Introduction
The International Agency for Research on Cancer
estimates that one in five individuals will develop cancer during
their lifetime, with one in nine men and one in 12 women succumbing
to the disease (1). Lung cancer is
the most commonly diagnosed cancer worldwide, accounting for 12.4%
of cases, and remains the leading cause of cancer-related
mortality, responsible for 18.7% of all cancer-associated deaths
(1). The prevalence of smoking
among men in densely populated countries such as China (41.5%),
underscores the growing concern over escalating global lung cancer
mortality rates (2).
Non-small cell lung carcinoma (NSCLC) constitutes
~85% of all lung cancer cases, with adenocarcinoma being the most
prevalent histological subtype (3). Early-stage NSCLC is primarily treated
with surgical resection, often supplemented with radiotherapy,
chemotherapy or targeted therapies (4). However, metastatic recurrence occurs
in 30–75% of patients despite these interventions (5,6).
While patients at stage IA may achieve a 5-year recurrence-free
survival rate of ≤82% (7), those
with advanced disease experience a considerably lower 5-year
overall survival rate of ~20%, largely due to metastases, even with
the availability of targeted therapies and immunotherapy (8). Metastasis remains the primary barrier
to long-term survival, as tumor cells often disseminate via the
bloodstream or to target organs before clinical detection (9,10).
Thus, early diagnosis and reliable postoperative evaluation are
important for improving survival rates and reducing mortality.
Low-dose computed tomography (LDCT) has enhanced early lung cancer
detection but is associated with a high false-positive rate, with
>10% of patients being misdiagnosed with cancer (11,12).
Additionally, CT imaging struggles to differentiate
post-radiotherapy pulmonary fibrosis from tumor recurrence and
often fails to detect micrometastases, limiting its accuracy in
assessing radiotherapy outcomes (13). Solid biopsies, although
traditionally used for tumor evaluation, are invasive and
unsuitable for real-time monitoring, emphasizing the need for less
invasive diagnostic tools (14).
Liquid biopsy offers a non-invasive, efficient and accurate
alternative for tumor detection and monitoring. Analyzing the
biological information present in blood enables real-time
assessment and comprehensive profiling of cancer (14).
The present small-scale pilot study employed
matrix-assisted laser desorption/ionization time-of-flight
(MALDI-TOF) mass spectrometry (MS)-based serum peptidomics for
detecting differential peptide signals between patients with lung
cancer and individuals with benign pulmonary nodules. These
findings highlight the potential of this approach while
underscoring the need for rigorous validation in larger
cohorts.
Materials and methods
Study rationale and design
To illustrate the practical application and inherent
challenges of clinical peptidomics, a small-scale, preliminary
study was performed. The primary aim was exploratory: To assess the
feasibility of generating differential serum peptide profiles
between malignant and benign pulmonary nodules. The study cohort
consisted of 32 patients from the Affiliated Hospital of Jining
Medical University (Jining, China) between January 2025 and June
2025; this included 29 patients with pathologically confirmed lung
cancer (the cancer group) and 3 patients with benign pulmonary
nodules (the control group). The inclusion criteria were patients
aged 18–75 years with a confirmed diagnosis of lung cancer or
benign pulmonary nodules. Exclusion criteria included patients with
previous treatment (chemotherapy, radiotherapy or surgery), active
infections, or any history of other malignancies. Benign nodule
status was confirmed either by biopsy or radiographic stability
over a period of ≥2 years. Key demographic and clinical
characteristics of the participants are summarized in Table I. The present study was approved by
the Institutional Review Board of the Institute of Medical Science,
Affiliated Hospital of Jining Medical University (approval no.
2024-02-C011).
 | Table I.Clinicopathological characteristics of
the patients recruited in the present study. |
Table I.
Clinicopathological characteristics of
the patients recruited in the present study.
|
| Cancer (n=29) | Normal (n=3) |
|
|---|
|
|
|
|
|
|---|
| Characteristic | N | % | N | % | P-value |
|---|
| Age, years |
|
|
|
| 0.851 |
| ≥60 | 18 | 62.1 | 2 | 66.7 |
|
|
<60 | 11 | 37.9 | 1 | 33.3 |
|
| Sex |
|
|
|
| 0.548 |
|
Female | 15 | 51.7 | 2 | 66.7 |
|
| Male | 14 | 48.3 | 1 | 33.3 |
|
| Smoking history |
|
|
|
| 0.095 |
|
Smoker | 15 | 51.7 | 1 | 33.3 |
|
|
Non-smoker | 14 | 48.3 | 2 | 66.7 |
|
| Location |
|
|
|
| - |
| Right
upper lobe | 8 | 27.6 | - | - |
|
| Right
middle lobe | 4 | 13.8 | - | - |
|
| Right
lower lobe | 3 | 10.3 | 1 | 33.3 |
|
| Left
upper lobe | 10 | 34.5 | 1 | 33.3 |
|
| Left
lower lobe | 4 | 13.8 | 1 | 33.3 |
|
| Histopathology |
|
|
|
| - |
|
Adenocarcinoma | 24 | 82.8 | - | - |
|
| Squamous
cell | 2 | 6.9 | - | - |
|
| Small
cell | 1 | 3.4 | - | - |
|
|
Other | 2 | 3.4 | - | - |
|
| Tumor stage |
|
|
|
| - |
|
T1a | 9 | 31.0 | 2 | 66.7 |
|
|
T1b | 16 | 55.2 | - | - |
|
|
T1c | 4 | 13.8 | - | - |
|
| T2 | - | - | 1 | 33.3 |
|
Serum sample collection and
preparation
Peripheral blood samples (5 ml) were collected from
all participants. Serum was separated by centrifugation at 4°C for
10 min at 500 × g, then aliquoted and stored at −80°C until
analysis. Upon receipt of peptidomic profiling, all samples were
transported on dry ice and remained frozen. Visual inspection
confirmed the absence of hemolysis or lipemia in all samples.
Peptide extraction
Serum peptidome analysis, including peptide
extraction, matrix-assisted laser desorption/ionization
time-of-flight mass spectrometry (MALDI-TOF MS) analysis and
quality control (QC), was performed by Hangzhou Well-healthcare
Technologies Co., Ltd., using their proprietary platform. Peptides
were extracted from serum using the Well-healthcare Serum Peptide
Detection Kit according to the manufacturer's protocol. Briefly, 10
µl serum was mixed with 70 µl ultrapure water and added to a
96-well plate pre-loaded with nanoporous silica microspheres. The
mixture was incubated at room temperature with agitation at 1,350
rpm for 15 min. After incubation, the supernatant was removed by
centrifugation at 4°C for 10 min at 500 × g. The pellet was washed
once with 80 µl ultrapure water and centrifuged again at 4°C for 10
min at 500 × g to remove the supernatant.
MALDI-TOF MS analysis
The extracted peptides were eluted with a matrix
solution containing acetonitrile and trifluoroacetic acid, mixed
with an excess of α-cyano-4-hydroxycinnamic acid matrix. A 1-µl
aliquot of the mixture was spotted onto a stainless-steel MALDI
target plate and allowed to dry under vacuum. MS analysis was
performed using a ClinMS-Plat I MALDI-TOF MS instrument (Hangzhou
Well-healthcare Technologies Co., Ltd). Data were acquired in
positive ion linear mode with the following parameters: Extraction
voltage, 2.00 kV; detector voltage, 2.30 kV; delay time, 200 nsec.
For each spectrum, 800 laser shots were accumulated across a mass
range of 680-18,600 Da.
QC
Rigorous QC measures were implemented. On each
target plate, the following control spots were included alongside
patient samples: One negative QC (N-QC; from pooled negative serum,
prepared by mixing negative serum samples from healthy
individuals), one positive QC (P-QC; from pooled positive serum,
prepared by mixing serum from patients with lung cancer), and three
baseline QCs (B-QC; from pooled negative serum, prepared similarly
to N-QC). The positions of N-QC, P-QC, B-QC and calibration
standards were randomly distributed on the target plate. QC samples
underwent the same pre-treatment process as the test samples.
System suitability required B-QC spectral similarity scores to be
≤0.34 (Euclidean and Manhattan distances), N-QC to test negative
(score ≤0) and P-QC to test positive (score >0). All samples
passed QC criteria, with a minimum of 500 laser shots and a minimum
peak detection proportion of 50% per spectrum.
Preprocessing and peak detection
Raw mass spectral data were preprocessed using MDAS
PreData software (version 2.23; Well-healthcare Technologies Co.,
Ltd.). This included baseline correction, smoothing, peak alignment
and peak picking. A total of 444 mass spectral peak signals were
detected across all samples. These peaks were matched against the
PeptideAtlas database (http://www.peptideatlas.org), resulting in the
identification of 188 unique peptide sequences.
Identification of differential peptide
signals
For statistical comparison between the cancer (n=29)
and control (n=3) groups, peptide peak intensity values were used.
Peptide signals detected in <80% of the samples within either
group were filtered out. Peptides with an absolute log2 fold-change
(|log2FC|) >0.2 and P<0.05 were considered differentially
expressed. No correction for multiple testing (for example, false
discovery rate or Bonferroni) was applied due to the exploratory
nature and small sample size of this pilot study.
Functional annotation and enrichment
analysis
The proteins corresponding to the identified
differential peptides were subjected to functional annotation and
enrichment analysis. Gene Ontology (GO) enrichment, Clusters of
Orthologous Groups (COG/KOG) classification, and Kyoto Encyclopedia
of Genes and Genomes (KEGG) pathway analyses were performed using
InterProScan (https://www.ebi.ac.uk/interpro), KAAS (http://www.genome.jp/kegg/kaas/), UniProt
(https://www.uniprot.org), and eggNOG (http://eggnogdb.embl.de). Protein-protein interaction
(PPI) networks were constructed using the STRING database
(https://string-db.org) and visualized with
Cytoscape software (https://cytoscape.org).
Statistical analysis
Categorical variables were presented as numbers and
percentages. For comparisons between the cancer (n=29) and control
(n=3) groups Fisher's exact test was used for all 2×2 contingency
tables due to the small sample size, particularly in the control
group. Differential peptides were identified using a non-parametric
Mann-Whitney U test, suitable for comparing two independent groups
with non-normally distributed data. P<0.05 was considered to
indicate a statistically significant difference. All statistical
analyses were performed using R software (version 4.1.3; Posit
software), which can be accessed at https://www.r-project.org.
Results
Patient characteristics
The present preliminary feasibility study included
serum samples from 32 patients. The cohort consisted of 29 patients
with pathologically confirmed lung cancer (the cancer group) and 3
patients with benign pulmonary nodules (the control group), as
detailed in Table I. There were no
statistically significant differences between the two groups in
terms of age distribution (P=0.851) or sex (P=0.548) (Table I). The majority of lung cancer
cases were adenocarcinoma (24/29; 82.8%) and were at an early stage
(T1a-T1c, 29/29; 100%). Detailed histopathological descriptions are
provided in Table II.
| Table II.Patient pathology information. |
Table II.
Patient pathology information.
| Patient ID | Pathological
information |
|---|
| D01 | (Right) malignant
tumor of the lung (upper lobe), inclined to carcinosarcoma, mass
size 3×1.7×1.5 cm |
| D02 | (Right) peripheral
infiltrating adenocarcinoma (solid + alveolar) of the lung (upper
lobe) with necrosis, mass size 2×1×1 cm |
| D03 | (Right) peripheral
infiltrating moderately-lowly differentiated adenocarcinoma of the
lung (middle lobe; alveolar + micropapillary + solid), mass size
3×3×2 cm |
| D04 | (Left) invasive
adenocarcinoma (solid type predominant) of the lung (upper lobe),
poorly differentiated, focal mucinous cell carcinoma, mass size
1.5×1.5×1 cm |
| D05 | (Right) peripheral
infiltrating moderately differentiated adenocarcinoma of the lung
(upper lobe; predominantly alveolar, locally solid), mass size
1.8×1.8×1.2 cm |
| D06 | (Upper lobe of
right lung) peripheral type moderately-lowly differentiated
squamous cell carcinoma, size 2×1.5×1.2 cm |
| D07 | (Left) peripheral
type invasive adenocarcinoma of the lung (lower lobe; alveolar +
appressed + solid), mass size 2.5×1.5×1 cm |
| D08 | (Left) peripheral
type invasive adenocarcinoma of the lung (upper lobe; papillary +
micropapillary + solid + adnexal), mass size 2×1×0.7 cm |
| D09 | Microinvasive
adenocarcinoma (upper lobe of the left lung), size 1×0.6×0.6 cm, no
clear pleural invasion observed |
| D10 | (Right)
infiltrating highly differentiated squamous carcinoma of the lung
(lower lobe), mass size 2×2×1 cm |
| D11 | (Left) peripheral
type invasive adenocarcinoma (alveolar + adnexal) of the lung
(lower lobe), measuring 1×0.6×0.6 cm, without definite alveolar
luminal dissemination and pleural invasion |
| D12 | (Left)
microinvasive adenocarcinoma of the lung (upper lobe), mass size
1×0.6×0.6 cm |
| D13 | (Lower lobe of the
right lung) lung tissue shows acute and chronic inflammatory cell
infiltration, fibrous tissue proliferation and necrosis, and a
fibrous connective tissue capsule wall with no obvious lining
epithelium, accompanied by aggregation of surrounding tissue cells.
The findings are consistent with a pulmonary hydatid cyst
(echinococcosis) (Control group sample) |
| D14 | (Left) peripheral
infiltrating highly differentiated adenocarcinoma of the lung
(upper lobe; alveolar + adnexal type), mass size 1×1×0.4 cm |
| D15 | (Right)
adenosquamous carcinoma of the lung (upper lobe; invasive
moderately differentiated adenocarcinoma (alveolar type), ~50% of
the tumor component + moderately - poorly differentiated squamous
cell carcinoma, ~50% of the tumor component), mass size 1.2×1×0.5
cm |
| D16 | (Left) widening of
alveolar septa in the lungs (upper lobes) with interstitial fibrous
tissue hyperplasia, lymphocytic infiltration and carbon dust
deposition (Control group sample) |
| D17 | (Left) Invasive
adenocarcinoma (lower lobe of left lung; alveolar + papillary +
adnexal), size 1.5×1×0.7 cm |
| D18 | (Left) peripheral
type invasive adenocarcinoma of the lung (upper lobe; alveolar +
adnexal type), mass size 1.5×0.8×0.7 cm |
| D19 | (Right) peripheral
infiltrating adenocarcinoma of the lung (middle lobe; alveolar +
adnexal type), mass size 0.7×0.6×0.5 cm |
| D20 | (Right) invasive
mucinous adenocarcinoma of the lung (lower lobe), mass 1 cm in
diameter |
| D21 | (Left)
hypo-differentiated invasive adenocarcinoma of the lung (lower
lobe; predominantly sieve-like structures and solid areas), size
1.7×1.5×0.8 cm |
| D22 | (Right) peripheral
type microinvasive adenocarcinoma of the lung (middle lobe) with a
mass measuring 0.8×0.6×0.6 cm without definite pleural
invasion |
| D23 | (Upper lobe of left
lung) neuroendocrine tumor, combined with immunohistochemistry and
morphology consistent with small cell carcinoma (2 foci), the
larger measuring 1.2×1×0.8 cm |
| D24 | (Left) fine
bronchial adenoma of the lung (lower lobe), size 0.8×0.8×0.4 cm;
fibrous tissue hyperplasia and focal alveolar epithelial
hyperplasia with carbon dust deposition were seen in the
surrounding lung tissue (Control group sample) |
| D25 | (Right) peripheral
infiltrating moderately differentiated adenocarcinoma of the lung
(lower lobe; predominantly alveolar, partially adnexal and
papillary), mass size 1.5×1×0.6 cm |
| D26 | (Right)
microinvasive adenocarcinoma of the lung (upper lobe), mass size
0.7×0.6×0.5 cm |
| D27 | (Right)
microinvasive adenocarcinoma of the lung (upper lobe), mass size
1×0.8×0.6 cm |
| D28 | (Left) highly
differentiated invasive adenocarcinoma of the lung (upper lobe; a
lepidic-predominant pattern and focal acinar components), mass size
1.5×0.7×0.7 cm |
| D29 | (Left) peripheral
type invasive adenocarcinoma of the lung (upper lobe; alveolar +
adnexal type), mass size 2.5×1.3×1.3 cm |
| D30 | Microinvasive
adenocarcinoma (upper lobe of left lung), size 1.3×1.2×0.7 cm |
| D31 | (Right)
microinvasive adenocarcinoma of the lung (middle lobe), mass size
1.7×0.7×0.6 cm |
| D32 | (Right) peripheral
infiltrating moderately differentiated adenocarcinoma of the lung
(upper lobe; alveolar predominant type), mass size 1.4×1×0.8
cm |
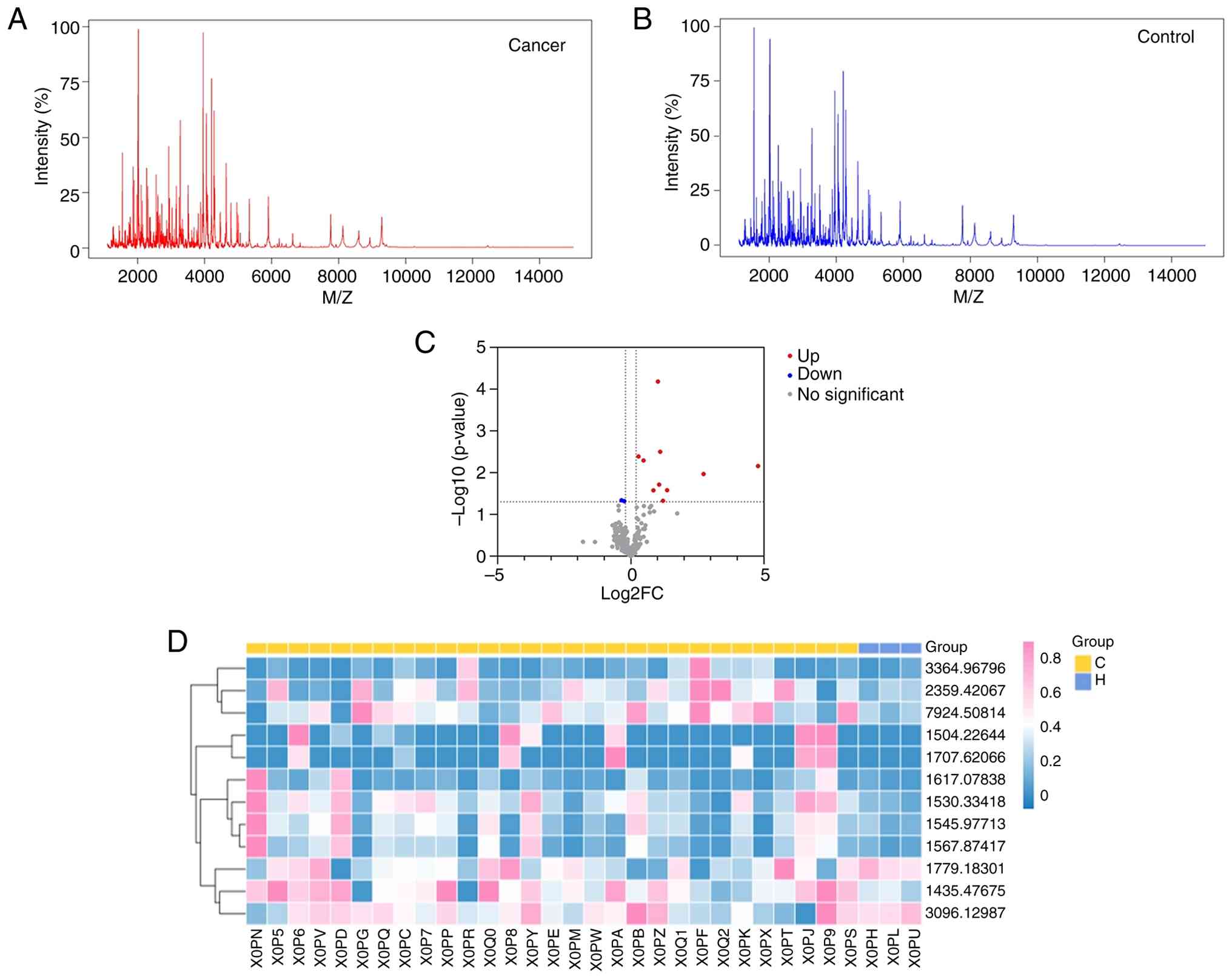
Serum peptidomic profiling and
differential peptide identification
The average peptide spectra for the cancer (n=29)
and control (n=3) groups are presented in Fig. 1A and B, respectively. Comparative
analysis identified 12 peptide signals that met the pre-defined
exploratory threshold for differential expression (|log2FC| >0.2
and P<0.05, Mann-Whitney U test; not corrected for multiple
testing). As shown in the volcano plot (Fig. 1C), 10 peptides were upregulated and
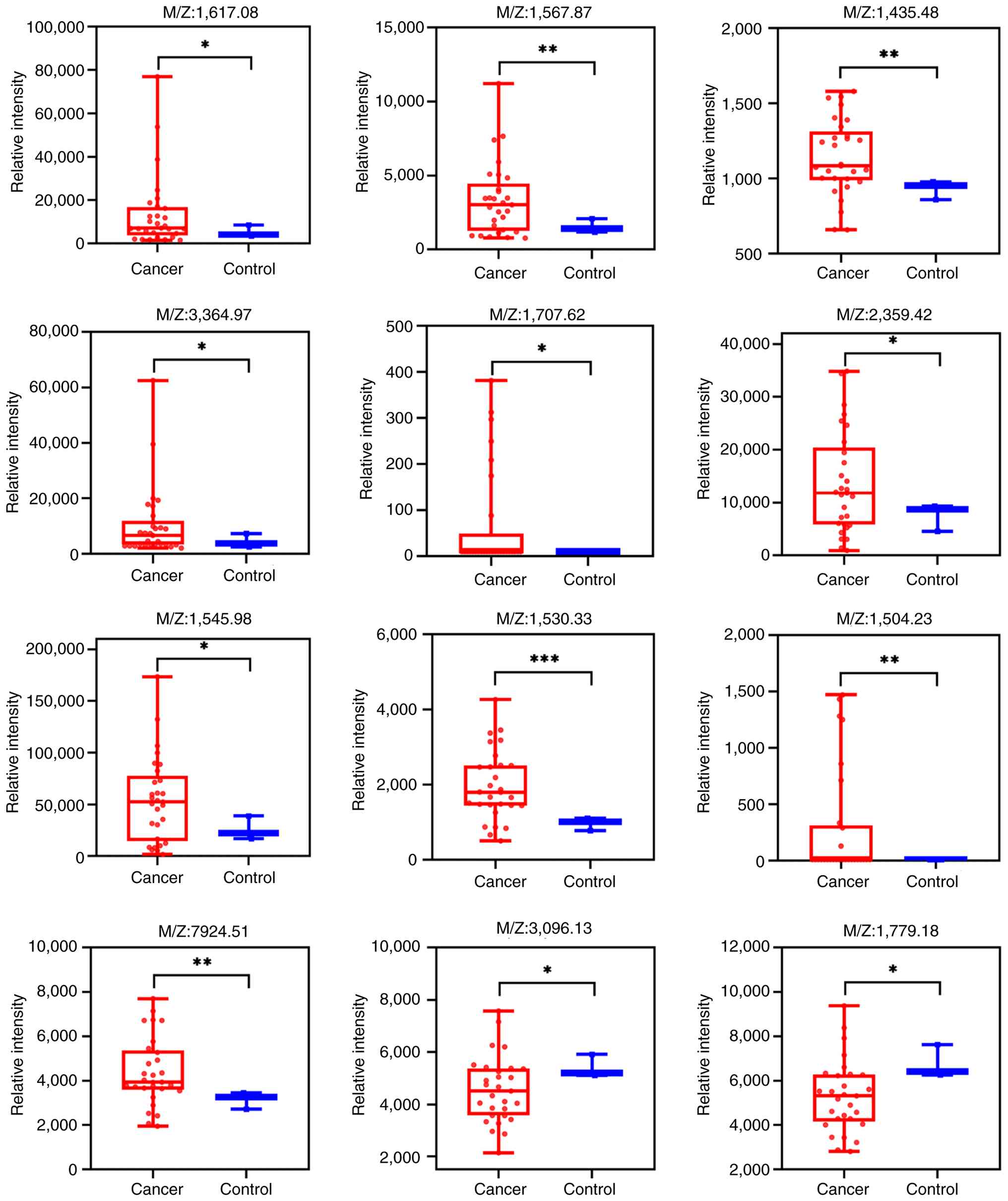
2 were downregulated in the cancer group. The clustering heatmap
(Fig. 1D) shows a general
separation trend between the two groups, and the expression
intensity distribution of these differential peptides is detailed
in the box plots (Fig. 2).
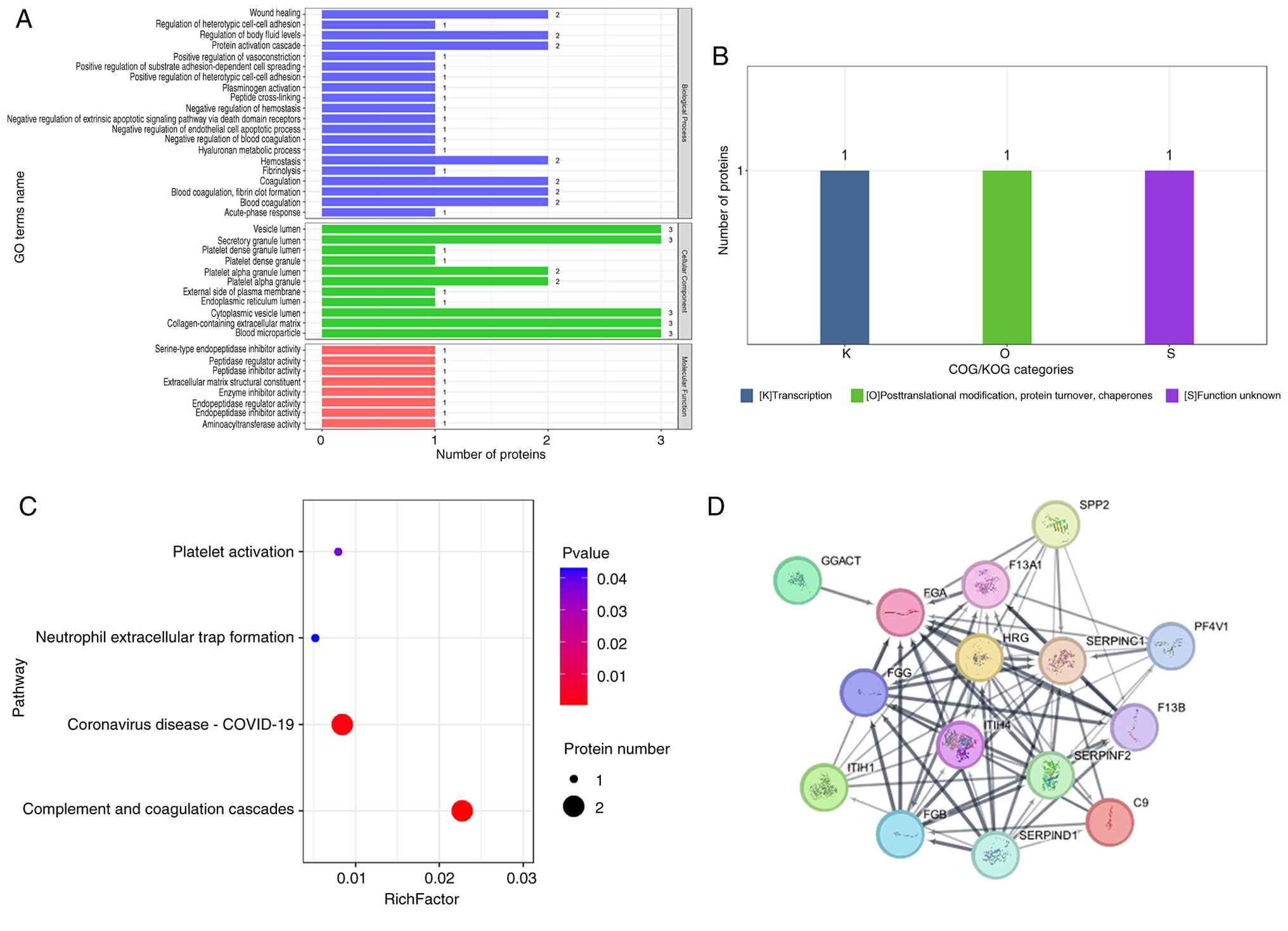
Biological annotation and pathway
analysis of candidate proteins
The 12 differential peptides mapped to three parent
proteins: Fibrinogen α chain (FGA), inter-α-trypsin inhibitor heavy
chain H4 (ITIH4) and coagulation factor XIII A chain (F13A1). GO
enrichment analysis (Fig. 3A;
Table SI) revealed that these
proteins were primarily enriched in biological processes such as
‘platelet alpha granule lumen’ and ‘blood coagulation, fibrin clot
formation’. COG/KOG functional classification (Fig. 3B) categorized the main function of
these differential proteins under ‘Posttranslational modification,
protein turnover, chaperones’ (Category O), Categories K
(transcription), O (posttranslational modification, protein
turnover, chaperones), and S (function unknown) were also observed.
KEGG pathway analysis (Fig. 3C)
indicated significant enrichment (P<0.05) in four pathways:
‘Platelet activation’, ‘Complement and coagulation cascades’,
‘Neutrophil extracellular trap formation’ and ‘Coronavirus
disease-COVID-19’. PPI network analysis further demonstrated
connectivity among these three candidate proteins (Fig. 3D).
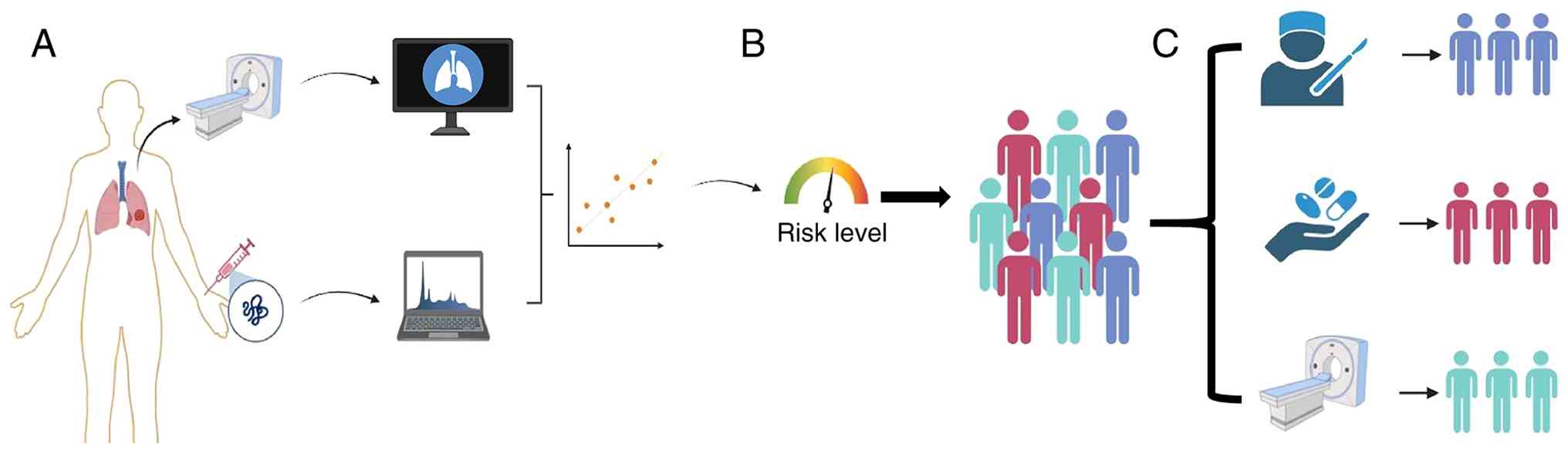
A conceptual framework for integrated
diagnosis
Based on the aforementioned findings, the present
study proposes a conceptual framework for future pulmonary nodule
management (Fig. 4). This
framework envisages the integration of validated multi-analyte
serum biomarker profiles with clinical and imaging data to achieve
more precise risk stratification. The utility of this strategy is
contingent upon rigorous future validation of the implicated
biomarkers.
Discussion
Th present preliminary exploratory study focused on
the diagnostic potential of serum-based biomarkers in lung cancer,
focusing on MALDI-TOF MS-based serum peptidomics.
In the exploratory peptidomic component of the
present study, MALDI-TOF MS was applied, which preliminarily
identified 12 peptides showing differential expression between lung
cancer and benign nodules within a small sample set. These peptides
map to three parent proteins: FGA, ITIH4 and F13A1. Functional
enrichment analyses revealed notable involvement of these candidate
proteins in pathways such as platelet activation, complement and
coagulation cascades and neutrophil extracellular trap formation.
These observations align with the well-established systemic
hypercoagulable state and local inflammatory responses frequently
observed in lung cancer (15,16).
Tumor-associated thrombosis is a common complication in patients
with lung cancer, potentially driven by coagulation-inflammation
crosstalk that promotes disease progression and metastasis
(17). FGA and F13A1, as core
components of the coagulation cascade, may reflect tumor
microenvironment remodeling and prothrombotic tendencies through
their fragmented peptides (18,19);
whereas ITIH4, an acute-phase protein, may represent a systemic
host response elicited by the tumor (20). Thus, the preliminarily screened
peptides in the present study provide initial clues and
hypothesis-generating directions for exploring serum diagnostic
biomarkers from the perspective of ‘coagulation-inflammation’
interplay in lung cancer.
However, it is crucial to emphasize the considerable
limitations inherent in the present study, particularly its
exploratory peptidomic component, which dictate the preliminary
nature of its findings. The primary limitation is the extremely
small sample size, particularly in the control group, which
comprised only three individuals with benign nodules. This severe
imbalance markedly reduces statistical power, rendering observed
differences more likely attributable to inter-individual variation
or chance rather than disease-specific signals. Secondly, owing to
the constrained sample size, no correction for multiple testing was
applied; the reported P-values carry a risk of false positives, and
the results should be regarded as descriptive rather than
confirmatory. Thirdly, the present study did not match or adjust
for key clinical confounders such as age, smoking history or
comorbidities, which can substantially influence the serum
peptidome and confound disease-associated interpretations.
Consequently, the principal value of this investigation lies in
demonstrating the technical feasibility of the MALDI-TOF MS-based
serum peptidomics workflow and generating a focused list of
candidate peptides for prioritized evaluation in future large-scale
validation studies, rather than proposing novel diagnostic
biomarkers.
Looking ahead, translating serum biomarkers into
routine clinical practice requires a concerted effort to address
several key challenges beyond sample-size limitations. Priority
must be given to adequate matching of relevant clinical confounders
in case-controlled studies. More importantly, there is an
imperative need for robust multicenter validation of single- and,
more promisingly, multi-analyte panels in large-scale prospective
cohorts. The future of cancer diagnostics lies in developing
integrated diagnostic models that combine the genetic specificity
of circulating tumor methylation, the rich proteomic information of
the peptidome and exosomes, and the cellular insights from
circulating tumor cells. Combining this multidimensional liquid
biopsy data with established clinical and radiographic parameters
will enable the development of reliable algorithms for personalized
risk stratification.
The primary challenge in evaluating pulmonary
nodules remains the need to facilitate timely intervention for
malignancy while minimizing invasive procedures for benign disease.
The high false-positive rate associated with LDCT underscores the
need for more precise diagnostic approaches. The integration of
imaging findings with emerging serum marker profiles, as
conceptualized in this work, represents a promising pathway toward
achieving superior risk stratification and personalized management.
This integrated approach aligns with the principles of precision
medicine, aiming to tailor interventions to each patient's unique
and dynamic profile.
In conclusion, while serum biomarkers represent a
frontier in lung cancer diagnostics with notable potential to
improve early detection and patient outcomes, their journey from
discovery to clinical utility is iterative and demands rigorous
validation. By embracing a framework of methodological rigor,
transparent reporting of limitations, as demonstrated in the
preliminary study and collaborative validation in large trials, the
field can move closer to making liquid biopsy an integral and
reliable component of precision oncology for lung cancer.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The present study was supported by funding from the National
Natural Science Foundation of China (grant no. 82472959,82273069),
the Tai Shan Young Scholar Foundation of Shandong Province (grant
nos. tsqn201909192 and tsqn202312383), the Shandong Province
Medical and Health Science and Technology Project (grant no.
202404020093), the Jining City Major Research and Development
Programs (grant no. 2024YXNS067) and the Jining Medical University
Affiliated Hospital Clinical Research Fund Project (grant no.
LCYJ-016).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author. The data generated in the
present study may be found in the ProteomeXchange Consortium under
accession number PXD072901 at the following URL: https://proteomecentral.proteomexchange.org.
Authors' contributions
QL, JS, HW, LN, BH and ZZ conceived and designed the
study, and wrote and edited the manuscript. QL and ZZ confirm the
authenticity of all the raw data. QL and JS analyzed the data. All
authors have read and approved the final manuscript.
Ethics approval and consent to
participate
All patients provided written informed consent, and
the present study was performed in accordance with the principles
of The Declaration of Helsinki. The present study was approved by
the Institutional Review Board of the Institute of Medical Science,
Affiliated Hospital of Jining Medical University (approval no.
2024-02-C011).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
NSCLC
|
non-small cell lung carcinoma
|
|
LDCT
|
low-dose computed tomography
|
References
|
1
|
Bray F, Laversanne M, Sung H, Ferlay J,
Siegel RL, Soerjomataram I and Jemal A: Global cancer statistics
2022: GLOBOCAN estimates of incidence and mortality worldwide for
36 cancers in 185 countries. CA Cancer J Clin. 74:229–263.
2024.PubMed/NCBI
|
|
2
|
Doctors O: In Health at a Glance 2021:
OECD indicators. OECD Publishing; Paris, France: 2021
|
|
3
|
Boukansa S, Benbrahim Z, Gamrani S, Bardai
S, Bouguenouch L, Mazti A, Boutahiri N, Serraj M, Amara B,
Ouadnouni Y, et al: Correlation of epidermal growth factor receptor
mutation with major histologic subtype of lung adenocarcinoma
according to IASLC/ATS/ERS classification. Cancer Control. Mar
29–2022.(Epub ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zappa C and Mousa SA: Non-small cell lung
cancer: Current treatment and future advances. Transl Lung Cancer
Res. 5:288–300. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Uramoto H and Tanaka F: Recurrence after
surgery in patients with NSCLC. Transl Lung Cancer Res. 3:242–249.
2014.PubMed/NCBI
|
|
6
|
Sasaki H, Suzuki A, Tatematsu T, Shitara
M, Hikosaka Y, Okuda K, Moriyama S, Yano M and Fujii Y: Prognosis
of recurrent non-small cell lung cancer following complete
resection. Oncol Lett. 7:1300–1304. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rajaram R, Huang Q, Li RZ, Chandran U,
Zhang Y, Amos TB, Wright GWJ, Ferko NC and Kalsekar I:
Recurrence-free survival in patients with surgically resected
non-small cell lung cancer: A systematic literature review and
meta-analysis. Chest. 165:1260–1270. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Siegel RL, Miller KD, Wagle NS and Jemal
A: Cancer statistics, 2023. CA Cancer J Clin. 73:17–48.
2023.PubMed/NCBI
|
|
9
|
Martínez-Ruiz C, Black JRM, Puttick C,
Hill MS, Demeulemeester J, Larose Cadieux E, Thol K, Jones TP,
Veeriah S, Naceur-Lombardelli C, et al: Genomic-transcriptomic
evolution in lung cancer and metastasis. Nature. 616:543–552. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Jeong Y, Hellyer JA, Stehr H, Hoang NT,
Niu X, Das M, Padda SK, Ramchandran K, Neal JW, Wakelee H and Diehn
M: Role of KEAP1/NFE2L2 mutations in the chemotherapeutic response
of patients with non-small cell lung cancer. Clin Cancer Res.
26:274–281. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
National Lung Screening Trial Research
Team, . Aberle DR, Adams AM, Berg CD, Black WC, Clapp JD,
Fagerstrom RM, Gareen IF, Gatsonis C, Marcus PM and Sicks JD:
Reduced lung-cancer mortality with low-dose computed tomographic
screening. N Engl J Med. 365:395–409. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Takiguchi Y, Sekine I and Iwasawa S:
Overdiagnosis in lung cancer screening with low-dose computed
tomography. J Thorac Oncol. 8:e101–2. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Dammak S, Gulstene S, Palma DA, Mattonen
SA, Senan S and Ward AD: Distinguishing recurrence from
radiation-induced lung injury at the time of RECIST progressive
disease on post-SABR CT scans using radiomics. Sci Rep.
14:37582024. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ma L, Guo H, Zhao Y, Liu Z, Wang C, Bu J,
Sun T and Wei J: Liquid biopsy in cancer: Current status,
challenges and future prospects. Sig Transduct Target Ther.
9:3362024. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Charpidou A, Gerotziafas G, Popat S,
Araujo A, Scherpereel A, Kopp HG, Bironzo P, Massard G, Jiménez D,
Falanga A, et al: Lung cancer related thrombosis (LCART): Focus on
immune checkpoint blockade. Cancers. 16:4502024. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Di W, Xu H, Xue T and Ling C: Advances in
the prediction and risk assessment of lung cancer-associated venous
thromboembolism. Cancer Manag Res. 13:8317–8327. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Myrou A, Penopoulos A, Barmpagiannos K,
Ouzouni S and Girtovitis F: Coagulation abnormalities in lung
cancer: Diagnostic challenges and therapeutic perspectives. Clin
Appl Thromb Hemost. 31:107602962513592932025. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Raungrut P, Jirapongsak J, Tanyapattrapong
S, Bunsong T, Ruklert T, Kueakool K, Thongsuksai P and Nakwan N:
Fibrinogen alpha chain as a potential serum biomarker for
predicting response to cisplatin and gemcitabine doublet
chemotherapy in lung adenocarcinoma: Integrative transcriptome and
proteome analyses. Int J Mol Sci. 26:10102025. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Luo Y, Li B, Li J, Zhang Y, Deng M, Hu C,
Yan W, Zhou Z and Zhang G: Coagulation Factor XIII subunit a is a
biomarker for curative effects and prognosis in malignant solid
tumors, Especially non-small cell lung cancer. Front Oncol.
11:7190852021. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wu X, Chen J, Sun W, Hart DA, Ackermann PW
and Ahmed AS: Network proteomic analysis identifies
inter-alpha-trypsin inhibitor heavy chain 4 during early human
Achilles tendon healing as a prognostic biomarker of good long-term
outcomes. Front Immunol. 14:11915362023. View Article : Google Scholar : PubMed/NCBI
|