Introduction
In 1889, the first case of multiple primary tumors
was reported by Billroth (1). In
1932, Warren and Gates (2)
established the diagnostic criteria for multiple primary tumors,
which are still used today. Simultaneous multiple primary
malignancies of the larynx are very rare. To our knowledge, only
six cases with simultaneous multiple primary malignancies of the
larynx have been reported to date. In this study, we report a case
of simultaneous laryngeal squamous cell carcinoma (SCC) and primary
malignant fibrous histiocytoma (MFH).
Case report
The present study was approved by the Institutional
Review Board of the Hangzhou First People's Hospital, Zhejiang
Province, China. A 69-year-old Chinese woman, with no history of
smoking or alcohol consumption, was referred to our hospital in
August 2007. She complained of hoarseness for more than one year,
becoming progressively during the last two months prior to
presentation, without other symptoms. Significant physical findings
were limited to the head and neck. Indirect and flexible electronic
laryngoscopy revealed a 1.5×1.0×1.0 cm mass derived from the
subglottic region (under the anterior commissure) and the
involvement of the anterior commissure. The activity of the
bilateral vocal cord was symmetrically limited. The surface of the
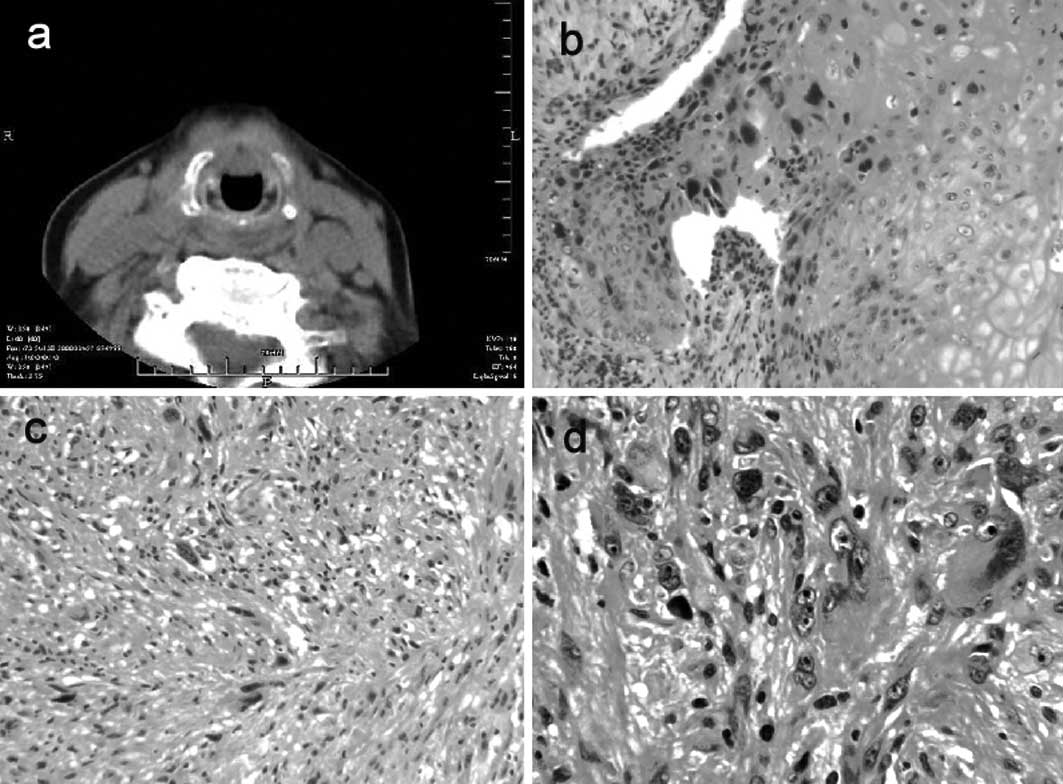
mass was smooth without ulcers, erosion or hemorrhaging. The CT
scans showed the presence of a subglottic mass under the anterior
commissure and no pathological swollen lymph nodes (Fig. 1a). The results of neck and
abdominal ultrasonography, chest X-ray and laboratory tests were
normal. The patient had a ten-year plus history of hypertension and
diabetes mellitus and her blood pressure and blood glucose were
well controlled using medication. No radiotherapy, surgery or
trauma to the neck was reported prior to onset. Biopsy was
performed prior to surgery.
A fronto-lateral partial laryngectomy with bilateral
arytenoid preservation under general anesthesia with safety margins
(>10 mm), coupled with a bilateral neck selective dissection,
were performed. The mass was removed successfully and the defection
resulting from partial laryngectomy was reconstructed with
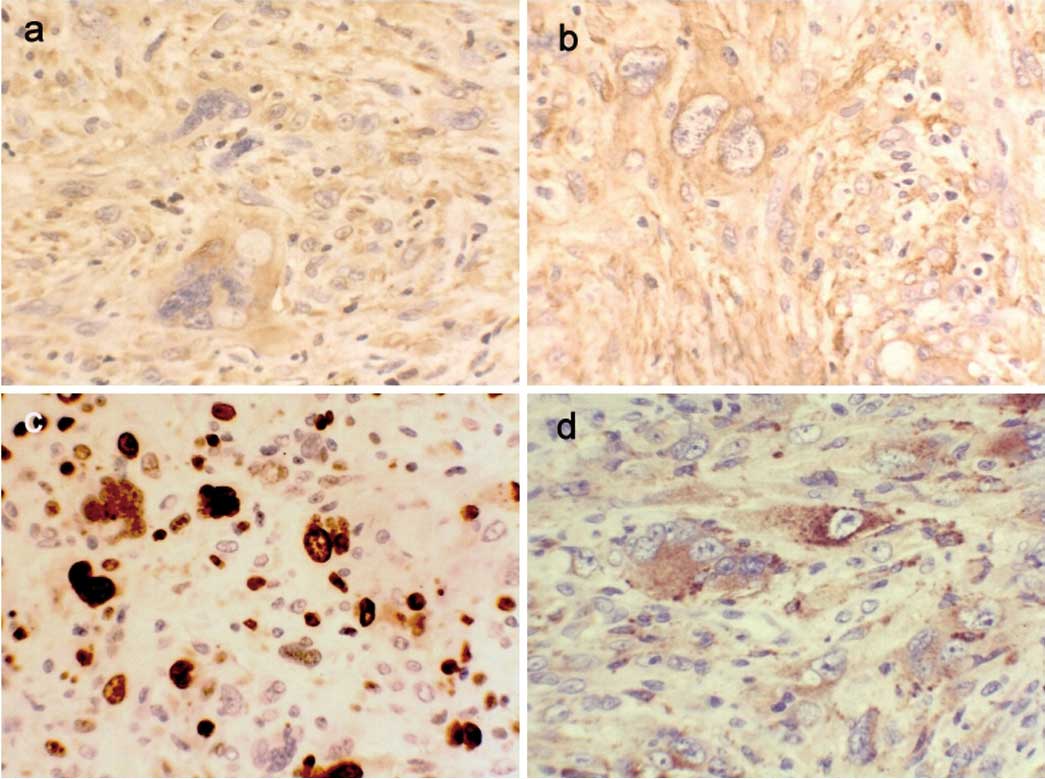
bilateral sternohyoid muscles. The excised tumor was confirmed as
moderately differentiated SCC and MFH using H&E staining
(Fig. 1b-d) and
immunohistochemical pathological testing (Fig. 2a-d). Table I lists the results of the
immunohistochemical testing of the tumor. The final pathological
diagnosis was moderately differentiated SCC with MFH, all margins
of the resected tumors appeared to be free of disease and no
metastatic lymph nodes were found in the excised neck tissue. The
follow-up period was more than 46 months, and the patient survived
without recurrence and metastasis.
 | Table IResults of immunohistochemical
analysis. |
Table I
Results of immunohistochemical
analysis.
| Antibody | Result |
|---|
| Cytokeratins
AE1/AE3 | − |
| Epithelial membrane
antigen | − |
| Desmin | − |
| Vimentin | + |
| Smooth muscle
actin | + |
| S-100 protein | − |
| Ki-67:30 | + |
| CD68 | + (sporadic) |
| MyD1 | − |
Discussion
Over 95% of laryngeal malignant neoplasms are SSCs
which are derived from mucous epithelium of the larynx. Other
tumors, including adenocarcinoma, undifferentiated carcinoma and
lymphosarcoma, are rare. MFH, a subtype of sarcoma, is a type of
non-epithelial tumor that may be of mesenchymal origin and is
composed of various cell types, including fibroblasts,
histiocyte-like cells and atypical giant cells. The incidence of
MFH is reported to be less than 2% of all malignancies in the
larynx and accounts for approximately 5% of all sarcomas of the
head and neck.
Although the etiology of MFH remains unclear, it is
generally accepted that radiation may induce MFH (3). According to the diagnostic criteria
proposed by Cahan et al (4)
and Bradley (5), the majority of
cases with MFH of the larynx are associated with radiation
(6). Our patient denied history of
treatment with or exposure to radiation and had no other observed
pathogenic factors, indicating that the etiology of MFH requires
further investigation. The prognosis of cases with MFH is
associated with tumor size, age, gender and histological grade.
Tumor size less than 3 cm, age over 60 years, female gender and
low-grade histology are regarded as favorable prognostic factors
for MFH (7). The patient in our
study was a 69-year-old woman, with tumor size smaller than 3 cm,
indicating favorable prognosis. In this case, the patient survived
without tumors for more than three years following surgery. These
results are consistent with those of previous studies and suggest
that the markers for evaluating the prognosis of MFH may also be
used in patients with laryngeal SCC with simultaneous primary
MFH.
The incidence of primary multiple malignant tumors
in the larynx is exceedingly low. The diagnostic criteria of
multiple primary tumors, which remain in use to date, were proposed
by Warren and Gates (2) in 1932.
We reviewed the previous literature and found that all six cases
were male patients with a history of tobacco and alcohol
consumption. With the exception of one case with chondrosarcoma and
epidemoid carcinoma, these cases comprised simultaneous SCC and
adenocarcinoma (two cases), chondrosarcoma (one case),
leiomyosarcoma (one case), verrucous carcinoma and squamous
papilloma (one case). To our knowledge, this is the first report of
a case with simultaneous SCC and primary MFH. In cases with
multiple tumors of the larynx, treatment is carried out according
to the types of tumor involved. For well- and
moderately-differentiated SCC, surgery is the first treatment
considered. For MFH, simple radiotherapy or simple chemotherapy is
not recommended, whereas surgery or comprehensive therapy combined
with surgery is regarded as the best choice. Sabesan et al
(8) suggested that radical
resection of a tumor is a more efficacious method for improving
survival and reducing recurrence. However, partial laryngectomy
(9) and laryngomicrosurgery
(10), which preserve laryngeal
function and improve quality of life following surgery, are
recommended in early MFH. Since the tumor in our patient was small
and localized to one region, partial laryngectomy with bilateral
neck dissection was performed without radiotherapy/chemotherapy
(pre- or post-operation). During the follow-up period, no evidence
was found of local recurrence, cervical lymph nodes or distant
metastasis. Therefore, laryngectomy with preservation of laryngeal
function can be performed in many patients with early-stage
tumors.
In conclusion, simultaneous multiple malignancies of
the larynx are rare. In this study, we report a unique case with
laryngeal moderately differentiated SCC and simultaneous primary
MFH, which was confirmed by H&E staining and
immunohistochemical testing. Our results show that the markers used
to assess the prognosis of MFH may also be used to assess
simultaneous laryngeal SCC and primary MFH and that, to preserve
laryngeal function, laryngectomy can be performed in patients with
early-stage tumors.
Abbreviations:
|
SCC
|
squamous cell carcinoma
|
|
MFH
|
malignant fibrous histiocytoma
|
References
|
1
|
T BillrothDie allgemeine chirurgische
pathologie und therapie51 Vorlesungen: Ein Handbuch Fur Studirende
und Arzte14th editionReimer GBerlin9081889
|
|
2
|
S WarrenO GatesMutiple primary malignant
tumors: a survey of the literature and a statistical studyAm J
Cancer16135814141932
|
|
3
|
YM KirovaF FeuilhadeE
CalitchiRadiation-induced sarcoma after breast cancer. Apropos of 8
cases and review of the literatureCancer
Radiother2381238619989755752
|
|
4
|
WG CahanHQ WoodardNL HiginbothamFW
StewartBL CloeySarcoma arising in irradiated bone: report of eleven
casesCancer82834199810.1002/(SICI)1097-0142(19980101)82:1%3C8::AID-CNCR3%3E3.0.CO;2-W9428476
|
|
5
|
PJ BradleyRadiation-induced tumors of the
head and neckCurr Op Otolaryngol Head Neck
Surg1097103200210.1097/00020840-200204000-00006
|
|
6
|
E GuneyOG YigitbasiS BalkanliOM
CanozPostirradiation malignant fibrous histiocytoma of the larynx:
a case reportAm J
Otolaryngol23293296200210.1053/ajot.2002.12455412239696
|
|
7
|
I HaberalE SamimM AstarciC
OzeriRadiation-induced malignant fibrous histiocytoma of the neck
in a patient with laryngeal carcinomaAm J
Otolaryngol22146149200110.1053/ajot.2001.2257911283832
|
|
8
|
T SabesanW XuexiQ YongfaT PingzhangV
IlankovanMalignant fibrous histiocytoma: outcome of tumours in the
head and neck compared with those in the trunk and extremitiesBr J
Oral Maxillofac
Surg44209212200610.1016/j.bjoms.2005.06.00616026908
|
|
9
|
KB SohGA WestmoreAA MoirPS
CollobyMalignant fibrous histiocytomas of the larynx - report of
two casesAnn Acad Med Singapore2587888119969055021
|
|
10
|
H KuwabaraK SaitoT ShibanushiT
KawaharaMalignant fibrous histiocytoma of the larynxEur Arch
Otorhinolaryngol251178182199410.1007/BF001818328080639
|