in which multiple papers were
written on the same trial, the study with the largest sample size
was selected.
Data recorded and discussed as part of the present
systematic review arose from distinct article selection and data
extraction steps. All articles were assessed against the previously
described inclusion and exclusion criteria at both title and
abstract and full-text screening stages by two independent
reviewers. Conflicts were resolved by a third-party reviewer.
Following study selection, the following data were extracted from
the included studies: i) Citation data; ii) study design
characteristics; iii) study population characteristics (number,
disease, intervention, age, sex, presenting symptoms, primary
cancer histology, lesion location and lesion size); iv)
intervention characteristics (aim/indication, preoperative
assessment, operative route, operative technique, adjunctive tools
and therapies, post-operative assessment; and v) outcome measures
(procedure success, duration, adverse events, length of hospital
stay (LOS), mean follow-up, and clinical outcomes). Details
surrounding the number of articles screened at each stage and the
extracted data are presented in the Results section.
Results
Study selection
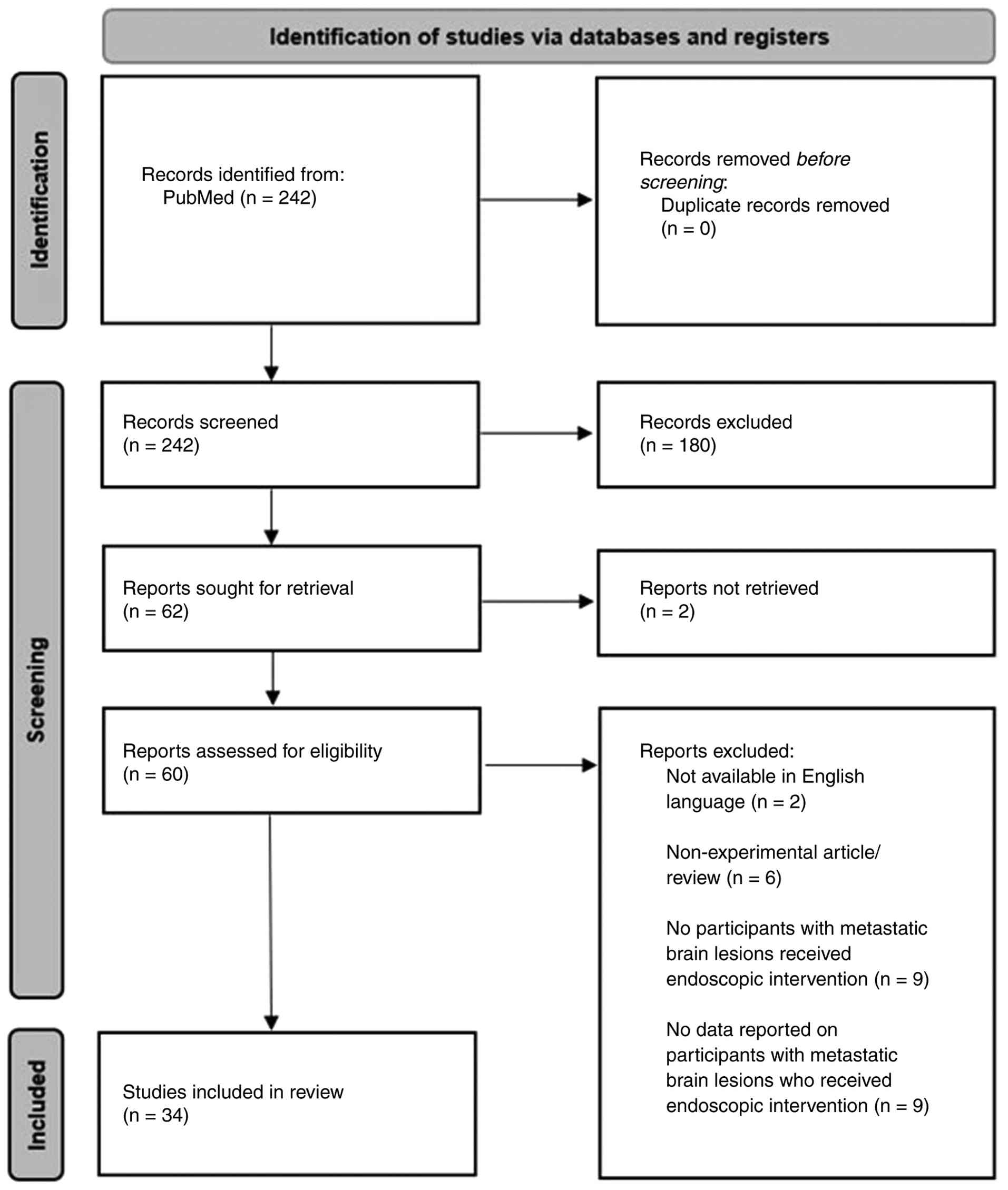
Findings from the electronic database search and
article screening stages are outlined in accordance with the most
recent PRISMA guidelines published by Page et al (6) in Fig. 1.
The literature search identified 242 articles. Covidence software
identified none of these as duplicates. Title and abstract
screening identified 62 articles meeting the inclusion and
exclusion criteria for full-text review. Upon full-text review,
studies that could not be retrieved, duplicate studies, and those
that did not meet the inclusion and exclusion criteria were
identified and removed, as illustrated in Fig. 1. Ultimately, 34 studies were selected
for data extraction and subsequent analysis as part of the present
systematic review. These are listed in Table I (7-40).
 | Table IList of the studies included in the
present systematic review. |
Table I
List of the studies included in the
present systematic review.
| First author, year
of publication | Title of study | (Refs.) |
|---|
| Andreev, 2020 | Breast cancer
metastasis into a giant hormone-inactive pituitary adenoma
(clinical case and literature review). | (7) |
| Ansari, 2020 | The Supraorbital
Eyebrow Craniotomy for Intra- and Extra-Axial Brain Tumors: A
Single-Center Series and Technique Modification. | (8) |
| Barkhoudarian,
2017 | Microsurgical
Endoscope-Assisted Gravity-Aided Transfalcine Approach for
Contralateral Metastatic Deep Medial Cortical Tumors. | (9) |
| Bettag, 2022 | Endoscope-assisted
visualization of 5-aminolevulinic acid fluorescence in surgery for
brain metastases. | (10) |
| Cathel, 2019 | Metastatic Disease
to Clivus: Biopsy or Not? | (11) |
| Ceylan, 2009 | Extended endoscopic
approaches for midline skull-base lesions. | (12) |
| Choo, 2018 | Neuroendoscopic
Cylinder Surgery and 5-Aminolevulinic Acid Photodynamic Diagnosis
of Deep-Seated Intracranial Lesions. | (13) |
| Gazzeri, 2014 | Endoscopic
supraorbital eyebrow approach for the surgical treatment of
extraaxialand intraaxial tumors. | (14) |
| Hanada, 2010 | Metastatic pineal
tumors treated by neuroendoscopic surgery-two case reports. | (15) |
| Hong, 2016 | Comparison of
endoscope- vs. microscope-assisted resection of deep-seated
intracranial lesions using a minimally invasive port retractor
system. | (16) |
| Hu, 2020 | Pituitary
Metastasis of Pulmonary Large Cell Neuroendocrine Carcinoma: A Case
Report. | (17) |
| Iacoangeli,
2012 | Endoscopy-verified
occult subependymal dissemination of glioblastoma and brain
metastasis undetected by MRI: prognostic significance. | (18) |
| Jeon, 2018 | Endoscopic
transorbital surgery for Meckel's cave and middle cranial fossa
tumors: surgical technique and early results. | (19) |
| Jimenez-Vazquez,
2017 | Neuroendoscopic and
histopathological correlation in 13 cases of cystic fluid filled
brain tumours. | (20) |
| Kassam, 2009 | Completely
endoscopic resection of intraparenchymal brain tumors. | (21) |
| Kruljac, 2010 | Hypopituitarism
caused by pituitary metastasis of supraglottic laryngeal carcinoma:
case report. | (22) |
| Kutlay, 2016 | Fully Endoscopic
Resection of Intra-Axial Brain Lesions Using Neuronavigated
Pediatric Anoscope. | (23) |
| Kutlay, 2021 | Fluorescein
Sodium-Guided Neuroendoscopic Resection of Deep-Seated Malignant
Brain Tumors: Preliminary Results of 18 Patients. | (24) |
| Kutlay, 2021 | Resection of intra-
and paraventricular malignant brain tumors using fluorescein
sodium-guided neuroendoscopic transtubular approach. | (25) |
| Ma, 2018 | Endoscopy in
Temporal Lobe Glioma and Metastasis Resection: Is There a
Role? | (26) |
| Maeshima, 2022 | Hemorrhagic brain
metastasis from small-cell carcinoma of the urinary bladder. | (27) |
| McLaughlin,
2012 | Side-Cutting
Aspiration Device for Endoscopic and Microscopic Tumor
Removal. | (28) |
| Mitsumasa,
2020 | Diplopia Presenting
in a Case of Pineal Metastasis of Pulmonary Sarcomatoid Carcinoma
Refractory to Treatment. | (29) |
| Nemoto, 2013 | Isolated pineal
region metastasis from lung adenocarcinoma with obstructive
hydrocephalus: a case report. | (30) |
| Newman, 2019 | Stereotactic-Guided
Dilatable Endoscopic Port Surgery for Deep-Seated Brain Tumors:
Technical Report with Comparative Case Series Analysis. | (31) |
| Plaha, 2014 | Minimally invasive
endoscopic resection of intraparenchymal brain tumors. | (32) |
| Serra, 2020 | Microneurosurgical
removal of thalamic lesions: surgical results and considerations
from a large, single-surgeon consecutive series. | (33) |
| Shirane, 2001 | Surgical treatment
of posterior fossa tumors via the occipital transtentorial
approach: evaluation of operative safety and results in 14 patients
with anterosuperior cerebellar tumors. | (34) |
| Souweidane,
2000 | Endoscopic Biopsy
for Tumors of the Third Ventricle. | (35) |
| Stamates, 2018 | Combined Open and
Endoscopic Endonasal Skull Base Resection of a Rare Endometrial
Carcinoma Metastasis. | (36) |
| Villanueva,
2015 | Endoscopic and
Gravity-Assisted Resection of Medial Temporo-occipital Lesions
Through a Supracerebellar Transtentorial Approach: Technical Notes
With Case Illustrations. | (37) |
| Zacharia, 2015 | Endoscopic
Endonasal Management of Metastatic Lesions of the Anterior Skull
Base: Case Series and Literature Review. | (38) |
| Zagzoog, 2017 | Metastatic
Liposarcoma of the Skull Base: A Case Report and Review of
Literature. | (39) |
| Zhang, 2018 | Clival metastasis
of renal clear cell carcinoma: Case report and literature
review. | (40) |
Patient demographics
Demographic data for the included studies are
outlined in Table SI. In total, the
included studies reported data on 686 participants, 150 of whom
received an endoscopic intervention on a non-primary brain tumour.
Within this cohort, the average age of the patients was 57 years
(range, 37-80 years), and the female-to-male ratio was 51 to 54.
Patient presenting symptoms were reported in 18 studies and are
outlined below. Tumour histology was reported by 27 of the included
34 studies for a total of 113 patients. Metastases from the lung
(42/113), breast (18/113) and melanoma (16/113) represented the
most common diagnoses. The remaining tumours were either
unclassified adenocarcinomas (10/113) or small numbers of other
tumour types, including renal (5/113), GIT (5/113) and bladder
(4/113).
Lesion location was reported in 29 studies for a
total of 115 patients and was subclassified with relation to the
tentorium cerebelli for the purposes of the present systematic
review. Supratentorial tumours represented 93 of the 115 cases and
primarily comprised tumours located in the cortex (38/115), sella
(14/115), and ventricles (10/115). Alternative locations included
subcortical (9/115), sinuses (4/115) and other/not otherwise
specified (18/115). Infratentorial tumours comprised 22 of the 115
described lesions and primarily comprised those located in the
cerebellum (10/115). Lesion size was reported in 13 of the included
34 studies. Maximum dimension was the most commonly reported
metric, with measurements ranging from 10 to 41 mm across 8
studies.
Procedures performed
Details on the operative procedure undertaken are
summarised in Table SII. Of the 34
included studies, the goal of the procedure was resection in 23,
biopsy in six studies (with ventriculostomy in 3), and both in 5
studies. The procedure was undertaken using a fully endoscopic
approach in 26 studies and in combination with microsurgery in
eight studies. The majority of procedures were undertaken using a
transcranial route via a corticotomy (20/32). Alternative routes
included extended endonasal (8/32), transorbital (3/32) and a
combined transorbital and extended endonasal approach utilised in
one study. Procedures were undertaken using rigid endoscopes in 18
of the 21 studies that reported this. Furthermore, intraoperative
fluorescence was utilized in procedures undertaken in 7 of the
included studies.
Table SII also
includes a summary of the pre- and post-operative assessments
undertaken alongside the use of adjuvant therapy. Magnetic
Resonance Imaging (MRI) was utilised in pre-operative assessment in
all 32 studies that reported on this. Computed Tomography (CT)
imaging was also performed in the preoperative assessment, utilised
in nine studies. Similarly, MRI and CT scan were used in the
post-operative assessment of patients in 26 and 11 of the 27
studies reporting this variable, respectively. The use of
adjunctive chemotherapy and radiotherapy was poorly reported (10
and 13 studies, respectively), with 5 and 11 studies reporting
their use, respectively.
Outcomes of procedures
Periprocedural outcomes reported by the studies
included in this analysis are presented in Table SIII. Procedural time was reported in
two studies, yielding an average of 122 min (range, 83-160 min).
Procedural success was measured in terms of the extent of resection
[gross total resection (GTR), near total resection (NTR) and
subtotal resection (STR)] for resections and obtaining sufficient
tissue for histological assessment for biopsies. Of the 28 studies
reporting resection as a goal, 23 studies recorded the degree of
resection in terms of the definitions of GTR, NTR and STR utilised
by the present systematic review for a cohort of 93 patients.
Within this cohort, GTR was achieved in 60 patients, NTR was
achieved in 13, and STR was achieved in 20 patients. Furthermore,
of the six studies that performed biopsies alone, the procedure was
successful in all 7 patients.
Overall, 13 studies encompassing 34 patients
reported that 28 (82%) patients demonstrated post-operative
symptomatic improvement. The overall survival was reported for 50
patients across four studies, yielding a weighted average of 12.8
months.
Adverse events were classed as intraoperative and
post-operative, and LOS was reported in days. Overall, a total of
22 participants experienced adverse events from a total of 124
participants across 15 studies. Intraoperatively, there were seven
CSF leaks and one bleed requiring 400 ml transfusion, resulting in
a total of eight intraoperative complications. Post-operatively,
there was a total of 14 individuals who experienced post-operative
adverse events, which included 3 cases of wound infection; 3 cases
of panhypopituitarism, 2 cases of transient arm paresis; one
post-operative CSF leak; one patient who suffered both a brain
abscess and pulmonary embolism; one instance of re-cannulation
where a second cannulation was required to adequately access the
target lesion; one proximal optic radiation infarct; and two deaths
in the 30 days following the procedure arising from multiorgan
failure and pulmonary embolism, respectively. Post-operative LOS
was reported for the metastatic cohort in one study in which the
patient remained in hospital for 14 days after his surgery, before
being discharged with outpatient follow-up.
Discussion
Neuroendoscopy represents a promising avenue to
facilitate the diagnosis and treatment of metastatic brain lesions
both in isolation and in conjunction with microsurgical techniques.
The present systematic review aimed to assess and summarise the
existing evidence surrounding the role of neuroendoscopy in this
setting. In undertaking the present systematic review, the authors
assessed the existing evidence and have provided aggregate measures
of the demographic factors of the study population, details of the
operative procedures undertaken, and relevant outcome measures,
including procedural success and complication rates. Throughout
this section, the relevance of the findings concerning the existing
literature in this space and the strengths and limitations of the
study are discussed, and these are applied to yield recommendations
for future research.
The initial literature search yielded 242 articles.
Following the abstract and full-text screening, 34 studies were
included for data extraction and subsequent analysis; these are
listed in Table I. Across the 34
studies, there were 686 patients, of whom 150 patients had
neuroendoscopic procedures performed for the resection or biopsy of
metastatic brain tumours.
The number of patients relevant to the present
systematic review in each study was low, with an average of 4.41
patients per study. The largest number of patients in one study was
26, while 15 of the included papers only had 1 patient who had
undergone neuroendoscopy for the biopsy or resection of a
metastatic brain tumour.
The extraction sheets were designed to contain the
most critical characteristics and outcomes that the authors were
interested in summarising. However, surprisingly, a number of the
studies did not provide information on these outcomes that is
specific to metastatic patients who had undergone neuroendoscopy
(8,11-14,16,20-25,28,29,31-33,35).
Most strikingly, only two studies, conducted by the same group,
reported the total duration of surgery (24,25),
while only one study reported LOS (7). Furthermore, data were limited for the
total length of follow-up and detailed reports of clinical outcomes
post-procedure. Likewise, the number of studies that reported on
the lesion size, the use of fluorescence, adjuvant chemotherapy, or
adjuvant radiotherapy was limited.
The average age of patients with metastatic brain
disease who had undergone neuroendoscopy was 57.46 years (range, 37
to 80 years). This is consistent with data available demonstrating
that the most common age for the incidence of brain metastases is
the 6th decade of life (41).
Furthermore, this is similar to that reported by other groups, such
as Winther et al (42) who
reported a median age of 63 years (range, 18-89 years) in their
retrospective assessment of 373 patients who underwent conventional
craniotomy and resection of single brain metastases.
A total of 28 of the 34 included studies utilised
neuroendoscopy for the resection of tumours, while the remaining
percentage only carried out biopsies. The procedural time in this
series was reported in two studies, yielding an average of 122 min
(range, 83-160 min). This is comparable to that reported in the
study by Gupta et al (43);
they reported a median operative time of 139 min (interquartile
range, 98-193 min) following their assessment of 3,500 cases of
craniotomy for resection of brain metastasis.
GTR was achieved in 64.51% of the cases, whereas in
13.98 and 21.50% of cases, NTR and STR were achieved, respectively.
A recent retrospective study by Winther et al (42) examining patients with brain
metastases, reported improved survival with GTR compared to STR,
highlighting the importance of the extent of resection. The extent
of resection rates reported in the present analysis is similar to
those reported in the study by Winther et al (42), where they found that out of 373
patients, 64% achieved GTR, and 36% achieved STR. This indicates
that with neuroendoscopic procedures, it is possible to achieve
similar extents of resection to other techniques (42).
As regards clinical outcomes, it was found that
82.35% of patients were reported to have at least some level of
symptomatic improvement. There was overall very poor reporting of
overall survival for the included patients with metastatic brain
tumours. The average of overall survival reported in four studies
(50 patients) was 14.99 months (10,18,26,38).
When weighted by the number of patients in each study, the average
overall survival is 12.82 months. This is again in line with the
study by Winther et al (42),
which reported that the median overall survival was 11.0
months.
Adverse events were poorly reported in this series,
with only 15 of the 34 included studies reporting adverse event
outcomes on a subpopulation of 124 participants (8-10,15,17,21,24-26,31,32,37-40).
Overall, a total of 22 patients suffered adverse events across
intra-operative and post-operative time periods. Intra-operatively,
there was one major haemorrhage requiring transfusion (0.8%)
reported in this series, which is infrequent compared to that of
3.65% reported by Aziz et al (44) following their assessment of 40,883
patients who underwent craniotomy for brain tumour resection. There
were seven intra-operative CSF leaks, however, only 1 participant
(0.8%) went on to experience a post-operative CSF leak which is
similar to that of 1% reported by Winther et al (42). With regards to post operative adverse
events, the aggregate figure of 11.3% observed in the present study
cohort is comparable to the 7% reported by Winther et al
(42). Notably, 2 patients in the
series examined in the present study died within 30 days of surgery
(1.6%) due to pulmonary embolism and multiorgan failure
respectively, which is less than the 3.7% of those who died in the
6 weeks following intervention in the series published by Winther
et al (42)..
Neuroendoscopy provides several unique advantages
compared to conventional microsurgical approaches, particularly in
the setting of minimally invasive surgery and applications for
label-free imaging techniques.
Minimally invasive surgery aims to limit unnecessary
damage to intracranial and extracranial tissues by minimising the
size of the access site, surgical corridor, and the degree of
intraoperative tissue retraction utilised in neurosurgical
procedures (45). In pursuit of this
aim, neuroendoscopy demonstrates several clear advantages over
microscopic and unassisted approaches through allowing a wide field
of view, slim and flexible instrumentation, and improved
illumination, which allow the use of longer, narrower, and tortuous
surgical routes (45). While the use
of minimally invasive surgical techniques requires careful patient
selection and a significant learning curve, these approaches
demonstrate clear advantages over open transcranial techniques in
terms of decreased procedural morbidity and complication rate,
quicker recovery time and improved cosmesis (45).
Furthermore, the use of neuro-endoscopes capable of
label-free imaging techniques such as narrow band imaging (NBI) may
allow intra-operative histopathological diagnosis and improve
resection margins. NBI describes the use of optical filters that
transmit only light of 540 nm (green) and 415 nm (blue)
wavelengths, which are absorbed by haemoglobin, which provides
coloration to tissues based on capillary density and architecture
(46). Endoscopic narrow band
imaging has demonstrated utility in the detection of a wide range
of early cancers, including cancers of the head and neck, upper and
lower gastrointestinal tract, urological and gynaecological tracts,
and lungs and bronchus (46). NBI
has also demonstrated applications in the setting of cerebral
malignancy, such as that reported by Sasagawa et al
(47), who found that
neuroendoscopic NBI allowed for the intraoperative identification
and biopsy of tumour surfaces which were not perceptible on white
light imaging. Additionally, the development of endoscopes capable
of other label-free imaging techniques, such as confocal laser
endomicroscopy, coherent anti-stokes Raman scattering, two-photon
excitation fluorescence and second harmonic generation also
represents promising avenues to allow intraoperative diagnosis and
improve tumour resection margins (48-51).
The present study is subject to several limitations.
First, the majority of studies included in the present systematic
review were retrospective in nature and involved small numbers of
participants that meet the inclusion criteria. These factors should
be taken into account when assessing the aggregate data and limit
the strength by which recommendations can be made based on this
evidence. Second, the present systematic review undertook data
collection through the analysis of the published manuscripts. As a
result, in some cases, heterogeneity with regard to the type and
specificity of data reported limited the amount of data specific to
our cohort of interest that could be extracted and contributed to
data loss. Lastly, the present systematic review was limited to
published manuscripts in the English language. As such, evidence,
including ongoing trials, pre-prints or other grey literature, or
those not available in the English language, have not been included
in this review.
Despite these limitations, the produced work
demonstrates several key strengths. First, present systematic
review represents the most recent summary of the literature
regarding the use of neuroendoscopy in the setting of metastatic
brain lesions, providing an update as to the recent evidence in
this space. Second, the authors utilised a broad search strategy
and inclusion criteria, which allowed the inclusion and assessment
of all relevant studies regardless of study design or size. Lastly,
the present study assessed the existing evidence across numerous
domains, including participant demographics, procedural factors and
outcome measures, including procedural success and adverse events,
which are relevant to clinical decision-making and service
planning.
Following the completion of the present study, the
following future directions for research in this field are proposed
arising from limitations of this work. First, it is recommended
that future work should stratify reported data by disease histology
and procedures undertaken to allow assessment of differential
treatment efficacy across these different patient cohorts. Second,
it is recommended that the performance of more prospective studies
with greater numbers of participants is required in order to
increase the generalizability of the study findings and provide a
stronger evidence base to inform clinical practice. Third, it is
recommended that future work should incorporate greater comparisons
and incorporate alternative methods, such as microsurgery, to allow
comparisons of efficacy and inform clinical decision-making.
In conclusion, the analysis of the aggregated data
revealed that neuroendoscopy provides a similar resection rate and
overall survival to microsurgical techniques. However, the strength
of the analysis is limited by the quality of the included studies,
the majority of which were small in scale and retrospective in
nature, and data loss arising from heterogeneity in reported data.
From the findings of the present study, several priorities have
been identified for future research, including the stratification
of outcome measure reporting by disease histology, the performance
of large-scale prospective studies, and comparisons to alternative
diagnostic and treatment modalities. Overall, the present study
demonstrates the value of neuroendoscopy as a tool to facilitate
the diagnosis and treatment of metastatic brain lesions, and we
look forward to further research in this space.
Supplementary Material
Patient demographics.
Summary of the procedures performed in
the included studies.
Summary of outcomes of
procedures.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
BF and ML contributed equally to the study. BF and
ML contributed to the conception and design of the study, to the
literature search, data extraction, analysis, drafting, and the
revision of the manuscript. UAA contributed to the conception and
design of the study, to the literature search, data extraction, and
the drafting of the manuscript. YD contributed to the conception
and design of the study, to the literature search and data
extraction. TAS supervised the study and contributed to the
conception and design of the study, and to the editing of the final
manuscript. All authors have read and approved the final version of
the manuscript. BF and ML confirm the authenticity of all the raw
data.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bettegowda C: Metastatic Brain Tumors |
Johns Hopkins Medicine. Available from: https://www.hopkinsmedicine.org/health/conditions-and-diseases/metastatic-brain-tumors.
|
|
2
|
Brain metastases - Diagnosis and treatment
- Mayo Clinic. Available from: https://www.mayoclinic.org/diseases-conditions/brain-metastases/diagnosis-treatment/drc-20350140.
|
|
3
|
Upadhyay R, Palmer JD, Klamer BG, Perlow
HK, Schoenhals JE, Ghose J, Rajappa P, Blakaj DM, Beyer S, Grecula
JC, et al: Safety and feasibility of stereotactic radiosurgery for
patients with 15 or more brain metastases. Adv Radiat Oncol.
9(101509)2024.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Shim KW, Park EK, Kim DS and Choi JU:
Neuroendoscopy: Current and future perspectives. J Korean Neurosurg
Soc. 60:322–331. 2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Issa M, Dannehl C, Büsken CJ, Ueding N,
Seitz A, Krieg SM, Unterberg AW and El Damaty A: Assessment of the
efficacy and safety of neuroendoscopic procedures for intracranial
pathologies: A single-centre retrospective study with 318
intracranial endoscopic procedures. Brain Spine.
4(104142)2024.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Page MJ, McKenzie JE, Bossuyt PM, Boutron
I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan
SE, et al: The PRISMA 2020 statement: An updated guideline for
reporting systematic reviews. Syst Rev. 10(89)2021.PubMed/NCBI View
Article : Google Scholar
|
|
7
|
Andreev DN, Kim DS, Shishkina LV, Kalinin
PL, Astafieva LI, Tropinskaya OF, Voronina IA, Turkin AM, Nazarov
VV and Kadashev BA: Breast cancer metastasis into a giant
hormone-inactive pituitary adenoma adenoma. (Clinical case and
literature review). Zh Vopr Neirokhir Im NN Burdenko. 84:55–61.
2020.PubMed/NCBI View Article : Google Scholar : (In Russian).
|
|
8
|
Ansari SF, Eisenberg A, Rodriguez A,
Barkhoudarian G and Kelly DF: The supraorbital eyebrow craniotomy
for intra- and extra-axial brain tumors: A Single-Center Series and
technique modification. Oper Neurosurg. 19:667–677. 2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Barkhoudarian G, Farahmand D, Louis RG,
Oksuz E, Sale D, Villanueva P and Kelly DF: Microsurgical
endoscope-assisted gravity-aided transfalcine approach for
contralateral metastatic deep medial cortical tumors. Oper
Neurosurg. 13:724–731. 2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Bettag C, Hussein A, Schatlo B,
Barrantes-Freer A, Abboud T, Rohde V and Mielke D:
Endoscope-assisted visualization of 5-aminolevulinic acid
fluorescence in surgery for brain metastases. J Neurosurg.
137:1650–1655. 2022.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Cathel A, Khan YR, Blais D, Mahato B and
Mahato D: Metastatic disease to clivus: Biopsy or Not? Cureus.
11(e5658)2019.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Ceylan S, Koc K and Anik I: Extended
endoscopic approaches for midline skull-base lesions. Neurosurg
Rev. 32:309–319; discussion 318-9. 2009.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Choo J, Takeuchi K, Nagata Y, Ohka F,
Kishida Y, Watanabe T, Satoh Y, Nagatani T, Kato K, Wakabayashi T
and Natsume A: Neuroendoscopic cylinder surgery and
5-aminolevulinic acid photodynamic diagnosis of deep-seated
intracranial lesions. World Neurosurg. 116:e35–e41. 2018.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Gazzeri R, Nishiyama Y and Teo C:
Endoscopic supraorbital eyebrow approach for the surgical treatment
of extraaxialand intraaxial tumors. Neurosurg Focus.
37(E20)2014.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Hanada T, Oyoshi T, Hirano H and Arita K:
Metastatic pineal tumors treated by neuroendoscopic surgery-two
case reports. Neurol Med Chir (Tokyo). 50:232–236. 2010.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Hong CS, Prevedello DM and Elder JB:
Comparison of endoscope- versus microscope-assisted resection of
deep-seated intracranial lesions using a minimally invasive port
retractor system. J Neurosurg. 124:799–810. 2016.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Hu HP, Sengupta A and Bowes D: Pituitary
metastasis of pulmonary large cell neuroendocrine carcinoma: A case
report. Cureus. 12(e7226)2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Iacoangeli M, di Rienzo A, Colasanti R,
Zizzi A, Gladi M, Alvaro L, Nocchi N, Di Somma LG, Scarpelli M and
Scerrati M: Endoscopy-verified occult subependymal dissemination of
glioblastoma and brain metastasis undetected by MRI: Prognostic
significance. Onco Targets Ther. 5:449–456. 2012.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Jeon C, Hong CK, Woo KI, Hong SD, Nam DH,
Lee JI, Choi JW, Seol HJ and Kong DS: Endoscopic transorbital
surgery for Meckel's cave and middle cranial fossa tumors: Surgical
technique and early results. J Neurosurg. 131:1126–1135.
2018.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Jimenez-Vazquez O and Nagore N:
Neuroendoscopic and histopathological correlation in 13 cases of
cystic fluid filled brain tumours. Br J Neurosurg. 31:679–681.
2017.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Kassam AB, Engh JA, Mintz AH and
Prevedello DM: Completely endoscopic resection of intraparenchymal
brain tumors. J Neurosurg. 110:116–123. 2009.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Kruljac I, Sulentić P, Cigrovski-Berković
M, Petrović V, Pećina HI, Cerina V, Houra K, Pazanin L and Vrkljan
M: Hypopituitarism caused by pituitary metastasis of supraglottic
laryngeal carcinoma: Case report. Acta Clin Croat. 49:347–351.
2010.PubMed/NCBI
|
|
23
|
Kutlay M, Kural C, Solmaz I, Tehli O,
Temiz C, Daneyemez M and Izci Y: Fully endoscopic resection of
intra-axial brain lesions using neuronavigated pediatric anoscope.
Turk Neurosurg. 26:491–499. 2016.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Kutlay M, Durmaz O, Ozer I, Klrlk A, Yasar
S, Kural C, Temiz Ç, Tehli Ö, Ezgu MC, Daneyemez M and Izci Y:
Fluorescein sodium-guided neuroendoscopic resection of deep-seated
malignant brain tumors: preliminary results of 18 patients. Oper
Neurosurg. 20:206–218. 2021.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Kutlay M, Durmaz MO, Kırık A, Yasar S,
Ezgu MC, Kural C, Temiz C, Tehli O, Daneyemez M and Izci Y:
Resection of intra- and paraventricular malignant brain tumors
using fluorescein sodium-guided neuroendoscopic transtubular
approach. Clin Neurol Neurosurg. 207(106812)2021.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Ma R, Coulter CA, Livermore LJ, Voets NL,
Al Awar O and Plaha P: Endoscopy in temporal lobe glioma and
metastasis resection: Is there a role? World Neurosurg.
117:e238–e251. 2018.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Maeshima K, Sasaki T, Yamoto T, Fukai J,
Nishibayashi H and Nakao N: Hemorrhagic brain metastasis from
small-cell carcinoma of the urinary bladder. Surg Neurol Int.
13(20)2022.PubMed/NCBI View Article : Google Scholar
|
|
28
|
McLaughlin N, Ditzel Filho LF, Prevedello
DM, Kelly DF, Carrau RL and Kassam AB: Side-cutting aspiration
device for endoscopic and microscopic tumor removal. J Neurol Surg
B Skull Base. 73:11–20. 2012.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Mitsumasa A, Shinya N, Motoki O, Hirotaka
K and Tadashi K: Diplopia presenting in a case of pineal metastasis
of pulmonary sarcomatoid carcinoma refractory to treatment. Asian J
Neurosurg. 15(449)2020.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Nemoto K, Aoshiba K, Itoh M, Semba S,
Tsuji T, Adachi H and Nakamura H: Isolated pineal region metastasis
from lung adenocarcinoma with obstructive hydrocephalus: A case
report. J Med Case Rep. 7(71)2013.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Newman WC and Engh JA: stereotactic-guided
dilatable endoscopic port surgery for deep-seated brain tumors:
Technical report with comparative case series analysis. World
Neurosurg. 125:e812–e819. 2019.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Plaha P, Livermore LJ, Voets N, Pereira E
and Cudlip S: Minimally invasive endoscopic resection of
intraparenchymal brain tumors. World Neurosurg. 82:1198–1208.
2014.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Serra C, Türe H, Yaltirik CK, Harput MV
and Türe U: Microneurosurgical removal of thalamic lesions:
Surgical results and considerations from a large, single-surgeon
consecutive series. J Neurosurg. 135:458–468. 2020.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Shirane R, Kumabe T, Yoshida Y, Su CC,
Jokura H, Umezawa K and Yoshimoto T: Surgical treatment of
posterior fossa tumors via the occipital transtentorial approach:
evaluation of operative safety and results in 14 patients with
anterosuperior cerebellar tumors. J Neurosurg. 94:927–935.
2001.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Souweidane MM, Sandberg DI, Bilsky MH and
Gutin PH: Endoscopic biopsy for tumors of the third ventricle.
Pediatr Neurosurg. 33:132–137. 2000.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Stamates MM, Lee JM, Merrell RT, Shinners
MJ and Wong RH: Combined open and endoscopic endonasal skull base
resection of a rare endometrial carcinoma metastasis. J Neurol Surg
Rep. 79:e9–e13. 2018.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Villanueva P, Louis RG, Cutler AR, Wei H,
Sale D, Duong HT, Barkhoudarian G and Kelly DF: Endoscopic and
gravity-assisted resection of medial temporo-occipital lesions
through a supracerebellar transtentorial approach: Technical notes
with case illustrations. Oper Neurosurg. 11:475–483.
2015.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Zacharia BE, Romero FR, Rapoport SK, Raza
SM, Anand VK and Schwartz TH: Endoscopic endonasal management of
metastatic lesions of the anterior skull base: Case series and
literature review. World Neurosurg. 84:1267–1277. 2015.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Zagzoog N, Ra G, Koziarz A, Provias J,
Sommer D, Almenawer SA and Reddy K: Metastatic liposarcoma of the
skull base: A case report and review of literature. Neurosurgery.
80:219–223. 2017.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Zhang WQ, Bao Y, Qiu B, Wang Y, Li ZP and
Wang YB: Clival metastasis of renal clear cell carcinoma: Case
report and literature review. World J Clin Cases. 6:301–307.
2018.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Saha A, Ghosh SK, Roy C, Choudhury KB,
Chakrabarty B and Sarkar R: Demographic and clinical profile of
patients with brain metastases: A retrospective study. Asian J
Neurosurg. 8:157–161. 2013.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Winther RR, Hjermstad MJ, Skovlund E, Aass
N, Helseth E, Kaasa S, Yri OE and Vik-Mo EO: Surgery for brain
metastases-impact of the extent of resection. Acta Neurochir
(Wien). 164:2773–2780. 2022.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Gupta S, Dawood H, Giantini Larsen A,
Fandino L, Knelson EH, Smith TR, Lee EQ, Aizer A, Dunn IF and Bi
WL: Surgical and peri-operative considerations for brain
metastases. Front Oncol. 11(662943)2021.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Aziz N, Waqar U, Bukhari MM, Uzair M,
Ahmed S, Naz H and Shamim MS: Blood transfusions in craniotomy for
tumor resection: Incidence, risk factors, and outcomes. J Clin
Neurosci. 132(111009)2025.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Laguardia S, Piccioni A, Alonso Vera JE,
Muqaddas A, Garcés M, Ambreen S, Sharma S and Sabzvari T: A
comprehensive review of the role of the latest minimally invasive
neurosurgery techniques and outcomes for brain and spinal
surgeries. Cureus. 17(e84682)2025.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Yang Q, Liu Z, Sun H, Jiao F, Zhang B and
Chen J: A narrative review: Narrow-band imaging endoscopic
classifications. Quant Imaging Med Surg. 13:1138–1163.
2023.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Sasagawa Y, Akai T, Nakada S, Minato H,
Tachibana O, Nojima T and Iizuka H: Narrow band imaging-guided
endoscopic biopsy for intraventricular and paraventricular brain
tumors: Clinical experience with 14 cases. Acta Neurochir (Wien).
156:681–687. 2014.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Breuskin D, Szczygielski J, Urbschat S,
Kim YJ and Oertel J: Confocal laser endomicroscopy in
neurosurgery-an alternative to instantaneous sections? World
Neurosurg. 100:180–185. 2017.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Ziebart A, Stadniczuk D, Roos V, Ratliff
M, von Deimling A, Hänggi D and Enders F: Deep neural network for
differentiation of brain tumor tissue displayed by confocal laser
endomicroscopy. Front Oncol. 11(668273)2021.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Galli R, Uckermann O, Sehm T, Leipnitz E,
Hartmann C, Sahm F, Koch E, Schackert G, Steiner G and Kirsch M:
Identification of distinctive features in human intracranial tumors
by label-free nonlinear multimodal microscopy. J Biophotonics.
12(e201800465)2019.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Uckermann O, Galli R, Mark G, Meinhardt M,
Koch E, Schackert G, Steiner G and Kirsch M: Label-free multiphoton
imaging allows brain tumor recognition based on texture analysis -
A study of 382 tumor patients. Neurooncol Adv.
2(vdaa035)2020.PubMed/NCBI View Article : Google Scholar
|