Introduction
Developmental dysplasia of the hip (DDH), formerly
known as congenital dysplasia of the hip (CDH) affects 1–5‰ babies
in China and has a female-to-male ratio of 4–10:1 (1,2).
Shallow acetabulum, slacking joint capsule, and narrowing joint
space are the main anatomical features of DDH, which result in
chronic pain, joint stiffness, synovial inflammation, and
hyperplasia in fossa acetabuli.
As the hallmark symptom of DDH, the pain experience
is well-recognized as typically transitioning from an intermittent
weight-bearing pain to an increasingly persistent and chronic pain
around the hip joint. Besides, the characteristic pain in DDH is
increasing restriction of active and passive movement. The hip
joint becomes stiff with the progression of DDH, and this stiffness
is usually observed in the later stage of DDH and worsens with the
progression of osteoarthritis (OA).
Previous theories demonstrated that the initial hip
pain in OA is mainly derived from acetabular labral lesions
(3–5), followed by the infiltration of
sensory neurons into the synovium and labrum (6,7).
However, OA is a multifactorial inducing disease, which is not
commonly believed as mainly secondary from the progress of DDH.
Additionally, the development of OA is usually a long history, but
the phenomenon of many young adult patients with moderate DDH
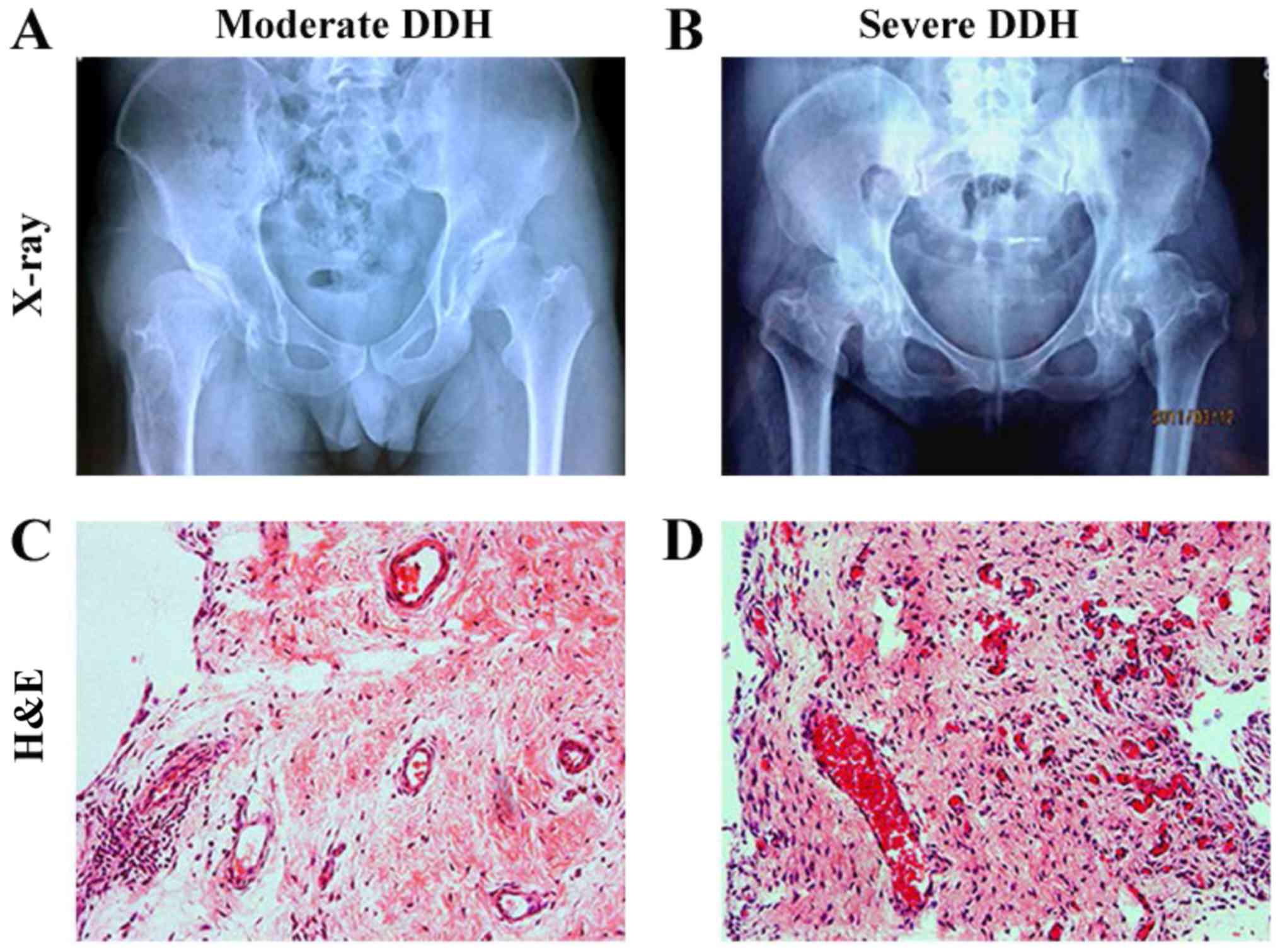
(slight pain and joint restriction) (Fig. 1A) developing into severe DDH (acute
pain and joint dysfunction) (Fig.
1B) within a few years was frequently observed in clinic, which
is not the characteristic process of OA. Therefore, this phenomenon
prompts us to investigate the underlying pathologic changes during
the development of DDH. As we know, moderate or severe DDH is
characterized by cartilage degeneration, synovial hyperplasia,
subchondral sclerosis, inflammation and osteophyte formation. So we
speculated that immune cells and inflammatory cells are derived
from two aspects: Peripheral blood and subchondral bone. On the one
hand, the abnormal stress may promote subchondral bone to release
chemotaxis signals. T cells, B cells, macrophages induced by the
signals migrate to hip joint synovium. Inflammatory mediators are
secreted by the cells into the hip joint cavity, causing the
destruction of articular cartilage. On the other hand, the abnormal
stress of subchondral bone force the immune cells and stem cells
which come from the bone marrow to move to osteochondral junction.
Chemokines and MMPs are released and cause osteochondral
destruction. The aim of this study is mainly to observe the
pathological changes and inflammatory infiltration in the
hypertrophic synovium of hip joint associated with the progression
of DDH and to investigate the effect of synovial hyperplasia on
cartilage degeneration.
Synovial membrane inflammation in OA is usually
secondary to adjacent cartilage degradation and characterized by
angiogenesis, invasion of immune cells and pro-inflammatory
mediators. Mast cells are widely distributed around the
microvasculature of the articular synovium, skin and visceral
mucosa which can secrete a variety of cytokines and are involved in
immune regulation such as T cells, B cells and APC cells
activation. Synovial inflammation is correlated with the severity
and progress of OA and is also the main cause of pain in patients
with OA (8,9). Recently, research on pain and
stiffness in musculoskeletal disorders has been advanced with
histological and immunohistochemical (IHC) analysis of synovium,
which has been increasingly useful in identifying pathological
changes in vivo (10,11).
Analysis of synovial tissues in OA represents inflammatory changes
and neuron infiltration (12,13),
whereas synovium from frozen shoulders display not only
inflammatory and angiogenesis but also fibrosis and proliferative
myelofibrosis (14,15). Undoubtedly, considerable cytokines
might become involved in the development of DDH, but the pathology
of this process remains unclear, especially in different stages of
DDH. Thus, the purpose of this study is to identify the cell type
involved in synovium of DDH by using novel IHC analysis and
antibodies and improve our understanding of pathophysiologic
progression in DDH.
Materials and methods
Patients and biopsies
This study was carried out in accordance with the
Declaration of Helsinki and was approved by the ethics committee of
Xinhua Hospital affiliated to Shanghai Jiao Tong University School
of Medicine. The samples obtained from the operations were prepared
for testing purposes only and with the approval and signed consent
of the patients.
The clinical biopsies used in this study were
obtained from patients who accepted surgical treatments in our
institution between November 2013 and December 2014. The patients
with DDH involved in this study were divided into two groups
according to their clinical diagnoses and severities (16). A total of 45 patients (F/M=38/7,
mean age=26.5 years) with DDH (Crowe: I–II) and grade 2 or less OA
of K-L classification (Kellgren and Lawrence Scale) were set as the
moderate DDH group. A total of 35 patients (F/M=27/8, mean age=29.6
years) with DDH (Crowe: I–II) and grade 3–4 OA of K-L
classification were set as the severe DDH group. The degrees of hip
joint dislocation and the severities of OA were divided according
to the classification of Crowe and the grade of K-L, respectively,
in clinic (17,18). Clinical and laboratory data for the
entire groups are presented in Table
I. Variables, such as erythrocyte sedimentation rate (ESR) and
C-reactive protein (CRP), were measured by a standard clinical
technology. The patients in two groups were matched according to
gender and age and absence of systemic disease.
 | Table I.Data and clinical details of patients
and normal people recruited in this study. |
Table I.
Data and clinical details of patients
and normal people recruited in this study.
|
Characteristics | Moderate DDH | Severe DDH |
|---|
| Number | 45 | 35 |
| Ages | 26.5±6.1 | 29.6±4.9 |
| Female/Male | 38/7 | 27/8 |
| BMI
(kg/m2) | 22.8±1.9 | 22.8±2.5 |
| Durations
(years) |
4.6±1.5 |
3.8±2.1 |
| CRP (mg/l) |
9.9±3.1 |
9.8±3.4 |
| ESR (mm/1st h) | 19.1±3.9 | 20.7±6.1 |
| Harris hip
score | 67.7±8.2 |
57.4±8.4a |
| Visual analogue
score | 4.1±0.7 |
4.4±0.9 |
The diagnosis of DDH was based on the standard
anteroposterior radiograph of hip with a sharp angle of <45° and
a center edge angle (CEA) of <20° (19,20).
The patients with moderate DDH received operation of periactabular
osteotomy (PAO), whereas those with severe DDH underwent total hip
arthroplasty (THA). The hyperplasia synovium was extracted from the
inner wall of the joint capsule when we opened the joint capsule
during the operation.
IHC analysis
Synovial specimens obtained from these patients
during the operation were immediately cut into pieces of 1
cm3 and immersed in 4% paraformaldehyde for 24 h, then
washed, dehydrated with a graded series of alcohol solutions, and
finally embedded in paraffin for 24 h. The blocks were cut into 5
µm sections with a Leica microtome (RM2255; Leica Microsystems
GmbH, Wetzlar, Germany) and were mounted on anti-off slides (no.
4951PLUS; Thermo Fisher Scientific, Inc., Waltham, MA, USA).
The slides were stained with hematoxylin and eosin
for histological analysis. After citrate antigen retrieval and
peroxidase inactivation treatment, immunohistochemistry was
performed with antibodies directed against CD45 (Leukocyte common
antigen; LCA), CD3 (T cells), CD20 (B cells), CD68 (macrophages),
neurofilament-200 (NF-200; neural marker), mindbomb homolog 1
(MIB1) (proliferative cell markers), substance P (SP;
neuropeptides), calcitonin gene-related peptide (CGRP;
neuropeptides), vimentin (fibroblasts), α smooth muscle actin
(α-SMA; myofibroblasts), and mast cell tryptase (mast cells). The
slides were rinsed in phosphate buffer saline (3×5 min) and
incubated with biotinylated secondary antibody (Dako, Ely, UK).
Finally, 3′-diaminobenzidine tetra-chloride) was used for the
visualization of immunoreactions.
The images of the microscopic fields were captured
by a camera (DEI750; Optronics Engineering, Goleta, CA, USA)
attached to the microscope. In each biopsy, two slides were
obtained at different depths, and eight microscopic fields from
each slide were photographed and analyzed. Thus, in every synovial
sample, 16 microscopic fields were collected. The mean optical
density (MOD) levels were measured with Image-Pro plus 6.0 (Media
Cybernetics, Inc., Rockville, MD, USA) as previously described
(21). The results were expressed
as the positive staining density in relation to the total area of
each microscopic field.
All these slides were detected under light
microscopy, and the presence of labeled cells is documented and
tabulated in Table II. The
absence of staining was documented as a negative result (−), and
the presence of staining was noted as a positive result (+) by
using a scale based on the number of cells per high-power field
(×400), (+), 1 to 4; (++), 5 to 10; (+++), >10; and (++++),
>100 (14).
| Table II.Results for immunocytochemical
staining of biopsy material from the DDH. |
Table II.
Results for immunocytochemical
staining of biopsy material from the DDH.
|
|
| Resulta |
|
|
|---|
|
|
|
|
|
|
|---|
| Antibody moderate
DDH | Cell type severe
DDH | Moderate DDH | Severe DDH | Number of patients
positive |
|---|
| CD3 | T cells | + | ++ | 30/45 | 29/35 |
| CD20 | B cells | + | +++ | 28/45 | 31/35 |
| CD45 | Leukocytes | ++ | +++ | 38/45 | 34/35 |
| CD68 | Macrophage | + | ++ | 34/45 | 30/35 |
| NF-200 | Neural fiber | + | ++ | 37/45 | 33/35 |
| Vimentin | Fibroblasts | +++ | ++++ | 43/45 | 34/35 |
| MIB-1 | Proliferating
cells | +++ | +++ | 44/45 | 31/35 |
| α-SMA | Myofibroblasts | + | +++ | 34/45 | 35/35 |
| Mast cell
tryptase | Mast cells | ++ | ++ | 38/45 | 26/35 |
| Neuropeptides |
|
|
|
|
|
| SP |
| + | ++ | 33/45 | 33/35 |
|
CGRP |
| + | ++ | 38/45 | 32/35 |
Statistics
The results in Table
I are expressed as mean ± standard deviation (SD). The
comparisons the between moderate and severe DDH groups with respect
to the MOD levels of each antibody in the synovium were preformed
using the Mann-Whitney U test. Graphpad software (version 5.01;
GraphPad Software, Inc., La Jolla, CA, USA) was used. A P<0.05
was considered to indicate a statistically significant difference.
The correlations analyses were performed with Spearman rank
correlation test. A two-sided P-value <0.01 was statistically
significant.
Results
Imaging, histological and IHC
analysis
Pelvic radiograph illustrate the morphology of the
femoral head and the acetabulum of the patients with moderate DDH
to severe DDH (Fig. 1A and B).
Histological analysis of the synovial tissue revealed evidence of
varied degrees of chronic inflammation, the hyperplasia of synovial
layers, and infiltration of inflammatory cells (Fig. 1 and Table II) during the process from
moderate DDH to severe DDH.
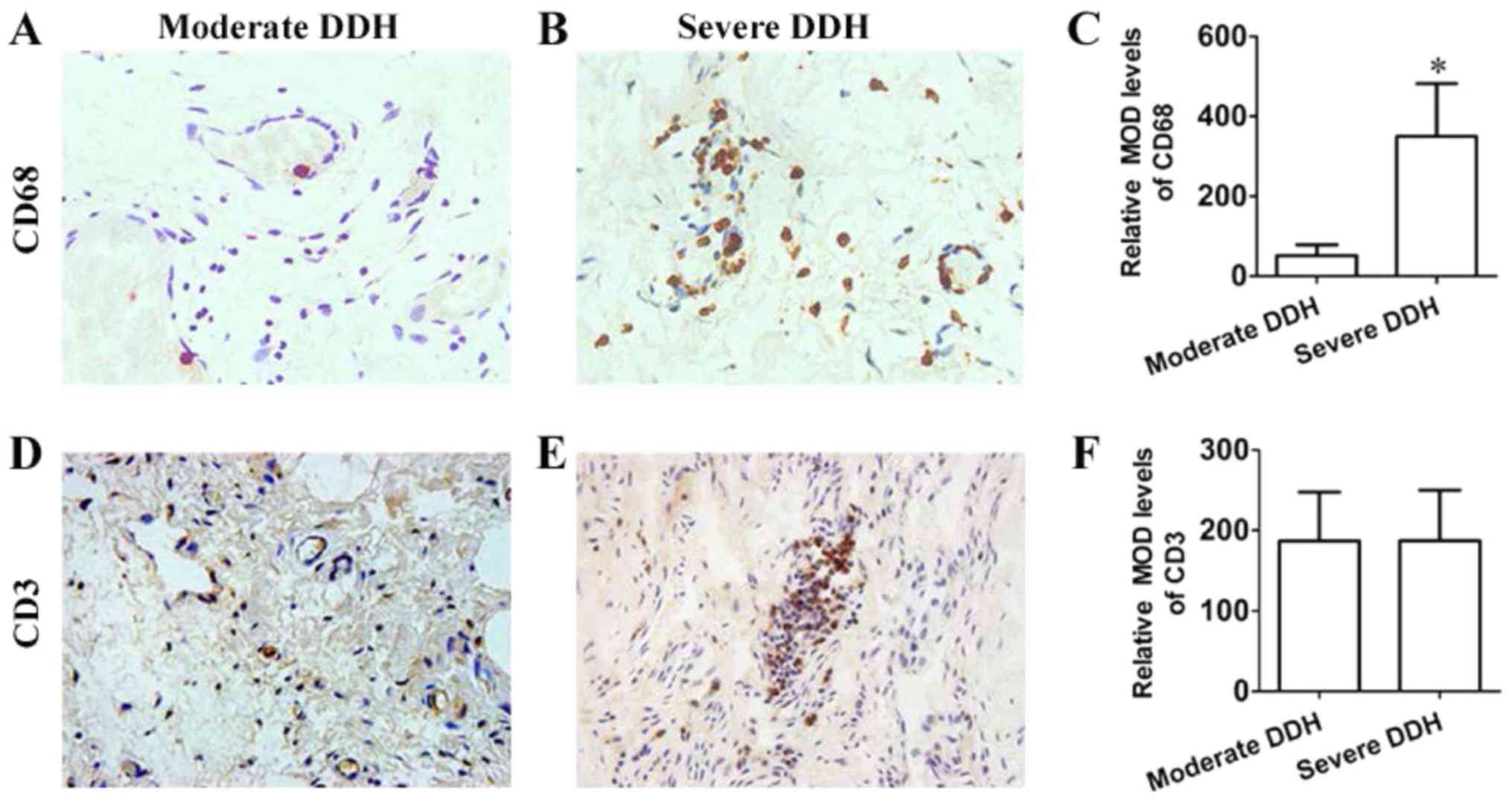
The immunohistochemistry stains showed macrophage
infiltration and proliferation of inflammatory cells through the
special positive staining of CD68 (macrophage), CD3 (T cells), CD45
(LCA), CD20 (B cells), and mast cell tryptase (mast cells). The
result of IHC staining implied that the CD68 expression in the
synovial tissue of severe DDH was higher than that of moderate DDH
(Fig. 2A-C). CD3 expression was no
significant difference between moderate DDH and severe DDH
(Fig. 2D-F). The positive targets
were indicated with fulvous staining in each figure. The
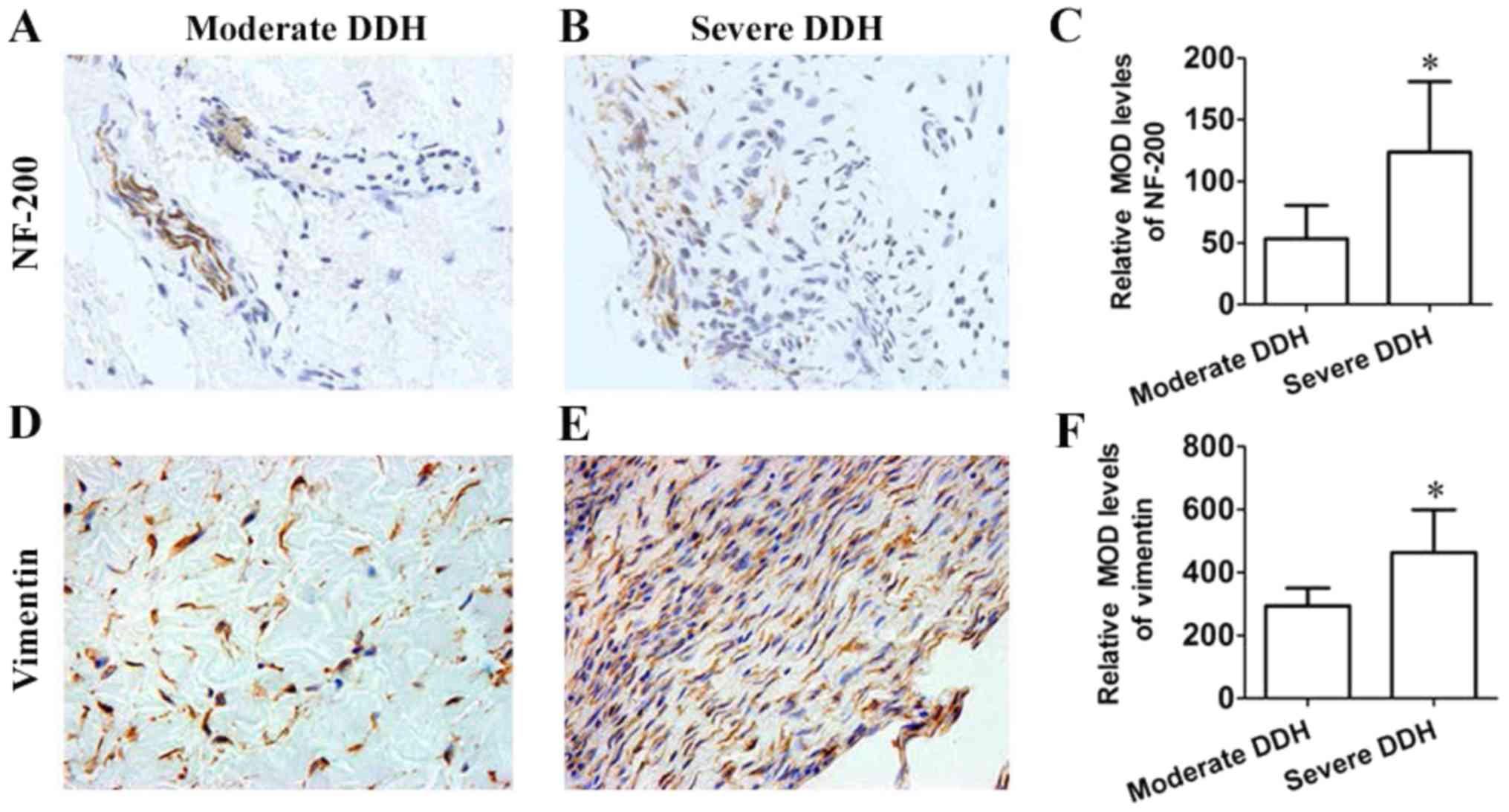
observation of nerve fibers was also confirmed by staining NF-200
(Fig. 3A and B), and the MOD of
NF-200 in severe DDH was higher than that in moderate DDH (Fig. 3C). Excessive staining with
vimentin, a biomarker of fibroblast, indicated that the fibroblast
had an overwhelming proportion in the synovial tissues affected by
severe DDH (Fig. 3D and E). The
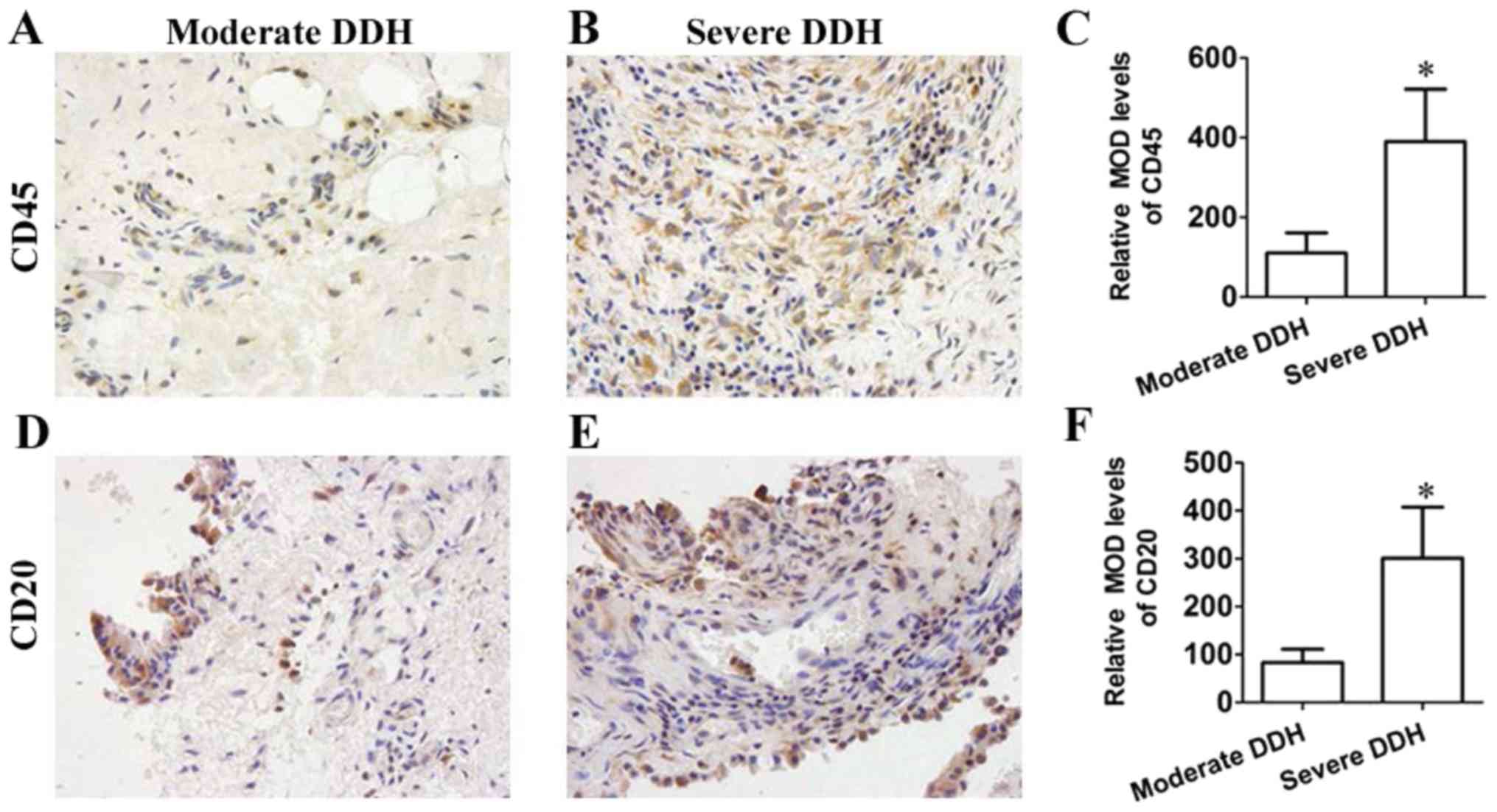
trend of vimentin coincided with NF-200 (Fig. 3F). CD20, CD45 are respectively
biomarker of B cells and leukocytes. The increased expression of
CD20, CD45 protein in the synovial tissue of patients experiencing
moderate DDH or severe DDH was detected by IHC staining (Fig. 4A-F). The results indicated chronic
inflammatory cells infiltration. IHC staining showed that the
expression of mast cell tryptase in the synovial tissue of severe
DDH was lower than that of moderate DDH (Fig. 5A-C). IHC staining showed that the
expression of mast cell tryptase in the synovial tissue of severe
DDH was lower than that of moderate DDH (Fig. 5A-C). Moreover, strong positive
staining of MIB1 also illustrated that the active proliferation
status of fibroblast (Fig. 5D-F).
α-SMA (smooth muscle cell and myofibroblast markers), which
symbolized the proliferation of microvascular and myofibroblast
(Fig. 5G-I) suggest excessive
vascularization and fibrosis in the synovium of severe DDH compared
with moderate DDH. Additionally, in severe DDH, staining of SP and
CGRP in synovium were significantly up-regulated compared with
those in moderate DDH (Fig. 6A-F),
indicating the involvement of neuropeptides into the synovium
during the development of DDH.
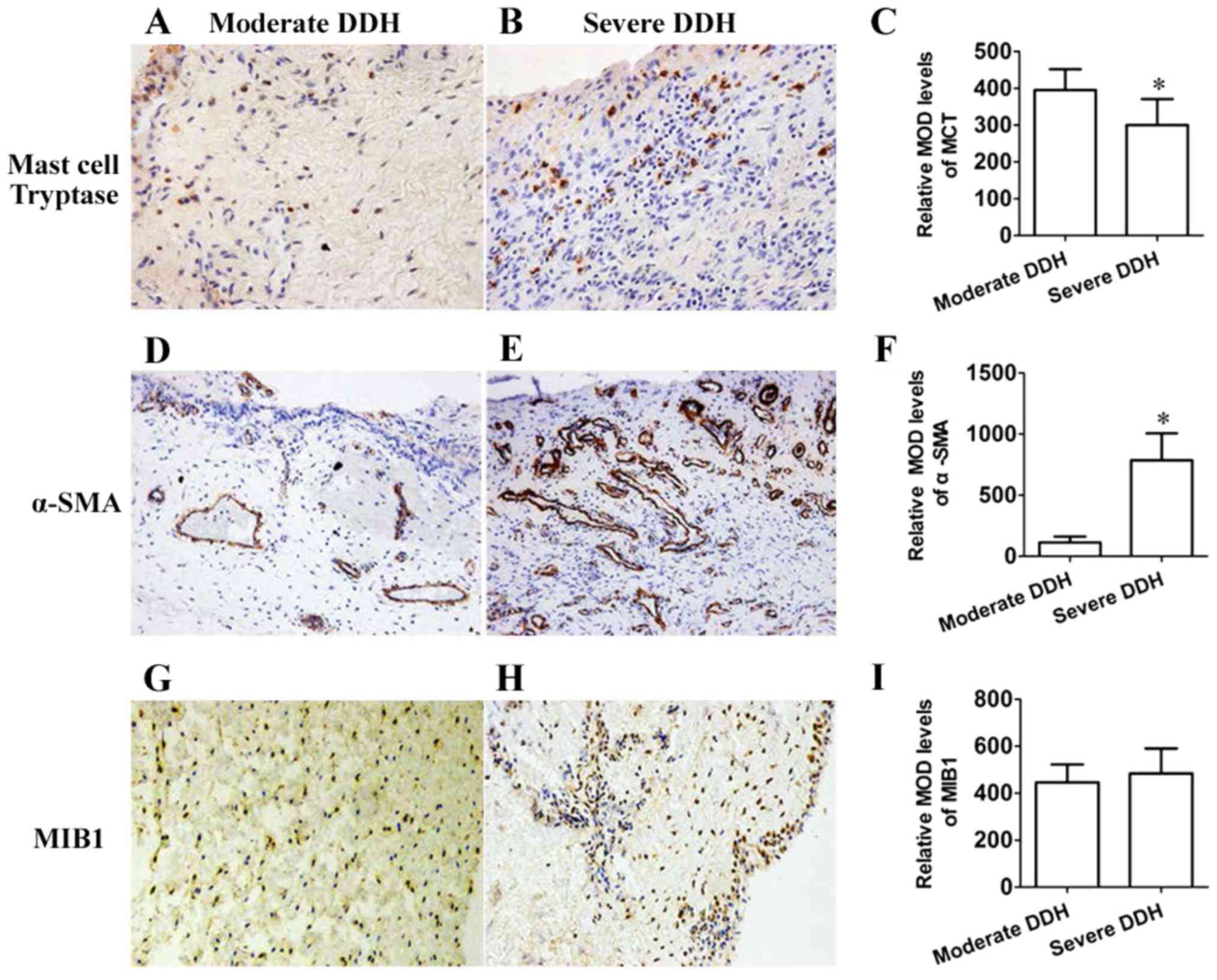 | Figure 5.(A-I) Immunohistochemical staining
and MOD analysis. (A, B, D, E, G and H) Immunohistochemical
staining of MCT, α-SMA and MIB1 in synovium between moderate and
severe DDH group. (A, B, G and H) Magnification: ×200; (D and E)
magnification: ×100. (C, F and I) Comparisons of MOD levels of MCT,
α-SMA and MIB1 in immunohistochemical staining between different
groups. *P<0.05 compared with moderate DDH. MOD, mean optical
density; DDH, developmental dysplasia of the hip; MCT, mast cell
tryptase; α-SMA, α-smooth muscle actin; MIB1, mindbomb homolog
1. |
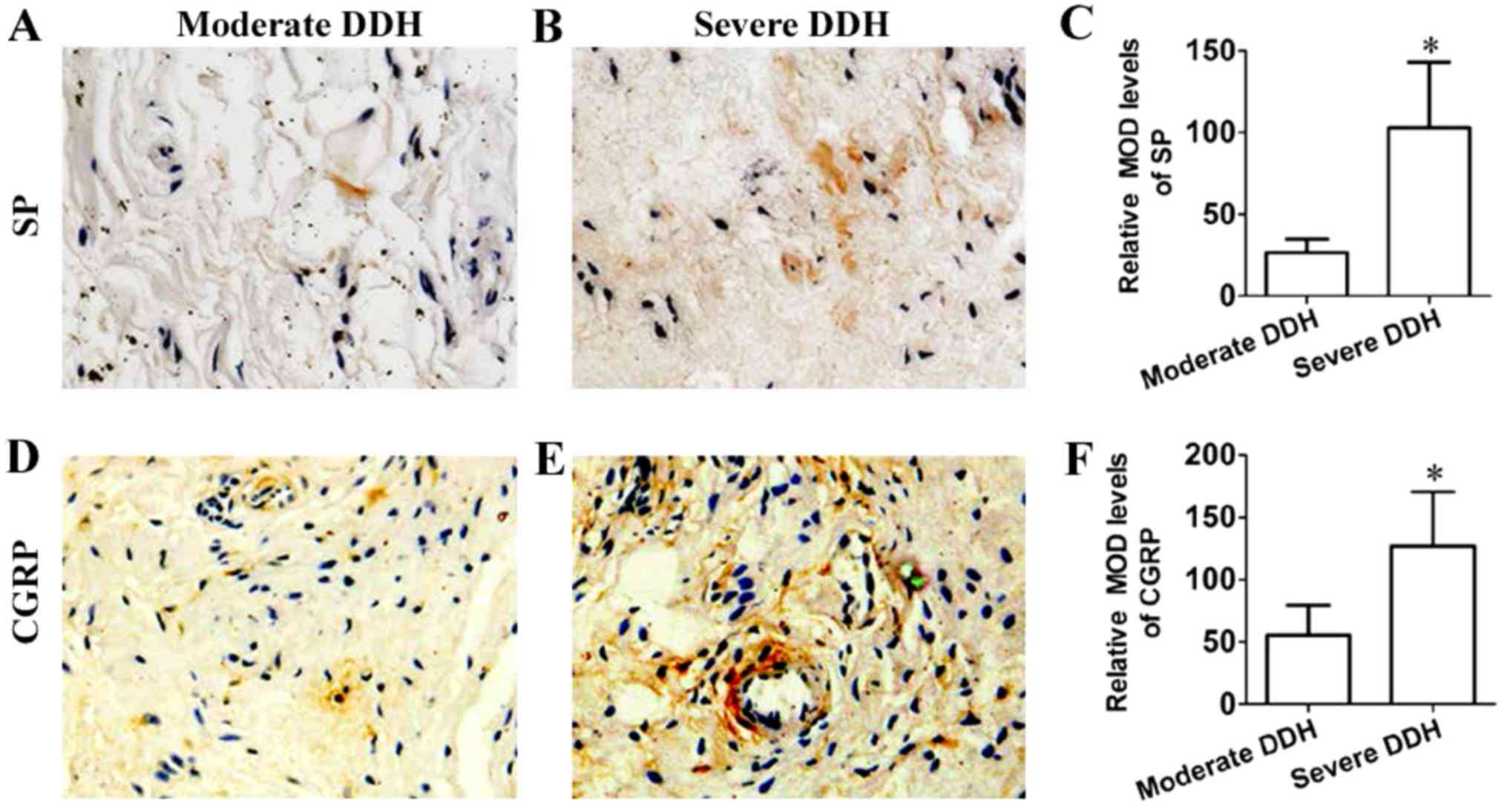 | Figure 6.(A-F) Immunohistochemical staining
and MOD analysis. (A, B, D and E) Immunohistochemical staining of
SP, CGRP in synovium between moderate and severe DDH group. (A, B,
D and E) Magnification: ×400. (C and F) Comparisons of MOD levels
of SP, CGRP in immunohistochemical staining between different
groups. *P<0.05 compared with moderate DDH. MOD, mean optical
density; DDH, developmental dysplasia of the hip; SP, substance P;
CGRP, calcitonin gene-related peptide. |
Comparisons of MOD levels of each targets between
moderate DDH and severe DDH. The results of MOD analysis,
particularly those performed on CD68 (Fig. 2C), NF-200 (Fig. 3C), vimentin (Fig. 3F), CD45 (Fig. 4C), CD20 (Fig. 4F), α-SMA (Fig. 5F), SP (Fig. 6C), and CGRP (Fig. 6F), presented increase in severe DDH
and not in moderate DDH, and these results coincided with the
results of the comparisons among the targets in IHC. However, mast
cell tryptase (Fig. 5C),
indicators of mast cell, presented significant decreased MOD levels
in synovial of severe DDH compared with that in moderate DDH. And,
the MOD levels of CD3 and MIB1 in these groups revealed
approximative results with no significant difference (Fig. 2F and Fig. 5I). In addition, the presence of
labeled cells is documented and tabulated in Table II.
Correlation tests of MOD levels of each antibody
with Harris hip score (HHS) and visual analogue score (VAS) in
patients between different groups. In correlation detection
(Table III), significant
correlations were observed in moderate DDH: CD45/VAS: r=0.555,
P<0.01; Vimentin/HHS: r=−0.368, P<0.01; MCT/VAS: r=0.571,
P<0.01. The following correlations were observed in Severe DDH
group: CD68/HHS: r=−0.669, P<0.01; NF-200/VAS: r=0.421,
P<0.01; CD68/VAS: r=0.518, P<0.01; α-SMA/HHS: r=−0.541,
P<0.01; Vimentin/HHS: r=0.479, P<0.01. Additionally,
neuropeptides: SP/VAS: r=0.433, P<0.01; CGRP/VAS: r=0.455,
P<0.01 were also observed in the severe DDH group.
| Table III.Correlation analysis of MOD levels of
each antibody with HHS and VAS. |
Table III.
Correlation analysis of MOD levels of
each antibody with HHS and VAS.
|
| Moderate DDH | Severe DDH |
|---|
|
|
|
|
|---|
|
| vs. HHS | vs. VAS | vs. HHS | vs. VAS |
|---|
|
|
|
|
|
|
|---|
| Antibody | R | P | R | P | R | P | R | P |
|---|
| Inflammatory
cells |
|
|
|
|
|
|
|
|
|
CD3 | 0.010 | 0.945 | 0.187 | 0.219 | −0.234 | 0.176 | 0.276 | 0.109 |
|
CD20 | −0.351 | 0.018 | 0.279 | 0.064 | −0.394 | 0.019 | 0.378 | 0.025 |
|
CD45 | −0.449 | 0.012 | 0.555 |
<0.001a | −0.101 | 0.564 | 0.233 | 0.178 |
|
CD68 | −0.453 | 0.018 | 0.239 | 0.113 | −0.669 |
<0.001a | 0.518 | 0.001a |
|
NF-200 | −0.122 | 0.425 | 0.349 | 0.029 | −0.167 | 0.339 | 0.421 | 0.009a |
|
α-SMA | −0.208 | 0.169 | 0.212 | 0.163 | −0.541 | 0.005a | 0.241 | 0.164 |
|
MIB1 | 0.141 | 0.356 | 0.193 | 0.205 | 0.063 | 0.721 | 0.265 | 0.124 |
|
Vimentin | −0.368 | 0.003a | 0.234 | 0.123 | 0.479 | 0.004a | −0.015 | 0.933 |
| Mast
cell tryptase | −0.209 | 0.166 | 0.571 |
<0.001a | −0.344 | 0.043 | 0.062 | 0.725 |
| Neuropeptides |
|
|
|
|
|
|
|
|
| SP | −0.091 | 0.551 | 0.208 | 0.171 | −0.349 | 0.039 | 0.433 | 0.009a |
|
CGRP | −0.059 | 0.697 | 0.237 | 0.117 | −0.333 | 0.051 | 0.455 | 0.006a |
Discussion
DDH is a major predisposing factor for hip OA and
can be caused by improper loadings on hip joints. Owing to this
reason, normal load-bearing regions in dysplasia hips, particularly
articular cartilage, labrum, and synovium, are subjected to
alterative mechanical overload. Among these components, the
synovium in the hip joint has been widely acknowledged as the
inflammation origin and an initial factor of arthritis progression
in OA (22,23). Therefore, considering the abnormal
mechanical environment of synovium from DDH, we deemed
investigating the biological appearance of synovium from DDH in
vivo necessary.
Although the application of IHC method in pain
research in vivo has been widely acknowledged (24,25),
limited progress has been made in identifying the mechanisms of
inflammatory progress of hip joint, especially the pathological
changes in the synovial layer. Thus, the most significant aspect in
this study was the use of IHC for hip joint synovium and the
exploration of pathological changes in the synovium of DDH, which
are useful in detecting the mechanism of progression from moderate
to severe DDH. In this study, patients with DDH were divided into
two groups (moderate and severe DDH) to investigate the differences
of pathophysiological process and inflammatory conditions between
these groups in the development from moderate to severe DDH. In
clinical practice, we observed that the durations of severe DDH is
shorter than that of moderate DDH. As we know, the patients with
severe DDH cannot tolerate the inconvenience caused by joint
dysfunction. Therefore, the patients will resort to surgery as
early as possible to improve hip function and relieve pain. It
seemed to us that there might be advantages in an earlier surgical
treatment.
The results of the histological analysis revealed an
upgrade of inflammatory infiltration into the synovium, which was
confirmed by IHC using a variety of antibodies. Analysis with CD3,
CD20, CD45, CD68, and mast cell tryptase antibodies identified
these cells to be predominantly T cells, B cells, leukocytes,
macrophages, and mast cells, indicating it to be a chronic
inflammatory cell infiltration. Among these, the MOD levels of
CD45, mast cell tryptase, and CD68 showed significant correlations
with VAS in moderate and severe DDH separately, which illustrate
the infiltration of leukocytes, macrophage, and mast cells might be
associated with the pain sensation of hip joint in DDH. Similarly,
the MOD levels of vimentin, α-SMA, and CD68 also presented
significant negative correlations with HHS separately, which means
the infiltration of fibroblast, myofibroblast, and macrophage
probably contribute to the disorders of hip joint in the
development of DDH.
The results of IHC also demonstrate the remarkable
up-regulation of SP, CGRP, and NF-200 in synovium from severe DDH
cases. But, no such remarkable up-regulation was observed in
moderate DDH cases. This process shows the increasing infiltration
of free nerve endings into the synovium during the process from
moderate DDH to severe DDH. Moreover, the MOD levels of NF-200, SP
and CGRP revealed positive correlation with VAS in patients with
severe DDH, and such correlation emphasizes the crucial roles of
free nerve endings and neuropeptides in the sensation of pain.
Previous studies proved that with the stimuli of peripheral pain,
SP and CGRP were increasingly synthesized in dorsal root ganglion
(DRG) then secreted by peripheral sensory nerve endings (26). Basing on our findings, we speculate
that with the time and duration of DDH, cartilage wearing degree
will gradually increase, and the cushion capacity of cartilage
progressively disappears. Therefore, the subchondral bone and
labrum tissue bear increasing shear and compressive loadings as the
cartilage abrasion evolves. During this process, the afferent
stimulation of joint pain gradually increases, and this increase in
turn induce the infiltration of peripheral nerve fibers (NF-200)
and is accompanied by the release of additional neuropeptides (SP
and CGRP) from the DRG.
As emphasized in our previous studies, SP and CGRP
might have the pro-inflammatory effect on synoviocyte from DDH
through the activation of NF-κB (16). Moreover, according to previous
studies, the activation of NF-κB in synoviocyte could induce the
release of chemokines, matrix metalloproteinases-1 (MMP-1), MMP-3
and interleukins-6 (IL-6) (27,28).
Among these, chemokines such as monocyte chemotactic protein-1
(MCP-1) and macrophage inflammatory protein-1 (MIP-1β) are
entrusted with the task of recruiting macrophage as well as other
monocytes for involvement in the inflammatory process of synovium.
Hence, we speculate that the abrasion of cartilage might stimulate
the release of SP and CGRP from the nerve fibers to the synovial
tissues during the progress of DDH, and this condition can
aggravate the degeneration of cartilage in DDH by recruiting
macrophages and other inflammatory effector cells from peripheral
blood. Moreover, these inflammatory effector cells can secrete a
series of harmful cytokines (MMPs and ILs etc.), which can further
accelerate the destruction of the cartilage of DDH.
Synovial fibrosis in DDH was explored by the
positive staining of α-SMA (myofibroblast) and vimentin
(fibroblast) in the synovium. Previous research reported the
extracellular matrix (ECM) exocrine function and biological
activity of myofibroblast. As the indicator of vascular smooth
muscle and angiogenesis, the appearance of myofibroblast was
acknowledged indispensable in fibrosis and chronic inflammation
(29,30). Fibroblast dedicates autonomous
contributions in the inflammatory process as effector cells
releasing pro-inflammatory mediators and undertaking antigen
presenting effect by expressing MHC-II and auto-antigens to
specific T cell hybridomas (31–34).
Thus, in this study, the increasing IHC staining of α-SMA and
vimentin in synovium combined with the positive correlations of
these targets with HHS and VAS imply the existence of fibrosis in
synovium and its harm to joint motion.
Moreover, as a hallmark of OA, synovial fibrosis is
characterized by fibroblast proliferation and imbalance between
collagen synthesis and catabolism (35). This imbalance results in the
excessive deposition of collagen into ECM leading to thickening and
stiffening of the synovial membrane, which is believed to be a
major contributor to joint pain and stiffness. This basic theory
has been verified by the positive correlations of these fibrosis
elements (α-SMA and vimentin) with clinic indexes (HHS). Therefore,
these synovial fibrosis related indexes could be promising therapy
targets, which probably help to reduce fibrosis and stiffness of
hip joint in DDH.
The current understanding of the involvement of mast
cells in inflammation included leukocyte recruitment and
activation, angiogenesis, fibroblast proliferation, matrix
remodeling, and injury to collagen and bone (36,37).
Herein, the presence of mast cells in synovium in this study makes
us speculate the involvement of mast cells in both chronic
inflammation and synovium fibrosis, which probably lead to
secondary injury and destruction of cartilage. By its pivotal
position in the inflammatory process, the mast cells may also hold
promise as a treatment target to relieve the inflammatory progress
of arthritis in DDH.
The biopsy material from the synovia of patients
with DDH with different stages revealed that this disorder is a
chronic inflammation and fibrotic condition. Together with the
presence of extensive angiogenesis and nerve fibers, this ascending
inflammation and fibrosis indicated from IHC in synovium probably
explains why the upgrade of DDH could combine with an increasingly
painful and stiff syndrome. Targeted prevention of synovial
inflammatory infiltration and fibrosis could relief the
degeneration of cartilage and restrain the progress of DDH.
Acknowledgements
Not applicable.
Funding
This study was supported by the National Natural
Science Foundation of Youth in China (grant nos. 81101381 and
81601866), Three-year planning for promoting clinical skills and
innovation in municipal hospitals by develop-center of Shanghai
Shenkang Hospital (grant no. 16CR2036B) and Foundation of Shanghai
Municipal Health Bureau (grant no. 20134002).
Availability of data and materials
The analyzed data sets generated during the study
are available from the corresponding author on reasonable
request.
Authors' contributions
DL participated in the design of the study, image
processing, and manuscript preparation and revision. HW performed
immunohistochemistry and revised the manuscript. JYH performed the
questionnaires of VAS and HHS. CLW and WJF participated in
immunohistochemistry and data statistical analysis. CS performed
statistical analysis and manuscript revision. JFZ participated in
the collection of synovial biopsies from patients. XDC and DLW
conceived the study, participated in its design and coordination,
and gave general supervision of the whole research group. All
authors have read and approved the final manuscript.
Ethics approval and consent to
participate
The implementation of this study was based on the
recommendations from the Declaration of Helsinki and was approved
by the ethical committee of Shanghai Jiaotong University School
Medicine Affiliate Xinhua Hospital (Approval no. XHEC-D-2013-009).
The samples obtained from the operations were prepared for testing
purposes only and with the approval and signed consent of the
patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
DDH
|
developmental dysplasia of the hip
|
|
CGRP
|
calcitonin gene-related peptide
|
|
SP
|
substance P
|
|
IHC
|
immunohistochemistry; Elisa
|
|
MMPs
|
matrix metalloproteinases
|
|
IL
|
interleukin
|
|
PAO
|
periacetabular osteotomy
|
|
THA
|
total hip arthroplasty
|
|
OA
|
osteoarthritis
|
|
MOD
|
mean optical density
|
|
HHS
|
harris hip score
|
|
VAS
|
visual analogue score
|
|
NF-200
|
Neurofilament-200
|
|
CDH
|
congenital dysplasia of the hip
|
|
ESR
|
erythrocyte sedimentation rate
|
|
CRP
|
C-reactive protein
|
|
CEA
|
centre edge angle
|
|
LCA
|
leukocyte common antigen
|
|
MIB1
|
mindbomb homolog 1
|
|
α-SMA
|
α smooth muscle actin
|
|
DRG
|
dorsal root ganglion
|
|
ECM
|
extracellular matrix
|
|
MCP-1
|
monocyte chemotactic protein-1
|
|
MIP-1β
|
macrophage inflammatory protein-1
|
|
MCT
|
mast cell tryptase
|
References
|
1
|
Lisle R, Boekelaar M, Stannage K and
Whitewood C: Delayed diagnosis of developmental dislocation of the
hip: The Western Australian experience. ANZ J Surg. 82:612–615.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Shi D, Dai J, Zhu P, Qin J, Zhu L, Zhu H,
Zhao B, Qiu X, Xu Z, Chen D, et al: Association of the D repeat
polymorphism in the ASPN gene with developmental dysplasia of the
hip: A case-control study in Han Chinese. Arthritis Res Ther.
13:R272011. View
Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sangal RB, Waryasz GR and Schiller JR:
Femoroacetabular impingement: A review of current concepts. R I Med
J (2013). 97:33–38. 2014.PubMed/NCBI
|
|
4
|
Alzaharani A, Bali K, Gudena R, Railton P,
Ponjevic D, Matyas JR and Powell JN: The innervation of the human
acetabular labrum and hip joint: An anatomic study. BMC
Musculoskelet Disord. 15:412014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Henak CR, Abraham CL, Anderson AE, Maas
SA, Ellis BJ, Peters CL and Weiss JA: Patient-specific analysis of
cartilage and labrum mechanics in human hips with acetabular
dysplasia. Osteoarthritis Cartilage. 22:210–217. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Haversath M, Hanke J, Landgraeber S,
Herten M, Zilkens C, Krauspe R and Jäger M: The distribution of
nociceptive innervation in the painful hip: A histological
investigation. Bone Joint J 95-B. 770–776. 2013. View Article : Google Scholar
|
|
7
|
Nakajima T, Ohtori S, Inoue G, Koshi T,
Yamamoto S, Nakamura J, Takahashi K and Harada Y: The
characteristics of dorsal-root ganglia and sensory innervation of
the hip in rats. J Bone Joint Surg Br. 90:254–257. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Henrotin Y, Lambert C and Richette P:
Importance of synovitis in osteoarthritis: Evidence for the use of
glycosaminoglycans against synovial inflammation. Semin Arthritis
Rheum. 43:579–587. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Henrotin Y, Pesesse L and Lambert C:
Targeting the synovial angiogenesis as a novel treatment approach
to osteoarthritis. Ther Adv Musculoskelet Dis. 6:20–34. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Shirai C, Ohtori S, Kishida S, Harada Y
and Moriya H: The pattern of distribution of PGP 9.5 and TNF-alpha
immunoreactive sensory nerve fibers in the labrum and synovium of
the human hip joint. Neurosci Lett. 450:18–22. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Takeshita M, Nakamura J, Ohtori S, Inoue
G, Orita S, Miyagi M, Ishikawa T and Takahashi K: Sensory
innervation and inflammatory cytokines in hypertrophic synovia
associated with pain transmission in osteoarthritis of the hip: A
case-control study. Rheumatology (Oxford). 51:1790–1795. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Beckmann J, Schubert J, Morhenn HG, Grau
V, Schnettler R and Lips KS: Expression of choline and
acetylcholine transporters in synovial tissue and cartilage of
patients with rheumatoid arthritis and osteoarthritis. Cell Tissue
Res. 359:465–477. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
de Lange-Brokaar BJ, Ioan-Facsinay A, van
Osch GJ, Zuurmond AM, Schoones J, Toes RE, Huizinga TW and
Kloppenburg M: Synovial inflammation, immune cells and their
cytokines in osteoarthritis: A review. Osteoarthritis Cartilage.
20:1484–1499. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kim YS, Kim JM, Lee YG, Hong OK, Kwon HS
and Ji JH: Intercellular adhesion molecule-1 (ICAM-1, CD54) is
increased in adhesive capsulitis. J Bone Joint Surg Am.
95:e181–e188. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hand GC, Athanasou NA, Matthews T and Carr
AJ: The pathology of frozen shoulder. J Bone Joint Surg Br.
89:928–932. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wang H, Zhang X, He JY, Zheng XF, Li D, Li
Z, Zhu JF, Shen C, Cai GQ and Chen XD: Increasing expression of
substance P and calcitonin gene-related peptide in synovial tissue
and fluid contribute to the progress of arthritis in developmental
dysplasia of the hip. Arthritis Res Ther. 17:42015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Crowe JF, Mani VJ and Ranawat CS: Total
hip replacement in congenital dislocation and dysplasia of the hip.
J Bone Joint Surg Am. 61:15–23. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hart DJ and Spector TD: The classification
and assessment of osteoarthritis. Baillieres Clin Rheumatol.
9:407–432. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cashman JP, Round J, Taylor G and Clarke
NM: The natural history of developmental dysplasia of the hip after
early supervised treatment in the Pavlik harness. A prospective,
longitudinal follow-up. J Bone Joint Surg Br. 84:418–425. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Nakamura S, Ninomiya S and Nakamura T:
Primary osteoarthritis of the hip joint in Japan. Clin Orthop Relat
Res. 190–196. 1989.PubMed/NCBI
|
|
21
|
Rondelet B, Kerbaul F, Motte S, van
Beneden R, Remmelink M, Brimioulle S, McEntee K, Wauthy P, Salmon
I, Ketelslegers JM and Naeije R: Bosentan for the prevention of
overcirculation-induced experimental pulmonary arterial
hypertension. Circulation. 107:1329–1335. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
O'Neill TW, Parkes MJ, Maricar N,
Marjanovic EJ, Hodgson R, Gait AD, Cootes TF, Hutchinson CE and
Felson DT: Synovial tissue volume: A treatment target in knee
osteoarthritis (OA). Ann Rheum Dis. 75:84–90. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Liu-Bryan R: Synovium and the innate
inflammatory network in osteoarthritis progression. Curr Rheumatol
Rep. 15:3232013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Adães S, Mendonça M, Santos TN,
Castro-Lopes JM, Ferreira-Gomes J and Neto FL: Intra-articular
injection of collagenase in the knee of rats as an alternative
model to study nociception associated with osteoarthritis.
Arthritis Res Ther. 16:R102014. View
Article : Google Scholar : PubMed/NCBI
|
|
25
|
Daghestani HN, Pieper CF and Kraus VB:
Soluble macrophage biomarkers indicate inflammatory phenotypes in
patients with knee osteoarthritis. Arthritis Rheumatol. 67:956–965.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Zhang RX, Ren K and Dubner R:
Osteoarthritis pain mechanisms: Basic studies in animal models.
Osteoarthritis Cartilage. 21:1308–1315. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Wakamatsu K, Nanki T, Miyasaka N, Umezawa
K and Kubota T: Effect of a small molecule inhibitor of nuclear
factor-kappaB nuclear translocation in a murine model of arthritis
and cultured human synovial cells. Arthritis Res Ther.
7:R1348–R1359. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
28
|
Laragione T and Gulko PS: Liver X receptor
regulates rheumatoid arthritis fibroblast-like synoviocyte
invasiveness, matrix metalloproteinase 2 activation, interleukin-6
and CXCL10. Mol Med. 18:1009–1017. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Mifková A, Kodet O, Szabo P, Kučera J,
Dvořánková B, André S, Koripelly G, Gabius HJ, Lehn JM and Smetana
K Jr: Synthetic polyamine BPA-C8 inhibits TGF-β1-mediated
conversion of human dermal fibroblast to myofibroblasts and
establishment of galectin-1-rich extracellular matrix in vitro.
Chembiochem. 15:1465–1470. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Minton K: Extracellular matrix:
Preconditioning the ECM for fibrosis. Nat Rev Mol Cell Biol.
15:766–767. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Shinde AV and Frangogiannis NG:
Fibroblasts in myocardial infarction: A role in inflammation and
repair. J Mol Cell Cardiol. 70:74–82. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Leech MT and Morand EF: Fibroblasts and
synovial immunity. Curr Opin Pharmacol. 13:565–569. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sobel K, Tham M, Stark HJ, Stammer H,
Prätzel-Wunder S, Bickenbach JR and Boukamp P: Wnt-3a-activated
human fibroblasts promote human keratinocyte proliferation and
matrix destruction. Int J Cancer. 136:2786–2798. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Kägebein D, Gutjahr M, Große C, Vogel AB,
Rödel J and Knittler MR: Chlamydia trachomatis-infected epithelial
cells and fibroblasts retain the ability to express
surface-presented major histocompatibility complex class I
molecules. Infect Immun. 82:993–1006. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Scanzello CR and Goldring SR: The role of
synovitis in osteoarthritis pathogenesis. Bone. 51:249–257. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Nigrovic PA and Lee DM: Synovial mast
cells: Role in acute and chronic arthritis. Immunol Rev. 217:19–37.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
da Silva EZ, Jamur MC and Oliver C: Mast
cell function: A new vision of an old cell. J Histochem Cytochem.
62:698–738. 2014. View Article : Google Scholar : PubMed/NCBI
|