Introduction
Cluster of differentiation (CD) 93 is a
transmembrane glycoprotein that is expressed in monocytes,
leukocytes and endothelial cells (1–3).
There are reports indicating an association between CD93 and
diseases of which inflammation is a fundamental characteristic,
such as asthma bronchitis (4,5), and
arthritis (3). As psoriasis is
characterised by chronic inflammation, the level of CD93 has been
shown to increase in psoriatic skin lesions (6). It has also been reported that in
patients with colorectal cancer, the level of CD93 is higher
compared to a normal reference population (7). An important association between CD93
and angiogenesis that might influence tumour growth has been
discussed in the literature (8).
In an interesting review by Khan et al (9), the authors also discuss the
relationship between CD93 and thrombomodulin, which has a central
position in the coagulation cascade. As CD93 and thrombomodulin
belong to the same transmembrane glycoprotein family, it is not
surprising to note the effects of thrombomodulin on inflammation,
which are similar to the effects influenced by CD93.
Cardiovascular diseases are among the most important
disease groups that occur in the Western population (10), with a high mortality. Inflammation
is one of the cornerstones in the development of ischaemic heart
disease (11–14). There has been information
indicating that single nucleotide polymorphisms (SNPs) from CD93
have an association with ischaemic heart disease; van der Net et
al (15) showed a 26%
increased risk for ischaemic heart disease with one specific
polymorphism of rs3746731 of CD93.
A soluble form of CD93 has been demonstrated
(1), and Youn et al
(16) reported increased levels of
this soluble form of CD93 in plasma from patients with myocardial
infarction, but also an association with adverse events and
mortality in those patients. This relation is important in the risk
evaluation of patients with ischaemic heart disease. However, in
the report from Youn et al (16), the sample sizes of the group
suffering from mortality were extremely small (all-cause mortality:
n=18; cardiovascular mortality; n=9); thus, the clinical
information is uncertain. Mälarstig et al (17) showed that the polymorphisms of
rs2749812 are associated with CD93 gene expression level in
human peripheral blood mononuclear cells (PBMCs).
Therefore, the aim of this study was to determine
whether the plasma concentration of CD93 and the polymorphism of
rs2749812 in CD93 were associated with well-known clinical
conditions, and mortality.
Materials and methods
Patient population
From a rural municipality in the south-east of
Sweden, a population of 470 individuals (men: 239, 50.9%; females:
230, 48.9%) with a median age of 76 years (interquartile range:18
years) were included in the study. All were part of a longitudinal
epidemiological project focusing on cardiovascular risk factors
among the elderly (18). The
participants in that project were invited to participate in the
present sub-study, with the first patient included on the 13th of
January 2003, and the last on the 28th of June 2005. The inclusion
criteria included all those living in a rural municipality aged
between 70 and 85 years. This was in order to minimise bias in the
selection process. The population that agreed to participate
delivered blood samples, and were given echocardiographic
examinations and an electrocardiogram (ECG). The New York Heart
Association functional class was evaluated by the including
physician based on the patient information.
All participants gave their written informed
consent, and the study was conducted in accordance with the
Declaration of Helsinki principles. The study protocol was approved
by the Regional Ethical Review Board of Linköping, Sweden (Dnr
95044). The mortality information was obtained from autopsy reports
or from the National Board of Health and Welfare in Sweden, which
registers all deaths.
Comorbidity
The following definitions have been used in this
study; hypertension was defined as a blood pressure of more than
140/90 mm Hg measured in the right arm with the patient in the
supine position after at least 30 min rest. Hypertension was also
assumed if the participant had previously been diagnosed with
hypertension and was receiving antihypertensive medication.
Diabetes mellitus was defined as a previous diagnosis with on-going
treatment, or a fasting blood glucose ≥7 mmol/l measured on one
single occasion. Ischaemic heart disease (IHD) was defined as a
history of angina pectoris/myocardial infarction or ECG-verified
myocardial infarction. Heart failure was defined as a previous
diagnosis with on-going treatment, or symptoms/signs of heart
failure and objective demonstration of reduced cardiac function in
terms of impaired cardiac function on echocardiography.
Cardiovascular death was defined as death caused by fatal
arrhythmias, myocardial infarction, heart failure, or
cerebrovascular insult.
For the methods in general we followed the methods
used in our previous publication (19).
Echocardiographic examinations
All echocardiography examinations were performed
using an Accuson XP-128c with the patient in a supine, left
position. Values for systolic function expressed as left
ventricular ejection fraction (EF), were categorised into four
classes with interclass limits of 30, 40 and 50%. Normal systolic
function was defined as EF≥50%. Thus, only the systolic function
was evaluated.
Determination of CD93 levels in
plasma
The blood samples were obtained while the patients
were at rest in a supine position, and all samples were collected
in pre-chilled plastic Vacutainer tubes (Terumo EDTA K-3). Plasma
was prepared by centrifugation at 3,000 × g for 10 min at 4°C. All
samples were stored at −70°C until analysis. None of the samples
was thawed more than twice. Determination of CD93 levels in plasma
was performed according to the recommendations (# DCD930, R&D
Systems Europe, Ltd.) and as previously described (7).
Genotype determination
DNA was isolated from peripheral blood using the
QIAmp DNA mini kit (Qiagen GmbH), following the manufacturer's
instructions. DNA (10 ng) was mixed with TaqMan Universal PCR
Master mix II and TaqMan SNP probes (Applied Biosystems; Thermo
Fisher Scientific, Inc.) and genotypes of SNPs rs2749812 were
analysed with the 7500 Fast Real-Time Polymerase Chain Reaction
(PCR) system with allelic discrimination according to the protocol
used in a previous publication (7).
Statistical analysis
Descriptive data are presented as percentages or
mean and standard deviation (SD). Comparative analyses were
performed using the Student's unpaired two-sided t-test, whereas
the Chi-square test was used for discrete variables, and ANOVA
analyses with Bonferroni post hoc tests were performed when
evaluating three or more groups with data on a nominal scale-level.
Both univariate and multivariate Cox proportional hazard regression
analyses were used to analyse the risk of mortality during the
follow-up period, where both all-cause mortality and cardiovascular
mortality were analysed. Kaplan-Meier evaluation which by
definition includes a log-rank test was used to illustrate
cardiovascular mortality as a function of follow-up time. Censored
patients were those who were still alive at the end of the study
period or who had died. Completed patients comprised those who had
died. In the multivariate regression model, adjustments were made
for the following co-variates: Age, IHD, hypertension, diabetes,
New York Heart Association functional class III, angiotensin
converting enzyme (ACE) inhibitors/Angiotensin receptor blockers,
beta-blockers, diuretics, and Hb <120 g/l.
A P-value <0.05 was considered statistically
significant. All data were analysed using standard software
packages (Statistica v. 13.2, Statsoft Inc, Tulsa, OK, USA).
Results
Study population characteristics
The basal characteristics of the three genotypes in
the total study population, divided into the two sexes, are
presented in Table I. From the
table, it can be noted that the population was a representative
elderly Western population, and it can be seen that in the total
study population only a small proportion, 3.6%, had the A/A
genotype. As regards the other two genotypes, 32.3% had the A/G
genotype, and 64% had the G/G genotype. Due to the small size of
the A/A genotype, considerable uncertainty would appear in
statistical evaluations of this genotype in comparison with the
other two. We therefore decided not to perform any risk evaluations
on those with the A/A genotype, but only on those with the A/G and
the G/G genotypes.
 | Table I.Basal characteristics of the study
population divided by genotypes. |
Table I.
Basal characteristics of the study
population divided by genotypes.
|
| Total population |
|
|---|
|
|
|
|
|---|
| Variable | A/A | A/G | G/G | P-value |
|---|
| Number | 17 | 152 | 301 |
|
| Age (years), mean
(SD) | 77.5 (3.7) | 77.0 (3.3) | 77.0 (3.5) |
|
| HT, n (%) | 12 (70.6) | 123 (80.9) | 219 (72.8) | 0.15 |
| IHD, n (%) | 2 (11.8) | 32 (21.1) | 68 (22.6) | 0.56 |
| Diabetes, n (%) | 4 (23.5) | 47 (30.9) | 102 (33.9) | 0.59 |
| NYHA III, n (%) | 5 (29.4) | 31 (20.4) | 59 (19.6) | 0.62 |
| AF, n (%) | 2 (11.8) | 15 (9.9) | 31 (10.3) | 0.97 |
| EF <40%, n
(%) | 1 (5.9) | 7 (4.6) | 28 (9.3) | 0.20 |
| ACEI/ARB, n (%) | 5 (39.4) | 47 (30.9) | 69 (22.9) | 0.17 |
| BB, n (%) | 2 (11.8) | 63 (41.4) | 101 (33.6) | 0.03 |
| Diuretics, n (%) | 7 (41.2) | 59 (38.8) | 106 (35.2) | 0.70 |
| Hb <120 g/l, n
(%) | 0 (0.0) | 20 (13.2) | 31 (10.3) | 0.36 |
| NT-proBNP (µg/l),
mean (SD) | 144.9 (157.0) | 167.6 (178.3) | 199.2 (380.0) | 0.54 |
| eGFR <60 ml/min, n
(%) | 7 (43.8) | 79 (52.0) | 142 (47.2) | 0.58 |
| BMI, mean (SD) | 27.6 (3.00) | 27.2 (3.9) | 27.2 (4.51) | 0.91 |
From Table I, it
can be seen that the population represents an elderly population as
generally found in the Western hemisphere, with a majority having
hypertension, and thus being treated with ACE
inhibitors/angiotensin receptor blockers or beta-blockers, while
around 20% suffered from IHD, and around 30% suffered from
diabetes. No significant differences regarding the basal
characteristics could be seen comparing the A/G and the G/G
genotypes.
During the follow-up period of 6.7 years, 106 cases
of all-cause mortality (22.6%), and 61 cases of cardiovascular
mortality (13%) were registered.
Plasma concentration and comorbidity
or mortality
In the study population 457 individuals were
evaluated regarding the plasma concentration of CD93 rs2749812. The
results of the plasma concentration were distributed into
quartiles, and clinical variables well-known to influence
cardiovascular (CV) prognosis as well as mortality were evaluated
in relation to the plasma concentration of CD93 (Table II). From this analysis it could be
seen that there was a higher plasma concentration of the cardiac
natriuretic peptide NT-proBNP in the fourth quartile (P=0.03).
However, as the number of groups evaluated was high, there was a
risk of missing significant differences between two groups when
performing significant tests of all groups. We therefore also
evaluated the quartiles with the lowest versus the highest plasma
concentration of CD93.
| Table II.Basal characteristics of the study
population divided into quartiles according to plasma concentration
of IL-32. |
Table II.
Basal characteristics of the study
population divided into quartiles according to plasma concentration
of IL-32.
|
| Total population |
|
|---|
|
|
|
|
|---|
| Variable | Q1 | Q2 | Q3 | Q4 | P-value |
|---|
| Number | 115 | 114 | 114 | 114 |
|
| Age (years), mean
(SD) | 77.5 (3.7) | 77.0 (3.3) | 77.0 (3.5) | 76.8 (3.4) |
|
| HT, n (%) | 12 (70.6) | 123 (80.9) | 219 (72.8) | 94 (82.5) | 0.15 |
| IHD, n (%) | 2 (11.8) | 32 (21.1) | 68 (22.6) | 26 (22.8) | 0.56 |
| Diabetes, n
(%) | 4 (23.5) | 47 (30.9) | 102 (33.9) | 36 (31.6) | 0.59 |
| NYHA III, n
(%) | 5 (29.4) | 31 (20.4) | 59 (19.6) | 22 (19.3) | 0.62 |
| AF, n (%) | 2 (11.8) | 15 (9.9) | 31 (10.3) | 9 (7.9) | 0.97 |
| EF <40%, n
(%) | 1 (5.9) | 7 (4.6) | 28 (9.3) | 9 (7.9) | 0.20 |
| ACEI/ARB, n
(%) | 5 (39.4) | 47 (30.9) | 69 (22.9) | 38 (33.3) | 0.17 |
| BB, n (%) | 2 (11.8) | 63 (41.4) | 101 (33.6) | 47 (41.2) | 0.03 |
| Diuretics, n
(%) | 7 (41.2) | 59 (38.8) | 106 (35.2) | 54 (47.4) | 0.70 |
| Hb <120 g/l, n
(%) | 0 (0.0) | 20 (13.2) | 31 (10.3) | 16 (14.0) | 0.36 |
| NT-proBNP (µg/l),
mean (SD) | 144.9 (157.0) | 167.6 (178.3) | 199.2 (380.0) | 261.3 (513.2) | 0.03 |
| eGFR <60 ml/min,
n (%) | 7 (43.8) | 79 (52.0) | 142 (47.2) | 60 (52.6) | 0.58 |
| BMI, mean (SD) | 27.6 (3.0) | 27.2 (3.9) | 27.2 (4.5) | 27.0 (4.3) | 0.91 |
From this evaluation, it was demonstrated that in
the fourth quartile, significantly more patients with hypertension
could be found than in the first quartile (94/114 vs. 78/115;
χ2:6.55; P=0.011). Also, there was a borderline
difference in the number of those on treatment with ACE
inhibitors/Angiotensin II receptor blockers in the fourth quartile,
compared to those in the first quartile (38/114 vs. 25/115;
χ2:3.86; P=0.05). No difference in treatment with
beta-blockers could be seen. However, significantly more patients
in the fourth quartile were on treatment with diuretics, compared
to the first quartile (54/114 vs. 37/115; χ2:5.52;
P=0.019).
Also, evaluating data on renal function revealed a
significantly higher s-creatinine level in the fourth quartile of
CD93 rs2749812, as compared to those in the first quartile (mean
Q1: 87 µmol/l vs. Q4:94 µmol/l; t=3.70; P=0.0003). Use of the
Modification of Diet in Renal Disease (MDRD) Study equation for
renal function, an estimated glomerular function model, showed a
higher estimated glomerular function for those in the first
quartile, as compared to those in the fourth quartile (71.8 ml/min
vs. 66.0 ml/min; t=3.46; P=0.0006).
The total mortality over 6.7 years distributed into
several groups is presented in Table
III. From that, it can be seen that even if a numerical
difference in CV mortality between those in the first and fourth
quartiles is apparent; no significant difference is demonstrated.
However, when evaluating the all-cause mortality, a significantly
higher mortality can be found in the fourth quartile group,
compared with the first quartile group (χ2:4.34;
p=0.037).
| Table III.Distribution of mortality in the
highest vs. the lowest quartile groups of plasma concentration of
CD93 in the study population during 6.7 years of follow-up. |
Table III.
Distribution of mortality in the
highest vs. the lowest quartile groups of plasma concentration of
CD93 in the study population during 6.7 years of follow-up.
| Variable | Quartile 1 | Quartile 4 | P-value |
|---|
| CV-mortality,
n | 13/114 | 17/114 | 0.43 |
| Tumors, n |
9/114 | 15/114 | 0.20 |
| Infections, n | 0 |
3/114 |
|
| All-cause
mortality, n | 24/114 | 38/114 | χ2:
4.34; P=0.037 |
When applied in a multivariate model, the high
plasma concentration of CD93 exhibited independent prognostic
information regarding all-cause mortality (HR: 1.91; P=0.002; 95%
CI: 1.28–2.86) Table IV.
| Table IV.Cox proportional hazard regression
analysis evaluating risk of all-cause mortality in the study
population regarding CD93. |
Table IV.
Cox proportional hazard regression
analysis evaluating risk of all-cause mortality in the study
population regarding CD93.
| Variable | Hazard ratio | 95% confidence
interval | P-value |
|---|
| Diabetes | 1.46 | 0.99–2.17 | 0.06 |
| Hypertension | 1.21 | 0.76–1.95 | 0.42 |
| Ischemic heart
disease | 1.82 | 1.18–2.79 | 0.006 |
| eGFR <6
ml/min/1.73 | 1.58 | 1.05–2.36 | 0.03 |
| ACEI/ARB | 1.00 | 0.66–1.54 | 0.98 |
| Beta blockers | 0.92 | 0.61–1.39 | 0.70 |
| CD93 Q4 | 1.91 | 1.28–2.86 | 0.002 |
The plasma concentration was also evaluated in the
three genotypes A/A, A/G and G/G. From this, a significantly higher
plasma concentration of CD93 could be found in the A/G, compared
with the G/G genotype (314 ng/ml vs. 285 ng/ml; T: 2.59; P=0.01).
No significant differences could be seen in the other genotype
comparisons. However, by analysing the participants who had a
plasma concentration within the fourth quartile, and who had also
suffered a CV death (n=17), three out of 17 belonged to the A/G
genotype, and 13 out of 17 belonged to the G/G genotype. Thus,
there was a significantly higher CV risk for the G/G genotype also
in the highest quartile of plasma concentration of CD93.
Genotypes and mortality
Mortality was evaluated during the same time span
(6.7 years), where both all-cause, and CV mortality were
registered. From this evaluation, significant differences in CV
mortality could be demonstrated, but not in all-cause mortality
when comparing the two genotypes A/G and G/G (CV mortality: A/G:
11/152=7.2%; G/G: 47/301=15.6%; χ2: 6.24; P=0.013;
all-cause mortality; A/G: 30/152=19.7%; G/G: 70/301=23.3%;
P=0.39).
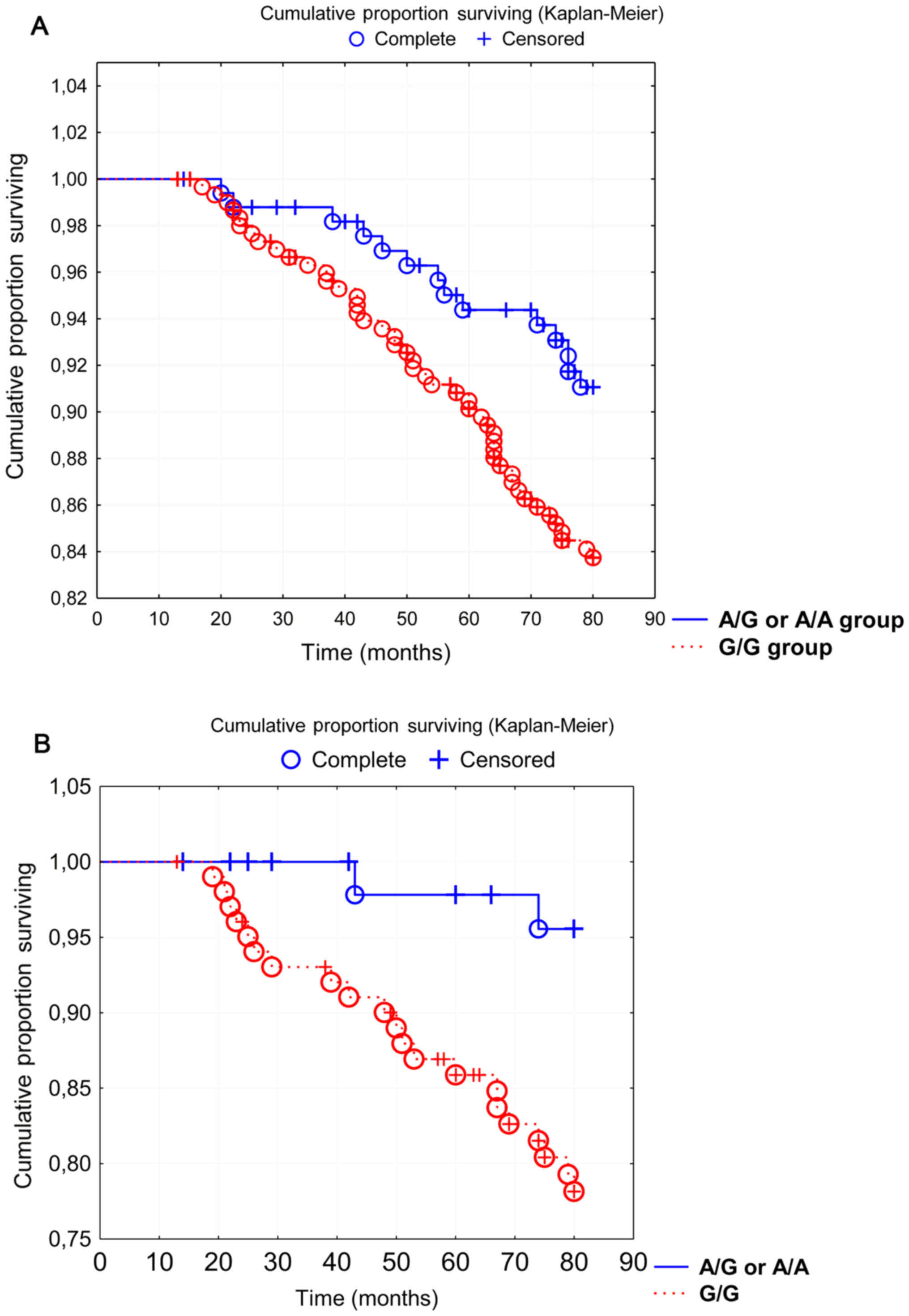
Applying a Kaplan-Meier graph of the CV mortality
during the follow-up period gave significantly higher mortality in
the G/G genotype (Z=2.23; P=0.026) (Fig. 1A).
By applying a risk evaluation of mortality using Cox
proportional hazard regression in a multivariate model, a
significantly higher CV mortality in the G/G genotype (Table V), but not in all-cause mortality
(Table VI) could be seen as
compared to the A/G genotype.
| Table V.Cox proportional hazard regression
analysis evaluating risk of cardiovascular mortality in the study
population regarding rs2749812 of CD93. |
Table V.
Cox proportional hazard regression
analysis evaluating risk of cardiovascular mortality in the study
population regarding rs2749812 of CD93.
|
| Total
population | Males | Females |
|---|
|
|
|
|
|
|---|
| Variable | HR | 95% CI | P-value | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age | 1.13 | 1.05–1.22 | 0.001 | 1.16 | 1.06–1.28 | 0.002 | 1.08 | 0.94–1.25 | 0.28 |
| IHD | 0.99 | 0.52–1.87 | 0.97 | 0.76 | 0.35–1.64 | 0.49 | 2.26 | 0.67–7.61 | 0.19 |
| Hypertension | 1.25 | 0.67–2.33 | 0.48 | 1.23 | 0.60–2.53 | 0.57 | 1.68 | 0.45–6.21 | 0.44 |
| Diabetes | 1.34 | 0.79–2.27 | 0.28 | 0.98 | 0.51–1.90 | 0.95 | 2.19 | 0.76–6.26 | 0.15 |
| NYHA III | 3.10 | 1.80–5.34 | <0.0001 | 4.00 | 2.08–7.69 | <0.0001 | 2.16 | 0.76–6.08 | 0.15 |
| ACEI/ARB | 1.04 | 0.58–1.87 | 0.89 | 1.30 | 0.63–2.69 | 0.47 | 0.99 | 0.35–2.86 | 0.99 |
| Beta blockers | 1.09 | 0.62–1.91 | 0.76 | 1.03 | 0.51–2.06 | 0.94 | 0.88 | 0.32–2.42 | 0.81 |
| Diuretics | 0.79 | 0.45–1.40 | 0.42 | 0.53 | 0.25–1.10 | 0.09 | 3.78 | 1.16–12.30 | 0.03 |
| Hb <120 g/l | 1.04 | 0.50–2.15 | 0.92 | 1.09 | 0.37–3.21 | 0.88 | 3.73 | 1.08–12.84 | 0.04 |
| Rs2749812 G/G | 1.96 | 1.07–3.57 | 0.03 | 2.21 | 1.11–4.42 | 0.02 | 7.08 | 1.31–38.42 | 0.02 |
| Table VI.Cox proportional hazard regression
analysis evaluating risk of all-cause mortality in the study
population regarding rs2749812 of CD93. |
Table VI.
Cox proportional hazard regression
analysis evaluating risk of all-cause mortality in the study
population regarding rs2749812 of CD93.
| Variable | HR | 95% CI | P-value |
|---|
| Age | 1.09 | 1.03–1.16 | 0.003 |
| IHD | 1.05 | 0.65–1.71 | 0.84 |
| Hypertension | 1.32 | 0.81–2.15 | 0.26 |
| Diabetes | 1.47 | 0.98–2.20 | 0.06 |
| NYHA III | 2.97 | 1.95–4.53 | <0.0001 |
| ACEI/ARB | 0.87 | 0.55–1.37 | 0.55 |
| Beta blockers | 1.08 | 0.70–1.65 | 0.73 |
| Diuretics | 0.93 | 0.61–1.43 | 0.74 |
| Hb <120 g/l | 0.83 | 0.45–1.53 | 0.54 |
| Rs2749812 G/G | 1.19 | 0.79–1.80 | 0.41 |
Dividing the population according to sex, a
significantly increased risk for the G/G genotype could be seen in
both sexes (Table V), with a
possible higher risk of the genotype among the females with a point
estimate of 7.08, compared to 2.21 in the male group; however,
there was a broad confidence interval, especially in the female
group.
In a sub-group analysis including the group with
diabetes, the same distribution among the three genotypes could be
seen (A/A: 2.6%; A/G: 30.5%; G/G: 66.2%). By applying the mortality
data, interesting results were obtained. Regarding CV mortality, a
significant difference between the A/G and the G/G groups could be
seen in those with diabetes (A/G: 2/47=4.3%; G/G: 21/102=20.6%;
χ2: 6.58; P=0.010); however, there was no significant
difference between the two groups in all-cause mortality (A/G:
9/47=19.1%; G/G: 32/102=31.4%; χ2: 2.41; P=0.12).
Fig. 1B shows the
results of applying the CV mortality data in a Kaplan-Meier graph,
where there is a significant difference in mortality between the
G/G and the A/G or A/A groups combined.
Applying the mortality data in a multivariate risk
model, where the CV mortality risk competes with several well-known
clinical risk factors, the G/G group still showed an increased
risk. The point estimate was high, HR: 5.2; however, as the
confidence interval was broad, the information should be
interpreted with caution (Table
VII).
| Table VII.Cox proportional hazard regression
analysis evaluating risk of cardiovascular mortality in the study
population with diabetes regarding rs2749812 of CD93. |
Table VII.
Cox proportional hazard regression
analysis evaluating risk of cardiovascular mortality in the study
population with diabetes regarding rs2749812 of CD93.
|
| Population with
diabetes |
|---|
|
|
|
|---|
| Variable | HR | 95%CI | P-value |
|---|
| Age | 1.14 | 0.99–1.30 | 0.07 |
| IHD | 1.92 | 0.63–5.82 | 0.25 |
| Hypertension | 1.37 | 0.52–3.62 | 0.52 |
| AECI/ARB | 0.76 | 0.30–1.94 | 0.57 |
| Beta blockers | 0.68 | 0.25–1.91 | 0.47 |
| Diuretics | 0.74 | 0.28–1.96 | 0.54 |
| Hb <120 g/l | 1.79 | 0.63–5.13 | 0.28 |
| NYHA III | 2.29 | 0.89–5.86 | 0.08 |
| CD93 rs2749812
G/G | 5.20 | 1.20–22.62 | 0.028 |
Discussion
In this study, significant differences could be
demonstrated in CV mortality between the G/G and the A/G genotypes,
with a higher risk in the G/G group. It is interesting to note that
in the study population an elderly community-living group of
persons were investigated, that is, all those aged 70 to 85 were
invited, and almost seven years of follow-up were applied. Even if
the median age at inclusion of the participants was high, 77 years,
significant differences in mortality could be demonstrated in the
G/G genotype.
Also, in the female group compared to the male
group, a tendency for a higher point estimate of the cardiovascular
risk by having the G/G genotype could be demonstrated. However, the
sample size was limited, and the confidence interval was wide, so
we interpret the result as indicating that both sexes having the
G/G genotype are exposed to a greater cardiovascular risk, and the
females might be exposed to the highest risk.
As patients with diagnosed diabetes are exposed to a
higher mortality risk in general, due to the diagnosis, the group
with diabetes was examined in a sub-group analysis. From the
results it could be seen that in this patient group the G/G
genotype group were also exposed to a higher cardiovascular risk
compared to the A/G group. No statistical evaluations of the A/A
group were performed, as the results would have suffered from a
high degree of uncertainty due to the small sample size. Taking
into consideration that the evaluation was performed in an elderly
patient group, where well-known diseases influencing mortality had
already occurred, the significant differences in mortality between
the genotypes could indicate that this effect still has important
prognostic information.
In the evaluation of a potential association between
the plasma concentration of CD93 and clinical conditions and
mortality, it could be demonstrated that in those with a higher
plasma concentration, a higher proportion of patients with
hypertension was found. Also, a higher proportion of patients on
treatment with ACE inhibitors/angiotensin receptor blockers could
be demonstrated in those with the higher plasma concentration of
CD93. This could imply that the same diseased population was
treated with pharmacotherapy. However, no difference in beta
blocker treatment between the two groups was demonstrated.
Finally, the mortality evaluations demonstrated a
higher all-cause mortality in those with a high concentration of
CD93. In this study, no statistical difference could be seen
regarding CV mortality; however, this could be an effect of the
sample size being too small to demonstrate a difference in this
variable. It could also indicate that besides the fact that it
appears that those with a higher plasma concentration of CD93 seem
to have more hypertension and poorer renal function, the end-result
appears to be increased mortality, which is interesting as this has
not been reported in the literature before.
The previously mentioned report on an association
between CD93 and IHD (15) is
based on SNPs of CD93 that are not identical to the one evaluated
in this report, rs2749812. However, Mälarstig et al
(17) were able to report that
those with the A allele of the same SNP exhibited a higher
expression of mRNA and the soluble form of CD93. This concurs with
the new and interesting results that we have presented in this
study. rs2749812 is located in exon 2 of CD93 and the mechanisms of
how the different genotypes affect mRNA expression and soluble CD93
protein are currently not known.
There can be arguments against the reliability of
the causes of death based on death certificates, as only 9.8% of
the deaths were followed by an autopsy. However a recent study
demonstrated a 55% accuracy of death certificates stating
cardiovascular diseases as a mortality reason in a Swedish
community (20). Therefore, we
believe that it is possible in this report to draw conclusions on
those who suffered cardiovascular mortality.
To validate the mortality results obtained, we
applied a three-step statistical procedure; after the Student
t-tests, we applied Kaplan-Meier evaluations, and finally a Cox
proportional hazard regression was employed. All evaluations
indicated results in the same direction, so we argue that in spite
of the small sample size the mortality information is correct.
From the literature it could be found that CD93 is
shed from neutrophils and monocytes during increased inflammatory
activity (2). In this study, those
that demonstrated an increased plasma concentration also had
conditions with increased inflammatory activity (hypertension,
impaired renal function); thus, the previous report concurs with
the results obtained here. In the literature, it has been suggested
that CD93 could be regarded as a candidate gene for atherosclerosis
based on its immunological activity (17,21).
Therefore, as health resources are increasingly under pressure and
society is calling for increased cost efficiency, the use of
biomarkers that could identify those at risk, and maybe even more
important, those at less risk, could be a way for the clinician to
optimise the individual handling of patients. Here evaluations of
genotypes, like those in CD93, could be an alternative, as
indicated from our results.
However, future research will be needed to discover
whether this glycoprotein could be one of the multitude of
potential biomarkers to identify risk patients for cardiovascular
disease and mortality.
The present study is based on a small study sample,
so the obtained results (point estimates, confidence intervals)
should be interpreted with caution. However, by applying different
types of evaluations, all pointing in the same direction, it seems
that the results add new and interesting information.
The study population had a limited age stratum, and
were already elderly at inclusion. This could limit the
interpretation into other age strata. The demonstrated data are
still of interest, even though it would have been even more
interesting to include a larger study sample with a greater age
span.
Finally, the included population consisted of a
homogenous Caucasian population, so we do not have information
regarding other populations.
In conclusion, in a healthy community-living
population of elderly persons, the plasma concentration of CD93 was
evaluated in relation to co-morbidities and mortality during a
follow-up period of 6.7 years. Those with the highest quartile
demonstrated a higher all-cause mortality, as compared to those
with a lower plasma concentration.
Evaluating the genotypes A/A, A/G and G/G of
rs2749812 of CD93 revealed a higher CV mortality in the G/G
genotype, which could be confirmed by risk evaluation using Cox
regressions. It seems that the female group demonstrated more
obvious genotype differences compared to the males.
Also, those with diabetes showed even greater
differences, indicating a higher risk for those with the G/G
genotype.
Therefore, the data indicate that CD93 could be used
in clinical situations in order to optimise the handling of
patients with ischaemic heart disease.
However, the obtained data, even though interesting,
should be regarded as hypothesis-generating, as the sample size was
limited, and thus interpretation should be carried out with
caution. It seems that more research in this interesting field is
needed.
Acknowledgements
Not applicable.
Funding
The present study was supported by grants from the
County Council of Östergötland, University of Linköping, Linköping,
Sweden, and the Swedish Heart and Lung Foundation.
Availability of data and materials
The datasets generated and/or analyzed during the
current study are not publicly available due to that under Swedish
Law, the authors cannot share the data underlying this study and
cannot do any further research than what is specified in the
ethical permissions application. For inquires on the data,
researchers should first reach out to the owner of the database,
the University of Linköping. Please reach out to the corresponding
author with requests and for assistance with data requests. If the
university approves the request, researchers can submit an
application to the Regional Ethical Review Board for the specific
research question that the researcher wants to examine.
Authors' contributions
UA and DW conceived and designed the experiments.
UA, LS and DW performed the experiments. UA and DW analyzed the
data. DW contributed reagents/material/analysis tools. UA and DW
wrote the manuscript. All authors read and approved final
manuscript.
Ethics approval and consent to
participate
All participants gave their written informed
consent, and have given written permission for publication of
obtained data, and the study was conducted in accordance with the
Declaration of Helsinki principles. The study protocol was approved
by the Regional Ethical Review Board of Linköping, Sweden (Dnr
95044).
Patient consent for publication
All participants have given their written permission
for publication of obtained data.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
CI
|
confidence interval
|
|
CV
|
cardiovascular
|
|
ECG
|
electrocardiogram
|
|
EF
|
ejection fraction
|
|
HR
|
hazard ratio
|
|
SD
|
standard deviation
|
References
|
1
|
Bohlson SS, Silva R, Fonseca MI and Tenner
AJ: CD93 is rapidly shed from the surface of human myeloid cells
and the soluble form is detected in human plasma. J Immunol.
175:1239–1247. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Greenlee MC, Sullivan SA and Bohlson SS:
Detection and characterization of soluble CD93 released during
inflammation. Inflamm Res. 58:909–919. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Jeon JW, Jung JG, Shin EC, Choi HI, Kim
HY, Cho ML, Kim SW, Jang YS, Sohn MH, Moon JH, et al: Soluble CD93
induces differentiation of monocytes and enhances TLR responses. J
Immunol. 185:4921–4927. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Park HJ, Han H, Lee SC, Son YW, Sim DW,
Park KH, Park YH, Jeong KY, Park JW and Lee JH: Soluble CD93 in
serum as a marker of allergic inflammation. Yonsei Med J.
58:598–603. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sigari N, Jalili A, Mahdawi L, Ghaderi E
and Shilan M: Soluble CD93 as a novel biomarker in asthma
exacerbation. Allergy Asthma Immunol Res. 8:461–465. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Duvetorp A, Slind Olsen R, Skarstedt M,
Söderman J and Seifert O: Psoriasis and pro-angiogenetic factor
CD93: Gene expression and association with gene polymorphism
suggests a role in disease pathogenesis. Acta Derm Venereol.
97:916–921. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Olsen RS, Lindh M, Vorkapic E, Andersson
RE, Zar N, Löfgren S, Dimberg J, Matussek A and Wågsäter D: CD93
gene polymorphism is associated with disseminated colorectal
cancer. Int J Colorectal Dis. 30:883–890. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Borah S, Vasudevan D and Swain RK: C-type
lectin family XIV members and angiogenesis. Oncol Lett.
18:3954–3962. 2019.PubMed/NCBI
|
|
9
|
Khan KA, McMurray JL, Mohammed F and
Bicknell R: C-type lectin domain group 14 proteins in vascular
biology, cancer and inflammation. FEBS J. 286:3299–3332. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
van der Ende MY, Hartman MH, Hagemeijer Y,
Meems LM, de Vries HS, Stolk RP, de Boer RA, Sijtsma A, van der
Meer P, Rienstra M and van der Harst P: The lifelines cohort study:
Prevalence and treatment of cardiovascular disease and risk
factors. Int J Cardiol. 228:495–500. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Nanchen D, Klingenberg R, Gencer B, Räber
L, Carballo D, von Eckardstein A, Windecker S, Rodondi N, Lüscher
TF, Mach F, et al: Inflammation during acute coronary
syndromes-risk of cardiovascular events and bleeding. Int J
Cardiol. 287:13–18. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Golia E, Limongelli G, Natale F, Fimiani
F, Maddaloni V, Pariggiano I, Bianchi R, Crisci M, D'Acierno L,
Giordano R, et al: Inflammation and cardiovascular disease: From
pathogenesis to therapeutic target. Curr Atheroscler Rep.
16:4352014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ndrepepa G: Myeloperoxidase-A bridge
linking inflammation and oxidative stress with cardiovascular
disease. Clin Chim Acta. 493:36–51. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kaplan RC and Frishman WH: Systemic
inflammation as a cardiovascular disease risk factor and as a
potential target for drug therapy. Heart Dis. 3:326–332. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
van der Net JB, Oosterveer DM, Versmissen
J, Defesche JC, Yazdanpanah M, Aouizerat BE, Steyerberg EW, Malloy
MJ, Pullinger CR, Kastelein JJ, et al: Replication study of 10
genetic polymorphisms associated with coronary heart disease in a
specific high-risk population with familial hypercholesterolemia.
Eur Heart J. 29:2195–2201. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Youn JC, Yu HT, Jeon JW, Lee HS, Jang Y,
Park YW, Park YB, Shin EC and Ha JW: Soluble CD93 levels in
patients with acute myocardial infarction and its implication on
clinical outcome. PLoS One. 9:e965382014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mälarstig A, Silveira A, Wågsäter D,
Öhrvik J, Bäcklund A, Samnegård A, Khademi M, Hellenius ML, Leander
K, Olsson T, et al: Plasma CD93 concentration is a potential novel
biomarker for coronary artery disease. J Intern Med. 270:229–236.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Alehagen U, Ericsson A and Dahlström U:
Are there any significant differences between females and males in
the management of heart failure? Gender aspects of an elderly
population with symptoms associated with heart failure. J Card
Fail. 15:501–507. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Alehagen U and Wågsäter D: Gender
difference and genetic variance in lipoprotein receptor-related
protein 1 is associated with mortality. Biomed Rep. 1:1–5.
2019.PubMed/NCBI
|
|
20
|
Eriksson A, Stenlund H, Ahlm K, Boman K,
Bygren LO, Johansson LA, Olofsson BO, Wall S and Weinehall L:
Accuracy of death certificates of cardiovascular disease in a
community intervention in Sweden. Scand J Public Health.
41:883–889. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Greenlee MC, Sullivan SA and Bohlson SS:
CD93 and related family members: Their role in innate immunity.
Curr Drug Targets. 9:130–138. 2008. View Article : Google Scholar : PubMed/NCBI
|