Introduction
Strong epidemiologic evidence indicates that
infections by certain types of human papillomaviruses (HPVs) are
causally linked to cervical cancer development (1). Among the high risk HPV types, HPV 16
and 18 are recognized as the main causes of invasive cervical
cancer and its precursor lesions. Little is known, however, about
HPV prevalence in patients with cervical cancer and healthy women
in Sudan, a country with a high incidence of cervical cancer.
In cervical cancer patients, alterations in many
tumor-suppressor genes have been reported (2). Among them, the two well-characterized
tumor-suppressor genes, the retinoblastoma gene (Rb) on chromosome
13q and the p53 on chromosome 17p, are both frequently inactivated
in a broad range of human cancer types (3).
Data concerning mutations of the Rb gene are
controversial with respect to cervical carcinoma. Most commonly,
pRb is inactivated by mutation of its regulators. pRb is known to
be inactivated by virally encoded oncoproteins such as E7 in
high-risk papillomaviruses (4,5).
However, the genomic changes associated both with mutations of the
Rb gene and HPV infection have not been fully established, mainly
due to the limited number and low informative capability of the
markers used.
A single nucleotide polymorphism in the p53 gene
resulting in the substitution of arginine (Arg) by proline (Pro) at
codon 72 was identified and shown to alter the primary structure of
the p53 protein (6). Biochemical
and functional differences between the two p53 forms have been
identified (7). In light of the
structural differences, it was hypothesized and subsequently
demonstrated experimentally that the Arg form of the p53 protein
was in fact more susceptible to binding and degradation by the
HPV-E6 oncoprotein than the Pro form (8). In the same study it was found that
women with invasive cervical cancer were more likely to be
homozygous for Arg at codon 72 compared to controls, suggesting
that the Arg/Arg genotype may confer greater susceptibility to
cervical cancer. Numerous subsequent investigations of the
possibility of an increased risk of cervical cancer associated with
the Arg/Arg genotype have been conducted on various populations
with controversial findings (9–14).
In summary, the two genetic alterations we analyzed
in this study have emerged as significant factors in the
pathogenesis and progression of many types of tumors and are
therefore likely to provide relevant information to assess the risk
of cervical cancer (15).
Materials and methods
Seventy-eight cervical cancer tissues and matched
peripheral blood samples were collected from patients with cervical
cancer. Patients were randomly selected regardless of age,
ethnicity or duration of the disease. Also, 36 formalin-fixed
paraffin-embedded tissues (PETs) of non-cancerous samples were used
as control for the presence of HPV. The control for the p53 study
was previously published data of 253 Sudanese individuals from
different ethnic groups (17). DNA
was extracted from fresh tissues using TRIzol reagent protocol,
while DNA from PETs was extracted using the JETQUICK kit
(Sigma-Aldrich). Histologically, the samples were diagnosed for two
types of cellular cancer, squamous cell carcinoma (SCC) and
adenocarcinoma (ADCA). The grades and stages were determined.
Detection of HPV-DNA sequence
The following primers were used: for HPV 16 (D,
5′-TTTTGGGTTACACATTTACAA-3′ and R, 5′-TGTCTGCTTTTATACTAACCG-3′);
for HPV 18 (D, 5′-GACACCTTAATGAAAAACGACG-3′ and R, 5′-CGT
CGTTGGAGTCGTTCCTG-3′). Polymerase chain reaction (PCR) was
performed in a total volume of 25 μl. The Master mix contained 1 μl
of 10 mM dNTP mix (2.5 mM dATP, 2.5 mM dGTP, 2.5 mM dCTP and 2.5 mM
dTTP), 1.5 μl of 25 mM MgCl2, 2.5 μl of 10X PCR buffer
[10 mM Tris-HCl (pH 8.3), 50 mM KCl], 1 μl of Taq polymerase (~1
U), 1.5 μl forward primer and 1.5 μl reverse primer. The final
volume was set to 25 μl per reaction mix with ddH2O. The
amplification was carried out by an initial denaturation stage at
95°C for 5 min, then 35 cycles of 95°C for 1 min and 50°C for 1
min, 55°C for 1 min and a final extension for 10 min at 72°C
followed by a final elongation stage at 72°C for 5 min.
PCR for p53 polymorphisms (Arg/Pro)
PCR was carried out for amplification of codon 72 in
the p53 gene using the following sets of proline primers: D,
5′-GCCAGAGGC TGCTCCCCC-3′ and R, 5′-CGTGCAAGTCACAGACTT-3′; and
arginine primers: D, 5′-TCCCCCTTGCCGTCCCAA-3′ and R,
5′-CTGGTGCAGGGGCCACGC-3′. The cycling profile, as well as agarose
gel electrophoresis, followed a previous protocol by Soulitzis
et al (16).
PCR-RFLP genotyping for Rb intron 1 and
17
Restriction fragment length polymorphism analysis
(RFLP) was utilized in this study to screen for loss of
heterozygosity (LOH) in two introns in the Rb gene (intron 1 and
17) using the primers: for intron 1 D, 5′-CAGGACAGCGGCCCGGAG-3′ and
R, 5′-CTGCAGACGCTCCGCCGT-3′; and for intron 17 D,
5′-TCCCACCTCAGCCTCCTTAG-3′ and R, 5′-GTAGGCCAAGAGTGGCAGCT-3′. The
PCR protocol for amplification of the Rb intron 1 and 17 was as
follows: initial denaturation was at 95°C for 5 min, followed by 30
cycles of denaturation at 95°C for 1 min and annealing at 58°C for
the primers of intron 1 and 65°C for the primers of intron 17 for 1
min. One additional cycle for the elongation step at 72°C for 5 min
completed the procedure. Five microliters of each PCR product was
added to 4 μl of loading dye and loaded onto a 2% agarose gel. DNA
molecular weight marker of 1 kb ladder was loaded onto the same
gel. The gel was examined under UV light to visualize the DNA. The
size of the bands was measured according to the migration of the
DNA ladder. Five microliters of the intronic polymorphism products
was digested overnight each with the appropriate restriction
enzymes – BamH1 for intron 1 and Xba1 for intron 17
(Fermentas Life Sciences). The resulting fragments were separated
using 2% agarose gel electrophoresis. The BamHI and
Xba1 enzymes digest PCR products with mutated alleles.
Results
Histopathology
Histopathology revealed that 82.1% (64/78) of the
cervical cancer cases were SCC and 17.9% (14/78) were ADCA. The
cases were characterized by different grades: 50% (39/78) were
moderately differentiated, 25.6% (20/78) were well differentiated
and 24.4% (19/78) were poorly differentiated. Stage II was noted in
51.3% (40/78) of the tumors followed by 24.4% (19/78) of stage III.
Stage I and IV accounted for 19.2% (15/78) and 5.1% (4/78) of the
tumors, respectively. HPV was detected in 93.6% (73/78) of cancer
samples while in non-cancerous samples these genotypes appeared in
only 8.3% (3/36) of cases. Sixty tumor samples harbored HPV
genotype 18. Single infection with this genotype was found in 40
samples (51.3%), while mixed infection was detected in 20 samples
(25.6%). The HPV genotype 16 was found in 33 tumor samples. Single
infection with this genotype appeared in 13 patients (16.7%), while
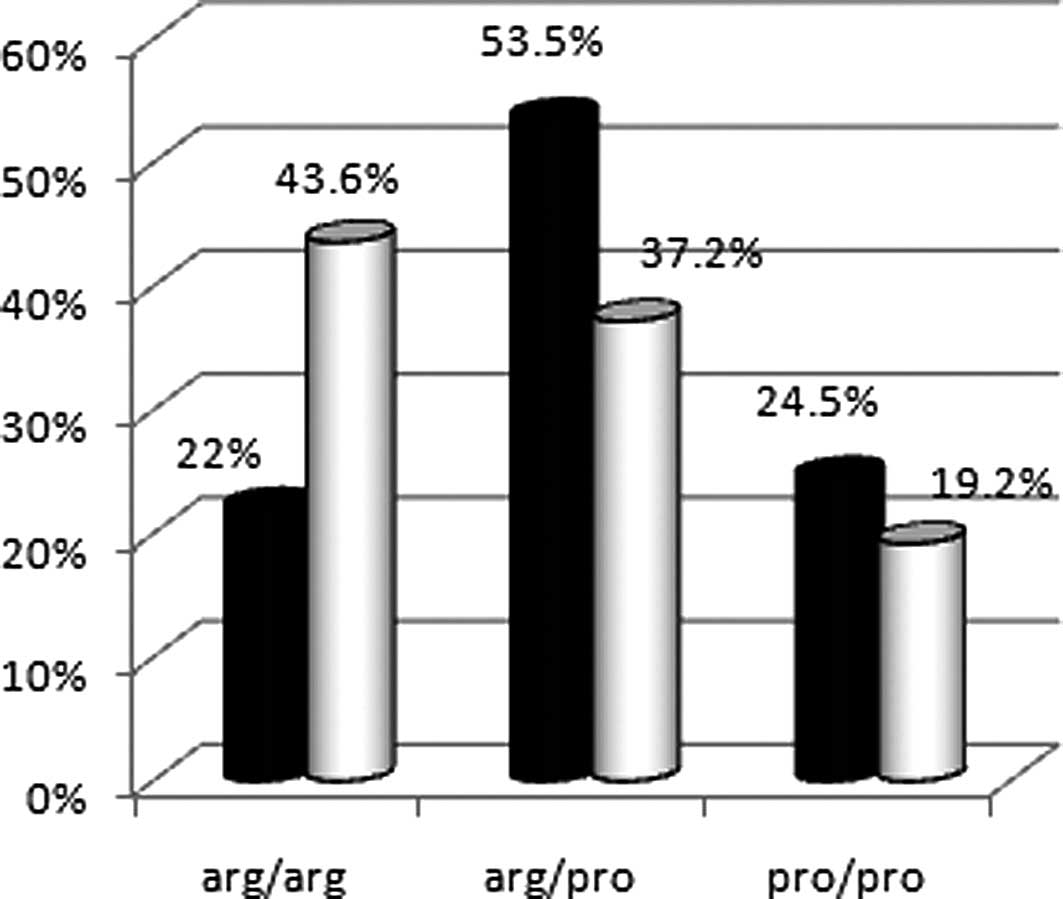
20 samples (25.6%) showed mixed infection. Genotype analysis of the
p53 codon 72 showed Arg/Arg in 43.6% (34/78), Arg/Pro in 37.2%
(29/78) and Pro/Pro in 19.2% (15/78) of tumor samples. The
P-values, confidence interval (CI) and odd ratios (OD) were
calculated for homozygous and heterozygote Arg allele. P-value was
0.015 and the OR was 2.4 (CI, 1.12–5.33) for Arg/Arg while the
heterozygous P-value was 0.78 and the OR was 0.91 (CI, 0.43–1.96).
The relative risk for Arg/Arg was 1.1.
p53 genotype distributions and allele frequencies of
cervical cancer patients were compared with data from a healthy
Sudanese control population published in 2003 (17) (Fig.
1).
LOH analysis of Rb intron 1 and 17 using
RFLP
LOH was detected in 25.6% (20/78) of patients in
intron 1 and in 37.2% (29/78) of patients in intron 17. LOH was
found in 62.8% of patients in intron 1 and/or 17. The relative risk
for LOH was 1.7.
Analysis of Rb RFLP with the p53
polymorphism
The genotypes of the p53 gene for patients wih LOH
in Rb were 43.9, 43.9 and 12.2% for Arg/Arg, Arg/Pro and Pro/Pro,
respectively, with a significant difference for the Arg allele
among this group (P=0.012). Possible epistatic effect of the Rb
RFLPs with the p53 Arg/Pro polymorphism was calculated and the
relative risk was found to be 2.5.
Histopathology of patients with LOH in
the Rb gene
SCC was noted in 80.5% of patients with LOH in the
Rb gene. Histopathology revealed that 51.2% of the cases were
moderately differentiated, 26.8% were poorly differentiated and 22%
were well differentiated. Stage II was predominant among the tumors
with LOH in the Rb gene, which was found in 61% of tumors, followed
by stage III in 24.4%, stage I in 9.8% and finally stage IV in 4.9%
of tumors. Table I summarizes the
molecular abnormalities found in patients compared with the healthy
control subjects.
 | Table IComparison between the healthy control
subjects and the cervical cancer patients regarding three
parameters: presence of HPV, p53 Arg/Pro polymorphism and LOH in
the Rb gene (intron 1 and 17). |
Table I
Comparison between the healthy control
subjects and the cervical cancer patients regarding three
parameters: presence of HPV, p53 Arg/Pro polymorphism and LOH in
the Rb gene (intron 1 and 17).
| Molecular
abnormality | Cervical cancer
patients (%) | Healthy controls
(%) |
|---|
| HPV infection |
| Frequency | 93.6 | 8.3 |
| Types |
| 18 | 51.3 | |
| 16 | 16.7 | |
| 16 plus 18 | 25.6 | |
| p53 |
| Arg/Arg | 43.6 | 22.0 |
| Arg/Pro | 37.2 | 37.2 |
| Pro/Pro | 19.2 | 53.5 |
| Rb gene (13q14)
LOH |
| Intron 1 | 25.6 | 3.0 |
| Intron 17 | 37.2 | 3.2 |
Discussion
The so-called ‘high-risk’ HPVs infect the anogenital
tract epithelium and are associated with the appearance of cervical
dysplasia in almost all cases of cervical cancer (18). In the present study, the frequency
of high-risk types HPV 16 and 18 is considered the etiological
factor in Sudanese cervical cancer patients with predominance of
HPV 18 (P=0.02). The tumor-suppressor protein p53 plays a critical
role in cell cycle control and apoptosis and response to genome
aberrations and environmental factors, including tumor viruses.
Somatic mutations in p53 have been found to exist in more than 50%
of human cancers (19). One of the
most common variant associated with cancer development is the codon
72 single nucleotide polymorphism (SNP), which results in the
substitution of proline for arginine. Codon 72 arginine homozygote
in p53 was reported to increase the risk of human
papillomavirus-associated cervical cancer (20). In this study we investigated the
association of the p53 codon 72 with cervical cancer and the
association between cancer and Arg/Arg was found to be significant
(P=0.01 and OR=2.4) although not as strongly. The Rb as well as the
p53 gene are thought to be the major target genes contributing to
the malignant transformation of the cervical epithelium in relation
to the role of HPV infection. We detected LOH of the Rb regions in
62.8% of our samples in intron 1 and/or intron 17 which is higher
than the 14% reported by Kim et al (21) and the 29% reported by Park et
al (22). The same markers
showed 55% LOH in informative cases of esophageal squamous cell
carcinoma specimens from a high-risk population in northern China
(23). Although it has been
suggested that the LOH of the chromosome 13 may be associated with
a more aggressive tumor behavior in other types of cancer, in our
cases the LOH of the Rb gene was not significantly associated with
conventional clinicopathological parameters, including clinical
stage and degree of differentiation, but our data showed a
significant association between LOH and histological type of the
tumor. Infections by the high-risk human papillomavirus (HPV)
genotypes 16 and 18 are significantly involved in cervical cancer
in Sudanese patients, and HPV 18 is the predominant one.
The p53 Arg/Arg polymorphism may be an important
determinant of the risk for cervical cancer, but it does not appear
to be sufficient for carcinogenesis. Furthermore, the
Arg72-containing allele is preferentially mutated and retained in
various human tumors, suggesting that polymorphic residue within
p53 modifies mutant behavior and in the presence of LOH Rb acts as
an additive factor increasing the risk of cervical cancer.
The LOH of the Rb gene was not significantly
associated with other parameters, such as clinical stage and degree
of differentiation and hence it cannot be a determinant of the
tumor behavior in cervical carcinoma. Although the significance of
the chromosomal allelic loss of Rb in this study may suggest that
it is a molecular marker for cervical cancer, further supportive
evidence is required.
Acknowledgements
The authors wish to acknowledge the collaboration of
the staff of the Khartoum Teaching Hospital and to thank the
patients who participated in this study. This study received
partial financial support from the International Center of Genetic
Engineering and Biotechnology (ICGEB).
References
|
1
|
Zur Hausen H: Papillomavirus infections -
a major cause of human cancers. Biochim Biophys Acta. 1288:55–78.
1996.
|
|
2
|
Kloth JN, Kenter GG, Spijker HS, et al:
Expression of Smad2 and Smad4 in cervical cancer: absent nuclear
Smad4 expression correlates with poor survival. Mod Pathol.
21:866–875. 2008.
|
|
3
|
Bookstein R and Allred DC: Recessive
oncogenes. Cancer. 71(Suppl 3): S1179–S1186. 1993.
|
|
4
|
Kamil JP, Hume AJ, Jurak I, Münger K,
Kalejta RF and Coena DM: Human papillomavirus 16 E7 inactivator of
retinoblastoma family proteins complements human cytomegalovirus
lacking UL97 protein kinase. Proc Natl Acad Sci USA.
106:16823–16828. 2009.
|
|
5
|
Heck DV, Yee CL, Howley PM and Münger K:
Efficiency of binding the retinoblastoma protein correlates with
the transforming capacity of the E7 oncoproteins of the human
papillomaviruses. Proc Natl Acad Sci USA. 89:4442–4446. 1992.
|
|
6
|
Matlashewski GJ, Tuck S, Pim D, Lamb P,
Schneider J and Crawford LV: Primary structure polymorphism at
amino acid residue 72 of human p53. Mol Cell Biol. 7:961–963.
1987.
|
|
7
|
Pim D and Banks L: p53 polymorphic
variants at codon 72 exert different effects on cell cycle
progression. Int J Cancer. 108:196–199. 2004.
|
|
8
|
Storey A, Thomas M, Kalita A, et al: Role
of a p53 polymorphism in the development of human
papillomavirus-associated cancer. Nature. 393:229–234. 1998.
|
|
9
|
Koushik A, Platt RW and Franco EL: p53
codon 72 polymorphism and cervical neoplasia: a meta-analysis
review. Cancer Epidemiol Biomarkers Prev. 13:11–22. 2004.
|
|
10
|
Jee SH, Won SY, Yun JE, Lee JE, Park JS
and Ji SS: Polymorphism p53 codon-72 and invasive cervical cancer:
a meta-analysis. Int J Gynaecol Obstet. 85:301–308. 2004.
|
|
11
|
Settheetham-Ishida W, Singto Y, Yuenyao P,
Tassaneeyakul W, Kanjanavirojkul N and Ishida T: Contribution of
epigenetic risk factors but not p53 codon 72 polymorphism to the
development of cervical cancer in Northeastern Thailand. Cancer
Lett. 210:205–211. 2004.
|
|
12
|
Lee SA, Kim JW, Roh JW, et al: Genetic
polymorphisms of GSTM1, p21, p53 and HPV infection with cervical
cancer in Korean women. Gynecol Oncol. 93:14–18. 2004.
|
|
13
|
Comar M, Molin GD, Guaschino S and
Campello C: p53 at codon 72 polymorphism, human papillomavirus
infection and cervical lesions: a cross-sectional study from
northeastern Italy. Eur J Obstet Gynecol Reprod Biol. 114:210–214.
2004.
|
|
14
|
Ueda M, Hung YC, Terai Y, Saito J,
Nunobiki O, Noda S and Ueki M: Glutathione-S-transferase and p53
polymorphisms in cervical carcinogenesis. Gynecol Oncol.
96:736–740. 2005.
|
|
15
|
Scambia G, Lovergine S and Masciullo V: RB
family members as predictive and prognostic factors in human
cancer. Oncogene. 25:5302–5308. 2006.
|
|
16
|
Soulitzis N, Sourvinos G, Sourvinos DN and
Spandidos DA: P53 codon 72 polymorphism and its association with
bladder cancer. Cancer Lett. 179:175–183. 2002.
|
|
17
|
Bereir RE, Mohamed HS, Seielstad M, et al:
Allele frequency and genotype distribution of polymorphisms within
disease-related genes is influenced by ethnic population
sub-structuring in Sudan. Genetica. 119:57–63. 2003.
|
|
18
|
Zur Hausen H: Papillomaviruses and cancer:
from basic studies to clinical application. Nat Rev Cancer.
2:342–350. 2002.
|
|
19
|
Smardová J, Nemajerová A, Trbusek M,
Vagunda V and Kovarík J: Rare somatic p53 mutation identified in
breast cancer: a case report. Tumor Biol. 22:59–66. 2001.
|
|
20
|
Zehbe I, Voglino G, Wilander E, et al: P53
codon 72 polymorphism and various human papillomavirus 16 E6
genotypes are risk factors for cervical cancer development. Cancer
Res. 61:608–611. 2001.
|
|
21
|
Kim JW, Lee CG, Han SM, et al: Loss of
heterozygosity of the retinoblastoma and p53 genes in primary
cervical carcinomas with human papillomavirus infection. Gynecol
Oncol. 67:215–221. 1997.
|
|
22
|
Park JS, Dong SM, Kim HS, et al: Detection
of p16 gene alteration in cervical cancer using tissue
microdissection and LOH study. Cancer Lett. 136:101–108. 1999.
|
|
23
|
Xing EP, Yang GY, Wang LD, Shi ST and Yang
CS: Loss of heterozygosity of the Rb gene correlates with pRb
protein expression and associates with p53 alteration in human
esophageal cancer. Clin Cancer Res. 5:1231–1240. 1999.
|