Introduction
Myelolipomas are rare, benign tumors composed of
mature fat and hematopoietic tissue, most commonly found in the
adrenal glands, where they account for ~6-16% of all adrenal
incidentalomas and represent the second most common adrenal lesion
following adrenal adenomas (1).
Their increased detection in recent decades is largely attributed
to the widespread use of cross-sectional imaging for unrelated
indications (2).
Extra-adrenal myelolipomas (EAMLs) are much less
common and are typically discovered incidentally (3). They most commonly arise in the
retroperitoneum, particularly the presacral region, although other
documented sites include the mediastinum, liver, spleen, lungs,
kidneys and paravertebral regions (3). When large or located in uncommon sites
such as the retroperitoneum, they can mimic malignant tumors, such
as well-differentiated liposarcoma on imaging, posing a significant
diagnostic challenge (4).
The pathogenesis of myelolipomas is not yet fully
understood. The proposed mechanisms include metaplastic
transformation of adrenal cortical cells, mesenchymal stem cell
differentiation and chronic stimulation by adrenocorticotropic
hormone (ACTH), as suggested by their association with conditions,
such as Cushing's disease and congenital adrenal hyperplasia
(1,5). Although these lesions are benign, the
presence of trilineage hematopoiesis can raise concern for
underlying hematologic disease, prompting further evaluation
(3).
The present case report describes the case of a male
patient with a large retroperitoneal EAML initially suspected to be
liposarcoma, ultimately diagnosed by core needle biopsy, with flow
cytometry used to rule out a clonal process. The present case
report highlights the diagnostic challenge posed by EAML, its
potential association with prior endocrine disorders, and the
importance of considering it in the differential for fat-containing
retroperitoneal masses.
Case report
A 79-year-old male patient with a complex medical
history, including Cushing's disease due to pituitary adenoma,
status post-transsphenoidal resection and radiation in 1999, with
resulting secondary adrenal insufficiency and secondary
hypothyroidism, diabetes, prostate cancer treated with radiation
therapy and pellet implantation in 2001, with no known recurrence,
presented to the Orlando Veterans Affairs Emergency Department
(Orlando, FL, USA) in November, 2024 with progressive weakness,
recurrent falls, and an unintentional weight loss of 18-20 lb over
a period of several months. He denied having any gastrointestinal
symptoms, such as dysphagia, nausea, or hematochezia, but reported
having a decreased appetite and intermittent constipation.
Upon admission, the patient was normotensive and his
complete blood count revealed a white blood cell count of
5.1x109/l, hemoglobin of 14.1 g/dl, hematocrit of 43.4%,
mean corpuscular volume of 94.8 fL and platelets of
208x109/l. Hemoglobin A1c was 5.9%. Endocrine laboratory
tests revealed a free T4 level of 1.6, while the morning cortisol
level was 20.6 mcg/dl and the ACTH level was 11 pg/ml, which was
consistent with his established profile on replacement therapy.
Endocrinology was consulted. Follicle-stimulating hormone and
luteinizing hormone levels had been within normal limits on
outpatient laboratory tests at 1 month prior to admission. The
analyses of vitamin B12 and folate levels, and the
electrocardiogram (EKG) results did not reveal any notable
findings. Brain magnetic resonance imaging (MRI) demonstrated a
stable pituitary gland with no evidence of a recurrent tumor. Given
his concerning constitutional symptoms, a malignancy workup was
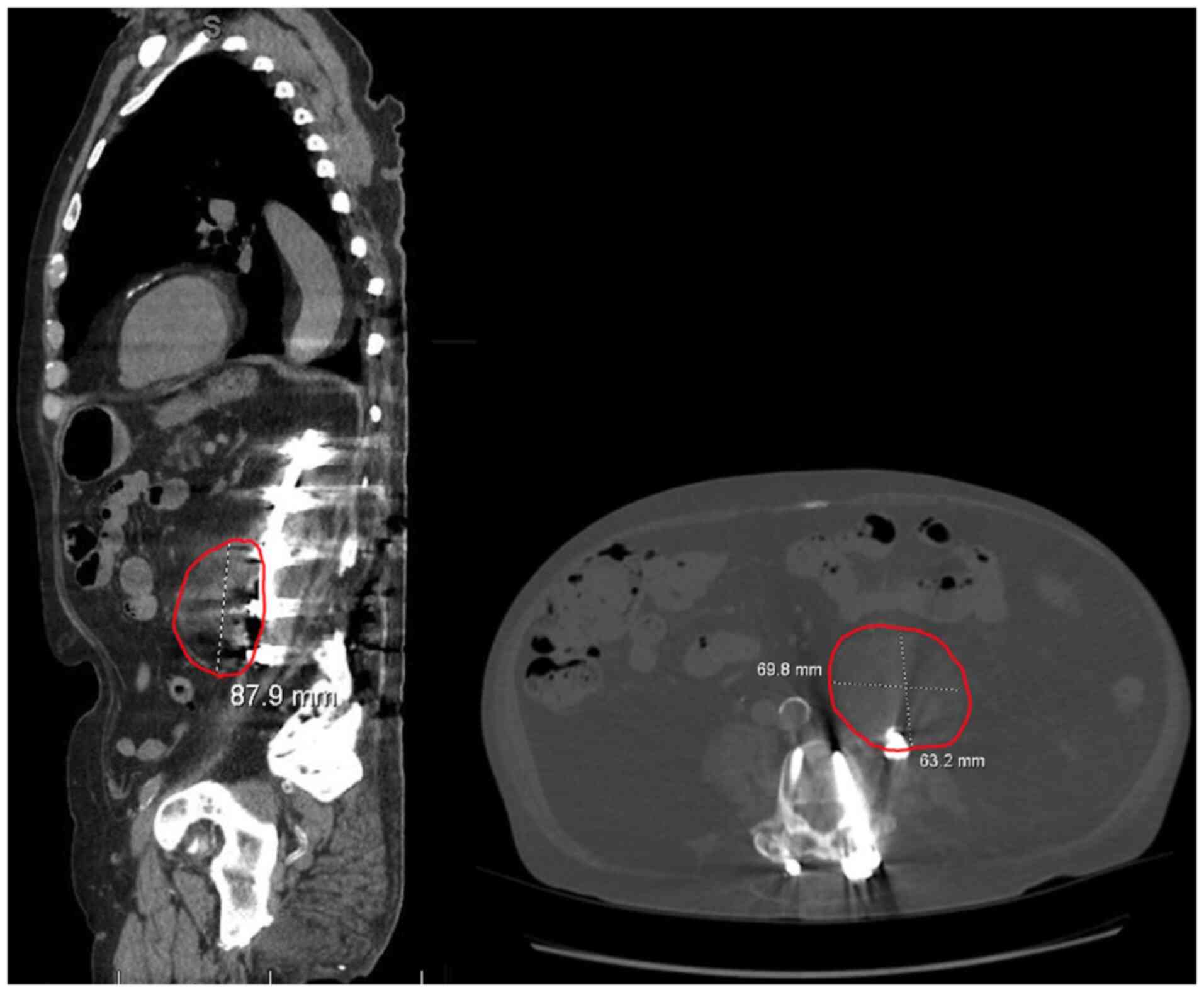
initiated. A non-contrast computed tomography (CT) scan of the
abdomen and pelvis revealed a heterogeneous fat-containing left
retroperitoneal mass measuring 6.3x7.0x8.8 cm (Fig. 1) with concerning features for
liposarcoma, including the apparent encasement of the left ureter.
Additional incidental findings included cystic pancreatic lesions
and a right renal lesion, both recommended for further
evaluation.
Due to critical comorbidities, the patient was
deemed a poor surgical candidate for mass resection. Interventional
radiologists performed a core needle biopsy. A histopathological
examination was performed using 3.5-µm-thick sections obtained from
formalin-fixed, paraffin-embedded tissue. The specimens were fixed
in 10% neutral-buffered formalin at 18-25˚C for 2-4 h. Hematoxylin
and eosin staining (Leica Biosystems) was performed at ambient
temperature for 45 min. The stained sections were examined using a
light microscope (Olympus BX43; Olympus Corporation). A
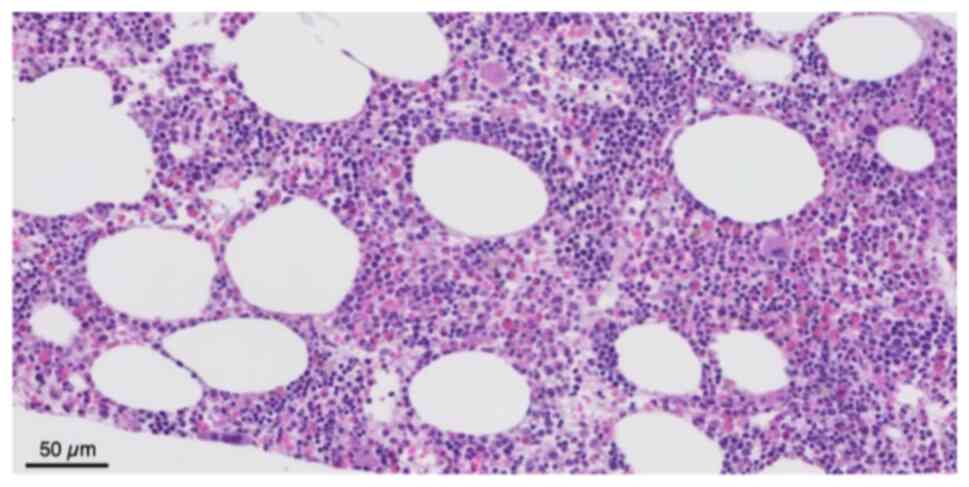
histopathological analysis revealed adipose tissue infiltrated by
trilineage hematopoietic elements, without evidence of dysplasia,
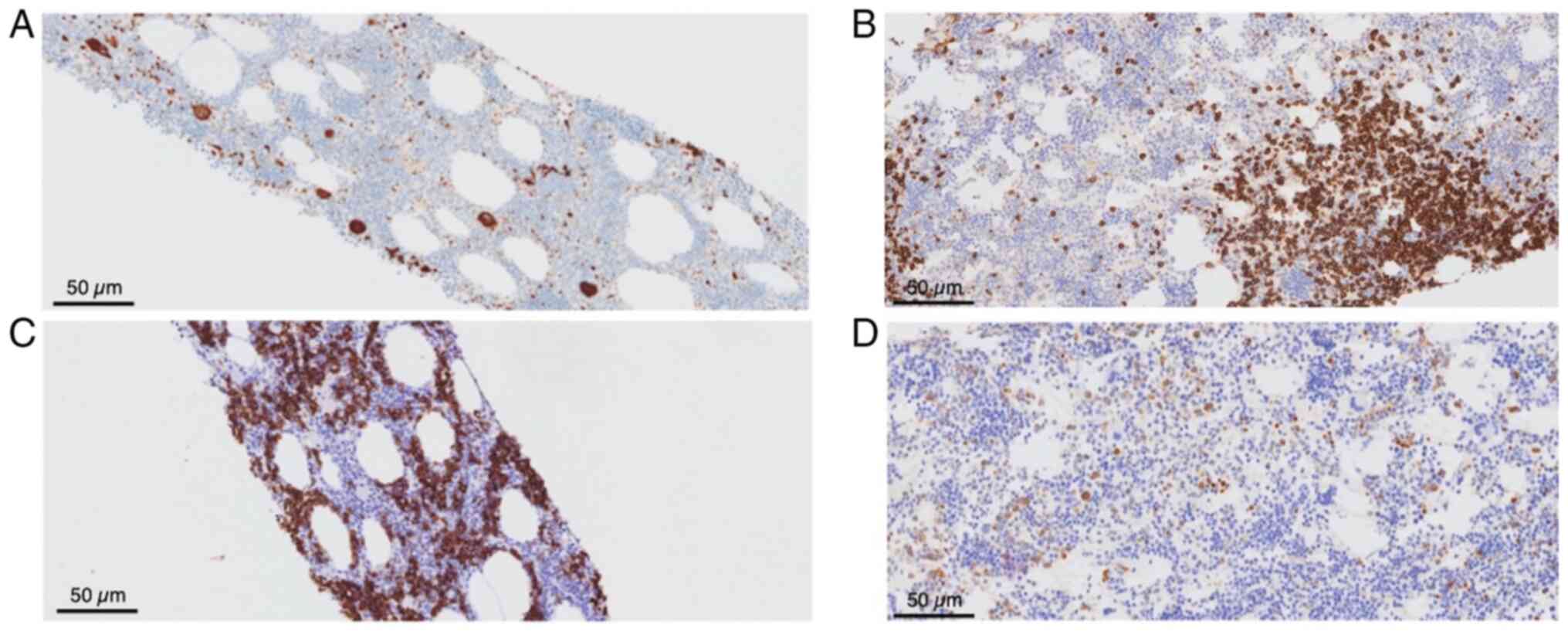
lipoblasts, or spindle cell morphology (Fig. 2). In addition, immunohistochemical
analysis was performed on 3.5-µm-thick formalin-fixed,
paraffin-embedded tissue sections using an automated Leica BOND
platform (Leica Biosystems) with a 3,3'-diaminobenzidine (DAB)
chromogenic detection system. Antigen retrieval was performed on
the Leica BOND platform under manufacturer-recommended conditions:
epitope retrieval using ER2 buffer (alkaline, Leica Biosystems) for
CD20, and ER1 buffer (citrate-based, Leica Biosystems) for MPO. For
intracellular antigens, permeabilization was achieved using the
automated Leica BOND protocol with manufacturer-provided
proprietary reagents. Blocking was performed using Leica BOND
system blocking reagents according to the manufacturer's
instructions. Primary antibodies against CD20 (clone L26, cat. no.
PA0200, Leica Biosystems, ready-to-use) and MPO (clone 59A5, cat.
no. PA0491, Leica Biosystems, ready-to-use) were incubated on the
Leica BOND platform at ambient temperature for 20 and 5 min,
respectively. CD71 and CD61 immunostains were performed at an
external reference laboratory (Quest Diagnostics) using their
validated protocols. A Leica BOND polymer-based detection system
(HRP-conjugated) was used for visualization with DAB chromogen.
Sections were counterstained with hematoxylin (Leica Biosystems) at
ambient temperature for 10 min. Immunostained sections were
examined using a light microscope (Olympus BX43; Olympus
Corporation). Immunohistochemical staining was positive for CD45,
MPO, CD71 and CD61, and negative for atypical markers (Fig. 3). Flow cytometry analysis did not
demonstrate evidence of a hematologic malignancy; however, the
corresponding raw plot data were not available for inclusion, as
only the finalized clinical report was accessible at the time of
review (data not shown). These findings were consistent with EAML,
a rare, benign lesion typically composed of mature fat and
hematopoietic tissue. Serum protein electrophoresis and globulin
fractions were also reviewed and no notable findings were obtained;
there was no evidence of a monoclonal process.
The patient remained clinically stable during
hospitalization and was discharged on the 8th hospital day with
outpatient follow-up planned with hematology/oncology.
Gastroenterology was consulted with plans for upper and lower
endoscopy as an outpatient to further evaluate his weight loss and
gastrointestinal symptoms. Given his notable comorbidities, an
echocardiogram was also recommended for outpatient follow-up to
assess cardiac function. Unfortunately, the patient succumbed
approximately 2 weeks following discharge of causes not related to
his medical condition.
Discussion
EAMLs are rare, benign tumors composed of mature
adipose tissue and trilineage hematopoietic elements (3). Of note <100 cases have been reported
in the literature, with the majority occurring in the
retroperitoneum or presacral space (3). Other documented extra-adrenal sites
include the mediastinum, liver, spleen, lungs, kidneys and
paravertebral regions (3). The mean
age at onset is 61 years and these lesions affect females more than
males (6). Lesion size varies,
although most range from 4 to 10 cm (7). The mass in the patient described herein
measured ~9 cm, placing it within the upper size range and
contributing to radiological concern for malignancy. Although
numerous patients are asymptomatic, larger lesions may cause
symptoms related to mass effect, including abdominal pain, early
satiety or urinary obstruction (8).
Unlike adrenal myelolipomas, which are more
frequently encountered, EAMLs are far less common and are often
discovered incidentally during imaging for unrelated concerns
(8). They are often identified on CT
scans or MRI as heterogeneous, fat-containing masses (8). However, their radiological appearance
can closely mimic malignancies, such as liposarcoma. The
differential diagnosis for fat containing retroperitoneal masses is
broad and carries critical management implications. Well
differentiated liposarcoma is the most important entity to exclude,
as it is the most common primary retroperitoneal fat containing
malignancy and can appear radiographically indistinguishable from
EAML on a CT scan or MRI. Histologically, liposarcomas are
characterized by the presence of lipoblasts and zones of cellular
atypia, which were absent in the patient in the present study.
Other fat-containing lesions in the differential include
angiomyolipoma, retroperitoneal teratoma, retroperitoneal lipoma
and extramedullary hematopoiesis (EMH)-related masses (9). EMH and EAML may share both imaging and
histopathological features; however, EMH typically presents as a
multifocal, poorly circumscribed lesion without macroscopic fat,
whereas EAML is usually well encapsulated with prominent adipose
tissue. Angiomyolipoma, while more commonly renal in origin, can
occasionally arise in extra-renal retroperitoneal locations and
should also be considered. Technetium-99m sulfur colloid
scintigraphy has been described in prior case reports as an
adjunctive imaging tool that can help differentiate EAML from
liposarcoma, as myelolipomatous tissue takes up the tracer, while
liposarcoma does not (6).
Nevertheless, tissue diagnosis via core needle biopsy remains the
definitive standard, as was performed in the case presented
herein.
The pathogenesis of EAMLs is not yet fully
understood. Proposed mechanisms include the metaplasia of
mesenchymal or reticuloendothelial cells, or development from
ectopic adrenal tissue (5). Although
in the patient described herein Cushing's disease was treated a
number of years prior, some literature suggests that chronic ACTH
stimulation, such as that observed in untreated or prolonged
Cushing's disease, may play a role in myelolipoma formation via
mesenchymal metaplasia (5,10). Although in the patient in the present
study Cushing's disease was surgically treated and biochemically
controlled for decades, prior prolonged exposure to elevated ACTH
levels before definitive treatment may have contributed to tumor
development. Reports of EAMLs in patients with remote endocrine
disorders are uncommon, rendering this case noteworthy.
In the patient in the present study, pathological
analysis revealed mature adipose tissue with trilineage
hematopoiesis, consistent with EMH, and no signs of atypia,
malignant transformation or necrosis, as previously described
(8). Grossly, EAMLs are
well-circumscribed, with a lobulated cut surface composed of yellow
fat and red-brown marrow-like areas (8). Flow cytometry did not reveal any clonal
populations (data not shown). Although EAMLs are considered benign
and nonfunctional, the presence of EMH raises a critical
consideration of the possibility of an underlying marrow disorder.
EMH is typically associated with conditions such as myelofibrosis,
chronic hemolysis, or thalassemia, but can also be observed in rare
benign tumors such as this one (1,11).
In the patient described herein, there were no
laboratory or clinical signs of a hematological disorder. Still,
hematology/oncology follow-up was appropriate to ensure that no
occult pathology was missed and to monitor for any evolving signs
of marrow dysfunction. Several prior case reports have described
retroperitoneal EAML initially misdiagnosed as liposarcoma,
highlighting the importance of histopathological confirmation
before committing to a treatment strategy, as the two entities
carry vastly different prognoses and operative implications
(3,4,6). Once
the diagnosis of retroperitoneal EAML is confirmed, management is
guided by lesion size, symptom burden and the presence of
complications. Conservative management with surveillance imaging is
appropriate for asymptomatic lesions. Surgical resection is
generally indicated for masses >6 cm in size, symptomatic
lesions, those causing mass effect on adjacent structures, such as
ureteral compression, or cases with persistent diagnostic
uncertainty (8). In the patient in
the present study, the mass measured 6.3x7.0x8.8 cm with apparent
ureteral encasement features that would conventionally favor
surgical resection. However, given his critical comorbidities,
operative intervention was deemed prohibitively high-risk, and a
tissue-first approach via CT-guided biopsy was appropriately
pursued. The present case report illustrates that in patients who
are poor surgical candidates, percutaneous core needle biopsy can
establish a definitive diagnosis and guide conservative management
without the risks of major surgery. Management is generally
conservative once the diagnosis is confirmed and the patient
remains asymptomatic (8). Surgery is
reserved for symptomatic lesions, diagnostic uncertainty, or rapid
growth (8). Prognosis is excellent,
with no malignant potential described (8).
The present case report highlights how EAML can
mimic malignancy and reinforces the importance of integrating
imaging, pathology, and clinical context when evaluating
fat-containing retroperitoneal masses. It also reflects how EMH,
while often benign, can sometimes serve as a clue to underlying
hematologic disease and should prompt further evaluation when
identified in unexpected locations. Additionally, it underscores
the potential role of prior endocrine disorders, such as Cushing's
disease, as a contributing factor in the pathogenesis of EAML, even
when the primary condition has been long controlled.
In the patient described herein, the experienced
weight loss was felt to be multifactorial. Contributing factors
included a decreased appetite from the mass effect of the
retroperitoneal lesion and age-related deconditioning. Thyroid
function was well controlled. It is worth noting that while
Cushing's disease is classically associated with weight gain, the
disease of the patient had been treated decades prior, and his
endocrine profile reflecting adrenal insufficiency rather than
active hypercortisolism, rendering it an unlikely contributor.
Cardiac evaluation included an EKG stable to prior, with no
clinical symptoms of cardiac disease; echocardiography was
recommended as an outpatient study to exclude cardiomyopathy.
Endoscopy was similarly deferred to the outpatient setting to rule
out an occult gastrointestinal source contributing to weight loss.
These represent limitations of this case, as a complete outpatient
workup could not be fulfilled given the unexpected passing of the
patient.
In conclusion, the present case report illustrates
the diagnostic challenge of distinguishing extra-adrenal
myelolipoma from malignancy based on imaging alone. EAML should be
considered in the differential for fat-containing retroperitoneal
lesions, particularly in patients with a history of chronic
endocrine disorders such as Cushing's disease, which may play a
role in pathogenesis. Histopathology remains essential for
definitive diagnosis, and management is typically conservative
unless the lesion is symptomatic or diagnostic uncertainty
persists.
Acknowledgements
The authors would like to express their gratitude
and sincere appreciation to the Orlando VA and University of
Central Florida College of Medicine in Orlando, FL, USA for their
support and assistance towards the completion of this project with
mentorship and access patient charts. The resources and support
provided by the hospital was invaluable in facilitating this
study.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
All authors (SZ, LD, RMA and VZ) were responsible
for the clinical workup, literature review and drafting of the
manuscript. All authors (SZ, LD, RMA and VZ) contributed to the
case interpretation and manuscript revision. All authors have read
and approved the final version of the manuscript to be published.
All authors (SZ, LD, RMA and VZ) confirm the authenticity of all
the raw data.
Ethics approval and consent to
participate
The present case report was conducted in accordance
with institutional guidelines. Consent was obtained from the
patient described herein for the presentation of his case.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of this case report and any
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Calissendorff J, Juhlin CC, Sundin A,
Bancos I and Falhammar H: Adrenal myelolipomas. Lancet Diabetes
Endocrinol. 9:767–775. 2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Bokhari MR, Zulfiqar H, Leslie SW and
Garla VV: Adrenal myelolipoma. In: StatPearls [Internet].
StatPearls Publishing, Treasure Island, FL, 2023.
|
|
3
|
Shimoda H, Kijima T, Takada-Owada A,
Ishida K and Kamai T: A case of perirenal extra-adrenal myelolipoma
mimicking liposarcoma. Urol Case Rep. 50(102523)2023.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Benko G, Kopjar A, Plantak M, Cvetko D,
Glunčić V and Lukić A: Rare case of multiple perirenal
extra-adrenal myelolipoma: Case report and literature review. Case
Rep Urol. 2021(6614641)2021.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Decmann Á, Perge P, Tóth M and Igaz P:
Adrenal myelolipoma: A comprehensive review. Endocrine. 59:7–15.
2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Cho J, Kinsey D, Kimchi ET, O'Carroll KS,
Nguyen V, Alsabbagh M and Gaballah A: Retroperitoneal extra-adrenal
myelolipoma misdiagnosed as liposarcoma: A case report. Radiol Case
Rep. 16:364–368. 2020.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Qin DA, Ren XQ, Zheng S and Bi H: An
unusual diagnosis of paravertebral lesions: Mediastinal
myelolipoma. J Int Med Res. 48(300060520936972)2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Hakim A and Rozeik C: Adrenal and
extra-adrenal myelolipomas-a comparative case report. J Radiol Case
Rep. 8:1–12. 2014.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Keshavamurthy J, Bell D and Weerakkody Y:
Extra-adrenal myelolipoma. Radiopaedia.org,
2025. https://doi.org/10.53347/rID-72212.
|
|
10
|
Park SY, Kwak MK, Kim HJ, Park HK, Suh KI,
Yoo MH, Jin SY, Yun S and Byun DW: Case report of bilateral adrenal
myelolipoma associated with Cushing disease. Medicine (Baltimore).
96(e9455)2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Gupta S, Krishnan AS, Singh J, Gupta A and
Gupta M: Clinicopathological characteristics and management of
extramedullary hematopoiesis: A review. Pediatr Hematol Oncol J.
7:182–186. 2022.
|