Introduction
Isodicentric Y chromosomes, containing two
centromeres and two symmetrically identical arms, are recognized as
the most common structural abnormalities of the human Y chromosome
(1). Due to the instability of
isodicentric chromosomes during cell division, different
proportions of chromosomal mosaics will usually occur, ordinarily
in association with a 45,X cell line (2,3).
These mosaic karyotypes can exhibit various clinical
manifestations, ranging from females with Turner symptoms to males
with spermatogenic failure (4–7).
Small supernumerary marker chromosomes (sSMCs),
smaller than, or equal in size to, chromosome 20, are structurally
abnormal chromosomes which cannot be usually identified through the
conventional banding technique (8). The incidence rate in the general
population is ~0.03–0.05%; however, in patients with fertility
problems, the rate of sSMCs is increased to 0.125%, and the
frequency of sSMC carriers is increased in males compared with
females (0.165% vs. 0.022%) (8,9).
sSMCs are usually derived from chromosome 15, i(12p), der(22), inv
dup (22), and i(18p) (10). Although the karyotype/phenotype
relationship between sSMCs and male infertility remains to be
elucidated, a previous study demonstrated that spermatogenesis
failure, for example oligoasthenozoospermia, may be associated with
the presence of sSMCs (11).
For marker chromosomes without any harbored
repetitive α-satellite (or alphoid) DNA, these uncommon marker
chromosomes are described as neocentric marker chromosomes, in
which the newly derived centromeres (termed neocentromeres) can
form functional kinetochores and maintain mitotic stability of the
chromosome (12,13). It has been reported that neocentric
marker chromosomes are formed when acentric chromosomal fragments
are rescued through the formation of neocentromeres (12). Currently, more than 100 cases of
sSMC with neocentromeres have been reported in literature; however,
cases of neocentromeres deriving from the Y chromosome are rare,
which has led to the failure in establishing karyotype/phenotype
relationships (14–16).
In general, the concrete constitution and origins of
the sSMC or neocentric marker chromosome were associated with
clinic phenotypic diversity, ranging from normal to severely
abnormal (8). The combined
application of molecular techniques could offer increasingly
reliable references for genetic counseling and therapeutic strategy
in clinics (9,10). The present study described a case
presenting a neocentric isochromosome Yp, neo(Yp), and an
isodicentric Yq, idic(Yq), in an azoospermic male using a
combination of G-banding, chromosome microarray analysis (CMA), and
fluorescence in situ hybridization (FISH) analysis.
Materials and methods
Patient
A 27-year-old Chinese male accepted infertility
consultation in The Center for Reproductive Medicine and Center for
Prenatal Diagnosis at The First Hospital of Jilin University after
1 year of regular unprotected coitus and no pregnancy in June,
2015. The patient's height and weight were 176 cm and 80 kg,
respectively. His penis development and growth were normal, and
testicular volume was ~4 and ~6 ml for the left and right testes,
respectively. No other physical abnormalities were observed. A
series of routine examinations were conducted. Semen analysis and
levels of sex hormones are presented in Table I. The male was eventually diagnosed
with azoospermia according to routine semen examination (17). The Ethics Committee of the First
Hospital of Jilin University approved the study protocol (permit
no. 2016-416), and the patient provided written informed consent
and agreed to participate in this study.
 | Table I.Semen analysis and levels of sex
hormones. |
Table I.
Semen analysis and levels of sex
hormones.
| Hormone | Results | Reference
range |
|---|
| FSH, mIU/ml | 10.00 | 1.5–12.4 |
| LH, mIU/ml | 12.40 | 1.7–8.5 |
| E2, pg/ml | 24.59 | 28–248 |
| PRL, uIU/ml | 287.00 | 86–258 |
| T, nmol/l | 6.60 | 9.9–27.8 |
| Semen volume,
ml | 2.0 | 1.5–5.5 |
| Sperm count,
million/ml | 0 | >20 |
Karyotype analysis
For the patient, a karyotype analysis of peripheral
blood lymphocytes was conducted: Peripheral blood (0.5 ml) was
cultured in lymphocyte culture medium containing 30 U/ml heparin
for 72 h at 37°C (Yishengjun; Baidi Biotechnology) and subsequently
treated with 50 µg/ml colchicine (Yishengjun; Baidi Biotechnology)
1 h before culture termination to arrest mitoses. The lymphocytes
were hypotonically treated in 0.075 M KCl for 20 min at 37°C and
fixed in methanol:acetic acid (3:1) for 10 min at room temperature,
G-banding of metaphase chromosomes and chromosomal karyotype
analysis were performed according to a previous study (18). The karyotype was described
according to the International System for Human Cytogenetic
Nomenclature 2016 (19).
CMA analysis
Following written consent from the patient, 5 ml
peripheral blood was collected from the patient using a standard
vacuum extraction blood-collecting system containing EDTA and
heparin. Genomic DNA was isolated from whole blood using a QIAamp
DNA Mini kit (Qiagen GmbH) according to the manufacturer's
protocol. CMA was performed using a CytoScan 750K array
(Affymetrix; Thermo Fisher Scientific, Inc.), according to the
manufacturer's protocol. The procedure included genomic DNA
extraction, digestion and ligation, PCR amplification, PCR product
purification, quantification and fragmentation, labeling, array
hybridization, washing and scanning. In the PCR amplification
process, 250 ng DNA samples was digested with Nsp1, amplified with
TITANIUM Taq DNA polymerase (cat. no. 190118EA; Clontech
Laboratories, Inc.), fragmented with Affymetrix fragmentation
reagent, and labeled with biotin end-labeled nucleotides. PCR was
performed using a Veriti Thermal Cycler 96-well, Alpha-SE (Applied
Biosystems; Thermo Fisher Scientific, Inc.). The thermocycling
conditions consisted of an initial denaturation step of 3 min at
94°C, followed by 30 cycles of 30 sec at 94°C, 45 sec at 60°C, and
15 sec at 68°C, with a final extension step at 68°C for 7 min. The
platform used included 550,000 nonpolymorphic probes and 200,436
single nucleotide polymorphic probes. Thresholds for genome-wide
screening were set at ≥200 kb for gains and ≥100 kb for losses. The
detected copy number variations were comprehensively estimated by
comparing them with published literature and public databases,
including Database of Genomic Variants (DGV; http://dgv.tcag.ca/dgv/app/home), DECIPHR v9.28
(http://decipher.sanger.ac.uk/), ISCA
(https://www.iscaconsortium.org/),
ECARUCA (http://www.ecaruca.net), and OMIM
(http://www.ncbi.nlm.nih.gov/omim).
FISH
Based upon the karyotype analysis and CMA results,
FISH analysis was carried out to further confirm the
characterization of chromosomal Y anomalies. Two sets of probes
were used according to the manufacturers' instructions in the
present study: Centromere probes specific for chromosomes X, Y
(cat. no. F01001, CSPX, spectrum green; CSPY, spectrum red; Beijing
GP Medical Technologies, Ltd.) and SRY probe (cat. no. RU-LPU026;
Cytocell). The SRY probes, labelled in red, consists of two
non-overlapping probes, 30 and 50 kb. The probes cover the entire
SRY gene and flanking DNA, including the RPS4Y1 gene. The probe mix
also contains control probes for the X centromere (DXZ1), labelled
in blue, and for chromosome Y (DYZ1, the heterochromaticblock at
Yq12), labelled in green. Lymphocytes cell suspensions fixed with
methanol:acetic acid (3:1) for the karyotype analysis were further
used for FISH analysis. The cell suspensions were centrifuged (931
× g for 5 min) at 4°C, then were dropped onto dry glass slides
(Shitai; Citotest Labware Manufacturing Co., Ltd.) using a dropper.
The procedure of slide preparation (including probe application,
co-denaturation, hybridization and post-hybridization washes) was
performed according to the manufacturer's instructions. The probes
were denatured for 2 min at 75°C. The hybridization mixture (1 µl
each probe and 7 µl hybridization solution) was applied to each
slide and covered with a coverslip 20×20 mm. Then, the slides were
sealed with rubber cement before hybridization was carried out
overnight in a moist chamber at 37°C. After hybridization, the
slides were washed for 2 min in a solution of 0.4X SSC at 72°C and
a second time for 30 sec in a solution of 2X SSC, 0.05% Tween-20 at
room temperature. Following the final wash, slides were air dried
and counterstained with a solution of 4′,6′-DAPI in the dark at 4°C
overnight. Appropriate viewing, analysis and imaging of FISH
results was accomplished using a fluorescent microscope (Leica
DM4000B; Leica Microsystems GmbH; magnification, ×1,000).
Azoospermia factor (AZF) microdeletion
analysis
Microdeletions in the AZF region were detected using
PCR, as previously described in accordance with the recommendations
of The European Academy of Andrology and the European Molecular
Genetics Quality Network. Specific sequence-tagged sites were
mapped in the AZF region, including SY84 and SY86 for AZFa; SY27,
SY134, and SY143 for AZFb; SY157, SY254, and SY255 for AZFc; and
SY152 for AZFd. Human zinc-finger protein-encoding genes (ZFX/ZFY)
located on the X and Y chromosomes were selected as internal
control primers (20). Genomic DNA
was isolated with the Tiangen Blood DNA Extraction Mini kit
(Tiangen Biotech Co., Ltd.) using peripheral blood lymphocytes
according to the manufacturer's protocol. The PCR process was
performed according to a previous study, and primer sequences are
presented in Table II (21). Each 20 ml reaction mix contained 50
ng genomic DNA, 5–10 pmol of each primer (Shanghai Sangon
Pharmaceutical Co., Ltd.), 100 mM potassium chloride, 200 mM
Tris-HCl (pH 8.8), 15 mM magnesium chloride, 1% Triton X-100, 500
mM of each dNTP and 2 U Taq polymerase (Beijing Dingguo Changsheng
Biotechnology Co., Ltd.). Multiplex PCR was carried out using a
Veriti 96-well PCR thermal cycler (Applied Biosystems; Thermo
Fisher Scientific, Inc.). The cycling program involved preliminary
denaturation at 94°C for 6 min, followed by 35 cycles of
denaturation at 95°C for 40 sec, annealing at 58°C for 45 sec, and
elongation at 72°C for 60 sec, followed by a final elongation step
at 72°C for 10 min. Classical AZF reaction products were analyzed
by electrophoresis in 1.5% agarose gels at 80 V for 30 min
(Biowest). All gels contained 0.5 mg/ml ethidium bromide and PCR
products were visualized under ultraviolet light.
| Table II.Primer sequences used in polymerase
chain reaction analysis of sequence-tagged sites for the
azoospermia factor region of the human Y chromosome. |
Table II.
Primer sequences used in polymerase
chain reaction analysis of sequence-tagged sites for the
azoospermia factor region of the human Y chromosome.
| STS | Primer
sequences | Product size
(bp) |
|---|
| ZFX/Y | Forward:
5′-ACCR(A,G)CTGTACTGACTGTGATTACAC-3′ |
|
|
| Reverse:
5′-GCACY(C,T)TCTTTGGTATCY(C,T)GAGAAAGT-3′ | 495 |
| SY14(SRY) | Forward:
5′-GAATATTCCCGCTCTCCGGA-3′ |
|
|
| Reverse:
5′-GCTGGTGCTCCATTCTTGAG-3′ | 472 |
| SY84 | Forward:
5′-AGAAGGGTCTGAAAGCAGGT-3′ |
|
|
| Reverse:
5′-GCCTACTACCTGGAGGCTTC-3′ | 326 |
| SY86 | Forward:
5′-GTGACACACAGACTATGCTTC-3′ |
|
|
| Reverse:
5′-ACACACAGAGGGACAACCCT-3′ | 320 |
| SY127 | Forward:
5′-GGCTCACAAACGAAAAGAAA-3′ |
|
|
| Reverse:
5′-CTGCAGGCAGTAATAAGGGA-3′ | 274 |
| SY134 | Forward:
5′-GTCTGCCTCACCATAAAACG-3′ |
|
|
| Reverse:
5′-ACCACTGCCAAAACTTTCAA-3′ | 301 |
| SY143 | Forward:
5′-GCAGGATGAGAAGCAGGTAG-3′ |
|
|
| Reverse:
5′-CCGTGTGCTGGAGACTAATC-3′ | 311 |
| SY152 | Forward:
5′-AAGACAGTCTGCCATGTTTCA-3′ |
|
|
| Reverse:
5′-ACAGGAGGGTACTTAGCAGT-3′ | 125 |
| SY157 | Forward:
5′-CTTAGGAAAAAGTGAAGCCG-3′ |
|
|
| Reverse:
5′-CCTGCTGTCAGCAAGATACA-3′ | 285 |
| SY254 | Forward:
5′-GGGTGTTACCAGAAGGCAAA-3′ |
|
|
| Reverse:
5′-GAACCGTATCTACCAAAGCAGC-3′ | 380 |
| SY255 | Forward:
5′-GTTACAGGATTCGGCGTGAT-3′ |
|
|
| Reverse:
5′-CTCGTCATGTGCAGCCAC-3′ | 123 |
Selection of neocentric chromosome Y
cases
The present study focused on cases presenting
neocentric chromosome Y associated with different clinical
manifestations. Based upon this selection criterion, a systematic
literature search was conducted by means of a PubMed literature
search (https://www.ncbi.nlm.nih.gov/pubmed/) using relevant
terms and their combinations [including neo(Y), neocentric
chromosome Y, chromosomal Y neocentromere, neocentric marker
chromosome Y and marker chromosome Y neocentromere], and by
searching the sSMC database (http://ssmc-tl.com/sSMC.html) (22).
Results
Karyotype analysis
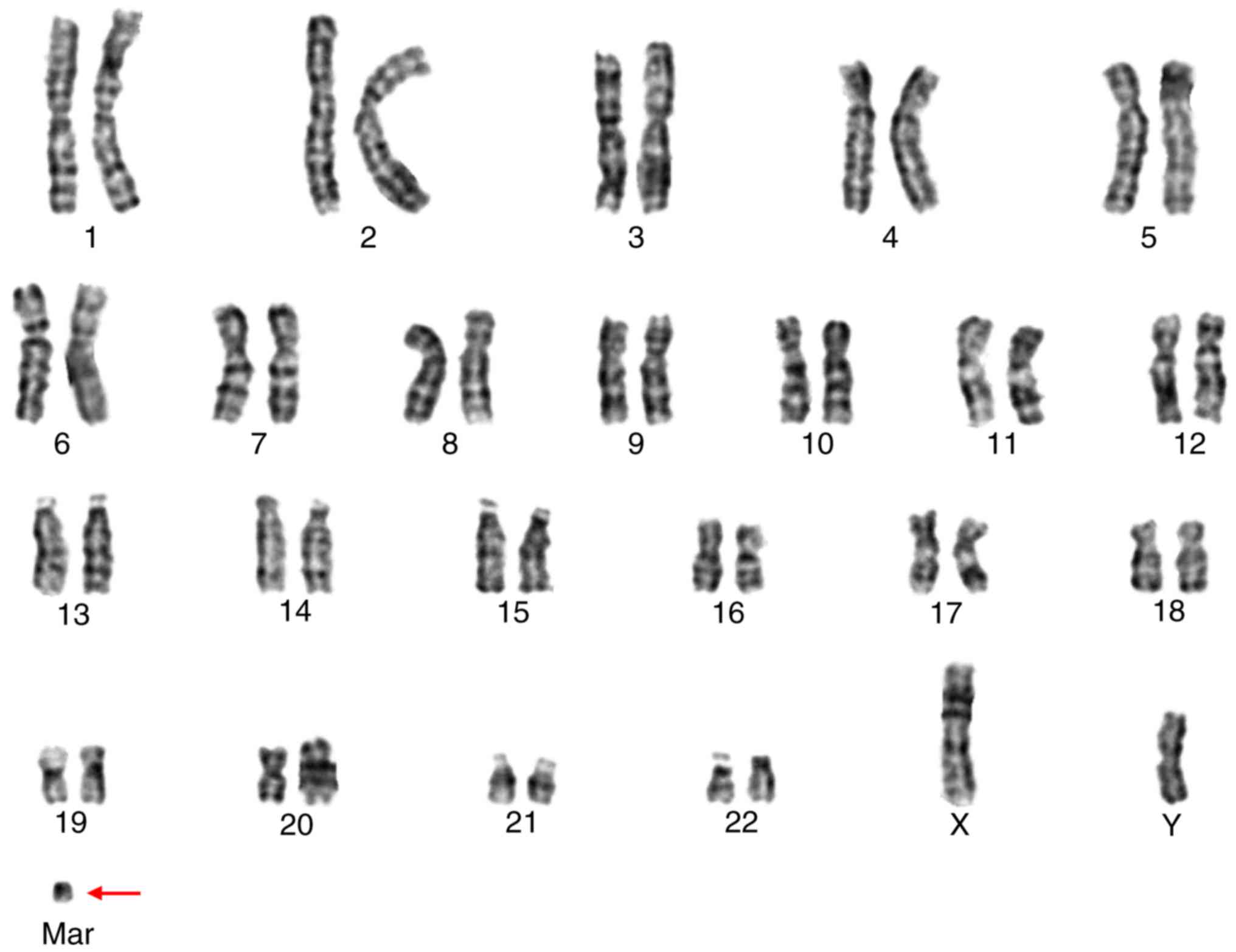
Cytogenetic G-banding analysis initially described
the karyotype as 47,X,i(Y)(q10),+mar (Fig. 1), consisting of an isochromosome Yq
[i(Yq)] and an sSMC.
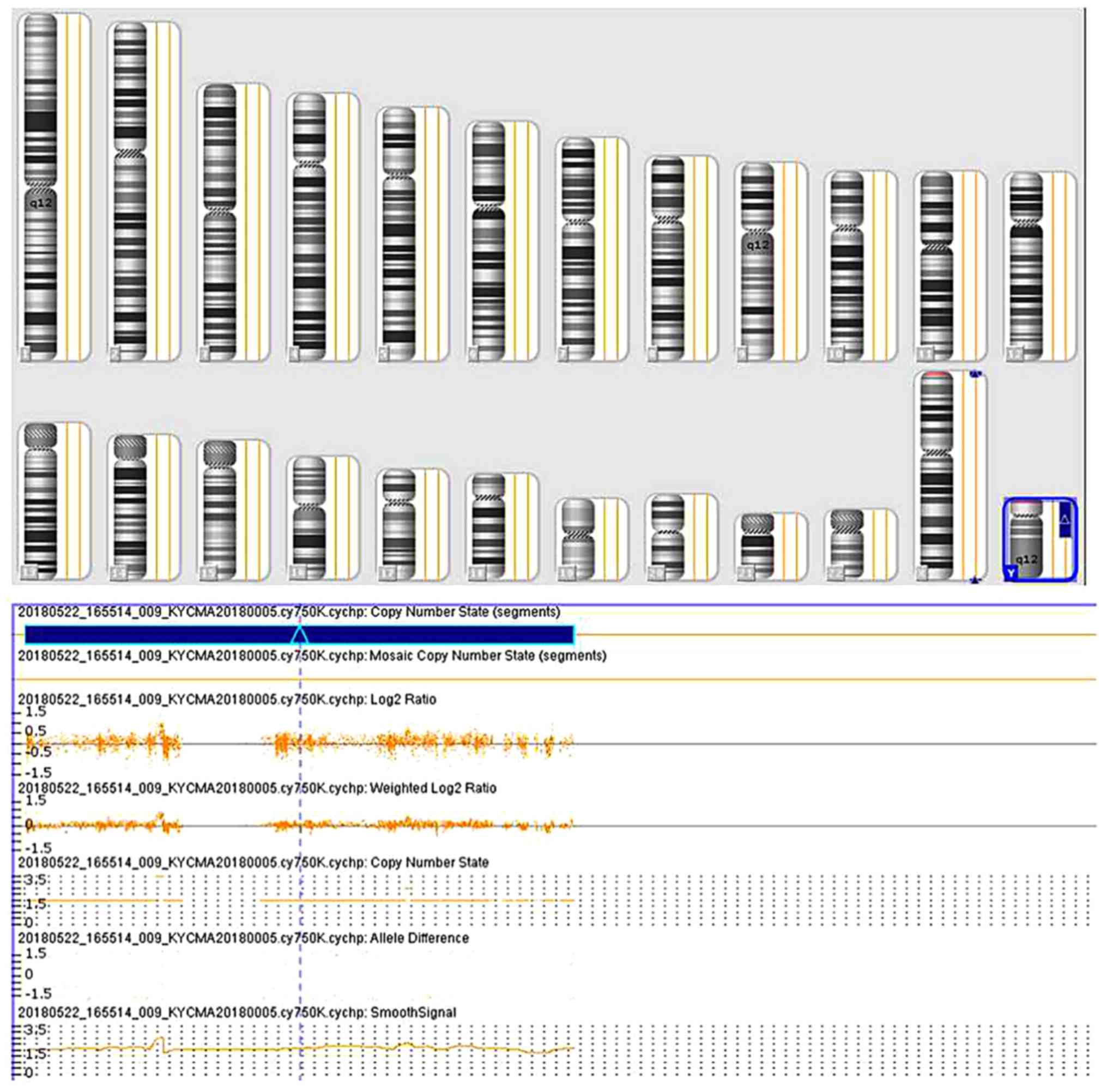
Molecular cytogenetic analysis
In order to delineate the origin of the marker
chromosome, CMA analysis was performed, describing the sSMC as
arr[hg19]Yp11.31q11.23(2,650,-424-28,799,654)×2 (Fig. 2), indicating that the patient had
an extra Y chromosome but that the karyotype was not 47,XYY. Based
on this, the karyotype was characterized as
47,X,i(Y)(p10),i(Y)(q10). The existence of two forms of the Y
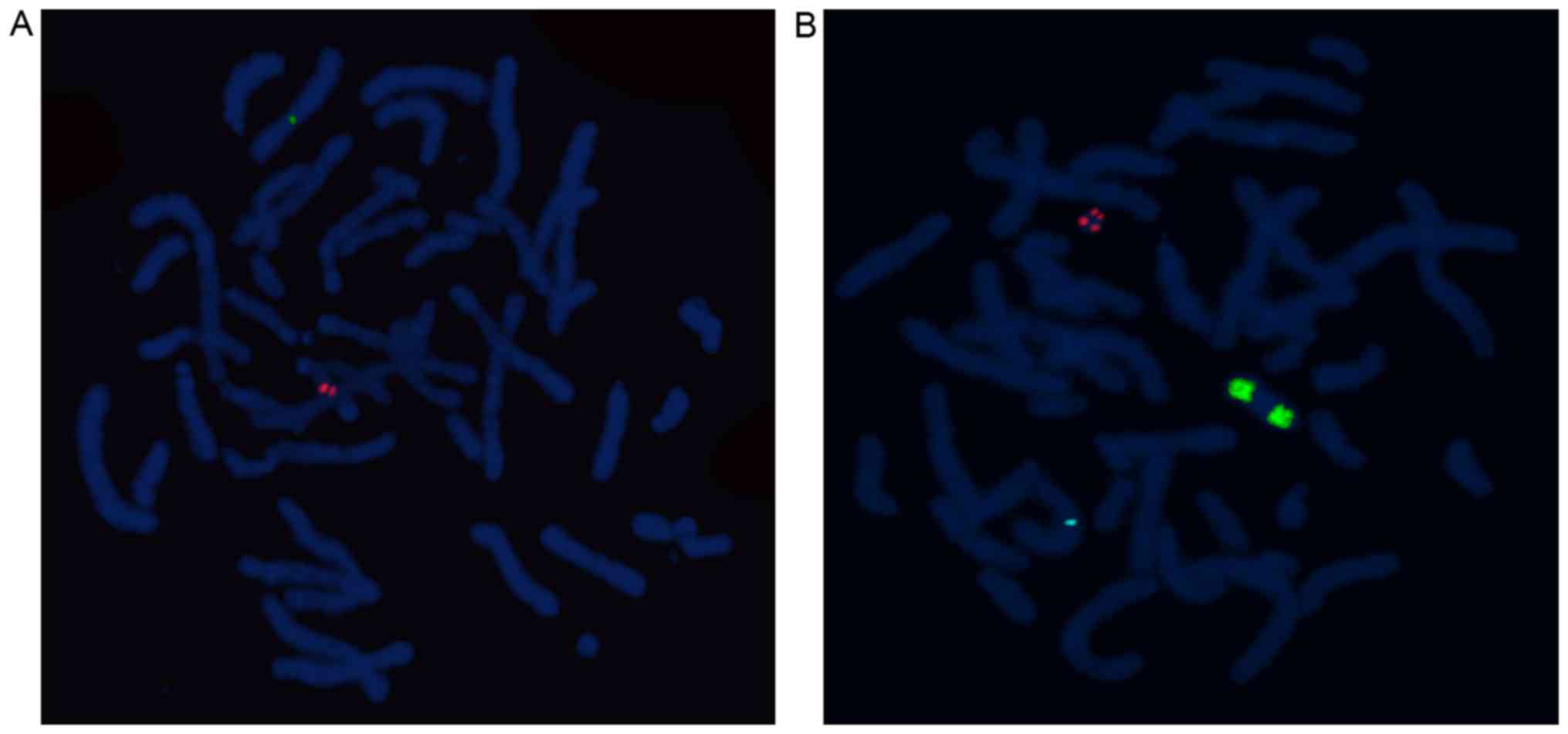
chromosome was further investigated with SRY and alphoid probes for
the Y centromere. FISH with centromere probes showed two close but
clearly distinct chromsomal Y centromere signals (red) in the
middle region of i(Yq) (Fig. 3A),
but no Y centromere signal was detected on the sSMC. Furthermore,
two DYZ1 signals (green) and no SRY signal indicated that i(Yq) was
actually an idic(Yq) (Fig. 3B).
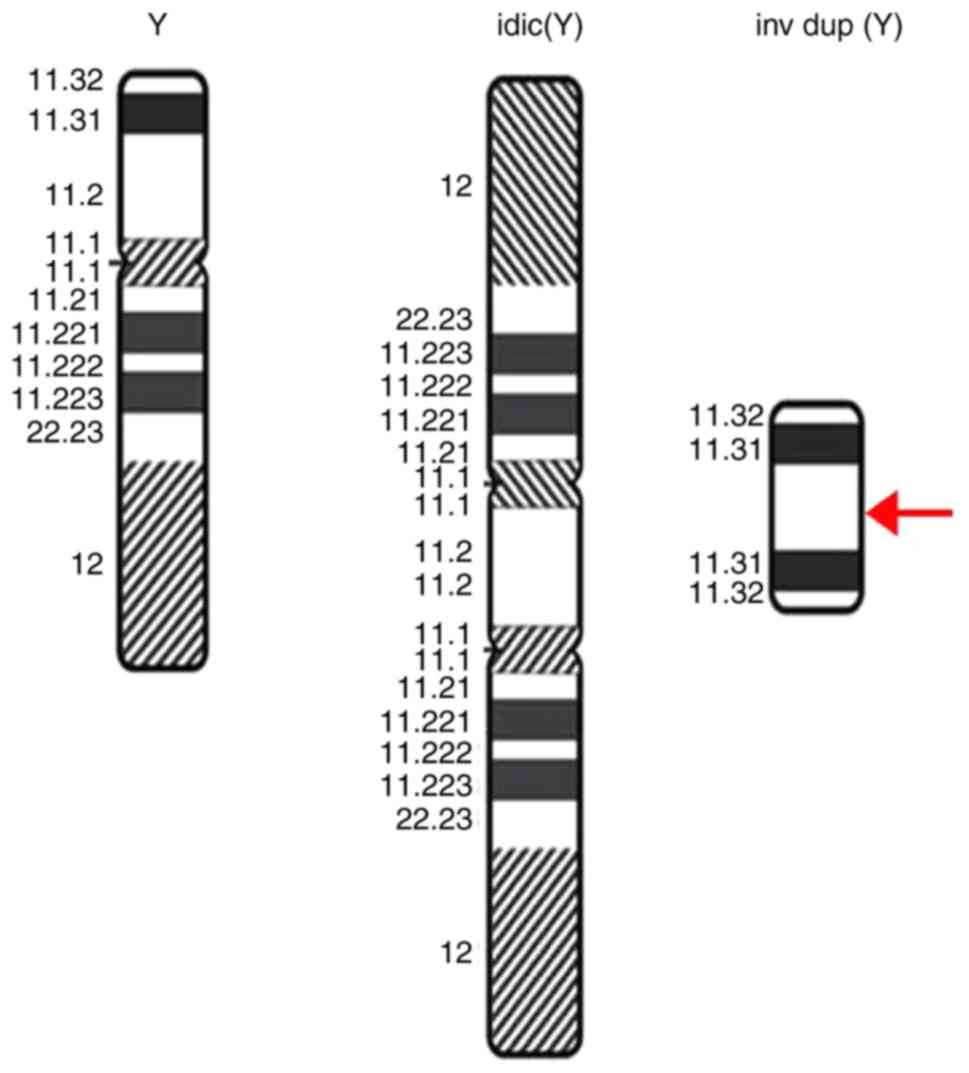
These results imply that two identical Y chromosomes, with
partially missing short arms, had integrated together symmetrically
(Fig. 4). The sSMC(Y) with two SRY
signals (red) revealed the presence of neo(Y)(pter→Yp11.2::
Yp11.2→pter) derived from Ypter to Yp11.2 without centromeric
material (Fig. 3B), which might
indicate the existing breakpoints in Yp11.2. The existence of the
neocentromere requires further verification. In addition, no
microdeletions in the AZF region were detected.
Summary of neo(Y) cases
A literature review on the cases with neocentric
chromosome Y was conducted, which are presented in Table III (13,14,22–28).
Of all cases, 4/9 were female, 3/9 were male, and the sex in 2/9
cases was not available. Among their chromosomal karyotypes, 4/9
were mosaic, 4/9 were non-mosaic and 1/9 was not reported. The
clinic manifestations of these patients were varied, ranging from
normal fetal ultrasound findings to abnormal phenotypes in
teenagers and adults.
| Table III.Clinical review and manifestations of
chromosome Y with neocentromere. |
Table III.
Clinical review and manifestations of
chromosome Y with neocentromere.
| Author, year | Case | Sex/age | Karyotype | Involved neocentric
Y | Other
description | Clinical
feathers/Reason to study | (Refs.) |
|---|
| Rivera et
al, 1993 | 1 | N.R./12 y | 45,X(37.5%)/46, X,
+ mar(30.5%)/46, X, psu dic(Y) (q11) (7.5%)/47,X, psu dic(Y) (q11),
psu dic(Y) (q11) (4.5%) | psu dic(Y)
(q11) | N.R. | Turner syndrome
phenotype | (27) |
| Bukvic et
al, 1996 | 2 | F/29 y | 45,X/46,XY/47,
XY,+mar | A rearranged Y
chromosome carrying an inactivated normal centromere. | N.R. | Short stature (138
cm); removed hypoplastic uterus and streak gonads (2 y) | (23) |
| Warburton et
al, 1997 | 3 | N.R. | N.R. | inv dup Y(q)
(qter-q11.2::q11.2-qter) | Consisting of Yq
heterochromatin and distal Yq euchromatin but lacking detectable
a-satellite DNA | N.R. | (25) |
| Floridia et
al, 2000 | 4 | F/fetus | 45,X[8]/46,X,
rea(Y)[18] | rea(Y)
(qter-q11.2::q11.2-qter) | Consisting of an
inverted duplication of the long arm heterochromatin and a small
amount of euchromatin, but lacking a normal centromere | Cystic hygroma;
intrauterine fetal death | (26) |
| Assumpção et
al, 2002 | 5 | F/18 y | 46,X,+mar |
rea(Y)(qter→q11::q11→qter) | Lacking Yp and
Y-centromere sequences | Primary amenorrhea;
hypogonadism | (24) |
| Sheth et al,
2009 | 6 | M/fetus | 47,XX,+mar | inv dup(Y)
(pter→Yp11.2::Yp11.2→pter) | N.R. | Normal in
ultrasound; pregnancy terminated; no abnormalities observed | (14) |
| Liehr, 2019 | 7 | F/28 y | 47,XX,+mar | inv dup(Y)
(qter→q11.23::q11.23→qter) | N.R. | Normal female;
infertile | (22) |
| Chen et al,
2011 | 8 | M/newborn |
46,X,+mar[8]/46,XY[16] |
r(Y)(::p11.31/q11.1::) (Ypter-, SRY+,
DYZ3+,DYZ1-, Yqter-,mBand Y+,SKY+)[8] | Lacking Yp and Yq
telomeric signals and DYZ1 signal | Advanced maternal
age | (28) |
| Pasantes et
al, 2012 | 9 | M/11 y | 47,X,i(Y)(p10),
i(Y)(q10) | inv dup(Y)
(qter→q11.221::q11.221→ q12→neo→q12→qter) | ish
idic(Y)(wcpY+,TEL++,SHOX++,SRY++,TSPY++, RBMY++,DYZ3++,UTY+, XKRY-,
DAZ-,CDY-,DYZ1-, SYBL-), inv dup(Y)(wcpY+, TEL++,SYBL++,DYZ1++,
DAZ+, CDY+,RBMY+, XKRY+, SHOX-,TSPY-, DYZ3-,UTY-). | an elevated blood
serum AFP in the mother; an urachal cyst (2 m) | (13) |
| The present
study | 10 | M/27 y | 47,X,i(Y)(q10),
+mar | neo(Y)
(pter→Yp11.2::Yp11.2→pter) |
47,X,idic(Y)(p11.2), neo(Y)
(pter→Yp11.2::Yp11.2→pter) | azoospermia | N/A |
Discussion
The present study reported an azoospermic male and
established the karyotype as a non-mosaic 47, X, idic(Y)(p11.2),
neo(Y)(pter→Yp11.2::Yp11.2→pter), consisting of an idic(Yq) and a
neo(Yp). In the karyotype, idic(Y) was shown to contain a copy of
the entire long arm of the Y chromosome, Y centromere, and partial
euchromatic part of Yp11.2. The neo(Yp) could be described as
neo(Y)(pter→Yp11.2::Yp11.2→pter), including two copies of SRY and
Yp11.2 to Ypter, lacking the original Y centromere. The primary
constriction appeared in the connecting regions, making it possible
to associate it with a functional neocentromere. However, further
tests will be required to confirm this. To the best of the authors'
knowledge, this is the first report of an infertile man with a
neo(Yp) in addition to an idic(Yq).
Considering the amount of Y chromosomal duplication
from CMA results, this azoospermic proband could be seen as being
equivalent to 47,XYY males. However, this did not reasonably
explain the male's spermatogenesis impairment, as patients with XYY
syndrome can have various spermatozoa counts, ranging from normal
to azoospermia (29–31). It is worth mentioning that CMA in
the present study serves a critical role in identifying the fact
that the marker chromosome is originated from chromosome Y, which
offers guidance for the following verification of the neo(Y) using
FISH.
Idic(Y) is one of the most common structural
abnormalities of the Y chromosome, most of which usually exist in a
mosaic form with 45,X (5,32). Patients with idic(Y) exhibit
various abnormal/ambiguous sexual developments, due predominantly
to differences in karyotypic mosaic proportions, breakpoints and Y
chromosome fusions (1,32,33).
Lange et al (6) proposed
that the formation of idic(Y) results from homologous recombination
between opposing arms of male-specific region of the Y(MSY)
palindromes, leading to outcomes ranging from dyszoospermia to sex
reversal or Turner syndrome. Idic(Y) can be generally divided into
idic(Yp) and idic(Yq); idic(Yp) with breakpoints in the long arm of
the Y chromosome can lead to spermatogenic failure due to the
deletion or rearrangement of the AZF region (5,34).
DesGroseilliers et al (5)
described two males with no observed genital abnormalities that
presented 46,X,idic(Y)(q11.21) separately, who lacked most of Yq
and were positive for the Y centromere DYZ3 and SRY, but negative
for the Yq heterochromatin DYZ1. The inactivation or synergic
action of the centromeres may be responsible for the stable
formation of idic(Y) in the process of early paternal gametogenesis
(5,35). Kuan et al (36) identified a non-mosaic
46,X,idic(Y)(q12) in a fetus and concluded that an i(Y) chromosome
can result from breakage and fusion at the Yq pseudo-autosomal
region. Kumar et al (37)
reported a 32-year-old non-obstructive azoospermia man with
non-mosaic 46,XY, whose dicentric Y fused at Yq12 [proximal to
pseudoautosomal region (PAR)2]. However, the association between
non-mosaic idic(Yq) and infertility remains unclear. Cui et
al (7) described a non-mosaic
46,X,idic(Y)(p11.32) male presenting short stature and severe
oligozoospermia. They concluded that PAR1 serves a critical role in
regulating the meiotic pairing and sperm production, the
aberrations of which could result in spermatogenic failure. Lehmann
et al (32) reported an
azoospermic male with idic(Y)(p11.3), speculating that extra copies
of the AZF region might be a contributing factor for spermatogenic
failure. In the present study, the proband presented no
microdeletions in AZF region, located in Yq11. The gain of
Yp11.31q11.23 detected by CMA, which was further testified using
two sets of FISH probes, additionally demonstrated the existence of
idic(Yq) with two integrated Yq arms, as well as two AZF regions.
The copy of AZF regions in the present study appeared to support
the hypothesis to some extent. However, the correlation between
extra copies of AZF regions and spermatogenesis still needs to be
investigated.
Chromosome Y is often involved in the formation of
marker chromosomes (23). The
majority of published neocentric sSMCs can be classified as small
inverted duplicated chromosomes, with the neocentromere forming on
an acentric fragment (14,16). If neocentromerization occurs in the
same cell cycle, a stable non-mosaic state, resulting from the
formation of an acentric fragment at meiosis, will develop
(38). In the present study, the
formation of a neocentromere on the stable
neo(Y)(pter→Yp11.2::Yp11.2→pter) was accompanied by the idic(Y),
which suggests that sequences in Yp might exist that facilitate the
combination of the centromeric proteins; this requires further
investigation. For the proband in the present study, it is probable
that the inactivation of one centromere in idic(Y) and the
activation of the neocentromere in neo(Y) may have happened
simultaneously after the formation of both idic(Y) and neo(Y)
(13). Currently, the clinical
phenotypes of sSMCs with neocentromeres include facial
dysmorphisms, renal defects, short stature and delayed development
(15). The genotype-phenotype
correlation on neocentric chromosome Y was summarized. Among them,
newborns or fetuses showed normal or no evident abnormalities
(cases 4, 6 and 8). Five cases presented gonadal dysgenesis or
spermatogenesis dysfunction (cases 1, 2, 5, 7 and 9). In addition,
the majority of the neocentric sites were located between Yq11.2
and Yq12 (cases 1,3–5,7 and 9), which demonstrated that
neocentromeres arising on the Y chromosome were inclined to emerge
on the Yq instead of Yp. In case 6, an unborn boy with karyoype
47,XX,+mar was described, with marker chromosome identified as
neo(Y)(pter→Yp11.2::Yp11.2→pter). Partial disomy of Ypter to Yp11.2
might not be associated with any major malformations (14), but fertility in adulthood could not
be established. In general, there might be phenotypic diversity
associated with neo(Y) carriers and the potential risk of
infertility for such carriers should be taken seriously.
An azoospermic male with a neocentric sSMC(Y)
accompanied by idic(Yq) was characterized according to karyotype
analysis, CMA and FISH. The sSMC was determined to be
neo(Y)(pter→Yp11.2::Yp11.2→pter). The present study contributed to
the understanding of clinical phenotypes associated with neocentric
Y chromosomes and provided information for the genetic counseling
of such aberrations.
Acknowledgements
Not applicable.
Funding
The present study was supported by The National Key
Research and Development Program of China (grant no.
2016YFC1000601).
Availability of data and materials
The data and materials of this study are available
from the corresponding author on reasonable request.
Authors' contributions
YJ obtained the clinical information, collected data
from the literature and wrote the manuscript. FY and RW critically
analyzed the data and revised the manuscript. HZ, LeL and LiL
performed the cytogenetic study, CMA and FISH experiments and
analyzed the results. SL and RL conceived and designed the study.
RL performed the final review and editing of the manuscript. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by The Medical Ethics
Committee of the First Hospital of Jilin University (permit no.
2016-416). The patient provided written informed consent for
participating in this study.
Patient consent for publication
The current case report was published with the
informed consent of the patient, whose anonymity was preserved.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kalantari H, Asia S, Totonchi M,
Vazirinasab H, Mansouri Z, Zarei Moradi S, Haratian K, Gourabi H
and Mohseni Meybodi A: Delineating the association between
isodicentric chromosome Y and infertility: A retrospective study.
Fertil Steril. 101:1091–1096. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tuck-Muller CM, Chen H, Martínez JE, Shen
CC, Li S, Kusyk C, Batista DA, Bhatnagar YM, Dowling E and
Wertelecki W: Isodicentric Y chromosome: Cytogenetic, molecular and
clinical studies and review of the literature. Hum Genet.
96:119–129. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Si YM, Dong Y, Wang W, Qi KY and Wang X:
Hypospadias in a male infant with an unusual mosaic 45,X/46,X,psu
idic(Y)(p11.32)/46,XY and haploinsufficiency of SHOX: A case
report. Mol Med Rep. 16:201–207. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Dundar M, Lowther G, Acar H, Kurtoglu S,
Demiryilmaz F and Kucukaydin M: A case of ambiguous genitalia
presenting with a 45,X/46,Xr(Y)(p11.2;q11.23)/47,X,idic(Y)(p11.2),
idic(Y)(p11.2) karyotype. Ann Genet. 44:5–8. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
DesGroseilliers M, Beaulieu Bergeron M,
Brochu P, Lemyre E and Lemieux N: Phenotypic variability in
isodicentric Y patients: Study of nine cases. Clin Genet.
70:145–50. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lange J, Skaletsky H, van Daalen SK, Embry
SL, Korver CM, Brown LG, Oates RD, Silber S, Repping S and Page DC:
Isodicentric Y chromosomes and sex disorders as byproducts of
homologous recombination that maintains palindromes. Cell.
138:855–869. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cui YX, Wang WP, Li TF, Li WW, Wu QY, Li
N, Zhang C, Yao Q, Hu YA and Xia XY: Clinical and cytogenomic
studies in a case of infertility associated with a nonmosaic
dicentric Y chromosome. Andrologia. 47:477–481. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Liehr T, Claussen U and Starke H: Small
supernumerary marker chromosomes (sSMC) in humans. Cytogenet Genome
Res. 107:55–67. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Liehr T and Weise A: Frequency of small
supernumerary marker chromosomes in prenatal, newborn,
developmentally retarded and infertility diagnostics. Int J Mol
Med. 19:719–731. 2007.PubMed/NCBI
|
|
10
|
Liehr T, Mrasek K, Weise A, Dufke A,
Rodríguez L, Martínez Guardia N, Sanchís A, Vermeesch JR, Ramel C,
Polityko A, et al: Small supernumerary marker chromosomes-progress
towards a genotype-phenotype correlation. Cytogenet Genome Res.
112:23–34. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Armanet N, Tosca L, Brisset S, Liehr T and
Tachdjian G: Small supernumerary marker chromosomes in human
infertility. Cytogenet Genome Res. 146:100–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Marshall OJ, Chueh AC, Wong LH and Choo
KH: Neocentromeres: New insights into centromere structure, disease
development, and karyotype evolution. Am J Hum Genet. 82:261–282.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Pasantes JJ, Wimmer R, Knebel S, Münch C,
Kelbova C, Junge A, Kieback P, Küpferling P and Schempp W:
47,X,idic(Y),inv dup(Y): A non-mosaic case of a phenotypically
normal boy with two different Y isochromosomes and neocentromere
formation. Cytogenet Genome Res. 136:157–162. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sheth F, Ewers E, Kosyakova N, Weise A,
Sheth J, Patil S, Ziegler M and Liehr T: A neocentric isochromosome
Yp present as additional small supernumerary marker
chromosome--evidence against U-type exchange mechanism? Cytogenet
Genome Res. 125:115–116. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Burrack LS and Berman J: Neocentromeres
and epigenetically inherited features of centromeres. Chromosome
Res. 20:607–619. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Poot M: Neocentromeres to the rescue of
acentric chromosome fragments. Mol Syndromol. 8:279–281. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
World Health Organization, . WHO
Laboratory Manual for the Examination and Processing of Human
Semen. 5th. Geneva: World Health Organization, Geneva; 2010
|
|
18
|
Jiang Y, Wang R, Li L, Xue L, Deng S and
Liu R: Molecular-cytogenetic study of de novo mosaic karyoype
45,X/46,X,i(Yq)/46,X,idic(Yq) in an azoospermic male: Case report
and literature review. Mol Med Rep. 16:3433–3438. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
McGowan-Jordan J, Simons A and Schmid M:
ISCN 2016: An International Ssystem for Human Cytogenomic
Nomenclature (2016) Reprint of Cytogenet. Genome Res. 149(1-2)1st.
S. Karger; Basel: 2016
|
|
20
|
Zhang HG, Zhang ZB, Wang RX, Yu Y, Yu XW,
Fadlalla E and Liu RZ: Male infertility in Northeast China:
Molecular detection of Y chromosome microdeletions in azoospermic
patients with Klinefelter's syndrome. Genet Mol Res. 12:4972–4980.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zhang YS, Dai RL, Wang RX, Zhang HG, Chen
S and Liu RZ: Analysis of Y chromosome microdeletion in 1738
infertile men from northeastern China. Urology. 82:584–588. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Liehr T: 2019. Small supernumerary marker
chromosomes. http://ssmc-tl.com/sSMC.htmlNovember 22–2018
|
|
23
|
Bukvic N, Susca F, Gentile M, Tangari E,
Ianniruberto A and Guanti G: An unusual dicentric Y chromosome with
a functional centromere with no detectable alpha-satellite. Hum
Genet. 97:453–456. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Assumpção JG, Berkofsky-Fessler W,
Viguetti Campos N, Trevas Maciel-Guerra A, Li S, Melaragno MI,
Palandi de Mello M and Warburton PE: Identification of a
neocentromere in a rearranged Y chromosome with no detectable DYZ3
centromeric sequence. Am J Med Genet. 113:263–267. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Warburton PE, Cooke CA, Bourassa S, Vafa
O, Sullivan BA, Stetten G, Gimelli G, Warburton D, Tyler-Smith C,
Sullivan KF, et al: Immunolocalization of CENP-A suggests a
distinct nucleosome structure at the inner kinetochoreplate of
active centromeres. Curr Biol. 7:901–904. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Floridia G, Gimelli G, Zuffardi O,
Earnshaw WC, Warburton PE and Tyler-Smith C: A neocentromere in the
DAZ region of the human Y chromosome. Chromosoma. 109:318–327.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Rivera H, Domínguez MG, Vásquez AI, Ramos
AL and Fragoso R: Centromeric association of a microchromosome in a
Turner syndrome patient with a pseudodicentric Y. Hum Genet.
92:522–524. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chen CP, Chen M, Ma GC, Chang SP, Chen YY,
Wu PC, Chen LF and Wang W: Prenatal diagnosis and molecular
cytogenetic characterization of a small marker chromosome derived
from Y chromosome. Taiwan J Obstet Gynecol. 50:253–257. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kim IW, Khadilkar AC, Ko EY and Sabanegh
ES Jr: 47,XYY syndrome and male infertility. Rev Urol. 15:188–196.
2013.PubMed/NCBI
|
|
30
|
Rives N, Milazzo JP, Miraux L, North MO,
Sibert L and Macé B: From spermatocytes to spermatozoa in an
infertile XYY male. Int J Androl. 28:304–310. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Faed M, Robertson J, MacIntosh WG and
Grieve J: Spermatogenesis in an infertile XYY man. Hum Genet.
33:341–347. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lehmann KJ, Kovac JR, Xu J and Fischer MA:
Isodicentric Yq mosaicism presenting as infertility and maturation
arrest without altered SRY and AZF regions. J Assist Reprod Genet.
29:939–942. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Faure AK, Aknin-Seifer I, Satre V, Amblard
F, Devillard F, Hennebicq S, Chouteau J, Bergues U, Levy R and
Rousseaux S: Fine mapping of re-arranged Y chromosome in three
infertile patients with non-obstructive
azoospermia/cryptozoospermia. Hum Reprod. 22:1854–1860. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Vogt PH, Edelmann A, Hirschmann P and
Köhler MR: The azoospermia factor (AZF) of the human Y chromosome
in Yq11: Function and analysis in spermatogenesis. Reprod Fertil
Dev. 7:685–693. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Hsu LY: Phenotype/karyotype correlations
of Y chromosome aneuploidy with emphasis on structural aberrations
in postnatally diagnosed cases. Am J Med Genet. 53:108–140. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Kuan LC, Su MT, Chen M, Kuo PL and Kuo TC:
A non-mosaic isodicentric Y chromosome resulting from breakage and
fusion at the Yq pseudo-autosomal region in a fetus. J Assist
Reprod Genet. 30:1559–1562. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Kumar P, Jain M, Kalsi AK and Halder A:
Molecular characterisation of a case of dicentric Y presented as
nonobstructive azoospermia with testicular early maturation arrest.
Andrologia. 50:2018. View Article : Google Scholar
|
|
38
|
Voullaire L, Saffery R, Earle E, Irvine
DV, Slater H, Dale S, du Sart D, Fleming T and Choo KH: Mosaic inv
dup(8p) marker chromosome with stable neocentromere suggests
neocentromerization is a post-zygotic event. Am J Med Genet.
102:86–94. 2001. View Article : Google Scholar : PubMed/NCBI
|