Introduction
Unplanned expansions of cities, along with economic
development and to rising energy demand, have caused numerous
environmental problems and serious risks for human health. Indeed,
air pollution has always been a serious threat for society health
and for environment on the global scale (1–3).
Industries, urban traffic and combustion of fossil
fuels for energy production are main sources of most of the organic
and mineral compounds, oxidants and acids, and fine particles. They
play a significant role in air pollution of most of the urban areas
(4).
Impact of air pollution on human health has been
investigated for many years. Mechanisms through which air pollution
affects human health are very complex and not yet fully understood
(5).
Since nasal cavity is the most common route of
entrance of pollutants into the body, the combinations of gases,
fine particles and chemical compounds in the indoor and outside
environments can have adverse effects on health. Moreover,
respiratory mucosa is very vulnerable to degeneration. It is the
first organ damaged in its functionality due to air pollution
(6–10). However, the consequences of
long-term exposure to air pollution have not been clarified.
Epidemiological researches confirmed there is a
direct relationship among air pollution and respiratory disease
symptoms, lung failure, chronic bronchitis and number of deaths due
to respiratory problems (11).
Various epidemiological studies, carried out in the
USA and Europe, showed that air pollution might increase risk of
lung cancer (12) and the
mortality rate due to cardiovascular strokes (13). Other studies, also conducted in
USA, showed there is a direct relationship between rate of
mortality and the amount of sulphate and other pollutants in the
air (14).
Thus, air pollution has been declared by the World
Health Organization (WHO) as one of main causes of human cancer
(5).
PM10 plays a leading role in different
respiratory symptoms. Indeed, they cause temporal alteration of
lung function and, so, they cause increase of respiratory disease
rate and hospital admissions and the morbidity rate of
cardiovascular diseases (15–19).
In 2005 edition of Air Quality Guideline, WHO
established that nitrogen dioxide (NO2), ozone
(O3), sulfur trioxide (SO3), and particulate
matter (PM) are air pollutants that affect human health
significantly (1). The
Environmental Protection Agency (EPA) fixed National Ambient Air
Quality Standards for six principal pollutants, which are called
‘criteria’ air pollutants (2).
Although, since the first decade of the 20th
century, some air pollution control programs have been conducted in
many industrially developed countries to preserve human health and
prevent environmental pollution, actually air quality is daily
getting worse in most developing countries (1). Due to growth of air pollution, the
residents have an increased risk perception of respiratory diseases
(20).
Shiraz is the third largest city of Iran in terms of
extension also it is in a special geographical location (being
enclosed by mountains). Shiraz has both a high density of
industries near urban area and a major urban traffic. All these
factors lead to air pollution increase in the city.
Therefore, the main aim of the present study was to
investigate the relationship between air pollutants and mortality
rate related to leukemia and lung cancer.
Materials and methods
Pollutant data
This longitudinal study was carried out in Shiraz.
Data on six main air pollutants, CO, SO2, O3,
NO2, PM10 and PM2.5 were obtained
from Fars Environmental Protection Agency and these data are
related to 3,001 measurement days starting from, 1 January, 2005.
These data were collected from two fixed monitoring stations
located at opposite points of the city (Kazeroon gate and Imam
Hussein square). Moreover, the daily minimum, maximum and average
measurements of climatic factors such as temperature, humidity,
wind speed and air pressure were obtained from Shiraz
Meteorological Organization. Additionally, we considered rainfall,
sunshine hours and daily evaporation rate.
Although meteorological data were complete, data
related to air pollutants had some missing days. Lack of
measurements of some pollutants in different times may have
different reasons including obstruction of the filter that measure
specific pollutants, blackout of electricity due to technical
reasons. Thus, when data were accessible from both stations, we
used mean concentration of pollutants to be more accurate.
However, some days, no information was available
from any station. We used statistical methods to forecast pollutant
concentrations in these cases: i) time series method was used for
prediction in case that missing data were <5% of the earlier
period, e.g., data related to CO concentration were completed using
this method. ii) Missing items, which were >5% of the earlier
period, were predicted by these data and by nonlinear regression
method.
In total, more than 2,000 different models were used
for all variables in this study to complete data properly.
Finally, data related to number of deaths due to
both lung cancer and leukemia, in the investigated period, were
obtained from Shiraz University Hospital.
Statistical analysis
Principal component analysis was performed on the
meteorological variables and three major factors, were selected.
Based on this statistical model, maximum and minimum temperature,
maximum humidity and evaporation were replaced only by mean
temperature variable. The variables known as sunshine magnitude and
rainfall level were replaced only by rainfall level. Additionally,
the maximum wind speed was considered as a separate factor. Then,
correlation of the above factors with pollutants and cancers was
analyzed and the correlation coefficient was determined.
Autoregressive Moving Average (ARMA), Auto
Regression Integrated Moving Average (ARIMA) and Moving Average,
statistical models were used for the factor fluctuation modeling
over time. P<0.05 indicates a statistically significant
difference.
Results
Tables I–III show statistical analyses for
cancer, air pollution, and meteorological parameters. As shown in
Table I, the cancers studied in
this survey did not match with any models. However, consistencies
of air pollution and meteorological parameters are reported in
Tables II and III.
 | Table I.Fitting models for cancer data. |
Table I.
Fitting models for cancer data.
| Sites of cancer | Models (p, d, q) |
|---|
| Lung cancer in
male | NAa |
| Lung cancer in
female | NAa |
| Lymphoid cancer in
male | ARIMA (0,0,0) |
| Lymphoid cancer in
female | ARIMA (0,0,0) |
| Myeloid cancer in
male | NAa |
| Myeloid cancer in
female | ARIMA (0,0,0) |
| Table III.Fitting models for meteorological
data. |
Table III.
Fitting models for meteorological
data.
| Meteorological
parameters | Models (p, d,
q) |
|---|
| Minimum
temperature | IMA (0,1,16) |
| Maximum
temperature | ARIMA (2,1,14) |
| Mean
temperature | ARIMA (1,1,12) |
| Minimum
humidity | IMA (0,1,7) |
| Maximum
humidity | ARIMA (1,1,2) |
| Precipitation | ARMA (1,0,7) |
| Sunshine | ARMA (1,0,3) |
| Evaporation | ARIMA (2,1,2) |
| Maximum wind
velocity | IMA (0,1,2) |
| Table II.Fitting models for air pollution
data. |
Table II.
Fitting models for air pollution
data.
| Air pollutant
parameters | Models (p, d,
q) |
|---|
| CO | IMA (0,1,8) |
| PM | ARMA (2,0,2) |
| NO | IMA (0,1,15) |
| NO2 | ARIMA (1,1,14) |
| NOX | IMA (0,1,14) |
| O3 | IMA (0,1,11) |
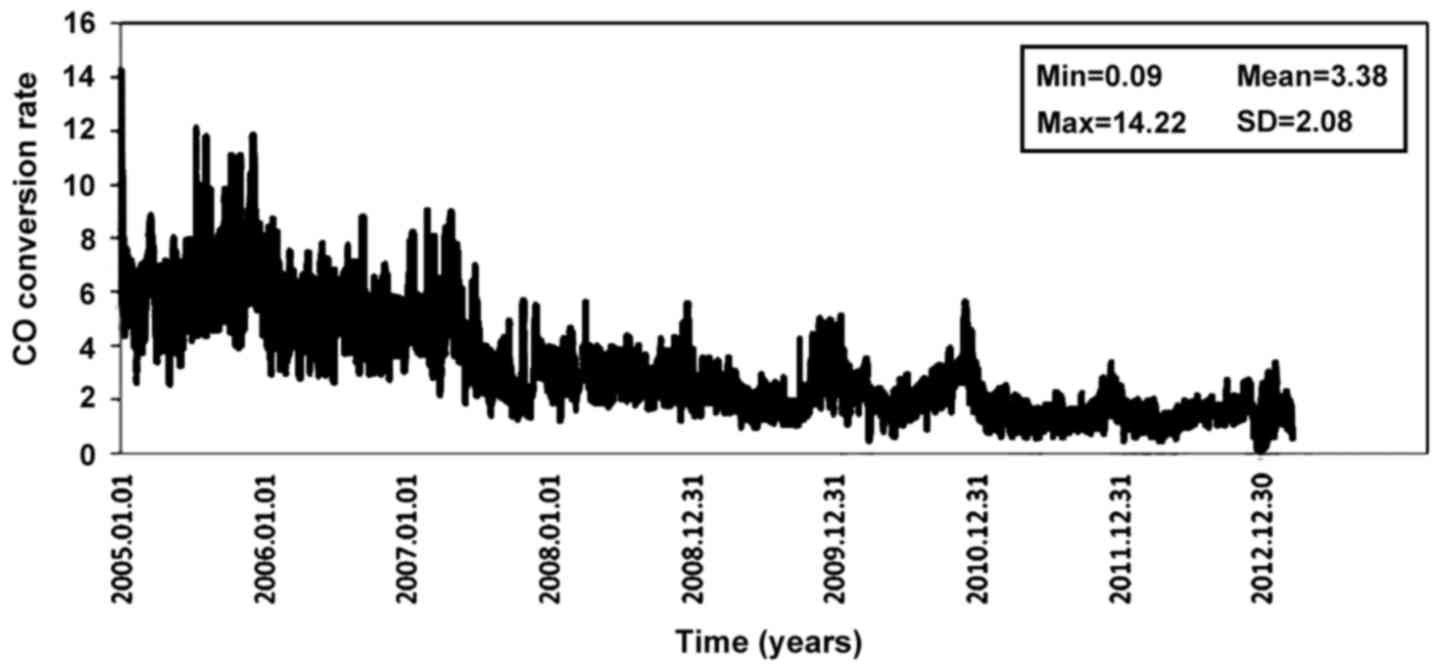
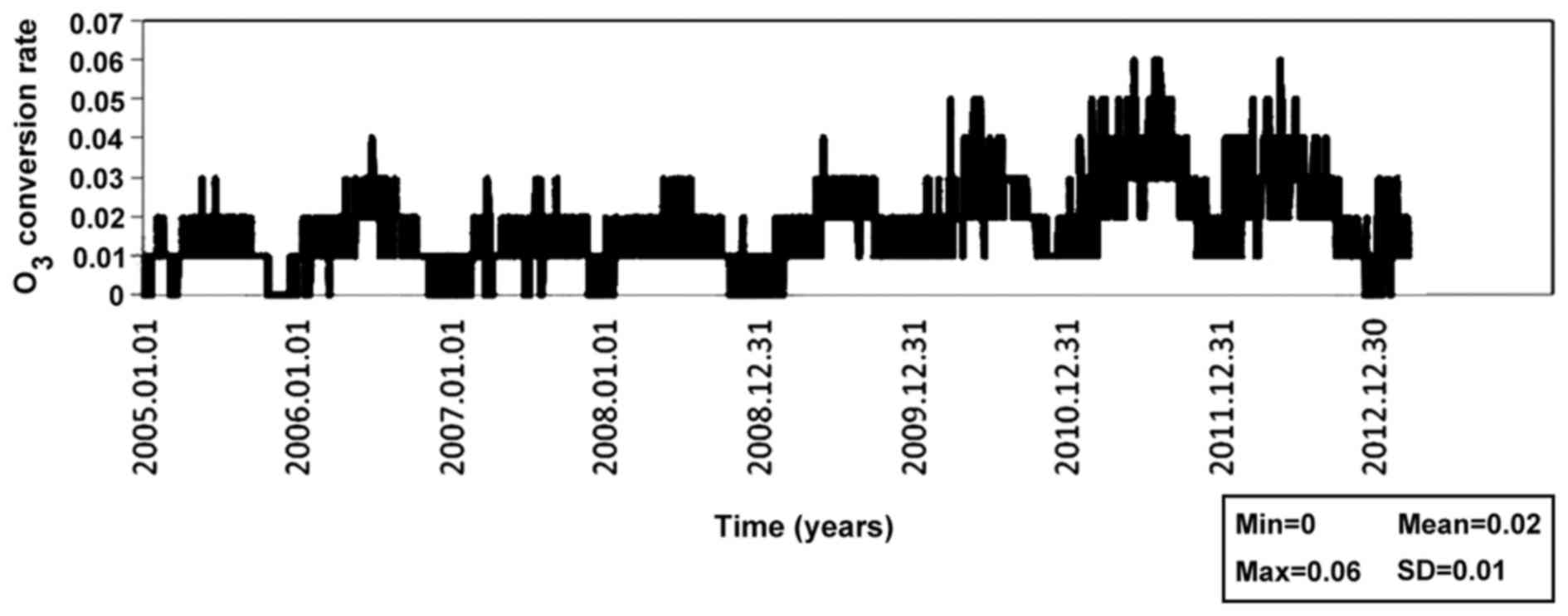
Figs. 1–6 show variations in time of air
pollutants more significantly for some studied substancies. As
shown in figures, concentrations of CO, NO, NO2 and
NOX decreased during the present study, while
O3 concentration increased. There was a periodic
alteration of the CO, NO and NOX concentrations. Peak of
pollutant concentrations was in the tenth month of each year. An
extreme reduction occurred in subsequent six months. The trend of
O3 concentration was quite reverse compared to the other
pollutants, with peak of concentrations in the warmer months.
Indeed, no specific pattern was observed for NO2
concentrations.
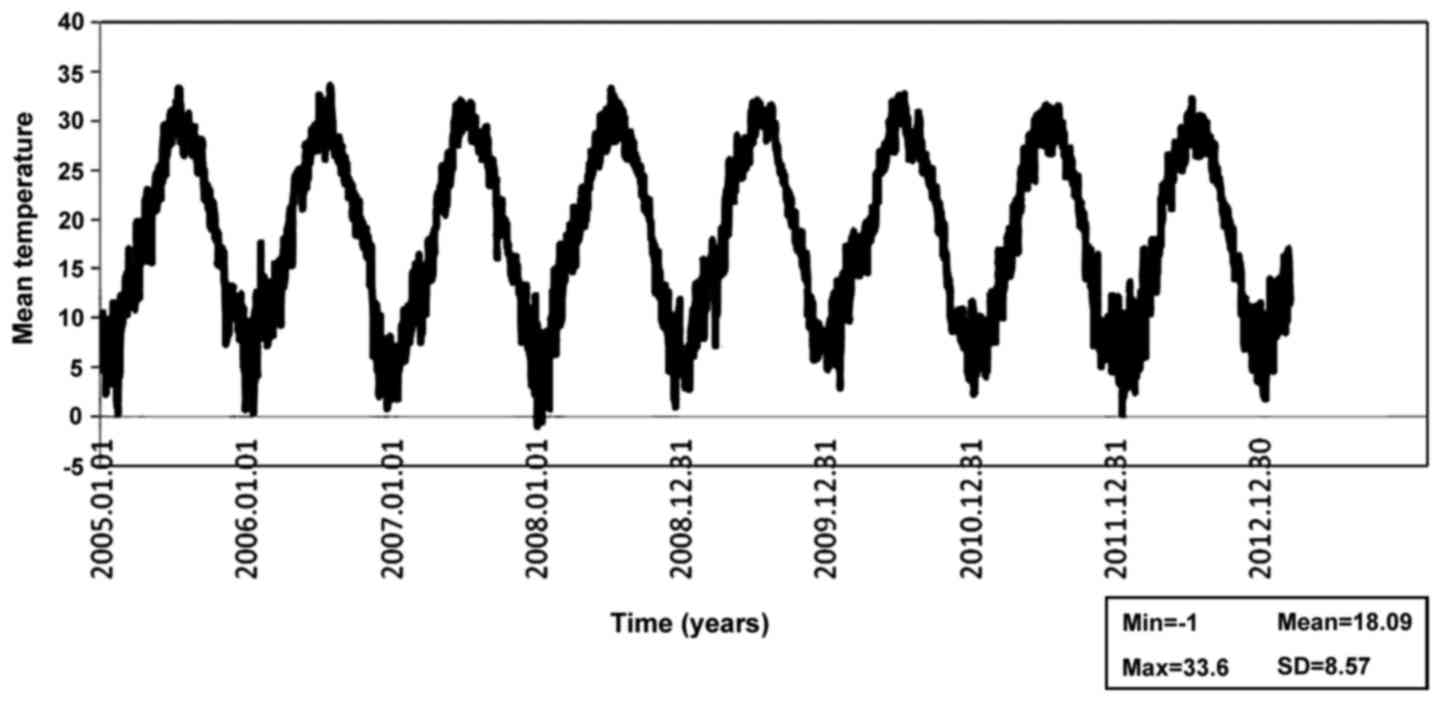
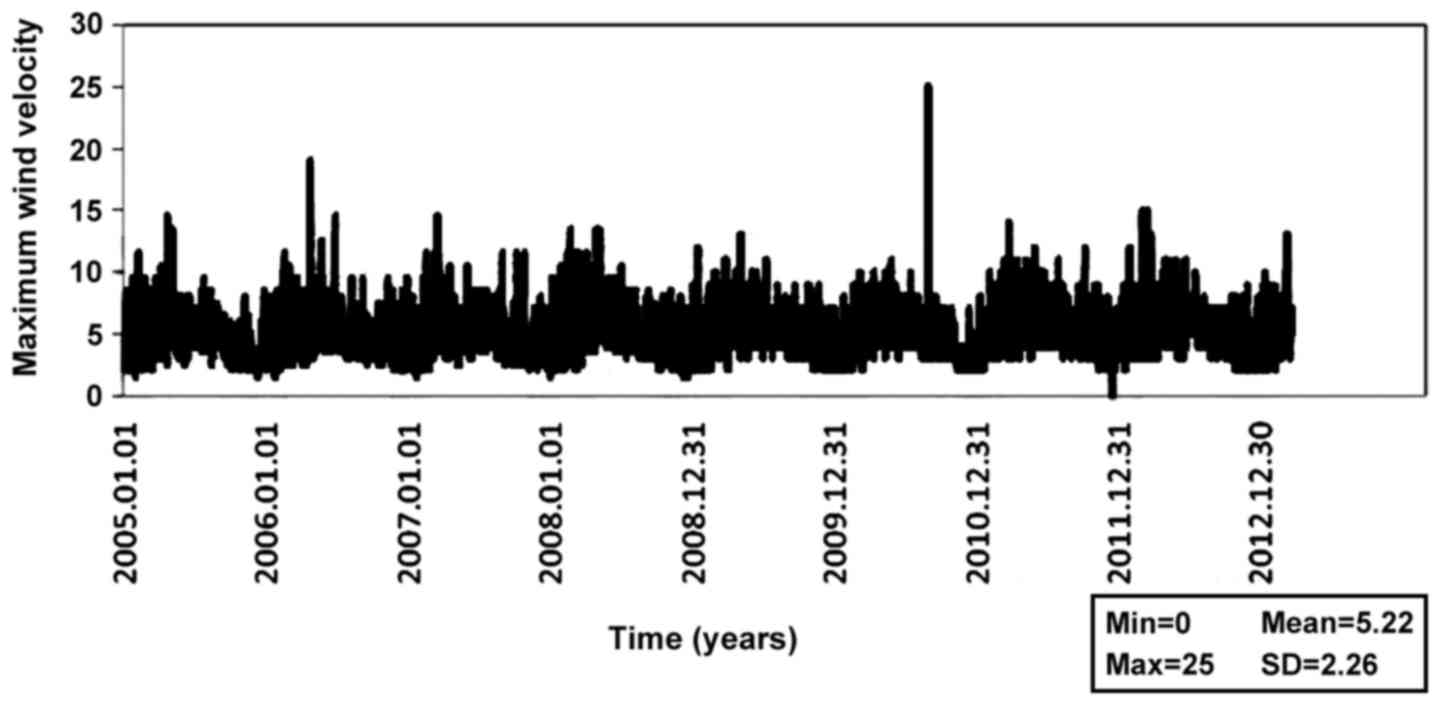
Figs. 7–9 show variation in time of weather
conditions. Annually, highest rainfall level, the lowest
temperature and the lowest wind speed occurred in the tenth month
of each year. The lowest rainfall and the maximum temperature were
observed approximately six months later.
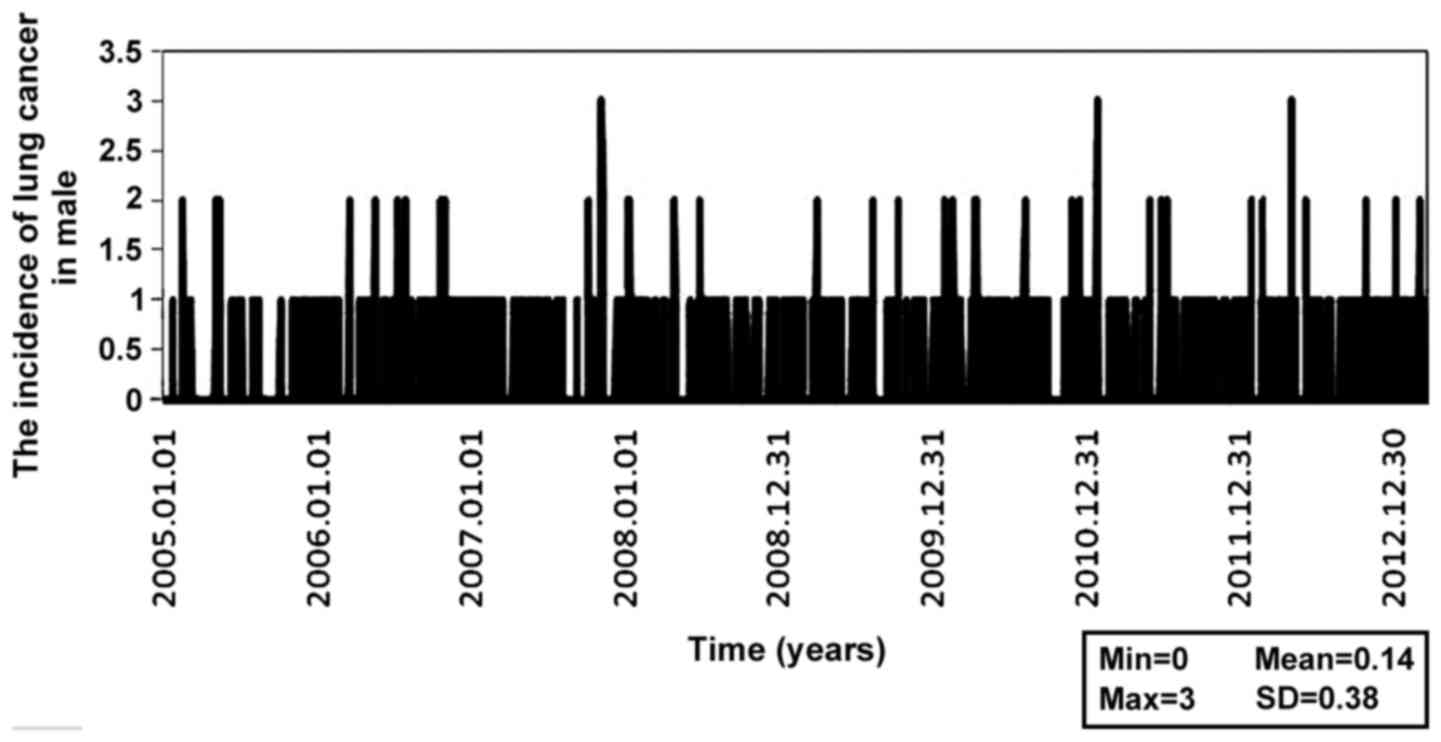
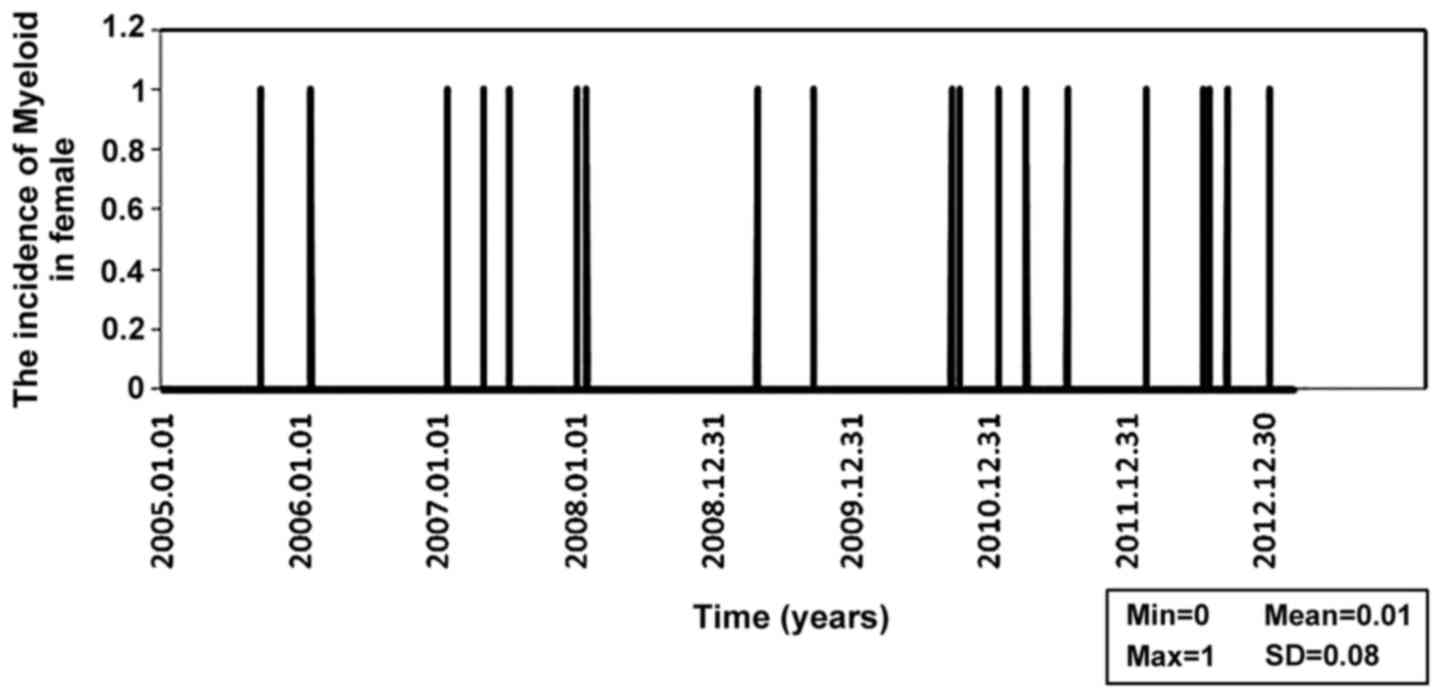
Figs. 10–15 show the number of different cancer
cases in the studied period. The above figures indicate that none
of diseases follows a specific pattern. Also, average temperatures
and precipitations level have no relationship with concentrations
of CO. Instead, we observed the following relationships: i) both
maximum wind speed and NO2 concentration have a weak but
significant inverse linear relationship with lung cancer in men
(P<0.001 and r<-0.079); ii) in the total population, lung
cancer has a weak but significant inverse linear relationship with
the maximum wind speed and NO2 concentration (P<0.001
and r<-0.085); iii) lymphatic cancer in women has a weak but
significant inverse linear relationship with concentration of
NO2 (P<0.001 and r<-0.052); iv) myeloid cancer in
men has a weak but significant inverse linear relationship with
NO2 concentration (P<0.001 and r<-0.043); v)
lymphoid cancer in men and women has a weak but significant inverse
linear relationship with concentration of NO2
(P<0.001 and r<-0.042); and vi) total cancers have a weak but
significant inverse linear relationship with the maximum wind speed
and NO2 concentration (P<0.001 and r<-0.092).
Generally, it seems that concentration of
NO2 in Shiraz has a weak and inverse relationship with
the mortality rate of lung and lymph node cancers. Furthermore, in
some cases the maximum wind speed has the same relationship with
mortality of lung and lymph node cancers.
According to our statistical analysis, it seems
there is a weak relationship between the pollutant levels and the
above mortality.
Discussion
The results of the present study indicated that the
number of deaths due to lung cancer and leukemia had a weak but
significant relationship (P<0.05) with the concentration of
NO2 and CO in the air.
Wong et al studied (5) epidemiological and experimental issues
relating to genotoxic effects of air pollution and DNA reporting
that due to the increasing number cases of lung cancer, it would be
essential that governments pay special attention to all preventive
measures to reduce air pollution, to develop clean energy programs,
and to improve research on investigation of carcinogenesis effects
of air pollution.
Study of Chalbot et al on PM2.5 in
USA in 2014 showed that implementation of law and air pollution
regulations had major effects even in areas with high main risk
factors of mortality as obesity and smoking (21).
Pope et al revealed prolonged contact with
fine particles by combustion was related to lung cancer and
cardiovascular disease (13).
Vineis and Husgafvel-Pursiainen demonstrated that air pollution
increased lung cancer, especially in combination with some other
known risk factors such as smoking, passive cigarette smoke, and
occupational exposures. The present study also showed that organic
air pollutants, especially PAH compounds, had genotoxic and
oxidative effects on DNA (12).
Gilliland et al proclaimed that short-term
changes in the amount of O3 caused respiratory diseases
that led to absence of 10-12-year-old children from school.
Therefore, adverse effect of O3 on children's health has
been established (11). Previous
studies carried out in Tehran city also showed that CO,
SO2 and NO2 were the most important causes of
deaths due to heart disease (7).
Masjedi et al showed the concentrations of SO2
and NO2 had a significant correlation with asthma
attacks in Tehran (22).
Previous studies in Ahwaz city carried out by Zolghi
et al, using appropriate models, indicated that the
percentage of deaths due to air suspending PM10 measured
in 2010 was 17.5% which was 5.5% higher than the preceding year
(23). Research in Australia,
revealed that the most important reasons for hospital emergency
admissions for respiratory disease were PM10 such as
ozone concentrations (24).
The study of Lewis et al also showed the
major reasons of hospital admission of children were asthma attacks
due to high concentrations of PM2.5 and ozone (25).
Moreover, Italian studies reported significant
correlation between air pollution in urban area and risk of
childhood leukemia (26,27).
However, the present study is unique as it shows the
correlation among factors such as air pollutants, local
meteorological conditions, and mortality rate due to cancer in
Shiraz and help local authorities, politicians and all those
involved in this topic to pay special attention to these issues and
to control sources of air pollution such as industries and
transport systems and to standardize use of fuels. Therefore,
special attention should be paid to sources of these pollutants and
we need better management to decrease air pollutant concentrations
through, e.g., using clean energy in respect to fossil fuels,
better managing of urban traffic planning, improved public
transport service and car sharing.
Acknowledgements
The authors would like to thank the Deputy of
Research and Technology of Shiraz University of Medical Sciences
for their financial support of this project no. 9301218095.
References
|
1
|
Wong MC, Tam WW, Wang HH, Lao XQ, Zhang
DD, Chan SW, Kwan MW, Fan CK, Cheung CS, Tong EL, et al: Exposure
to air pollutants and mortality in hypertensive patients according
to demography: A 10 year case-crossover study. Environ Pollut.
192:179–185. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
EPA: Criteria Air Pollutants. NAAQS Table.
https://www.epa.gov/criteria-air-pollutants/naaqs-tableAccessed.
January 9–2017.
|
|
3
|
Conti Oliveri G, Heibati B, Kloog I, Fiore
M and Ferrante M: A review of AirQ models and their applications
for forecasting the air pollution health outcomes. Environ Sci
Pollut Res Int. 2017.https://doi.org/10.1007/s11356-016-8180-1PubMed/NCBI
|
|
4
|
Cohen AJ: Outdoor air pollution and lung
cancer. Environ Health Perspect. 108:(Suppl 4). 743–750. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wong IC, Ng YK and Lui VW: Cancers of the
lung, head and neck on the rise: Perspectives on the genotoxicity
of air pollution. Chin J Cancer. 33:476–480. 2014.PubMed/NCBI
|
|
6
|
Calderón-Garcidueñas L, Azzarelli B, Acuna
H, Garcia R, Gambling TM, Osnaya N, Monroy S, DEL Tizapantzi MR,
Carson JL, Villarreal-Calderon A and Rewcastle B: Air pollution and
brain damage. Toxicol Pathol. 30:373–389. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Henriksson J and Tjälve H: Manganese taken
up into the CNS via the olfactory pathway in rats affects
astrocytes. Toxicol Sci. 55:392–398. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Morgan KT and Monticello TM: Airflow, gas
deposition, and lesion distribution in the nasal passages. Environ
Health Perspect. 85:209–218. 1990. View
Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nakashima T, Tanaka M, Inamitsu M and
Uemura T: Immunohistopathology of variations of human olfactory
mucosa. Eur Arch Otorhinolaryngol. 248:370–375. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Paik SI, Lehman MN, Seiden AM, Duncan HJ
and Smith DV: Human olfactory biopsy. The influence of age and
receptor distribution. Arch Otolaryngol Head Neck Surg.
118:731–738. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gilliland FD, Berhane K, Rappaport EB,
Thomas DC, Avol E, Gauderman WJ, London SJ, Margolis HG, McConnell
R, Islam KT and Peters JM: The effects of ambient air pollution on
school absenteeism due to respiratory illnesses. Epidemiology.
12:43–54. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Vineis P and Husgafvel-Pursiainen K: Air
pollution and cancer: Biomarker studies in human populations.
Carcinogenesis. 26:1846–1855. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Pope CA III, Burnett RT, Thun MJ, Calle
EE, Krewski D, Ito K and Thurston GD: Lung cancer, cardiopulmonary
mortality, and long-term exposure to fine particulate air
pollution. JAMA. 287:1132–1141. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pope CA III, Thun MJ, Namboodiri MM,
Dockery DW, Evans JS, Speizer FE and Heath CW Jr: Particulate air
pollution as a predictor of mortality in a prospective study of US
adults. Am J Respir Crit Care Med. 151:669–74. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kloog I, Coull BA, Zanobetti A, Koutrakis
P and Schwartz JD: Acute and chronic effects of particles on
hospital admissions in New-England. PLoS One. 7:e346642012.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zanobetti A, Redline S, Schwartz J, Rosen
D, Patel S, O'Connor GT, Lebowitz M, Coull BA and Gold DR:
Associations of PM10 with sleep and sleep-disordered
breathing in adults from seven U.S. urban areas. Am J Respir Crit
Care Med. 182:819–825. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rice MB, Rifas-Shiman SL, Litonjua AA,
Oken E, Gillman MW, Kloog I, Luttmann-Gibson H, Zanobetti A, Coull
BA, Schwartz J, Koutrakis P, Mittleman MA and Gold DR: Lifetime
exposure to ambient pollution and lung function in children. Am J
Respir Crit Care Med. 193:881–888. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Calderón-Garcidueñas L, Mora-Tiscareño A,
Ontiveros E, Gómez-Garza G, Barragán-Mejía G, Broadway J, Chapman
S, Valencia-Salazar G, Jewells V, Maronpot RR, et al: Air
pollution, cognitive deficits and brain abnormalities: A pilot
study with children and dogs. Brain Cogn. 68:117–127. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Miri M, Derakhshan Z, Allahabadi A, Ahmadi
E, Conti Oliveri G, Ferrante M and Aval HE: Mortality and morbidity
due to exposure to outdoor air pollution in Mashhad metropolis,
Iran. The AirQ model approach. Environ Res. 151:451–457. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Calderón-Garcidueñas L, Engle R,
Mora-Tiscareño A, Styner M, Gómez-Garza G, Zhu H, Jewells V,
Torres-Jardón R, Romero L, Monroy-Acosta ME, et al: Exposure to
severe urban air pollution influences cognitive outcomes, brain
volume and systemic inflammation in clinically healthy children.
Brain Cogn. 77:345–355. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chalbot MC, Jones TA and Kavouras IG:
Trends of non-accidental, cardiovascular, stroke and lung cancer
mortality in Arkansas are associated with ambient PM2.5
reductions. Int J Environ Res Public Health. 11:7442–7455. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Masjedi MR, Jamaati HR, Dokouhaki P,
Ahmadzadeh Z, Taheri SA, Bigdeli M, Izadi S, Rostamian A, Aagin K
and Ghavam SM: The effects of air pollution on acute respiratory
conditions. Respirology. 8:213–230. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zolghi E, Godarzi Gh, Gravandi S, Mohamadi
M, Vosoghi Nayeri M, Visi E, et al: Estimate of cardiovascular and
respiratory diseases related to particle matter pollutant in Tabriz
air, northwest of Iran, 2011. J Ilam Univ Med Sci. 22:84–91.
2014.
|
|
24
|
Petroeschevsky A, Simpson RW, Thalib L and
Rutherford S: Associations between outdoor air pollution and
hospital admissions in Brisbane, Australia. Arch Environ Health.
56:37–52. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lewis TC, Robins TG, Mentz GB, Zhang X,
Mukherjee B, Lin X, Keeler GJ, Dvonch JT, Yip FY, O'Neill MS, et
al: Air pollution and respiratory symptoms among children with
asthma: Vulnerability by corticosteroid use and residence area. Sci
Total Environ. 448:48–55. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Malagoli C, Malavolti M, Costanzini S,
Fabbri S, Tezzi S, Palazzi G, Arcolin E and Vinceti M: Increased
incidence of childhood leukemia in urban areas: A population-based
case-control study. Epidemiol Prev. 39:102–107. 2015.PubMed/NCBI
|
|
27
|
Filippini T, Heck JE, Malagoli C, Del
Giovane C and Vinceti M: A review and meta-analysis of outdoor air
pollution and risk of childhood leukemia. J Environ Sci Health C
Environ Carcinog Ecotoxicol Rev. 33:36–66. 2015. View Article : Google Scholar : PubMed/NCBI
|