Introduction
Liver fibrosis is a wound-healing response to
several chronic liver diseases including chronic viral hepatitis,
alcoholic liver disease and autoimmune hepatitis (1,2).
Liver fibrosis is a serious public health problem which may
progress to cirrhosis, liver cancer and death (3).
Certain therapeutic approaches executed in
experimental or clinical studies have been demonstrated to prevent
the progression of liver fibrosis, however numerous patients do not
respond to these strategies (4–7). In
addition, numerous pharmacological agents have been investigated in
preclinical studies. However, few of them have entered clinical
validation (7,8). At present, the only effective
treatment for advanced cirrhosis is liver transplantation, however
this is limited by numerous factors including donor shortage, risk
of rejection and high costs (9).
Stem cell therapy is another attractive approach for liver fibrosis
that has been researched in recent years. The preliminary results
appear promising, however, the experimental design has not been
appropriate for the demonstration of its safety and efficacy in
liver cirrhosis (10). Thus, novel
therapies to reverse fibrosis are urgently required (11).
Vascular endothelial growth factor (VEGF), one of
the most widely studied angiogenic growth factors, is critical for
migration and proliferation of endothelial cells and formation of
new vessels (12). Previous
studies have indicated that VEGF gene injection or simultaneous
preoperative injection of recombinant adenoviral vectors with VEGF
gene effectively stimulates liver regeneration in cirrhotic rats
(13,14). However, the half-life of VEGF is
short and the metabolic degradation is too fast, thus it cannot be
retained at a high enough level at the target site for a sufficient
period to execute its function (15). Therefore, increasing the local
concentration may improve the efficiency of VEGF.
It has been demonstrated that collagen-binding VEGF
(CBD-VEGF) can specifically bind to collagen I and maintain its
biological activity in vitro and in vivo (16). Liver fibrosis is characterized by
increased deposition of extracellular matrix (ECM), which contains
collagens I and III (17). Thus,
collagen may be a potential target for VEGF at the fibrotic
site.
In the current study, the anti-fibrotic effect of
CBD-VEGF was investigated in a carbon tetrachloride
(CCl4)-induced liver fibrotic mouse model.
Materials and methods
Preparation of CBD-VEGF
CBD-VEGF was prepared as previously described
(16). Briefly, the full-length
complementary DNA of human VEGF165 was amplified from the
complementary DNA of human breast tumor cell line MCF-7. CBD-VEGF
was constructed by linking a sequence that encodes the
collagen-binding domain (TKKTLRT) with human VEGF165 complementary
DNA. Then, the encoding gene of CBD-VEGF was inserted into pET-28a.
The plasmid was transformed into the BL21 strain of Escherichia
coli. The protein was expressed and then purified by nickel
chelate chromatography and HiTrap heparin HP columns.
Animals
Male Balb/c mice (n=30; age, 6 weeks; weight, 22–25
g) were obtained from Experimental Animal Center of Nanjing Medical
University (Nanjing, China) and were kept in a standard laboratory
in an air-conditioned room with free access to food and water. All
experimental protocols were conducted according to the Guide for
the Care and Use of Laboratory Animals (18) and were approved by the Ethics
Review Board for Animal Studies of Nanjing Drum Tower Hospital,
Nanjing University Medical School (Nanjing, China).
Induction of liver fibrosis
Liver fibrosis was induced as described previously
with slight modifications (19).
Specifically, 19 mice were treated with CCl4 (diluted 1:5 in olive
oil, 5 µl/g) intraperitoneally twice weekly for 12 weeks. Three
mice died during the period of CCl4 injection. For the
normal control group, 11 mice were injected with the same volume of
olive oil. Following 12 weeks of the injection, 6 mice in the
normal control group and 6 mice with the CCl4 injection
group were sacrificed by cervical dislocation, and blood samples
were collected from the heart and the liver samples were also
collected.
CBD-VEGF injection
Subsequent to being treated with CCl4 for 12 weeks,
a total of 15 mice were randomly assigned to three groups: The i)
normal saline (NS) group (n=5); ii) CBD-VEGF group; and Balb/c mice
were assigned as the normal control group (n=5). Mice were
anesthetized by intraperitoneal injection with 40 mg/kg body weight
of 1% pentobarbitol sodium (Merck & Co., Inc., Whitehouse
Station, NJ, USA). Subsequent to anesthesia, 50 µl (10 µg) CBD-VEGF
was injected directly into 6 sites of the liver tissue of mice. For
NS and the normal control group, the same volume of NS was injected
into the liver tissue of mice as control. Mice of the CBD-VEGF and
NS groups were continued to be injected intraperitoneally with CCl4
with a lower dose (5 µl/g; diluted 1:6 in olive oil) twice weekly
for 4 weeks.
Assessment of liver functions
After 4 weeks of CBD-VEGF injection, mice were
sacrificed by cervical dislocation and the blood samples were
collected from the heart. Serum alanine aminotransferase (ALT) and
albumin (ALB) were measured using a 7600-020E full-automatic
biochemical analyzer (Hitachi, Ltd., Tokyo, Japan).
Histological analysis and
immunohistochemistry
Subsequent to sacrifice, the liver tissue was
collected. The liver tissues were then fixed with 4%
paraformaldehyde and embedded in paraffin, then sectioned (2 µm)
and stained with hematoxylin and eosin (HE) for general observation
or with Masson's trichrome staining for detection of collagen
deposition. The relative area of liver fibrosis was measured from 6
randomly selected fields in the slide using Image-Pro Plus software
(IPP version 6.0; Media Cybernetics, Inc., Silver Spring, MD,
USA).
For immunohistochemistry, serial sections were
deparaffinized, hydrated and incubated with antibodies from Abcam
(Cambridge, MA, USA) against α-smooth muscle actin (α-SMA; 1:800;
ab5694), CD31 (1:600; ab28364) and Ki67 (1:300; ab16667),
respectively. The sections were incubated at 4 ̊C overnight with
the primary antibodies. The sections were washed with
phosphate-buffered saline (PBS) three times, and incubated for 20
min at 37 ̊C with IgG antibody conjugated to horseradish peroxidase
(HRP; ZhongShan-Golden Bridge Biological Technology Company,
Beijing, China; catalog no. PV-8000). The slices were washed with
PBS for three times, and incubated in diaminobenzidine (DAB) and
counterstained with hematoxylin for 1 min. α-SMA positive areas
were quantified from 6 randomly selected fields from each animal
sample using Image-Pro Plus software [α-SMA positive area =
(percent of α-SMA positive area in the selected region-vascular
luminal area)/total α-SMA positive area]. The number of
CD31-positive microvessels and Ki67-positive proliferation
hepatocytes were counted from 6 randomly selected fields of each
sample in the operative region under a magnification of ×400.
TUNEL assay
The fluorescent terminal deoxynucleotidyl
transferase dUTP nick-end labeling (TUNEL) assay was performed
using an in situ cell death detection kit (Roche Diagnostics
GmbH, Mannheim, Germany) to evaluate the hepatocyte apoptosis.
Briefly, following routine deparaffinization and treatment with 3%
H2O2 for 20 min, the sections were digested
with pepsin at 37°C for 30 min and incubated with the TUNEL
reaction mixture at 37°C for 60 min. DAB was added and visualized
using a Converter-POD. Hematoxylin dye was used for
counterstaining. Apoptotic cells were quantified by counting
TUNEL-positive nuclei. For each sample, the number of
TUNEL-positive cells was counted under a magnification of ×400. Six
representative fields were evaluated for each mouse of the
experimental groups.
Statistical analysis
All the data were expressed as mean ± standard
deviation and were analyzed with SPSS software for Windows (version
16.0; SPSS, Inc., Chicago, IL, USA). An independent sample t-test
was used to determine the statistical differences between two
groups. Multiple group comparisons were tested using one-way
analysis of variance. P<0.05 was considered to be indicate a
statistically significant difference.
Results
CCl4-induced liver
fibrosis
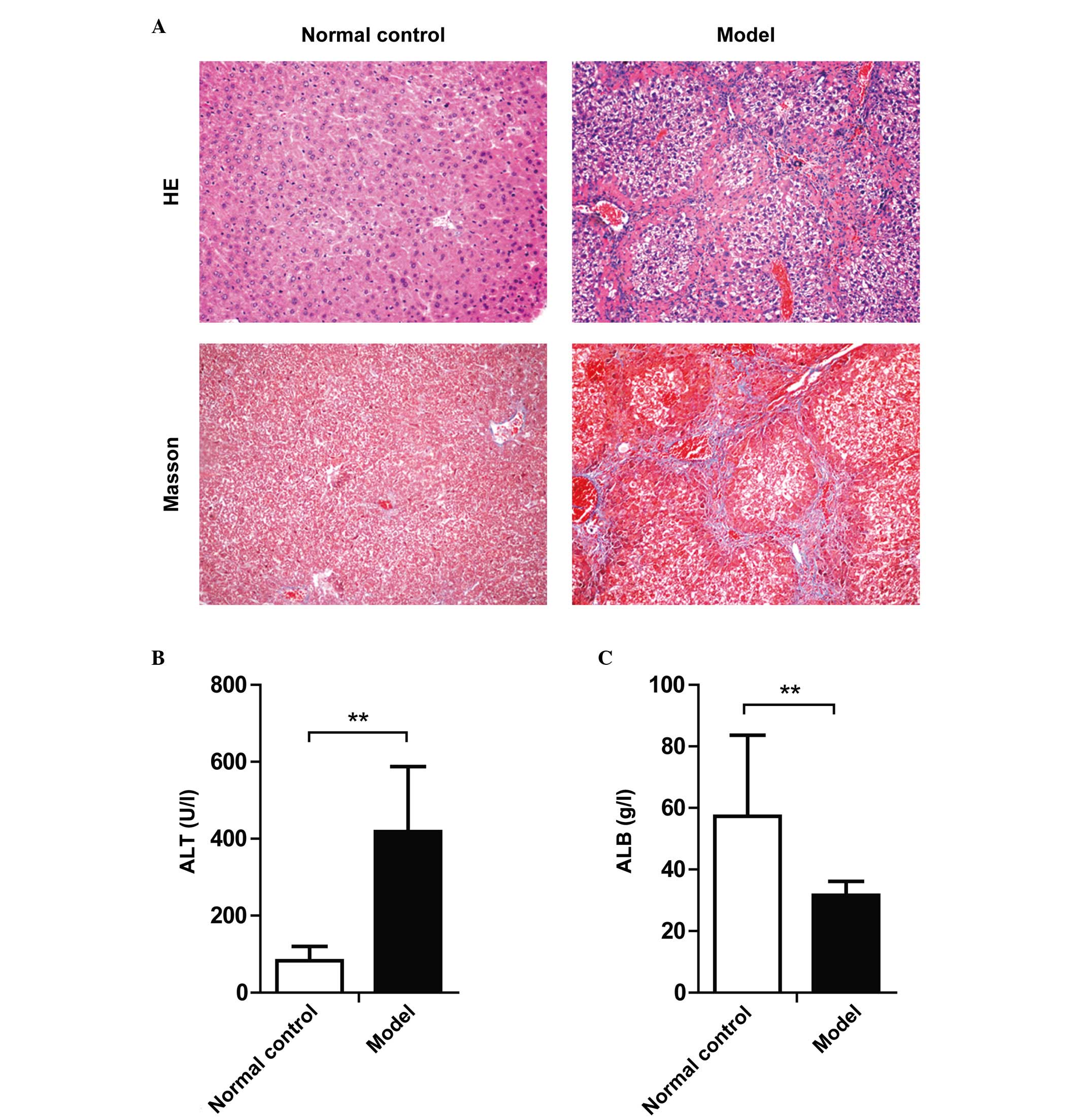
As indicated by the HE and Masson's trichrome
staining, significant liver cell degeneration, necrosis,
inflammatory cell infiltration and collagen deposition were
identified in the liver tissue of mice after 12 weeks of CCl4
injection (Fig. 1A). In addition,
significant elevation of serum ALT and reduction of serum ALB
levels was observed (Fig. 1B and
C). Serological and histological analysis demonstrated that the
liver fibrosis mouse model was constructed successfully.
CBD-VEGF alleviated
CCl4-induced liver inflammation and fibrosis
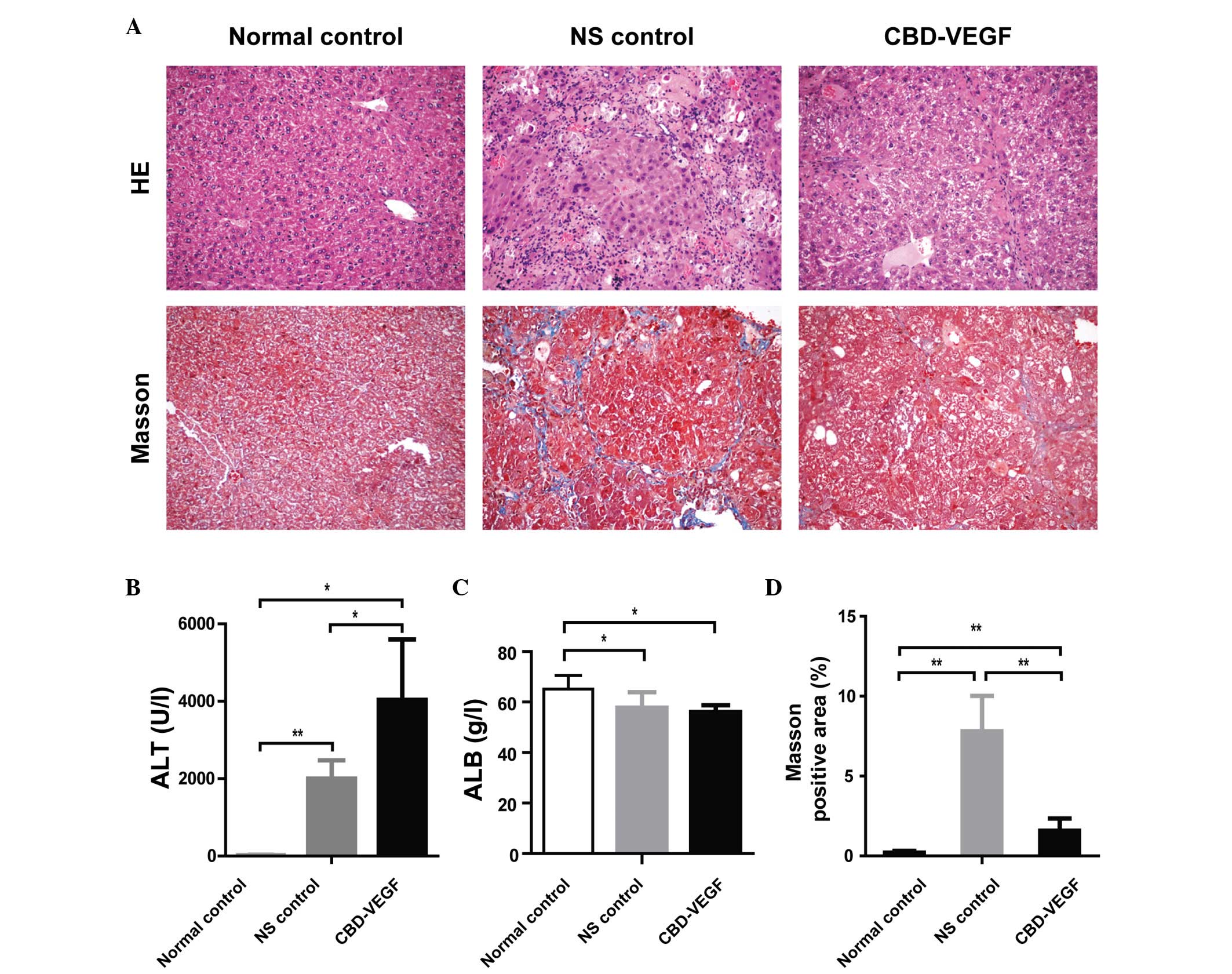
As demonstrated in tissue sections stained with HE,
compared with sections from livers in the normal controls,
CCl4 injection resulted in prominent degeneration,
necrosis and inflammatory cell infiltration. However, the necrosis
and inflammation of the liver in the CBD-VEGF group were slighter
than NS group (Fig. 2A).
After 4 weeks of CBD-VEGF injection, the serum ALT
levels were significantly increased in the CBD-VEGF and NS groups
as compared with the normal control group (Fig. 2B). The serum ALT levels of the
CBD-VEGF group were significantly higher than that of the NS group
(P<0.05). The ALB levels were significantly reduced in the
CBD-VEGF group and NS group as compared with the normal control
group. However, no significant difference was identified between
the CBD-VEGF and NS groups (Fig.
2C).
To assess the impact of CBD-VEGF on hepatic
fibrogenesis resulting by CCl4, liver sections were
stained with Masson's trichrome for detecting the deposition of
collagens (Fig. 2A). Compared with
sections from normal controls, liver sections from NS group
indicated prominent blue staining in the fibrotic septa between
nodules, suggesting a high level of collagen deposition. However,
the CBD-VEGF injection could significantly reduce the size stained
with Masson's trichrome in the livers when compared with the NS
group (P<0.01; Fig. 2D).
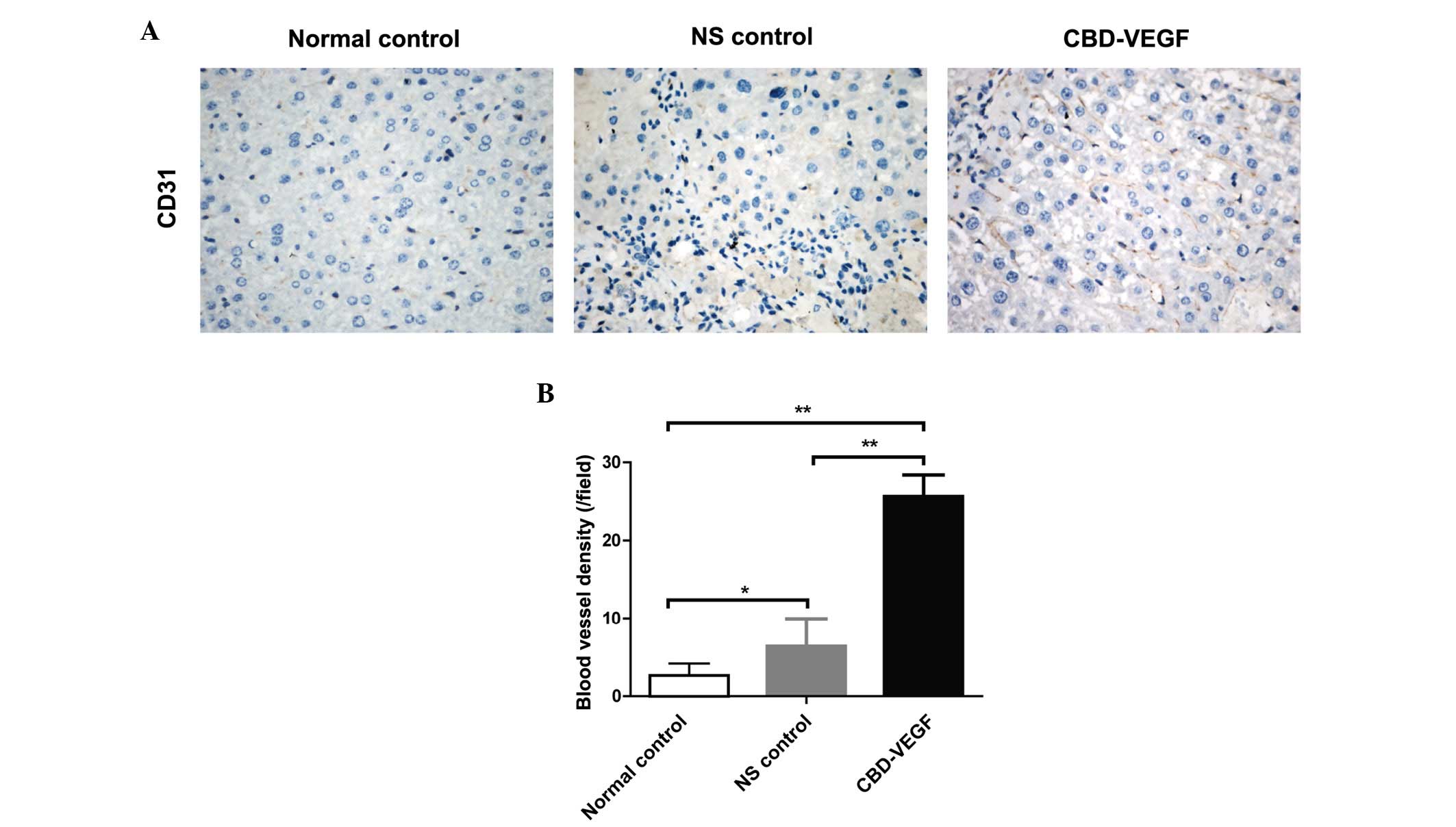
CBD-VEGF increased blood vessel
formation
To detect the angiogenesis effect of CBD-VEGF,
microvessels in the liver tissue where measured by
immunohistochemical staining for CD31 (Fig. 3A). Following 4 weeks of CBD-VEGF
injection, the blood vessel density in the CBD-VEGF group was
significantly higher than that of NS group (Fig. 3B; P<0.01).
CBD-VEGF promoted hepatocyte
proliferation, suppressed hepatocyte apoptosis and activated
hepatic stellate cell (HSC) activation
Ki67, a nuclear antigen for cell proliferation, was
used to determine whether CBD-VEGF could promote hepatocyte
proliferation (Fig. 4A). Following
4 weeks of CBD-VEGF injection, the numbers of proliferative
hepatocytes in the CBD-VEGF group were significantly increased
compared with that of the NS group (P<0.01; Fig. 4B).
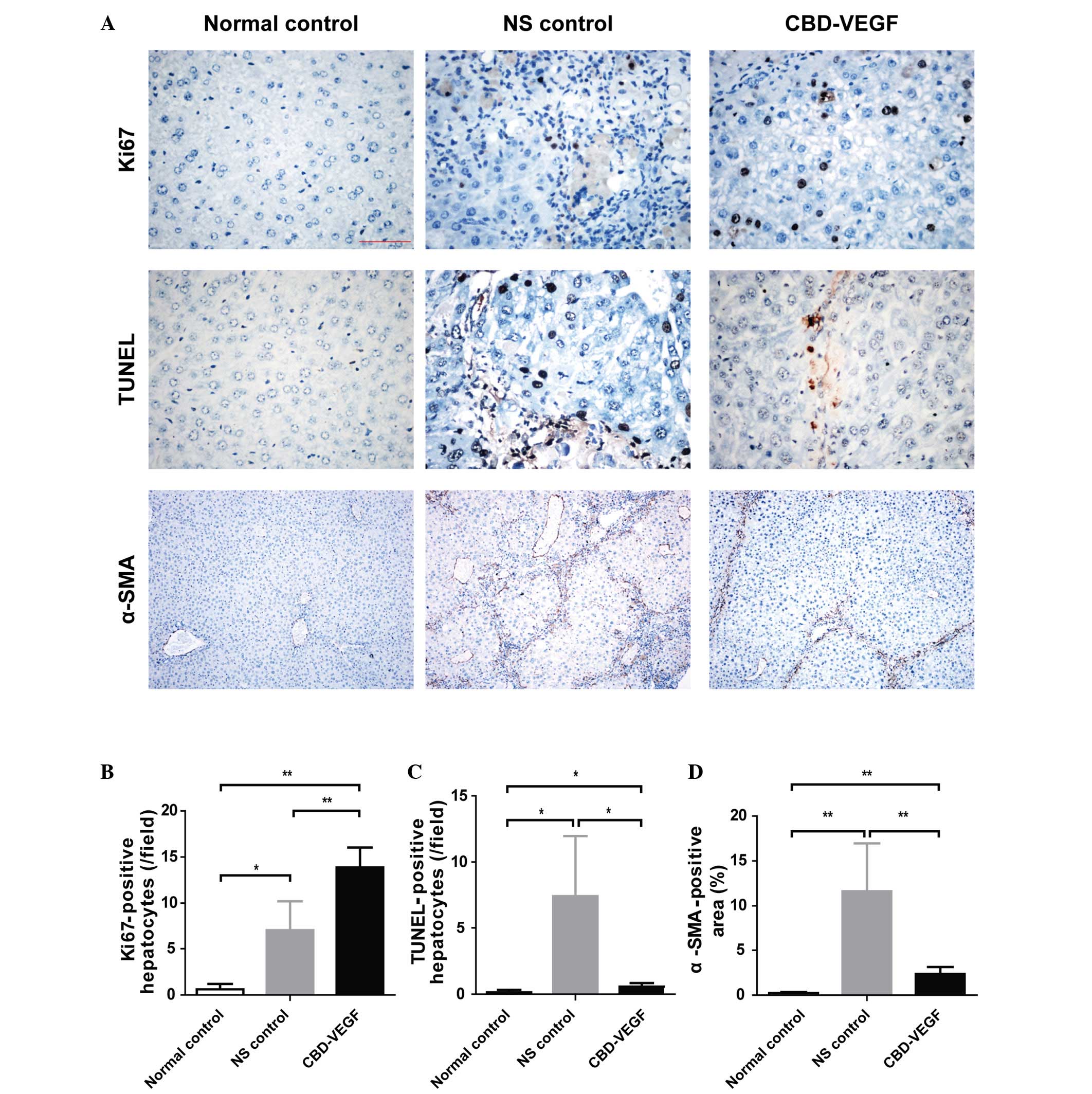 | Figure 4.CBD-VEGF promoted hepatocyte
proliferation and suppressed hepatocyte apoptosis and HSC
activation. Immunohistochemical staining of Ki67 and α-SMA in
addition to a TUNEL assay were performed in the liver sections of
each group. (A) Upper panels, Ki67 immunohistochemical staining
(magnification, ×400); middle panels, TUNEL assay for evaluation of
hepatocyte apoptosis (magnification, ×400); lower panels, α-SMA
immunohistochemical staining (magnification, ×100). (B) Statistical
analysis of proliferative hepatocytes, (C) TUNEL-positive
hepatocytes and (D) α-SMA positive area of each group. n=5 for each
group. Data are presented as the mean ± standard deviation;
**P<0.01, *P<0.05. CBD-VEGF, collagen-binding domain-vascular
endothelial growth factor; HSC, hepatic stellate cells; α-SMA,
α-smooth muscle actin; NS, normal saline. |
TUNEL assay was performed to evaluate the hepatocyte
apoptosis (Fig. 4C). The NS group
indicated a significant increase of hepatocyte apoptosis as
compared with the normal control group (P<0.01). However, the
CBD-VEGF group indicated a significantly smaller number of
TUNEL-positive hepatocytes than that of NS group (P<0.05).
α-SMA is the unique marker for HSC. To evaluate the
effect of CBD-VEGF on HSC activation, α-SMA immunohistochemistry
was examined in liver tissue (Fig.
4A). Compared with the normal control group, the α-SMA positive
areas were significantly increased in the NS group (Fig. 4D; P<0.01). However, the
SMA-positive areas were significantly reduced following CBD-VEGF
injection (P<0.01).
Discussion
Liver fibrosis is a characteristic of numerous types
of chronic liver diseases resulting from chronic injury to the
liver (20). Following chronic
damage, HSC are activated and transdifferentiate into
myofibroblast-like cells, secreting large amounts of ECM.
Accumulation of the ECM would distort the hepatic vasculature and
lead to shunting of the portal and arterial blood, impairing the
material exchange between hepatocyte and hepatic sinusoidal blood
(3). Hepatocytes cannot obtain the
necessary oxygen and nutrients and thus this results in cell
apoptosis (21). Therefore,
promoting angiogenesis can improve hepatic microcirculation, and in
turn reduce fibrosis (22).
VEGF is an endothelial cell-specific mitogen that
improves the proliferation and migration of endothelial cells in
vitro and induces new blood vessel growth in vivo
(12). VEGF-induced angiogenesis
has been used in tissue repair and regeneration (23). Administrating exogenous VEGF in
injury site is an effective therapeutic method for promoting tissue
repair and regeneration.
In patients with liver cirrhosis, the VEGF levels
have been observed to be significantly reduced and therefore,
administration of exogenous VEGF may be beneficial (21,24,25).
Administering an adenoviral vector encoding murine VEGF into bile
duct ligation fibrotic mice can promote tissue repair, and blockade
of VEGF can significantly delay tissue repair (26). Injection of a plasmid encoding VEGF
through the portal vein has been reported to induce the formation
of fenestrae and reduce portal vein pressure in
CCl4-induced cirrhotic rats (21).
However, it is difficult for VEGF to retain an
effective local concentration due to its short half-time and rapid
diffusion to extracellular fluids (15). Multiple injections may be required
to maintain VEGF concentration. This would thus increase both the
risk and cost of this potential therapy. Furthermore, excessive
VEGF at injection sites and the diffusion of VEGF may cause
possible adverse effects. Thus, a highly efficient and safe
delivery system is required to enhance its local therapeutic
efficiency and reduce its possible adverse effects.
Research groups are investigating how to localize
and sustain VEGF proteins at the sites of injury. A previous study
has demonstrated that CBD-VEGF had the characteristics of both
specific binding to collagen and a stimulating effect on
endothelial cell proliferation in vitro (16). It has been demonstrated that
CBD-VEGF can be retained and concentrated at the border zone of
infarction to improve cardiac function in the rat myocardial
infarction model (16). CBD-VEGF
can also be retained and concentrated at the local wound and
promote diabetic wound healing in a rat diabetic wound model
(27). In the full-thickness rat
uterus injury model, CBD-VEGF injection was observed to result in a
high local concentration and prolonged biological effect of the
growth factor, and thus promote remodeling of the scarred uterus
and improve uterine function (28).
Liver fibrosis is associated with major alterations
in the composition of the ECM. In advanced cirrhosis, the liver
contains approximately 6 times more ECM than normal, including
collagens I and III (29). The
native collagen could serve as a potential target for CBD-VEGF. In
the present study, CBD-VEGF was injected directly into the liver
tissue of the CCl4 induced fibrotic mice. The results
indicated that CBD-VEGF injection could significantly attenuate the
CCl4-induced chronic liver injury and fibrosis.
It remains unclear how CBD-VEGF promotes liver
regeneration. The current study demonstrated that angiogenesis is
significantly increased in the CBD-VEGF group compared with the NS
group. It is suggested that the liver fibrotic attenuation by
CBD-VEGF may be due to the increased vascularity which leads to the
increased access to nutrients and oxygen for the hepatocytes. Ki67
was used to determine whether CBD-VEGF may promote hepatocyte
proliferation. The results indicated that CBD-VEGF may promote
hepatocyte regeneration in the mouse fibrotic liver model. To
evaluate whether CBD-VEGF injection may protect hepatocytes from
apoptosis, the TUNEL assay was performed. The results indicated
that hepatocyte apoptosis was significantly reduced following
injection of CBD-VEGF. Thus, it is hypothesized that exogenous
CBD-VEGF may facilitate the transportation of nutrients and growth
factors to hepatocytes through the microcirculation by upregulating
angiogenesis and thus promoting hepatocyte regeneration and
preventing hepatocyte apoptosis and HSC activation.
Taken together, the current study demonstrated that
injection of CBD-VEGF could significantly promote angiogenesis and
attenuate liver fibrosis in the liver of CCl4-induced
fibrotic mice. The anti-fibrotic mechanisms of CBD-VEGF may be
associated with the promotion of hepatocyte regeneration and the
reduction of hepatocyte apoptosis and HSC activation. CBD-VEGF may
potentially provide a novel treatment option for liver
fibrosis.
Acknowledgements
The current study was supported by the Strategic
Priority Research Program of the Chinese Academy of Sciences (grant
no. XDA01030000), the National Natural Science Foundation of China
(grant nos. 81470093 and 81672025), the Jiangsu Province's
Outstanding Medical Academic Leader Program (grant no. LJ201154),
the Jiangsu Province Clinical Medicine and Technology Special
Program (grant no. BL2012034) and the Natural Science Foundation of
Jiangsu Province for Young Scholars (grant no. BK20160121).
Glossary
Abbreviations
Abbreviations:
|
ALB
|
albumin
|
|
ALT
|
alanine aminotransferase
|
|
CBD
|
collagen-binding domain
|
|
CBD-VEGF
|
collagen-binding vascular endothelial
growth factor
|
|
CCl4
|
carbon tetrachloride
|
|
ECM
|
extracellular matrix
|
|
HE
|
hematoxylin and eosin
|
|
HSC
|
hepatic stellate cells
|
|
NS
|
normal saline
|
|
SMA
|
smooth muscle actin
|
|
TUNEL
|
terminal deoxynucleotidyl transferase
dUTP nick-end labeling
|
|
VEGF
|
vascular endothelial growth factor
|
References
|
1
|
Bataller R and Brenner DA: Liver fibrosis.
J Clin Invest. 115:209–218. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tsukada S, Parsons CJ and Rippe RA:
Mechanisms of liver fibrosis. Clin Chim Acta. 364:33–60. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Schuppan D and Afdhal NH: Liver cirrhosis.
Lancet. 371:838–851. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Inagaki Y, Nemoto T, Kushida M, Sheng Y,
Higashi K, Ikeda K, Kawada N, Shirasaki F, Takehara K, Sugiyama K,
et al: Interferon alfa down-regulates collagen gene transcription
and suppresses experimental hepatic fibrosis in mice. Hepatology.
38:890–899. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Veldt BJ, Heathcote EJ, Wedemeyer H,
Reichen J, Hofmann WP, Zeuzem S, Manns MP, Hansen BE, Schalm SW and
Janssen HL: Sustained virologic response and clinical outcomes in
patients with chronic hepatitis C and advanced fibrosis. Ann Intern
Med. 147:677–684. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bruno S, Stroffolini T, Colombo M, Bollani
S, Benvegnù L, Mazzella G, Ascione A, Santantonio T, Piccinino F,
Andreone P, et al: Sustained virological response to
interferon-alpha is associated with improved outcome in HCV-related
cirrhosis: A retrospective study. Hepatology. 45:579–587. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Schuppan D and Pinzani M: Anti-fibrotic
therapy: Lost in translation? J Hepatol. 56:(Suppl 1). S66–S74.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pinzani M, Rombouts K and Colagrande S:
Fibrosis in chronic liver diseases: Diagnosis and management. J
Hepatol. 42:(Suppl). S22–S36. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Alqahtani SA: Update in liver
transplantation. Curr Opin Gastroenterol. 28:230–238. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lorenzini S and Andreone P: Stem cell
therapy for human liver cirrhosis: A cautious analysis of the
results. Stem Cells. 25:2383–2384. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Popov Y and Schuppan D: Targeting liver
fibrosis: Strategies for development and validation of antifibrotic
therapies. Hepatology. 50:1294–1306. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yancopoulos GD, Davis S, Gale NW, Rudge
JS, Wiegand SJ and Holash J: Vascular-specific growth factors and
blood vessel formation. Nature. 407:242–248. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Oe H, Kaido T, Mori A, Onodera H and
Imamura M: Hepatocyte growth factor as well as vascular endothelial
growth factor gene induction effectively promotes liver
regeneration after hepatectomy in Solt-Farber rats.
Hepatogastroenterology. 52:1393–1397. 2005.PubMed/NCBI
|
|
14
|
Oe H, Kaido T, Furuyama H, Mori A and
Imamura M: Simultaneous transfer of vascular endothelial growth
factor and hepatocyte growth factor genes effectively promotes
liver regeneration after hepatectomy in cirrhotic rats.
Hepatogastroenterology. 51:1641–1647. 2004.PubMed/NCBI
|
|
15
|
Silva EA and Mooney DJ: Spatiotemporal
control of vascular endothelial growth factor delivery from
injectable hydrogels enhances angiogenesis. J Thromb Haemost.
5:590–598. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhang J, Ding L, Zhao Y, Sun W, Chen B,
Lin H, Wang X, Zhang L, Xu B and Dai J: Collagen-targeting vascular
endothelial growth factor improves cardiac performance after
myocardial infarction. Circulation. 119:1776–1784. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Friedman SL: Molecular regulation of
hepatic fibrosis, an integrated cellular response to tissue injury.
J Biol Chem. 275:2247–2250. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
National Research Council, . Guide for the
Care and Use of Laboratory Animals. NIH Publications (USA);
Bethesda: pp. 85–23. 1985
|
|
19
|
Zhang D, Jiang M and Miao D: Transplanted
human amniotic membrane-derived mesenchymal stem cells ameliorate
carbon tetrachloride-induced liver cirrhosis in mouse. PLoS One.
6:e167892011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Friedman SL: Liver fibrosis-from bench to
bedside. J Hepatol. 38:(Suppl 1). S38–S53. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Xu H, Shi BM, Lu XF, Liang F, Jin X, Wu TH
and Xu J: Vascular endothelial growth factor attenuates hepatic
sinusoidal capillarization in thioacetamide-induced cirrhotic rats.
World J Gastroenterol. 14:2349–2357. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kantari-Mimoun C, Castells M, Klose R,
Meinecke AK, Lemberger UJ, Rautou PE, Pinot-Roussel H, Badoual C,
Schrödter K, Österreicher CH, et al: Resolution of liver fibrosis
requires myeloid cell-driven sinusoidal angiogenesis. Hepatology.
61:2042–2055. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ferrara N: Vascular endothelial growth
factor: Basic science and clinical progress. Endocr Rev.
25:581–611. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Assy N, Paizi M, Gaitini D, Baruch Y and
Spira G: Clinical implication of VEGF serum levels in cirrhotic
patients with or without portal hypertension. World J
Gastroenterol. 5:296–300. 1999.PubMed/NCBI
|
|
25
|
Akiyoshi F, Sata M, Suzuki H, Uchimura Y,
Mitsuyama K, Matsuo K and Tanikawa K: Serum vascular endothelial
growth factor levels in various liver diseases. Dig Dis Sci.
43:41–45. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Yang L, Kwon J, Popov Y, Gajdos GB, Ordog
T, Brekken RA, Mukhopadhyay D, Schuppan D, Bi Y, Simonetto D and
Shah VH: Vascular endothelial growth factor promotes fibrosis
resolution and repair in mice. Gastroenterology. 146:1339–1350.e1.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yan X, Chen B, Lin Y, Li Y, Xiao Z, Hou X,
Tan Q and Dai J: Acceleration of diabetic wound healing by
collagen-binding vascular endothelial growth factor in diabetic rat
model. Diabetes Res Clin Pract. 90:66–72. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Lin N, Li X, Song T, Wang J, Meng K, Yang
J, Hou X, Dai J and Hu Y: The effect of collagen-binding vascular
endothelial growth factor on the remodeling of scarred rat uterus
following full-thickness injury. Biomaterials. 33:1801–1807. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Benyon RC and Iredale JP: Is liver
fibrosis reversible? Gut. 46:443–446. 2000. View Article : Google Scholar : PubMed/NCBI
|