Prostate cancer (PC) is one of the commonest cancer
types affecting men. It is the sixth cause of death worldwide with
359,000 cases in 2018 (1). The
discovery of the prostate specific antigen (PSA) together with
direct rectal examinations allowed the earlier detection of PC
(2). Steroids have been reported
as a modulating factor that changes the biochemical characteristics
of different tissues such as iris/ciliary body, aqueous outflow
pathway and sclera in the rabbit eye (3) and prostate tissue in human (3–5).
Testosterone and dihydrotestosterone (DHT) are the major classes of
sterols and sources for androgens in males. They pose a risk to PC
patients with higher levels of ‘free’ testosterone and a growth
hormone in their blood (6).
Steroidogenesis enzymes also have been related to modulation in
hormonal level and associated with related diseases (7–10).
Therefore, the hormonal biosynthesis pathway and their receptors
can be altered by genetic variations of the related genes altering
and contributing to individual susceptibility to PC (11,12). Androgen deprivation therapy (ADT)
is one of the standard care treatments in advanced and metastatic
cases, whether through testosterone reduction or antagonism of
their mechanism of action (13).
However, most patients respond well to the ADT, while some patients
still show recurrence and failure to therapy and proceed to
castration resistant PC (CRPC) (14). This resistance was referred to as
either synthesis of the intratumorally androgen from steroid
adrenal precursor or from synthesis of de novo cholesterol
(15).
A number of studies have focused on different
targets for steroid synthesis pathways such as P450 cytochromes of
CYP17 and CYP3A4, 5-alpha-reductase type-2 (SRD5A2) (16,17) and 3β-Hydroxysteroid dehydrogenase
(3BHSD) genes (18). The
3β-hydroxysteroid dehydrogenases (3β-HSD)/Δ4,5-isomerase is the
most important enzyme responsible for catalyzing the 3β-HSD
dehydrogenation and Δ4,5-isomerization of the Δ5-steroid precursors
into their corresponding Δ4-ketosteroids (19). The activity of this enzyme is
important for the synthesis of a number of steroidal hormones
including testosterone. 3β-HSD has two key isoenzymes designated as
type 1 and type 2 (20). Although
these two isoenzymes are encoded by two different genes, they are
93.5% homologous and located on chromosome 1p13.1 (21). The type 1 gene (HSD3B1) is the
most important isoenzyme and a rate-limiting enzyme required for
dihydrotestosterone synthesis (18), exclusively expressed in the
prostate tissue (20). By
contrast, the type 2 gene (HSD3B2) is predominantly expressed as
3β-HSD in the adrenal gland, ovary and testis. HSD3B1 converts DHT
to 3-α-diol which is metabolized further by uridine
diphosphate-glucuronosyltransferases (22). Excess biosynthesis of testosterone
is known to upregulate MMP-2 and/or MMP-9 in a number of tissues
including prostate (23,24). A number of studies propose a
mechanism of association between androgen level, MMPs and PC
progression (25–28). This is confirmed by the
association between significantly higher levels of MMP-2 and −9
levels in serum of PC patients compared with control subjects
(25,26). MMPs also serve a pivotal role in
determining the influence of the extracellular matrix and its
structure remodeling with cell phenotype, cell adhesion molecules,
a number of cytokines, chemokines and growth factors. Hence, this
results in increasing tumor growth, invasion and metastasis in
various pathological conditions such as cancer (26,29,30).
Several common forms of polymorphisms are correlated
to allele frequencies in HSD3B1 that affect synthesis, activity and
stability of DHT such as rs33937873, rs6203, rs33913717, rs6205 and
rs1047303 (31,32). rs6203 has been shown to be
implicated in several pathogenesis including myopia (33), gastric cancer (34), sex hormone metabolism (35), hypertensive disorders of pregnancy
(36) and hypertension (HTN) with
left ventricular structure abnormality (37). As to rs6203 and rs33937873, there
is no information about their role, effects or relationships with
prevalence of PC even in a small-scale study population. Therefore,
in the present study, these two SNPs were selected based on their
presence in coding region of HSD3B1 gene which may affect the gene
product. The genetic variation in HSD3B1 can lead to an elevation
in plasma aldosterone with subsequent elevation in HTN and risk of
PC (38). The present study
investigated the prevalence of rs6203, which is the C/T silent
substitution at codon 338 in exon 4 of HSD3B1 (33) and codon 313 of rs33937873 on
HSD3B1 gene in Egyptian PC patients. The present study demonstrated
the association between the single nucleotide polymorphisms of
rs6203 and rs33937873 in HSD3B1 gene and the risk of PC in Egyptian
patients. Additionally, the present study investigated the effect
of each SNP, alone or in combination, shedding the light on their
haplotype effect, disease susceptibility and any associated
clinical parameters.
A total of 366 Egyptian men were incorporated in the
study, categorized into 186 clinically diagnosed PC patients with a
mean age of 69.7±0.7 years (range, 54–84 years) and 180 healthy
controls with a mean age of 62.2±0.9 years (range, 58–79 years).
Patients were recruited from the Urology outpatient clinic of Cairo
University Hospital and Badr Hospital, Helwan University between
June and December 2021. All participants were acknowledged with the
study design and risks with written informed consents taken. The
present study protocol was performed according to the ethics
guidelines and regulations of the Helsinki Declaration. All
experimental protocols were approved by the Scientific Research
Ethics Committee of the Faculty of Pharmacy, Helwan University
(approval number 03H2021). The clinical guidelines for the National
Comprehensive Cancer Network (NCCN) were used for proper diagnosis
of PC patients (39). The
required informed written consents were obtained according to the
regulations of the Institutional Ethical Committee (Faculty of
Medicine, Cairo University) which govern the nature of the study.
The complete history for the patients including (age, family
history, history of benign prostatic hyperplasia (BPH), disease
onset and treatment) was recorded with essential laboratory
assessment including PSA, prostate size, MRI prostate volume and
Gleason grading system. A structured questionnaire was administered
to collect information on history of illness, occupation, smoking
status, and demographic and anthropometric characteristics of the
enrolled subjects. Inclusion criteria for control healthy patients
included no evidence of prostate cancer or tumor history before or
during the study, and patients were randomly selected for matching
by geographic region and the expected age distribution of cases.
Inclusion criteria for patients with prostate cancer were a
clinical diagnosis of primary adenocarcinoma of the prostate by
histopathology and a serum prostate-specific antigen level >4
ng/ml (normal range, 2.5-4.0 ng/ml). Exclusion criteria included:
i) Receipt of medical therapy known to affect PSA levels (such as
betamethasone or testosterone replacement therapy to increase PSA
level and aspirin, ibuprofen, naproxen, atorvastatin, simvastatin
and thiazide diuretics to decrease PSA level) (40); ii) previous invasive treatment for
benign prostatic hyperplasia, with indwelling urethral catheters
(40); iii) voided volume on
initial uroflowmetry of <150 ml (40); iv) previous prostate surgery,
including transurethral resection of the prostate (41); v) any other cancer or metastatic
cancer that has been present during the last 3 years (42); vi) a relationship with another
participant at the 3rd degree or closer (43); and vii) missing data pertaining to
the essential variables (43).
Blood samples (total volume of ~10 ml from each
patient) were used for the determination of PSA level (PSA-ELISA
Kit; catalog no. MBS590045; MyBioSource, Inc.) and DNA analysis in
both groups.
Whole blood samples were subjected for genomic DNA
extraction using spin-column technique (GeneJET Genomic DNA
Purification kit, Thermo Fisher Scientific, Inc.) according to the
manufacturer's protocol. SNPs genotyping assays were ordered as
follows: (rs6203: C_175679504_10 and rs33937873: C__25619111_10;
Thermo Fisher Scientific, Inc.). Genotyping of the two SNPs were
performed using TaqMan master mix (Applied Biosystems; Thermo
Fisher Scientific, Inc.). Analysis of data was performed by
investigating allele using built-in integrated software for
investigating allele frequency in Rotor gene-Q machine (Qiagen
GmbH).
The χ2 test was used to assess the association
between the investigated polymorphisms and PC. The odds ratio (OR)
and confidence intervals (CI) were performed using SPSS 21.00
software (IBM Corp.). Logistic regression analysis was used for the
prediction of risk factors using generalized linear models.
Hardy-Weinberg equilibrium and the linkage disequilibrium were both
calculated using a goodness-of-fit χ2 test. The HaploView program
(version 4.2; Broad Institute) was applied to estimate the
haplotypes (44) using the
expectation maximization algorithm. Comparisons were performed
using two-tailed unpaired t-test and one-way ANOVA (with Tukey's
post hoc test) using GraphPad Prism software (version 5.0; GraphPad
Software, Inc.). P<0.05 was considered to indicate a
statistically significant difference.
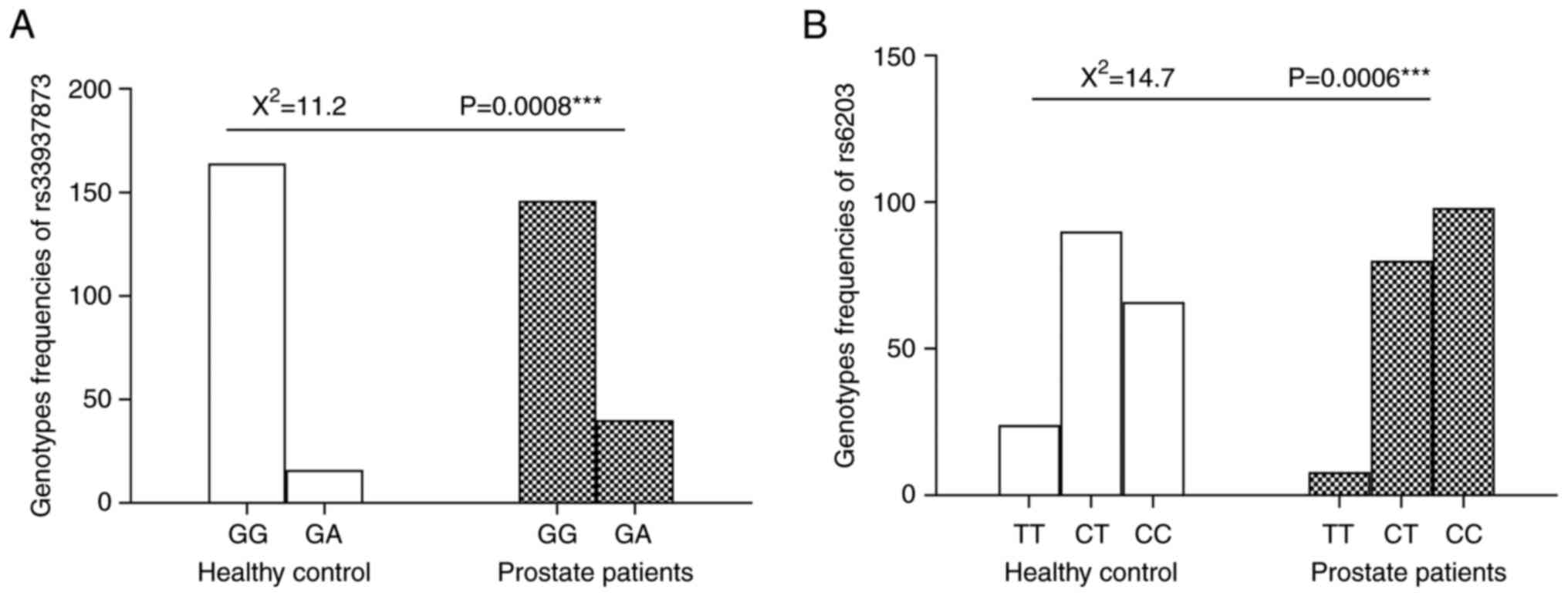
The genotypes distribution and allele frequencies of
(rs6203 and rs33937873) among the control subjects and PC patients
are shown in Table II and
Fig. 1, respectively. Significant
differences were observed in the genotype's distribution pattern of
rs33937873 between the patients and controls (P=0.0008).
Furthermore, the difference in the allele frequencies in rs33937873
was significant (P=0.001). It was quite noticeable that the AA
genotype was rare in both healthy subjects and patients (zero
subjects). The odds ratio between mutant GA genotypes and wild-type
GG genotype was 2.8 (95% CI: 1.5-5.2; P=0.001) in prostate patients
compared with controls. OR of A and G alleles was 2.5 (95% CI:
1.4-4.7; P=0.001) in prostate patients compared with controls,
suggesting that individuals carrying the A allele are 2.5 times
more subjected for developing PC compared with non-carriers.
In the rs6203, The CC genotype elevated the risk of
PC incidence (OR=1.9; 95% CI=1.3-2.9; P=0.002) compared with
control subjects. OR of C and T alleles was 1.8 (95% CI: 1.3-2.4,
P=0.0003) in prostate patients compared with control subjects
(Table II).
A total of four haplotypes were generated for the
two selected SNPs (rs33937873 and rs6203) of HSD3B1 among patients
and control; GC was the most frequent, while the AT was the least
frequent haplotypes among the studied groups. Higher frequency of
AC and lower frequency of GT were significantly associated with
prostate cases when compared with control group, as shown in
Table III. The prediction of
disease risk was weakly correlated with the susceptibility
variants. The predictive performance of genetic risk models
increases by merging multiple common low-risk loci. Therefore, the
haplotype effect between two SNPs on predisposition of PC in
Egyptian patients was studied and found that the polymorphism in
both genes had an amplified influence on the risk of PC than single
locus.
To investigate the effect of these gene
polymorphisms on PC, regression analysis was conducted for
prediction of PC susceptibility with examined family history, DM,
HTN and BPH as shown in Table
IV.
In univariate analysis, it was found that family
history, DM, HTN, history of BPH, GA genotype of rs33937873 and CC
genotype of rs6203 were associated with risk of PC. However, in
multivariable analysis, only patients with history of BPH, HTN and
GA genotype of rs33937873 were considered independent predictors of
PC susceptibility as shown in Table
IV. For the prediction of the PC recurrence regression
analysis, this was conducted using age, family history, DM, HTN,
BPH, GA genotype of rs33937873 and CC genotype of rs6203 as
covariates. Only positive family history was considered a predictor
of PC recurrence as represented in Table V.
To investigate the associations of the two selected
SNPs and various clinical outcomes in PC patients, patients were
stratified according to the type of allelic variant at the
polymorphic site of HSD3B1gene. For rs33937873, the statistical
analysis was applied to prostate patients carrying the mutant
genotype (GA; n=40; 21.5%) who were compared with those carrying
the wild-type genotype (GG group; n=146; 78.5%) as the reference
group. As for rs6203, the major risk genotype CC (n=98; 52.7%) was
compared with the genotype TT (n=8, 4.3%) and heterozygous genotype
CT (n=80; 43%; Table VI). In
rs33937873, PC patients who carry mutant GA genotypes showed
significant increase in prostate volume associated with DM compared
with wild ones.
Prostate cancer is associated with resistance, poor
recovery and metastasis. Hence, early diagnosis is essential for
improving the outcome (45). PSA
was considered as the gold marker in PC; however, the recorded
drawbacks, including non-specificity in PC patients leading to
misdiagnosis and failure in cancer treatment, limit its clinical
applications (46). Therefore,
the ideal for prostate tumor is a molecular marker that is highly
specific and sensitive to avoid false positive results. The use of
genotype information as an aid for selection can be a rapid and
accurate way to enhance selection efficiency of PC patient in a
cost-effective manner. In the present study, HSD3B1 was a major
enzyme of the androgen biosynthetic pathway (47). It catalyzes the conversion of
dehydroepiandrosterone to androstenedione in steroidogenic tissues
such as the adrenal and prostate tissues (48). HSD3B1 is considered to serve an
important role in the production of androgens that fuel PC
development with carcinogenesis and resistance later in a castrate
environment (49).
A total of two single nucleotide polymorphisms were
selected (rs33937873 with codon 313 and rs6203 with codon 338),
however, the functional impact of these two polymorphisms has not
yet been fully elucidated in PC and their ethnic distribution was
not studied in Egyptian PC patients. The mutant A allele and GA
genotype of HSD3B1 gene (rs33937873) indicated a positive
association with PC patients (individuals carrying the minor A
allele are 2.5 times more susceptible for developing PC compared
with non-carriers). The same situation in HSD3B1 gene (rs6203) was
observed with C allele significantly increasing the risk of PC
incidence and individuals carrying the C allele are 1.8 times more
susceptible for developing PC compared with non-carriers. These
results are consistent with a number of findings reported for other
polymorphisms in HSD3B1 gene suggesting that polymorphisms in this
gene is ‘probably damaging’. SNPs can be divided into two main
types; non-synonymous SNP or mutation when it presents within the
coding region of a gene and this leads to change in amino acid
sequence of the resultant protein (50). The other type is synonymous SNPs
that affect translation rates or mRNA half-life rather than change
the nature of the amino acid (51). SNPs can affect the binding
interaction of RNA-protein by modification of secondary structure
of RNA (52,53). Additionally, SNPs can affect both
gene expression level of the specific protein or its binding with
transcription factors (54,55). In all previously mentioned
mechanisms, these can lead to modifications in either function or
structure of the translated proteins (folding) and related
metabolic pathways such as increased cell proliferation, protein
dimerization and activation of a number of mediators (56). In the current study, the suggested
polymorphisms, either G313A or C338T, may create a new potential
protein with different structure and function which induces
cellular carcinogenesis, resistance and apoptosis (57). Another suggestion is that the two
polymorphisms may render HSD3B1 resistant to ubiquitination and
proteasomal degradation, leading to a large amount of protein (DHT)
accumulation in the cell, causing prostate tissue carcinogenesis as
well as resistance to androgen-deprivation therapy in PC recurrence
(57–60). The results suggested that these
variants of the HSD3B1 steroidogenic enzyme gene could be a
powerful new biomarker capable of identifying patients with
aggressive disease who warrant early escalated therapy and in
clinical management of the disease. Additionally, the data obtained
and suggestions were matched with literature about the role of this
enzyme in the degradation of DHT (61) and malfunction in accumulation of
DHT in prostatic tissue (62,63).
For the correlation of the contribution of the
studied SNPs to PC susceptibility, regression analysis was
performed using rs33937873, rs6203 and other variables as
covariates. Positive family history, DM, HTN, GA genotype of
rs33937873 and CC genotype of rs6203 were associated with risk of
PC in univariable analysis. On the other hand, in multivariable
analysis, only patients with a history of BPH, HTN and GA genotype
of rs33937873 were considered independent predictors of PC
susceptibility. Family history was considered the only predictor of
PC recurrence in the present study, as a well-known risk factor for
developing PC (64). The
literature matched this observation and shows that there is a trend
of increasing risk of PC incidence in patients with two or three
first degree relatives affected to have a five and 11-fold
increased risk of developing PC (65–68). In the US, those with a family
history of PC should be advised of their significantly increased PC
risk to ~9–10% in their lifetime (69). In Africa, some studies found a
correlation between PC incidence in different African cultures and
their family history reached between 30–70% (69,70). With respect to this biological
heterogeneity of PC, the observation is important in understanding
PC etiology and incidence risk factor to correctly assess the
clinical state of the patient using PSA continuous screening to
avoid aggressiveness and high mortality rate.
In addition, the findings of the present study
reported significant association between the mutant genotype GA of
rs33937873 in PC patients with DM. Although studies mention that DM
and PC have an inverse relationship (71–73), some other studies could not find
any evidence of the inverse relationship between DM and PC
(74–76). However, some other results in
population-based cohort study concur with the findings of the
present study suggesting that the relationship between DM and
high-grade PC has a positive correlation (77,78). The potential explanation for this
hypothesis is related to the activity of the patient such as
exercise, body mass index (79,80), glycemic control (78) and ethnicity (81) and further large scale studies are
required to understand the proper mechanisms controlling the
correlation in each case.
The data presented in the present study shed light
on the potential role of these two SNPs in HSD3B1gene as the
promising marker for the prediction of PC incidence. The future
perspective for is to illustrate the effect of both studied SNPs in
different advanced cases of PC such as CRPC through the activity of
HSD3B1 and to study their role in susceptibility and resistance of
prostate patients to treatments such as abiraterone.
The present study has suggested a potential impact
of SNPs in HSD3B1 gene (rs6203 and rs33937873) individually and in
combination in relation to the risk of PC in Egyptian patients.
These results deserve the trial on a larger study in the context of
PC susceptibility to shed the light on the function of HSD3B1 and
associated allelic variants in correlation to other
androgen-metabolizing enzymes. Moreover, the present study needs to
be applied using both in vitro and in vivo models to confirm the
hypothesis and elucidate the role of the gene and its corresponding
protein in PC pathogenesis.
The authors would like to thank Professor Sameh
Soror (Helwan University, Centre of Scientific Excellence ‘Helwan
Structural Biology Research’, Helwan University, Cairo) for the
opportunity to use the facilities/equipment available in the Helwan
Structural Biology Research Laboratory.
Funding: No funding was received.
All data generated or analyzed during this study are
included in this published article.
HH, HBA, YMA and DMA designed the study, performed
the experiments, and wrote and revised the manuscript. HBA, YMA and
HH analyzed the datasets. HH searched the literature. HH, HBA YMA
and DMA confirm the authenticity of all the raw data. All authors
read and approved the final manuscript.
All subjects gave their written informed consent to
participate in the study. The study was approved by Scientific
Research Ethics Committee of the Faculty of Pharmacy, Helwan
university (approval number 03H2021).
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Culp MB, Soerjomataram I, Efstathiou JA,
Bray F and Jemal A: Recent global patterns in prostate cancer
incidence and mortality rates. Eur Urol. 77:38–52. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Stanbrough M, Bubley GJ, Ross K, Golub TR,
Rubin MA, Penning TM, Febbo PG and Balk SP: Increased expression of
genes converting adrenal androgens to testosterone in
androgen-independent prostate cancer. Cancer Res. 66:2815–2825.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Knepper PA, Collins JA and Frederick R:
Effects of dexamethasone, progesterone, and testosterone on IOP and
GAGs in the rabbit eye. Investig Ophthalmol Vis Sci. 26:1093–1100.
1985.PubMed/NCBI
|
|
4
|
Ettinger SL, Sobel R, Whitmore TG, Akbari
M, Bradley DR, Gleave ME and Nelson CC: Dysregulation of sterol
response element-binding proteins and downstream effectors in
prostate cancer during progression to androgen independence. Cancer
Res. 64:2212–2221. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Heemers H, Maes B, Foufelle F, Heyns W,
Verhoeven G and Swinnen JV: Androgens stimulate lipogenic gene
expression in prostate cancer cells by activation of the sterol
regulatory element-binding protein cleavage activating
protein/sterol regulatory element-binding protein pathway. Mol
Endocrinol. 15:1817–1828. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Vis AN and Schröder FH: Key targets of
hormonal treatment of prostate cancer. Part 1: The androgen
receptor and steroidogenic pathways. BJU Int. 104:438–448. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hamad A, Kluk M, Fox J, Park M and Turner
JE: The effects of aromatase inhibitors and selective estrogen
receptor modulators on eye development in the zebrafish (Danio
rerio). Curr Eye Res. 32:819–827. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Deb S, Chin MY, Pham S, Adomat H,
Hurtado-Coll A, Gleave ME and Tomlinson Guns ES: Steroidogenesis in
peripheral and transition zones of human prostate cancer tissue.
Int J Mol Sci. 22:4872021. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Torres MJ, López-Moncada F, Herrera D,
Indo S, Lefian A, Llanos P, Tapia J, Castellón EA and Contreras HR:
Endothelin-1 induces changes in the expression levels of
steroidogenic enzymes and increases androgen receptor and
testosterone production in the PC3 prostate cancer cell line. Oncol
Rep. 46:1712021. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hou Z, Yang T, Mei Z, Zhang S, Gao Y, Chen
X, Tan Q, Zhu X, Xu C, Lian J, et al: Tracing steroidogenesis in
prostate biopsy samples to unveil prostate tissue androgen
metabolism characteristics and potential clinical application. J
Steroid Biochem Mol Biol. 210:1058592021. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cunningham JM, Hebbring SJ, McDonnell SK,
Cicek MS, Christensen GB, Wang L, Jacobsen SJ, Cerhan JR, Blute ML,
Schaid DJ and Thibodeau SN: Evaluation of genetic variations in the
androgen and estrogen metabolic pathways as risk factors for
sporadic and familial prostate cancer. Cancer Epidemiol Biomark
Prev. 16:969–978. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Holzbeierlein J, Lal P, LaTulippe E, Smith
A, Satagopan J, Zhang L, Ryan C, Smith S, Scher H, Scardino P, et
al: Gene expression analysis of human prostate carcinoma during
hormonal therapy identifies androgen-responsive genes and
mechanisms of therapy resistance. Am J Pathol. 164:217–227. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Crawford ED, Heidenreich A, Lawrentschuk
N, Tombal B, Pompeo ACL, Mendoza-Valdes A, Miller K, Debruyne FMJ
and Klotz L: Androgen-targeted therapy in men with prostate cancer:
Evolving practice and future considerations. Prostate Cancer
Prostatic Dis. 22:24–38. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shiota M, Yokomizo A and Naito S:
Pro-survival and anti-apoptotic properties of androgen receptor
signaling by oxidative stress promote treatment resistance in
prostate cancer. Endocr Relat Cancer. 19:R243–R253. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Montgomery RB, Mostaghel EA, Vessella R,
Hess DL, Kalhorn TF, Higano CS, True LD and Nelson PS: Maintenance
of intratumoral androgens in metastatic prostate cancer: A
mechanism for castration-resistant tumor growth. Cancer Res.
68:4447–4454. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Schiffer L, Barnard L, Baranowski ES,
Gilligan LC, Taylor AE, Arlt W, Shackleton CHL and Storbeck KH:
Human steroid biosynthesis, metabolism and excretion are
differentially reflected by serum and urine steroid metabolomes: A
comprehensive review. J Steroid Biochem Mol Biol. 194:1054392019.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Gsur A, Feik E and Madersbacher S: Genetic
polymorphisms and prostate cancer risk. World J Urol. 21:414–423.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Evaul K, Li R, Papari-Zareei M, Auchus RJ
and Sharifi N: 3beta-hydroxysteroid dehydrogenase is a possible
pharmacological target in the treatment of castration-resistant
prostate cancer. Endocrinol. 151:3514–3520. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mason JI, Keeney DS, Bird IM, Rainey WE,
Morohashi K, Leers-Sucheta S and Melner MH: The regulation of 3
beta-hydroxysteroid dehydrogenase expression. Steroids. 62:164–168.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Simard J, Ricketts ML, Gingras S, Soucy P,
Feltus FA and Melner MH: Molecular biology of the
3beta-hydroxysteroid dehydrogenase/delta5-delta4 isomerase gene
family. Endocr Rev. 26:525–582. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Rhéaume E, Lachance Y, Zhao HF, Breton N,
Dumont M, de Launoit Y, Trudel C, Luu-The V, Simard J and Labrie F:
Structure and expression of a new complementary DNA encoding the
almost exclusive 3 beta-hydroxysteroid dehydrogenase/delta 5-delta
4-isomerase in human adrenals and gonads. Mol Endocrinol.
5:1147–1157. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Schiffer L, Arlt W and Storbeck KH:
Intracrine androgen biosynthesis, metabolism and action revisited.
Mol Cell Endocrinol. 465:4–26. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Silva SA, Gobbo MG, Pinto-Fochi ME,
Rafacho A, Taboga SR, Almeida EA, Góes RM and Ribeiro DL: Prostate
hyperplasia caused by long-term obesity is characterized by high
deposition of extracellular matrix and increased content of MMP-9
and VEGF. Int J Exp Pathol. 96:21–30. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Edlund M, Sung SY and Chung LW: Modulation
of prostate cancer growth in bone microenvironments. J Cell
Biochem. 91:686–705. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Trudel D, Fradet Y, Meyer F, Harel F and
Têtu B: Significance of MMP-2 expression in prostate cancer: An
immunohistochemical study. Cancer Res. 63:8511–8515.
2003.PubMed/NCBI
|
|
26
|
Xie T, Dong B, Yan Y, Hu G and Xu Y:
Association between MMP-2 expression and prostate cancer: A
meta-analysis. Biomed Rep. 4:241–245. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Gong Y, Chippada-Venkata UD and Oh WK:
Roles of matrix metalloproteinases and their natural inhibitors in
prostate cancer progression. Cancers (Basel). 6:1298–1327. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Abdelaal MR, Soror SH, Elnagar MR and
Haffez H: Revealing the potential application of EC-synthetic
retinoid analogues in anticancer therapy. Molecules. 26:5062021.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Nemeth JA, Yousif R, Herzog M, Che M,
Upadhyay J, Shekarriz B, Bhagat S, Mullins C, Fridman R and Cher
ML: Matrix metalloproteinase activity, bone matrix turnover, and
tumor cell proliferation in prostate cancer bone metastasis. J Natl
Cancer Inst. 94:17–25. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Overall CM and López-Otín C: Strategies
for MMP inhibition in cancer: Innovations for the post-trial era.
Nat Rev Cancer. 2:657–672. 2002. View
Article : Google Scholar : PubMed/NCBI
|
|
31
|
Chang KH, Li R, Kuri B, Lotan Y, Roehrborn
CG, Liu J, Vessella R, Nelson PS, Kapur P, Guo X, et al: A
gain-of-function mutation in DHT synthesis in castration-resistant
prostate cancer. Cell. 154:1074–1084. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Sabharwal N and Sharifi N: HSD3B1
genotypes conferring adrenal-restrictive and adrenal-permissive
phenotypes in prostate cancer and beyond. Endocrinology.
160:2180–2188. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Chen ZTY, Wang IJ, Liao YT, Shih YF and
Lin LLK: Polymorphisms in steroidogenesis genes, sex steroid
levels, and high myopia in the Taiwanese population. Mol Vis.
17:2297–2310. 2011.PubMed/NCBI
|
|
34
|
Cho LY, Yang JJ, Ko KP, Ma SH, Shin A,
Choi BY, Han DS, Song KS, Kim YS, Chang SH, et al: Genetic
susceptibility factors on genes involved in the steroid hormone
biosynthesis pathway and progesterone receptor for gastric cancer
risk. PLoS One. 7:e476032012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Carmichael S, Witte J, Ma C, Lammer E and
Shaw G: Hypospadias and variants in genes related to sex hormone
biosynthesis and metabolism. Andrology. 2:130–137. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Shimodaira M, Nakayama T, Sato I, Sato N,
Izawa N, Mizutani Y, Furuya K and Yamamoto T: Estrogen synthesis
genes CYP19A1, HSD3B1, and HSD3B2 in hypertensive disorders of
pregnancy. Endocrine. 42:700–707. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Shimodaira M, Nakayama T, Sato N, Aoi N,
Sato M, Izumi Y, Soma M and Matsumoto K: Association of HSD3B1 and
HSD3B2 gene polymorphisms with essential hypertension, aldosterone
level, and left ventricular structure. Eur J Endocrinol.
163:671–810. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Gao H, Xu J, Ma Q, Tang F, Ga Q, Li Y,
Guan W, Ge R and Yang YZ: Association between the polymorphism of
steroid hormone metabolism genes and high-altitude pulmonary edema
in the Chinese Han population. Int J Gen Med. 15:787–794. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Mohler JL, Armstrong AJ, Bahnson RR,
Boston B, Busby JE, D'Amico AV, Eastham JA, Enke CA, Farrington T,
Higano CS, et al: Prostate cancer, version 3.2012: Featured updates
to the NCCN guidelines. J Natl Compr Canc Netw. 10:1081–1087. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Cormio L, Lucarelli G, Netti GS, Stallone
G, Selvaggio O, Troiano F, Di Fino G, Sanguedolce F, Bufo P,
Grandaliano G and Carrieri G: Post-void residual urinary volume is
an independent predictor of biopsy results in men at risk for
prostate cancer. Anticancer Res. 35:2175–2182. 2015.PubMed/NCBI
|
|
41
|
Jeong CW, Hong SK, Byun SS, Jeon SS, Seo
SI, Lee HM, Ahn H, Kwon DD, Ha HK, Kwon TG, et al: Selection
criteria for active surveillance of patients with prostate cancer
in Korea: A multicenter analysis of pathology after radical
prostatectomy. Cancer Res Treat. 50:265–274. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Solanki AA, Schroth CA, Authier C, Carlson
K, Garraway I, Haegerich T, Henry E, Jones JA, Joseph R, Koppes T,
et al: Veterans affairs seamless phase II/III randomized trial of
standard systemic therapy with or without PET-directed local
therapy for oligorecurrent prostate cancer (VA STARPORT). J Clin
Oncol. 40 (Suppl 6):TPS2032022. View Article : Google Scholar
|
|
43
|
Jiang Y, Meyers TJ, Emeka AA, Cooley LF,
Cooper PR, Lancki N, Helenowski I, Kachuri L, Lin DW, Stanford JL,
et al: Genetic factors associated with prostate cancer conversion
from active surveillance to treatment. HGG Adv.
3:1000702022.PubMed/NCBI
|
|
44
|
Barrett JC, Fry B, Maller J and Daly MJ:
Haploview: Analysis and visualization of LD and haplotype maps.
Bioinformatics. 21:263–265. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Litwin MS and Tan HJ: The diagnosis and
treatment of prostate cancer: A review. JAMA. 317:2532–2542. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Adhyam M and Gupta AK: A review on the
clinical utility of PSA in cancer prostate. Indian J Surg Oncol.
3:120–129. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Wu G, Huang S, Nastiuk KL, Li J, Gu J, Wu
M, Zhang Q, Lin H and Wu D: Variant allele of HSD3B1 increases
progression to castration-resistant prostate cancer. Prostate.
75:777–782. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Sharifi N, McPhaul MJ and Auchus RJ:
‘Getting from here to there’-mechanisms and limitations to the
activation of the androgen receptor in castration-resistant
prostate cancer. J Investig Med. 58:938–944. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Dai C, Heemers H and Sharifi N: Androgen
signaling in prostate cancer. Cold Spring Harb Perspect Med.
7:a0304522017. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Mendell JT and Dietz HC: When the message
goes awry: Disease-producing mutations that influence mRNA content
and performance. Cell. 107:411–414. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Nicholson P, Yepiskoposyan H, Metze S,
Zamudio Orozco R, Kleinschmidt N and Mühlemann O: Nonsense-mediated
mRNA decay in human cells: Mechanistic insights, functions beyond
quality control and the double-life of NMD factors. Cell Mol Life
Sci. 67:677–700. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Beaudoin JD and Perreault JP: 5′-UTR
G-quadruplex structures acting as translational repressors. Nucleic
Acids Res. 38:7022–7036. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Robert F and Pelletier J: Exploring the
impact of single-nucleotide polymorphisms on translation. Front
Genet. 507:5072018. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Das SC, Rahman M and Das Gupta S:
In-silico analysis unravels the structural and functional
consequences of non-synonymous SNPs in the human IL-10 gene. Egypt
J Med Hum Genet. 23:1–14. 2022. View Article : Google Scholar
|
|
55
|
Kucukkal TG, Petukh M, Li L and Alexov E:
Structural and physico-chemical effects of disease and non-disease
nsSNPs on proteins. Curr Opin Struct Biol. 32:18–24. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Gebert M, Jaśkiewicz M, Moszyńska A,
Collawn JF and Bartoszewski R: The effects of single nucleotide
polymorphisms in cancer RNAi therapies. Cancers (Basel).
12:31192020. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Park JY, Tanner JP, Sellers TA, Huang Y,
Stevens CK, Dossett N, Shankar RA, Zachariah B, Heysek R and
Pow-Sang J: Association between polymorphisms in HSD3B1 and UGT2B17
and prostate cancer risk. Urology. 70:374–379. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Han FF, Ren LL, Xuan LL, Lv YL, Liu H,
Gong LL, An ZL and Liu LH: HSD3B1 variant and androgen-deprivation
therapy outcome in prostate cancer. Cancer Chemother Pharmacol.
87:103–112. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Setlur SR, Chen CX, Hossain RR, Ha JS, Van
Doren VE, Stenzel B, Steiner E, Oldridge D, Kitabayashi N, Banerjee
S, et al: Genetic variation of genes involved in
dihydrotestosterone metabolism and the risk of prostate cancer.
Cancer Epidemiol Biomark Prev. 19:229–239. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Huang J, Huang D and Na R: The association
between genetic variants in HSD3B1 and clinical management of PCa.
J Transl Genet Genom. 5:240–249. 2021.PubMed/NCBI
|
|
61
|
Devgan SA, Henderson BE, Yu MC, Shi CY,
Pike MC, Ross RK and Reichardt JK: Genetic variation of 3
beta-hydroxysteroid dehydrogenase type II in three racial/ethnic
groups: Implications for prostate cancer risk. Prostate. 33:9–12.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Kosaka T, Miyajima A and Oya M: Is DHT
production by 5α-reductase friend or foe in prostate cancer? Front
Oncol. 4:2472014. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Stangl-Kremser J, Lemberger U, Hassler MR,
Bruchbacher A, Ilijazi D, Garstka N, Kramer G, Haitel A, Abufaraj M
and Shariat SF: Prevalence and prognostic value of the polymorphic
variant 1245A>C of HSD3B1 in castration-resistant prostate
cancer. Clin Genitourin Cancer. 17:389–394. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Johns L and Houlston R: A systematic
review and meta-analysis of familial prostate cancer risk. BJU Int.
91:789–794. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Barber L, Gerke T, Markt SC, Peisch SF,
Wilson KM, Ahearn T, Giovannucci E, Parmigiani G and Mucci LA:
Family history of breast or prostate cancer and prostate cancer
risk. Clin Cancer Res. 24:5910–5917. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Chen YC, Page JH, Chen R and Giovannucci
E: Family history of prostate and breast cancer and the risk of
prostate cancer in the PSA era. Prostate. 68:1582–1591. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Thomas JA II, Gerber L, Moreira DM,
Hamilton RJ, Bañez LL, Castro-Santamaria R, Andriole GL, Isaacs WB,
Xu J and Freedland SJ: Prostate cancer risk in men with prostate
and breast cancer family history: Results from the REDUCE study
(R1). J Intern Med. 272:85–92. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Cunningham GR, Ashton CM, Annegers JF,
Souchek J, Klima M and Miles B: Familial aggregation of prostate
cancer in African-Americans and white Americans. Prostate.
56:256–262. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Steinberg GD, Carter BS, Beaty TH, Childs
B and Walsh PC: Family history and the risk of prostate cancer.
Prostate. 17:337–347. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Acheampong E, Adu EA, Obirikorang C, Amoah
G, Afriyie OO, Yorke J and Yeboah FA: Association of genetic
variants with prostate cancer in Africa: A concise review. Egypt J
Med Hum Genet. 22:1–9. 2021. View Article : Google Scholar
|
|
71
|
Kasper JS, Liu Y and Giovannucci E:
Diabetes mellitus and risk of prostate cancer in the health
professionals follow-up study. Int J Cancer. 124:1398–1403. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Bonovas S, Filioussi K and Tsantes A:
Diabetes mellitus and risk of prostate cancer: A meta-analysis.
Diabetologia. 47:1071–1078. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Feng X, Song M, Preston MA, Ma W, Hu Y,
Pernar CH, Stopsack KH, Ebot EM, Fu BC, Zhang Y, et al: The
association of diabetes with risk of prostate cancer defined by
clinical and molecular features. Br J Cancer. 123:657–665. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Chan JM, Latini DM, Cowan J, Duchane J and
Carroll PR: History of diabetes, clinical features of prostate
cancer, and prostate cancer recurrence-data from CaPSURE (United
States). Cancer Causes Control. 16:789–797. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Au Yeung SL and Schooling CM: Impact of
glycemic traits, type 2 diabetes and metformin use on breast and
prostate cancer risk: A Mendelian randomization study. BMJ Open
Diabetes Res Care. 7:e0008722019. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Wu C, Moreira DM, Gerber L, Rittmaster RS,
Andriole GL and Freedland SJ: Diabetes and prostate cancer risk in
the REDUCE trial. Prostate Cancer Prostatic Dis. 14:326–331. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Li Q, Kuriyama S, Kakizaki M, Yan H, Sone
T, Nagai M, Sugawara Y, Ohmori-Matsuda K, Hozawa A, Nishino Y and
Tsuji I: History of diabetes mellitus and the risk of prostate
cancer: The Ohsaki cohort study. Cancer Causes Control.
21:1025–1032. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Park J, Cho SY, Lee YJ, Lee SB, Son H and
Jeong H: Poor glycemic control of diabetes mellitus is associated
with higher risk of prostate cancer detection in a biopsy
population. PLoS One. 9:e1047892014. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Leitzmann MF, Ahn J, Albanes D, Hsing AW,
Schatzkin A, Chang SC, Huang WY, Weiss JM, Danforth KN, Grubb RL
III, et al: Diabetes mellitus and prostate cancer risk in the
prostate, lung, colorectal, and ovarian cancer screening trial.
Cancer Causes Control. 19:1267–1276. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Fall K, Garmo H, Gudbjörnsdottir S,
Stattin P and Zethelius B: Diabetes mellitus and prostate cancer
risk; a nationwide case-control study within PCBaSe Sweden. Cancer
Epidemiol Biomarkers Prev. 22:1102–1109. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Moreira DM, Anderson T, Gerber L, Thomas
JA, Bañez LL, McKeever MG, Hoyo C, Grant D, Jayachandran J and
Freedland SJ: The association of diabetes mellitus and high-grade
prostate cancer in a multiethnic biopsy series. Cancer Causes
Control. 22:977–983. 2011. View Article : Google Scholar : PubMed/NCBI
|