Introduction
Recurrent pregnancy loss (RPL) accounts for 1/3 of
all cases of miscarriages and is characterized by ≥2 consecutive
miscarriages occurring before week 20 of gestation (1,2). RPL
has been attributed to multiple risk factors, such as
anti-phospholipid antibody syndrome, infections and endocrine,
anatomic and genetic disorders. However, after comprehensive
assessments, the pathological trigger of >1/2 of RPL cases
remains unknown, although environmental factors and aged ovaries
were suspected to serve a role (3).
In addition, immune disorders, such as endometritis and
anti-phospholipid antibody syndrome, are also implicated in the
development of RPL (3–5).
Anxa5 protein is enriched in the placenta to prevent
coagulation (6). In the presence of
calcium, ANXA5 can bind to phosphatidylserine located on
upper surface of syncytiotrophoblasts in the placenta to prevent
clotting (6–8). Moreover, ANXA5 plays a critical
role in enhancing epithelial repair to maintain placental integrity
(9). It has been reported that the
activity of ANXA5 in placenta tissue samples harvested from
patients with RPL was notably reduced, along with inhibited
ANXA5 expression. The aforementioned results suggested that
a decreased protein expression level of Anxa5 increased RPL
risk.
Recently, four single nucleotide polymorphisms
(SNPs), including rs112782763, rs28717001, rs28651243 and
rs113588187, were discovered in the ANXA5 promoter via
functional and genetic assessments. The group of four minor alleles
corresponding to these four SNPs, rs112782763 (c.-467 GNA),
rs28717001 (c.-448 ANC), rs28651243 (c.-422 TNC) and rs113588187
(c.-373 GNA), was named haplotype M2 (a combination of SNPs of
19G/A, 1A/C, 27T/C and 76G/A) and it can be inherited (10). On the other hand, a group of two
alleles, c.-448 ANC and c.-422 TNC, was named haplotype M1 (a
combination of SNPs of 1A/C,27T/C). ANXA5 expression is
notably affected by the presence of the M2 haplotype. In addition,
the activity of the ANXA5 promoter carrying the M1 alleles
is higher than the activity of the ANXA5 promoter carrying
the M2 alleles (10,11). Another allele termed ‘N’ in the
ANXA5 promoter shows certain advantages over M1 and M2
alleles by expressing a higher level of anti-coagulation factors in
the villi of the placenta to decrease the susceptibility to
pre-eclampsia (10).
It has been reported that the ANXA5 variants
can affect RPL risks (12). In
addition, in a study of 70 RPL cases, the promoter and coding
sequences of ANXA5 showed various mutations, including the
loss of prothrombin G20210A mutation (10). Moreover, haplotypes M2 and M1 were
shown to affect RPL risks. The present study enrolled subjects with
or without RPL to study the effect of the haplotype located in the
promoter region of ANXA5, as well as enrolled another group
of patients with intrauterine fetus death (IUFD) to compared them
with RPL cases and controls.
Materials and methods
Human sample collection
All patients were recruited during their visits to
the Outpatient Department of Qilu Hospital (Jinan, China) from
December 2014 to November 2019. Based on their diagnosis, the
present study enrolled 235 patients showing symptoms of RPL into
the RPL group, 154 patients diagnosed with IUFD into the IUFD group
and 375 healthy control subjects free of RPL and IUFD were
recruited into the control group. The inclusion criteria were based
on the diagnosis of each patient with RPL or IUFD without any other
underlying health conditions. Patients who were diagnosed with
endometriosis, endometrial carcinoma, renal failure, cirrhosis,
cardiac failure or had an abortion with known reason, including
abnormal chromosomes, abnormal uterus structure or antiphospholipid
syndrome, were excluded from the present study. For the patients in
the control group, they were age-matched with the RPL cases and
they were free of any obstetrics/gynecology medical condition.
Peripheral blood samples and placenta tissue samples
were collected from each subject in the three groups. The clinical
features of the subjects in the RPL, IUFD and control groups were
analyzed, summarized and compared in Table I; the differences among the three
groups in terms of gravidity and parity were examined using the
Kruskal Wallis test.
 | Table I.Characteristics of the study
participants of RPL (n=235), IUFD (n=154) and control (n=375)
groups. |
Table I.
Characteristics of the study
participants of RPL (n=235), IUFD (n=154) and control (n=375)
groups.
| Characteristic | RPL | IUFD | Control | P-value |
|---|
| Age, years | 33 (24–47) | 31 (21–46) | 32 (26–46) | 0.0838 |
| Gravidity | 5 (3–11) | 4 (2–11) | 1 (1–3) | P<0.0001 |
| Parity | 0 (0–3) | 0 (0–2) | 1 (0–3) | P<0.0001 |
| No. of fetal
losses | 5 (1–8) | 6 (3–13) | – | 0.0778 |
| Weeks of early
fetal losses | 8 (5–17) | 9 (5–17) | – | 0.2501 |
| Weeks of late fetal
losses | 18 (10–22) | 16 (10–19) | – | 0.0835 |
The Human Research Ethics Committees of The Third
Affiliated Hospital of Wenzhou Medical University approved this
research (approval no. 153368XX06) and all methods were performed
in accordance with the last vision of the Declaration of Helsinki.
Written informed consent was obtained from all participants before
the initiation of this study.
Cell culture
Hs 815.Pl cells and HUVECs were originally purchased
from the American Type Culture Collection. These two cell lines, a
placenta osteosarcoma cell line (H 815.PI cells) and an umbilical
vein endothelial cell line (HUVECs), were utilized since they were
both appropriate models to study RPL (13). These cells were conventionally
cultured in MEM (Invitrogen; Thermo Fisher Scientific, Inc.)
supplemented with 10% (v/v) FCS (Sigma-Aldrich; Merck KGaA), 0.3
mg/ml glutamine, 100 µg/ml streptomycin, 100 U/ml penicillin and 1%
(v/v) sodium pyruvate, according to the instructions provided by
the supplier of the cells. Both cell types were cultured under
saturated humidity in a 37°C tissue culture incubator supplied with
5% of CO2. Prior to the start of cell culture
experiments, all cells were tested for the presence of
contaminations and only cells that passed the tests were selected
for cell culture. During the cell experiments, the cells were
randomly allocated into various groups for transfection, which are
detailed in the luciferase assay section.
Genotyping using a Taqman assay
To determine the genotypes of haplotypes located in
the promoter region of ANXA5, a Taqman genotyping assay kit
(Applied Biosystems; Thermo Fisher Scientific, Inc.) was used
according to the manufacturer's instructions to examined the
genotypes of the four SNPs located in the promoter region of
ANXA5, including rs112782763 SNP (c.-467), rs28717001 SNP
(c.-448), rs28651243 SNP (c.-422) and rs113588187 SNP (c.-373).
RNA isolation and reverse
transcription-quantitative (RT-q) PCR
The RNA of cultured cells and collected blood and
tissue samples was extracted using a RNeasy FFPE Assay Kit (Qiagen,
Inc.) based on the manufacturer's instructions. Total RNA was
reverse-transcribed into cDNA using the PrimeScript® RT
Reagent Kit (Takara Biotechnology Co., Ltd.) according to the
manufacturer's protocol. Subsequently, the relative expression of
ANXA5 was determined using an Assay On Demand assay kit
(Applied Biosystems; Thermo Fisher Scientific, Inc.) and Power SYBR
Green PCR Master Mix (Takara Bio, Inc.) on a PRISM 7300 real time
PCR machine (Applied Biosystems; Thermo Fisher Scientific, Inc.)
following the RT-qPCR conditions as below: 95°C for 10 min;
followed by 40 cycles of 95°C for 15 sec and 60°C for 60 sec. The
analysis of relative ANXA5 (forward primer,
5′-GTGGCTCTGATGAAACCCTCTC-3′ and reverse primer,
5′-GGCTCTCAGTTCTTCAGGTGTC-3′) expression was conducting using the
software equipped in the PRISM 7300 real time PCR machine and the
2−∆∆Cq (14) method.
GAPDH (forward primer, 5′-CAGCCTCAAGATCATCAGCA-3′ and reverse
primer, 5′-GGCATGGACTGTGGTCATGAG-3′) was used as the reference gene
to normalize the expression of ANXA5.
Luciferase assay
To determine the effects of various haplotypes on
the transcription efficiencies of the ANXA5 promoter, a
dual-luciferase reporter system based on the pcDNA 3.1 basic
luciferase reporter vectors (Promega Corporation) were constructed
to contain the M1 and M2 haplotypes of the ANXA5 promoter
(ranging from −300 bp to +300 bp). Renilla luciferase
reporter gene was used. Then, Hs 815.Pl cells and HUVECs were
seeded into 24-well tissue culture plates at a density of
5×105 cells/well and transfected with 300 ng of each of
the different vectors containing the M1 or M2 haplotype of the
ANXA5 promoter for 24 h at 4°C. At 48 h after the
initialization of the transfection, the luciferase activity of
different groups of cells was measured using a Bright-Glo™
Luciferase Assay System (Promega Corporation) to compare the
transcription efficiencies of the ANXA5 promoter harboring
various haplotypes with the luciferase activity of Renilla
as the normalization reference. All transfection operations were
carried out using the Fugene HD transfection reagent (Promega
Corporation). The luciferase signal was read using a microplate
reader (BMG; Molecular Devices LLC).
Western blot analysis
The protein content of cultured cells and collected
blood and tissue samples was extracted using RIPA buffer (cat. no.
R0278; Sigma-Aldrich; Merck KGaA). Subsequently, the protein
concentration was determined with a BCA assay kit. Then, the
protein content in each sample lysate was resolved using 10%
SDS-PAGE. Subsequently, the resolved protein in each sample lysate
was transferred onto a PVDF membrane, which was initially blocked
with 7% non-fat milk for 1 h at room temperature. Then, the
membranes were incubated consecutively with anti-Anxa5 (1:1,000;
cat. no. ab108321; Abcam) primary antibodies for 8 h at room
temperature and then an appropriate HRP-conjugated secondary
antibody 1:1,000; cat. no. 56970; Cell Signaling Technology, Inc.)
for 1 h at room temperature. After development using a Pierce™ ECL
Western Blotting Substrate (cat. no. 32109; Pierce; Thermo Fisher
Scientific, Inc.), the relative expression of Anxa5 protein was
calculated with the expression of β-actin (1:1,000; cat. no.
ab8226; Abcam) being used as the internal control.
Immunohistochemistry analysis
The tissue samples collected from the RPL, IUFD and
control groups were fixed for 15 min at room temperature in PBS
containing 10% neutral formalin and sliced into 5-µm thick tissue
slides to prepare paraffin-embedded specimens. Samples were blocked
in 10% goat serum (Thermo Fisher Scientific, Inc.) for 1 h at room
temperature, permeabilized for 1 h at room temperature with 0.1%
Triton X-100 (Sigma-Aldrich; Merck KGaA) and immunostained for 24 h
at 4°C with anti-Anxa5 monoclonal primary antibodies (1:100; cat.
no. ab108321; Abcam). After washing with PBS, the slides were
stained with the appropriate biotin-conjugated secondary antibodies
(1:1,000; cat. no. 39681; Cell Signaling Technology. Inc.) for 2 h
at room temperature, treated with DAB, counterstained with
hematoxylin for 30 min at room temperature and observed under a
fluorescence microscope (magnification, ×200).
Detection of Anxa5 activity using
ELISA
The activity of Anxa5 in the placenta tissue samples
collected from the RPL (n=28), IUFD (n=26) and control (n=32)
groups was determined using the Human ANXA5/Annexin V (Sandwich
ELISA) ELISA Kit (cat. no. LS-F21936; LifeSpan Biosciences, Inc.)
according to the manufacturer's instructions.
Statistical analysis
The clinical features of all recruited patients were
analyzed using a Kruskal Wallis test followed by Dunn's post hoc.
The associations between ANXA5 haplotypes and the risk of
RPL were determined using Fisher's exact test and logistic
regression. The other data obtained during this research were
analyzed using one-way ANOVA with Newman-Keuls test as the post hoc
test. Data are presented as the mean ± SD and the average of each
value was derived from three repeated experiments. All data
analysis was performed using SAS 9.0 software (SAS Institute, Inc.)
in conjunction with Microsoft Excel 2013 (Microsoft
Corporation).
To clarify the relationship between M2 and RPL, a
logistic regression model was built based on the corrected age,
gravidity and parity. The establishment and assessment of the
logistic regression model were carried out using SPSS 22.0 (IBM
Corp.). The intensity of immunochemistry staining was evaluated
using a Cox regression model with multiple variables. The sample
size was evaluated using Raosoft Sample Size Calculator (http://www.raosoft.com/samplesize.html;
version 2004; Raosoft, Inc.). Each experiment in this study was
repeated for three times. P<0.05 was considered to indicate a
statistically significant difference.
Results
Clinical features of RPL, IUFD and
control cases
Peripheral blood was collected from RPL and IUFD
cases, as well as from healthy control subjects. Their clinical
features were analyzed and are listed in Table I. It was found that the majority
(n=214) of women with RPL showed a history of early RPL, whereas 31
(13.1%) RPL cases had a history of both early and late episodes of
RPL. In the IUFD group, 95/154 (61.7%) subjects experienced IUFD.
Moreover, a significant difference was found between case and
control groups in terms of gravidity (Kruskal Wallis test,
P<0.001) and parity (Kruskal Wallis test, P<0.05), whereas no
significant differences were noted (P>0.05) in terms of age.
Association between the ANXA5 M2
haplotype and RPL
The genotype frequencies of haplotype M2 located in
the promoter of ANXA5 was further analyzed. The results are
summarized in Table II and
demonstrated that the rate of M2 haplotype in the control group (60
cases, 16%) was lower compared with that in the RPL group [71
cases, 30.2%; Fisher's exact test, P<0.0001; odds ratio (OR),
0.41; 95% CI, 0.28–0.62, RPL vs. control]. The incidence of the M2
haplotype in patients with IUFD was 22/154 (14%; Fisher's exact
test, P>0.05, IUFD vs. controls) and showed no difference with
the control group.
| Table II.Genotype frequencies of haplotypes in
the ANXA5 promoter in RPL, IUFD and control groups. |
Table II.
Genotype frequencies of haplotypes in
the ANXA5 promoter in RPL, IUFD and control groups.
| Index | RPL (n=235) | IUFD (n=154) | Control
(n=375) | RPL vs. Control
P-value | IUFD vs. Control
P-value |
|---|
| Genotypes |
|
|
| N/A | N/A |
|
N/N | 148 (63.0) | 125 (81.2) | 298 (79.5) | N/A | N/A |
|
N/M1 | 14 (6.0) | 7 (4.5) | 17 (4.5) | N/A | N/A |
|
M1/M1 | 0 | 0 | 0 | N/A | N/A |
| N/M2,
M1/M2a | 71 (30.2) | 22 (14.3) | 60 (16.0) | P<0.0001 | P>0.05 |
|
M2/M2 | 2 (0.8) | 0 | 0 | N/A | N/A |
| Total | 235 | 154 | 375 | N/A | N/A |
To clarify the relationship between M2 and RPL, a
logistic regression model was established based on the corrected
age, gravidity and parity. The results demonstrated that the M2
haplotype was significantly and independently associated with the
risk of RPL (P=0.047; OR, 3.1; 95% CI, 1.1–9.5; Table III).
| Table III.Logistics regression analysis of the
association between Annexin A5 haplotype and RPL/IUFD. |
Table III.
Logistics regression analysis of the
association between Annexin A5 haplotype and RPL/IUFD.
| Group | OR; 95% CI | P-value |
|---|
| RFL | 3.1;
(1.1–9.5) | 0.047 |
| IUFD | 1.31;
(0.7–2.3) | 0.250 |
Taken together, it was suggested that the M2
haplotype was involved in the risk of RPL as an independent risk
factor.
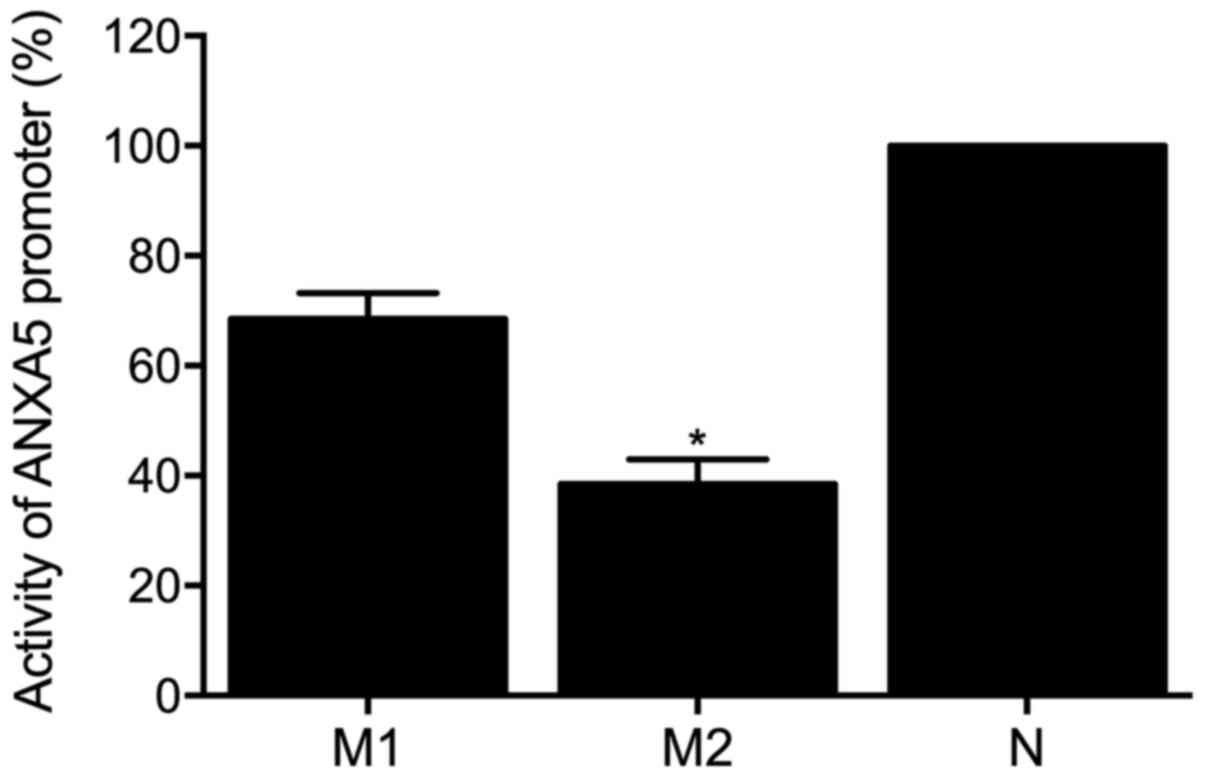
Effects of the M2 haplotype of ANXA5
on the ANXA5 promoter activity
To determine which haplotype is critical for
ANXA5 activity, luciferase assays were performed to detect
the effects of different ANXA5 haplotypes on the
transcription efficiency of ANXA5 promoter. The results
(Fig. 1) showed a reduction of
ANXA5 promoter activity in the presence of all four minor
alleles of the SNPs, i.e., the M2 haplotype. Furthermore, the M1
haplotype induced no significant change compared with the control
group.
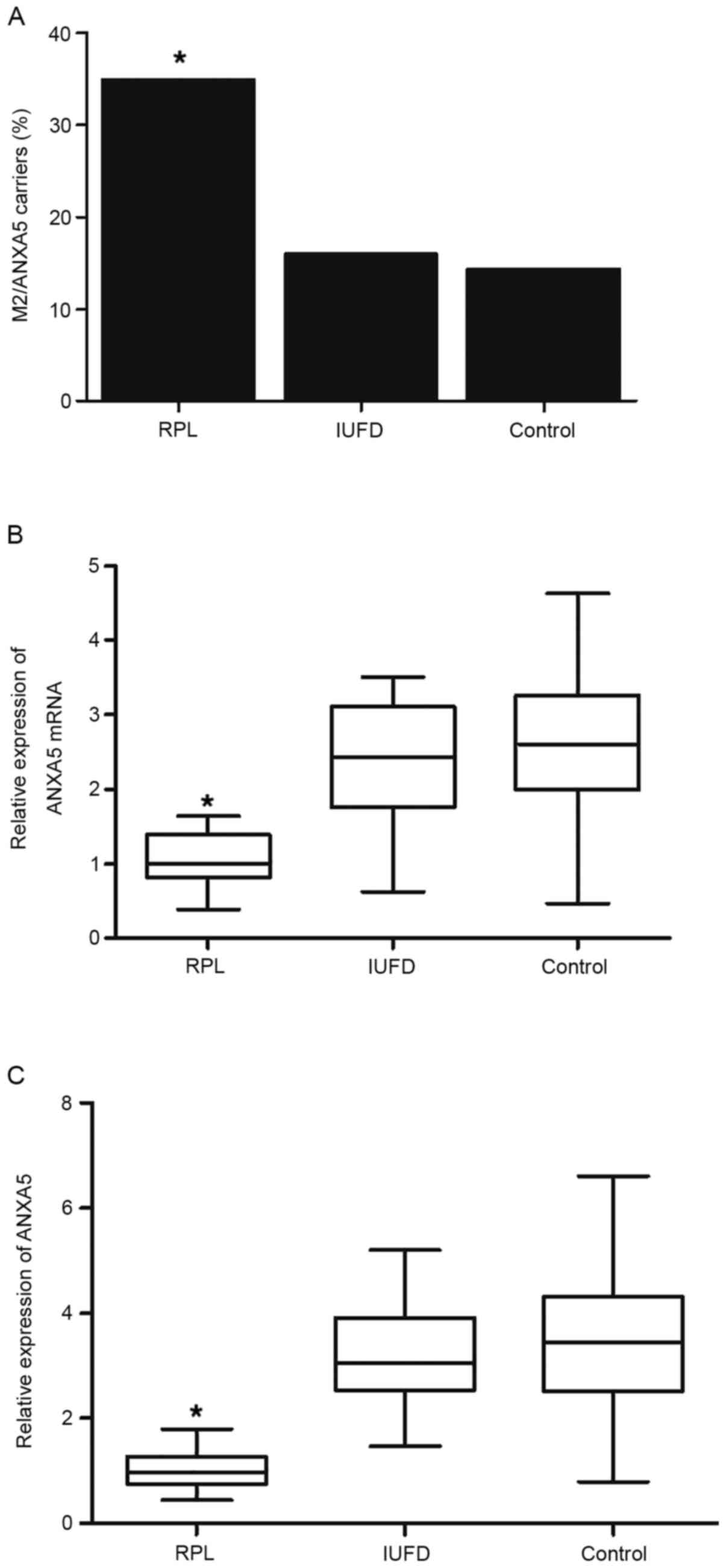
Placenta tissues were collected from RPL (n=28),
IUFD (n=26) and control (n=32) groups with one sample collected
from each patient to examine the effect of the M2 haplotype on the
risk of RPL. As shown in Fig. 2A,
10/28 (35.7%) of patients with RPL carried the M2 haplotype and the
rate was significantly higher compared with that in the control
(5/32, 15.6%) and IUFD (4/26, 15.4%) groups. The results of
statistical analysis with samples from RPL, IUFD and control groups
also showed a similar trend (Table
II).
Subsequently, the ANXA5 mRNA and Anxa5 protein
expression levels in the placenta tissue samples were determined
via RT-qPCR and western blotting. As shown in Fig. 2B, ANXA5 mRNA expression was
significantly decreased in patients with RPL compared with that in
the IUFD and control groups. Moreover, western blot analysis of
Anxa5 protein expression (representative blots shown in Fig. S1) demonstrated significantly
suppressed Anxa5 expression in patients with RPL compared with the
IUFD and control groups (Fig.
2C).
The expression level of Anxa5 protein in placental
tissues was further examined via immunohistochemistry. As shown in
Fig. 3, the protein expression
level of Anxa5 was decreased in the RPL group with compared with
the control and IUFD groups.
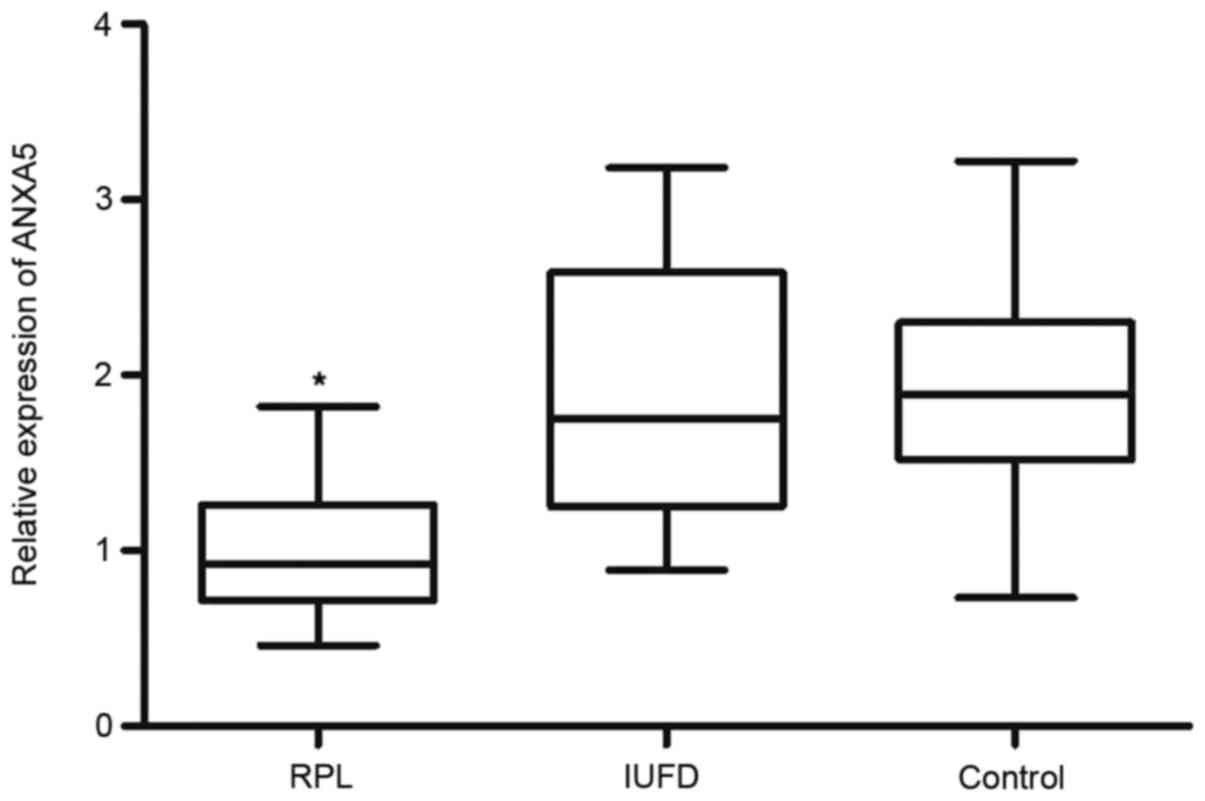
Next, peripheral blood samples were collected from
the three groups to assess their Anxa5 activity using ELISA. As
shown in Fig. 4, the activity of
Anxa5 was decreased in the RPL group compared with that in the
control and IUFD groups.
Taken together, these results suggested that the
ANXA5 M2 haplotype was essential for Anxa5 activity, which
was decreased in patients with RPL.
Discussion
The Anxa5 protein is highly expressed in the
placenta and can promote its anti-coagulant activity (15). In addition, a haplotype termed M2
located in the promoter of ANXA5 was shown to increase the
risk of RPL by reducing the expression of ANXA5 (10). In fact, Anxa5 proteins were shown to
generate a protective layer on the apical cell membrane of
syncytiotrophoblasts located in the villi of the placenta to
maintain a balance of hemostasis during pregnancy (16). The plasma expression of ANXA5
in healthy pregnant women is typically <5 ng/ml (17). However, a case controlled
comparative research on the plasma levels of ANXA5 in both healthy
pregnant women and patients with RPL showed a significantly
decreased level of circulating Anxa5 in RPL participants,
especially in those patients who have experienced ≥3 episodes of
RPL (18). It was also reported
that a combination of SNPs located in ANXA5 promoter, i.e.,
the M2 haplotype formed by four minor alleles of SNPs [SNP4: (−)373
G>A, SNP3: (−)422 T>C, SNP2: (−)448 A>C and SNP1: (−)467
G>A] located in chromosome 4q27, can promote the onset and
development of RPL, as well as other complications including
pre-eclampsia and thrombophilia or thromboembolism related to
pregnancy, presumably by reducing the expression of Anxa5 and by
increasing the coagulation in the placenta (10,19–23).
It was revealed that the transcription efficiency of the promoter
of ANXA5 harboring the M2 haplotype was reduced by ~60% when
compared with the transcription efficiency of the promoter of
ANXA5 harboring the N haplotype, i.e., the wild-type
haplotype of the promoter of ANXA5 (10). Moreover, both M2 and M1 haplotypes
can be frequently observed in the promoter of ANXA5
expressed in the healthy population (10). It was also demonstrated that the
promoter of ANXA5 harboring the M2 and M1 haplotypes showed
similar transcriptional efficiencies, in spite of the fact that the
M2 haplotype in the promoter of ANXA5 involves four SNPS,
i.e., rs112782763 (c.-467 GNA), rs28717001 (c.-448 ANC), rs28651243
(c.-422 TNC) and rs113588187 (c.-373 GNA), while the M1 haplotype
in the promoter of ANXA5 only involves two SNPS, i.e.,
c.-448 ANC and c.-422 TNC (10).
The present study collected peripheral blood samples from RPL, IUFD
and control groups to show that the incidence of M2 haplotype was
notably higher (35%) in patients with RPL. Next, a logistic
regression model was built based on corrected age, gravidity and
parity to show that the M2 haplotype was significantly and
independently associated with the risk of RPL.
Although it was previously reported that several
women with a history of RPL that could not be explained by
pathological diagnosis showed decreased Anxa5 expression, the
incidence of RPL induced by abnormal Anxa5 expression remains
unknown (18). The transcription
efficiency of the promoter of ANXA5 appears to be correlated
to the expression of IgG antibodies against domain I (24). At present, accumulating evidence
obtained from thrombo-elastography experiments and coagulation
assays has shown an increased level of coagulation activity in
patients with RPL (25,26). In women with RPL, the prevalence of
M2 haplotype is notably increased compared with that observed in
healthy controls (10). In
addition, M2 haplotype was detected in ~30% of RPL cases in a
Japanese population, while the incidence of M2 haplotype in healthy
controls of the Japanese population was <10% (27). Moreover, it was revealed that the M2
haplotype could be found in ~20% of residents in Europe, while the
M2 haplotype was found in >30% of European women suffering from
RPL (21,28). In addition, there is a close
relationship between the M2 haplotype and the occurrence of
pre-eclampsia and gestational disorders, while the susceptibility
to FGR is increased by M2 haplotype (29,30).
It has also been shown that the activity of ANXA5 promoter
in placental tissue samples harvested from patients with RPL was
markedly reduced to decrease Anxa5 expression, suggesting that the
M2 haplotype increased RPL risk by reducing the expression of Anxa5
(31). In the present study, the
luciferase assays demonstrated that the M2 haplotype was
responsible for the transcription efficiency of the ANXA5
promoter. In addition, the current results indicated that the rate
of the M2 haplotype was higher in patients with RPL. It was also
identified that the mRNA and protein expression levels of ANXA5 in
the placenta tissues were decreased in patients with RPL, and that
the activity of ANXA5 was decreased in this group.
The present study investigated the effect of the
ANXA5 haplotype on RPL, thereby providing a possible approach and
candidate biomarker for the prediction, diagnosis and prognosis of
RPL in future clinical applications. However, due to the limitation
of available cases in Qilu Hospital, the sample size was relatively
limited for the correlation analysis between haplotype and RPL
risk. The outcome of the statistical analysis may be different or
influenced by the different sample size. Moreover, the cases
recruited in the current study were all patients who attended Qilu
Hospital, which raised a potential selection bias since the
recruited cases may be suffering from other health complications.
In addition, an appropriate animal study to validate the current
finding is also necessary. Therefore, in future studies, to
validate the aforementioned finding, a larger sample size from the
general population, as well as animal studies, are necessary to
eliminate the potential selection bias generated during the process
of patient recruitment.
In conclusion, the present study demonstrated that
the M1/M2 haplotypes in ANXA5 were associated with an
increased risk of RPL. The results also indicated that ANXA5
expression was decreased in the carriers of the M2 haplotype.
Therefore, the presence of the M2 haplotype in ANXA5 may be
used as a novel biomarker to predict the prognosis of RPL, thus
providing a potential approach for the prediction of RPL risk in
future clinical applications.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The study was supported by Wenzhou Science and Technology Bureau
Project (grant no. Y20180276).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
ZC supervised the study and XD designed the study.
XZ, YC and FC collected the literature. ZC, XZ, YC and LC conducted
the experiments. FC and XD collected and analyzed the data. ZC and
XZ drafted the manuscript and XD revised the manuscript. ZC and XD
confirmed the authenticity of all the raw data. All authors have
approved the final version for publication.
Ethics approval and consent to
participate
The Human Research Ethics Committees of The Third
Affiliated Hospital of Wenzhou Medical University approved this
research (approval no. 153368XX06) and all methods were performed
in accordance with the last vision of the Declaration of Helsinki.
Written informed consent was obtained from all participants before
the initiation of this study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Rasmark Roepke E, Christiansen OB and
Hansson SR: Reliability of recurrent pregnancy loss diagnosis
coding in the Swedish National Patient Register: A validation
study. Clin Epidemiol. 11:375–381. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Larsen EC, Christiansen OB, Kolte AM and
Macklon N: New insights into mechanisms behind miscarriage. BMC
Med. 11:1542013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Practice Committee of American Society for
Reproductive Medicine, . Definitions of infertility and recurrent
pregnancy loss. Fertil Steril. 90 (Suppl 5):S602008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Practice Committee of the American Society
for Reproductive Medicine, . Evaluation and treatment of recurrent
pregnancy loss: A committee opinion. Fertil Steril. 98:1103–1111.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
McQueen DB, Bernardi LA and Stephenson MD:
Chronic endometritis in women with recurrent early pregnancy loss
and/or fetal demise. Fertil Steril. 101:1026–1030. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ueki H, Mizushina T, Laoharatchatathanin
T, Terashima R, Nishimura Y, Rieanrakwong D, Yonezawa T, Kurusu S,
Hasegawa Y, Brachvogel B, et al: Loss of maternal Annexin A5
increases the likelihood of placental platelet thrombosis and
foetal loss. Sci Rep. 2:8272012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Markoff A, Gerdes S, Feldner S, Bogdanova
N, Gerke V and Grandone E: Reduced allele specific annexin A5 mRNA
levels in placentas carrying the M2/ANXA5 allele. Placenta.
31:937–940. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rand JH and Wu XX: Antibody-mediated
interference with annexins in the antiphospholipid syndrome. Thromb
Res. 114:383–389. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bouter A, Carmeille R, Gounou C, Bouvet F,
Degrelle SA, Evain-Brion D and Brisson AR: Review: Annexin-A5 and
cell membrane repair. Placenta. 36 (Suppl 1):S43–S49. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bogdanova N, Horst J, Chlystun M, Croucher
PJ, Nebel A, Bohring A, Todorova A, Schreiber S, Gerke V, Krawczak
M and Markoff A: A common haplotype of the annexin A5 (ANXA5) gene
promoter is associated with recurrent pregnancy loss. Hum Mol
Genet. 16:573–578. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Rogenhofer N, Engels L, Bogdanova N,
Tüttelmann F, Markoff A and Thaler CJ: The haplotype M2 of the
ANXA5 gene is not associated with antitrophoblast antibodies. J
Assist Reprod Genet. 30:711–716. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Carcedo MT, Iglesias JM, Bances P, Morgan
RO and Fernandez MP: Functional analysis of the human annexin A5
gene promoter: A downstream DNA element and an upstream long
terminal repeat regulate transcription. Biochem J. 356:571–579.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wang Y, Liu HZ, Liu Y, Wang HJ, Pang WW
and Zhang JJ: Downregulated MALAT1 relates to recurrent pregnancy
loss via sponging miRNAs. Kaohsiung J Med Sci. 34:503–510. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gerke V, Creutz CE and Moss SE: Annexins:
Linking Ca2+ signalling to membrane dynamics. Nat Rev Mol Cell
Biol. 6:449–461. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kutteh WH and Hinote CD: Antiphospholipid
antibody syndrome. Obstet Gynecol Clin North Am. 41:113–132. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kutteh WH: Antiphospholipid antibody
syndrome and reproduction. Curr Opin Obstet Gynecol. 26:260–265.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rand JH, Arslan AA, Wu XX, Wein R,
Mulholland J, Shah M, van Heerde WL, Reutelingsperger CP, Lockwood
CJ and Kuczynski E: Reduction of circulating annexin A5 levels and
resistance to annexin A5 anticoagulant activity in women with
recurrent spontaneous pregnancy losses. Am J Obstet Gynecol.
194:182–188. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Dahm AE, Tiscia G, Holmgren A, Jacobsen
AF, Skretting G, Grandone E and Sandset PM: Genetic variations in
the annexin A5 gene and the risk of pregnancy-related venous
thrombosis. J Thromb Haemost. 13:409–413. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
de Jong PG, Hiddink L, Meijers JC,
Kiemeney LA, van Heerde WL and Middeldorp S: No association between
Annexin A5 genetic variants and deep venous thrombosis. Br J
Haematol. 169:301–304. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tiscia G, Colaizzo D, Chinni E, Pisanelli
D, Sciannamè N, Favuzzi G, Margaglione M and Grandone E: Haplotype
M2 in the annexin A5 (ANXA5) gene and the occurrence of obstetric
complications. Thromb Haemost. 102:309–313. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Grandone E, Tiscia G, Colaizzo D, Chinni
E, Pisanelli D, Bafunno V and Margaglione M: Role of the M2
haplotype within the annexin A5 gene in the occurrence of
pregnancy-related venous thromboembolism. Am J Obstet Gynecol.
203:461.e1–e5. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Miyamura H, Nishizawa H, Ota S, Suzuki M,
Inagaki A, Egusa H, Nishiyama S, Kato T, Pryor-Koishi K, Nakanishi
I, et al: Polymorphisms in the annexin A5 gene promoter in Japanese
women with recurrent pregnancy loss. Mol Hum Reprod. 17:447–452.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
de Laat B, Wu XX, van Lummel M, Derksen
RH, de Groot PG and Rand JH: Correlation between antiphospholipid
antibodies that recognize domain I of beta2-glycoprotein I and a
reduction in the anticoagulant activity of annexin A5. Blood.
109:1490–1494. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Rai R, Tuddenham E, Backos M, Jivraj S,
El'Gaddal S, Choy S, Cork B and Regan L: Thromboelastography,
whole-blood haemostasis and recurrent miscarriage. Hum Reprod.
18:2540–2543. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Romagnuolo I, Attanasio M, Cozzolino M,
Paladino E, Castaman G, Coccia ME and Fatini C: Thrombin potential
and traditional coagulation assay: Are they useful in exploring
recurrent pregnancy loss risk? Blood Coagul Fibrinolysis.
29:160–166. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Hiddink L, de Visser MC and van Heerde WL:
Polymorphisms in the Annexin A5 gene influence circulating Annexin
A5 levels in healthy controls. Thromb Res. 129:815–817. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Tüttelmann F, Ivanov P, Dietzel C,
Sofroniou A, Tsvyatkovska TM, Komsa-Penkova RS, Markoff A, Wieacker
P and Bogdanova N: Further insights into the role of the annexin A5
M2 haplotype as recurrent pregnancy loss factor, assessing timing
of miscarriage and partner risk. Fertil Steril. 100:1321–1325.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Tiscia G, Colaizzo D, Favuzzi G, Vergura
P, Martinelli P, Margaglione M and Grandone E: The M2 haplotype in
the ANXA5 gene is an independent risk factor for idiopathic
small-for-gestational age newborns. Mol Hum Reprod. 18:510–513.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chinni E, Tiscia GL, Colaizzo D, Vergura
P, Margaglione M and Grandone E: Annexin V expression in human
placenta is influenced by the carriership of the common haplotype
M2. Fertil Steril. 91:940–942. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lan Y, Wang J, Zhang Q, Yang X, Li L, Yin
J, Li H, Song X, Chen Z and Liu Y: Genetic variations and
haplotypes in the annexin A5 gene are associated with the risk of
recurrent pregnancy loss. J Cell Physiol. 234:18308–18316. 2019.
View Article : Google Scholar : PubMed/NCBI
|