Introduction
Prostate cancer (PCa) is the second most prevalent cancer type among men worldwide, with an estimated 1,466,680 new cases and 396,792 deaths reported in 2022 (1). The global increase in PCa cases can be attributed to an aging demographic and shifts in lifestyle choices. This trend is particularly pronounced in China, where it has emerged as a major public health concern (2). Worldwide, PCa is the second most common cancer in men, with both the number of new diagnoses and death rates increasing rapidly (3). The symptoms of PCa vary widely; early stages often show no symptoms, and variations in access to screening and healthcare can result in late diagnoses, causing many individuals to be diagnosed at more advanced stages (2,4). Poor treatment results for metastatic PCa severely affect both the survival rates and the overall quality of life of patients (5). These issues highlight the pressing need for more targeted and effective treatment options.
The tumor microenvironment (TME) orchestrates a complex immunosuppressive network composed of various immune cells, stromal elements and soluble substances (6). Regulatory T cells (Tregs) are recognized as key players in the maintenance of immune tolerance and suppression (7). Tregs primarily promote tumor immune evasion by inhibiting the growth and activity of effector T cells, which is a fundamental aspect of cancer-related immunosuppression (8,9). In PCa, the presence of Tregs is significantly linked to an immunosuppressive TME and is often associated with unfavorable outcomes in immunotherapy and disease progression (10,11). Tregs utilize a range of immunosuppressive strategies, such as releasing cytokines, including interleukin-10 (IL-10) and transforming growth factor-β (TGF-β), expressing high levels of immune checkpoint proteins such as cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) and programmed cell death protein 1 (PD-1) and disrupting metabolic processes (12,13). Their recruitment, growth and activation are regulated by a complex network of signaling pathways and transcription factors, including signal transducer and activator of transcription 3 (STAT3), interferon regulatory factor 4 and chemokines produced by tumors, which influence Treg differentiation, longevity and suppression capabilities (14–16).
Owing to their essential functions, focusing on Tregs has become a promising approach to boost anti-tumor immunity and address challenges in immunotherapy (17,18). For example, antibodies targeting glycoprotein A repetitions predominant or CTLA-4 have shown strong immune-stimulating effects in both laboratory and clinical settings (12,18). Additionally, leveraging artificial intelligence alongside multi-omics data may help identify patient groups that are most likely to benefit from therapies targeting Tregs (19,20). Therefore, gaining a more comprehensive understanding of Treg biology and their regulatory systems is vital for the development of innovative immunotherapeutic methods for PCa.
The central role of Tregs in immune evasion is not unique to PCa; it is a common feature in numerous solid tumor types. For instance, in melanoma and lung cancer, Treg infiltration is similarly associated with poor prognosis and resistance to immunotherapy, leading to the successful clinical deployment of Treg-targeting agents, such as anti-CTLA-4 ipilimumab (9,12). However, the PCa TME is notoriously ‘cold’ and immunosuppressive, often exhibiting lower baseline T-cell infiltration and a greater reliance on myeloid-derived suppressor cells (MDSCs) and androgen signaling compared to ‘hot’ tumors like melanoma (21,22). This distinct immunological landscape suggests that Treg-targeting strategies that are effective in other cancers may require adaptation, such as a combination with androgen deprivation therapy (ADT) or myeloid-modulating agents, to achieve similar efficacy in PCa (23,24).
This review intends to comprehensively consolidate information regarding the formation, functional traits and regulatory frameworks of Tregs in the context of the PCa microenvironment. The influence and therapeutic possibilities of both current and novel approaches on Treg activity, such as monoclonal antibody (mAb) treatments and combination immunotherapies, were assessed. Additionally, the potential for clinical applications and the challenges faced by Treg-targeting methods were explored. By merging basic research with clinical progress, this review aimed to establish a conceptual basis and offer fresh insights into immunotherapy for PCa, with a particular focus on translating the growing understanding of Treg subset heterogeneity and spatial dynamics into more effective and precise targeted treatment strategies.
Biology of Tregs in PCa
Tregs are a unique group of CD4+ T cells that play a crucial role in preserving tolerance. However, within the TME, they are often used to inhibit the body's anti-tumor immune responses. This section explores their development, mechanisms of suppression and specific functional characteristics in relation to PCa (Fig. 1).
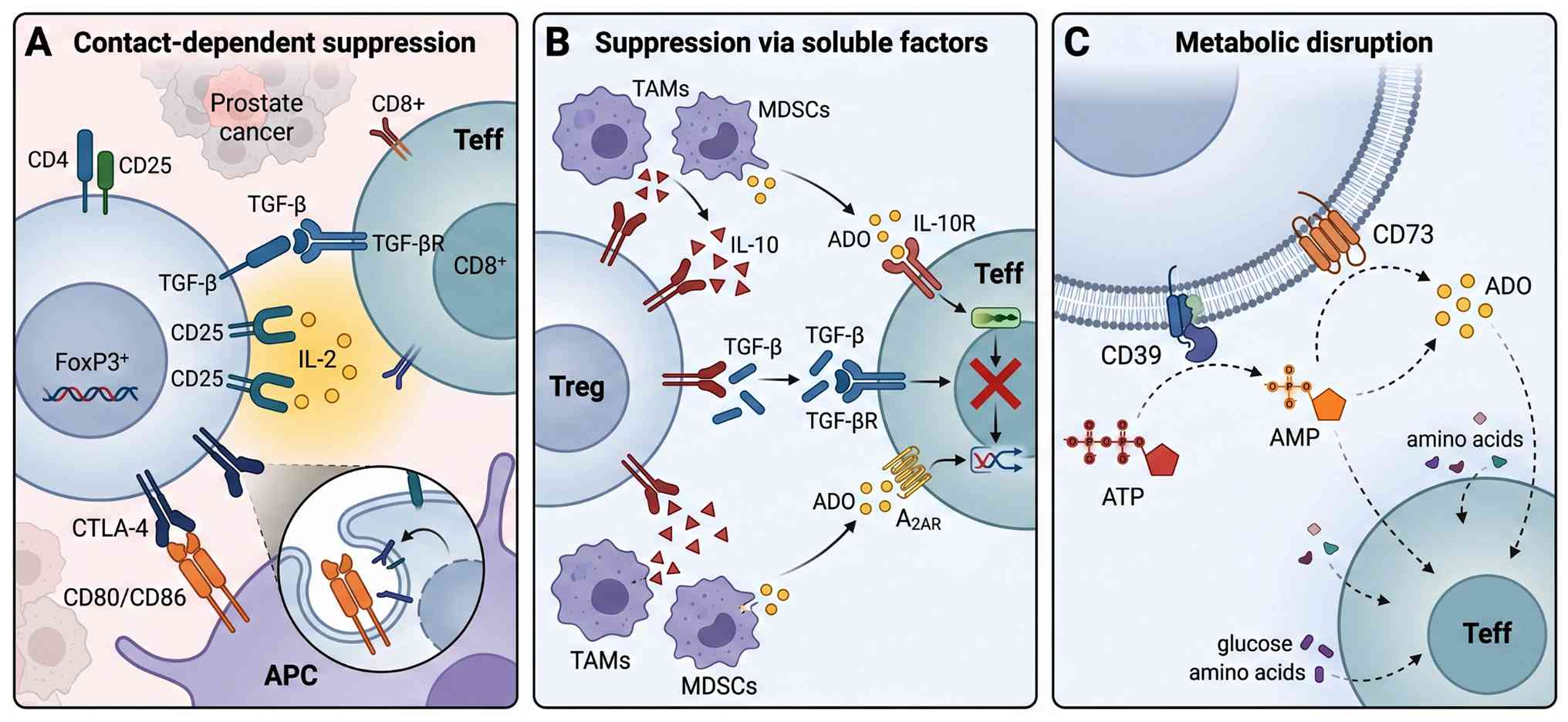 |
Figure 1.
Immunosuppressive mechanisms of Tregs in the prostate cancer microenvironment. (A) Contact-dependent suppression. Tregs suppress Teff through membrane-bound TGF-β and by sequestering IL-2 via the high-affinity CD25. Tregs also express CTLA-4, which mediates trans-endocytosis of CD80/CD86 from APCs. (B) Suppression via soluble factors. Tregs and other cells produce soluble factors such as IL-10, TGF-β and ADO to suppress Teff function. (C) Metabolic disruption. Tregs express ectoenzymes CD39 and CD73, which convert ATP/AMP to immunosuppressive ADO, depriving Teff of essential growth factors and metabolites. ADO, adenosine; AMP, adenosine monophosphate; APC, antigen-presenting cell; ATP, adenosine triphosphate; CD25, cluster of differentiation 25 (IL-2 receptor α chain); CD39, ectonucleoside triphosphate hydrolase 1; CD73, ecto-5′-nucleotidase; CTLA-4, cytotoxic T-lymphocyte-associated protein 4; IL-2, interleukin-2; IL-10, interleukin-10; p-STAT5, phosphorylated signal transducer and activator of transcription 5; SMAD2/3, mothers against decapentaplegic homolog 2/3; Teff, effector T cell; TGF-β, transforming growth factor-β; Treg, regulatory T cell.
|
Development and immunosuppressive mechanisms of Tregs
Tregs are mainly characterized by the expression of the transcription factor forkhead box (Fox)p3, which serves as a key regulator of their development and functionality (25–27). They have two main origins: Natural Tregs that develop in the thymus (tTregs) and those induced in the periphery (iTregs) (28). tTregs undergo maturation in the thymus, where the stable expression of Foxp3 is enhanced through epigenetic changes, ensuring their commitment to a long-term immunosuppressive role (29,30). However, iTregs are formed from conventional CD4+ T cells outside the thymus, primarily influenced by TGF-β signaling (31).
Tregs utilize a variety of strategies to inhibit immune reactions: i) They release suppressive cytokines, including IL-10 and TGF-β (32); ii) they exhibit elevated levels of immune checkpoint proteins, such as CTLA-4, which reduces the activity of antigen-presenting cells (APCs) (33); iii) they interfere with metabolism through enzymes like CD73, leading to the production of immunosuppressive adenosine (34,35); and iv) they can directly kill effector cells (36).
Proper functioning of Tregs is influenced by multifaceted interactions between transcriptional control, epigenetic changes and metabolic processes (37). Key signaling pathways form an interconnected network that governs Treg identity and function. The phosphoinositide 3-kinase (PI3K)-Akt pathway, particularly the PI3Kδ isoform, is essential for maintaining Treg homeostasis and suppressive capacity; its disruption impairs Treg stability and function (38,39). Downstream of the IL-2 receptor, the JAK-STAT5 pathway is indispensable for sustaining Foxp3 expression and regulating Treg survival. In the PCa TME, Tregs exploit this pathway by outcompeting effector T cells for IL-2, leading to effector T-cell exhaustion (40). This signaling axis is further integrated with Treg-intrinsic TGF-β signaling mediated by SMAD transcription factors, which are critical for the differentiation and functional stability of iTregs in the periphery (31). Together, these pathways orchestrate a transcriptional program that reinforces Treg lineage stability and the suppressive machinery. Non-coding RNAs, including microRNAs and long non-coding RNAs, add another layer of regulatory complexity, modulating Treg adaptability in different disease contexts (41,42).
Phenotype and function of Tregs in the PCa TME
In PCa, Tregs exhibit unique features that highlight their function in facilitating tumor immune evasion (43–45). Research involving both clinical trials and animal studies has repeatedly shown a notable increase in Treg populations within PCa tissues and the bloodstream, which is frequently linked to unfavorable patient outcomes (46–48). For example, in a natural canine model of PCa, the presence of Tregs within tumors served as a negative prognostic factor, emphasizing their consistent role across different species (49).
At the molecular level, Tregs in PCa exhibit significant heterogeneity, with specific subsets driving immunosuppression (50). Single-cell RNA sequencing analyses in patients with high-risk PCa have identified not only an increase in Tregs, but also the predominance of an activated, highly suppressive subset characterized by elevated expression of CTLA-4, inducible T cell costimulator (ICOS) and TNF receptor superfamily member 9 (4-1BB). This subset is spatially associated with exhausted CD8+ T cells, collectively sculpting a profoundly immunosuppressive TME (51). Furthermore, spatial transcriptomics have revealed that Tregs residing within the tumor stroma, particularly those in close proximity to M2-polarized tumor-associated macrophages (TAMs), are key drivers of immune exclusion and are strongly linked to biochemical recurrence (52,53). These findings underscore the necessity of moving beyond total Treg counts to characterize functional subpopulations and their spatial niches.
The immunosuppressive capabilities of Tregs are significantly enhanced by their interaction with various myeloid cells present in the TME, including TAMs and MDSCs (54,55). Research on the spatial dynamics of the PCa TME has revealed that the presence of Tregs within the stroma is a crucial indicator of biochemical recurrence, a conclusion supported by numerous patient studies (52). This arrangement, which typically shows Tregs situated near immunosuppressive M2 macrophages, is a characteristic of a high-risk immune environment (52).
Emerging therapeutic approaches have focused on targeting Tregs in PCa (56,57). The use of nanoparticles to deliver small inhibitory RNAs targeting essential Treg transcription factors, including basic leucine zipper ATF-like transcription factor (BATF) and PR domain zinc finger protein 1 (PRDM1), significantly inhibits Treg activity and slows tumor progression (58,59). Additionally, ADT triggers a complex immune reorganization, resulting in an increase in both CD8+ T cells and Tregs in the TME. This indicates that combining ADT with agents targeting Tregs may improve treatment outcomes (60–62).
Immune cell interactions in the PCa microenvironment
The effectiveness of anti-tumor immunity in PCa is significantly influenced by the ongoing interactions between Tregs and various immune cells in the TME. This section emphasizes how Tregs directly inhibit effector cells and their mutual interactions with macrophages associated with tumors.
Treg-mediated suppression of effector T cells
The relationship between Tregs and effector T cells, especially CD8+ cytotoxic T cells, is fundamental for immune suppression in PCa (40). This dynamic significantly influences the effectiveness of anti-tumor immune responses and treatment results (40). Tregs deploy multiple well-defined mechanisms to suppress effector T cells, including sequestration of IL-2 via CD25 (which reduces CD8+ T-cell proliferation by >50% in the PCa TME), secretion of TGF-β and IL-10 (which inhibit cytotoxic granule release) and CTLA-4-mediated trans-endocytosis of CD80/CD86 from antigen-presenting cells. These coordinated actions collectively impair anti-tumor immunity and correlate with reduced patient survival (63,64).
Mechanisms of direct suppression
One key mechanism involves the release of immunosuppressive cytokines (64). For example, TGF-β (whose immunosuppressive mechanisms are detailed above) not only directly hinders the growth and cytotoxic functions of CD8+ T cells but can also lead them into a state of exhaustion (65). Additionally, Tregs consistently express the high-affinity IL-2 receptor (CD25), which enables them to compete for and reduce local IL-2 levels. This reduction in IL-2 levels deprives the effector T cells of an essential growth factor, resulting in their diminished functionality. In PCa, the sequestration of IL-2 by Tregs activates the IL-2/STAT5 signaling pathway within Tregs, while also contributing to the exhaustion of CD8+ T cells (40). Imaging studies have shown that the close proximity of Tregs to effector T cells in the TME enhances these suppressive interactions, which are mediated by both direct contact and cytokines (40).
Indirect inhibition through APCs
Tregs can also indirectly inhibit T-cell responses indirectly by influencing APCs (66). For instance, Tregs may inhibit type 1 conventional dendritic cells (DC1s) located in lymph nodes associated with tumors via major histocompatibility complex II-dependent interactions, which hinders the initial activation of naive CD8+ T cells (67). Additionally, the downregulation of co-stimulatory molecules, such as CTLA-4 on Tregs, boosts their inhibitory effects by interacting with CD80/CD86 on APCs, leading to the transmission of suppressive signals or the degradation of these co-stimulatory ligands (68).
Coordination by additional immune cells
Inhibitory networks are frequently managed by various stromal elements. TAMs have the ability to attract both Tregs and CD8+ T cells through the C-X-C motif chemokine ligand/C-X-C chemokine receptor type 4 pathway, facilitating their interaction and promoting suppression (40). Likewise, mast cells that infiltrate tumors and are activated by IL-33 secrete IL-2, which selectively promotes the growth of ICOS+ Tregs and subsequently inhibits the activity of CD8+ T cells (69).
Cross-talk between Tregs and TAMs
Tregs and TAMs engage reciprocally, which amplifies immunosuppression. In the PCa TME, TAMs recruit Tregs and promote their differentiation (55,70). In turn, Tregs reinforce the immunosuppressive milieu by secreting key cytokines. As detailed in the above chapter, Treg-derived IL-10 and TGF-β are potent drivers of macrophage polarization toward a pro-tumor M2-like phenotype (characterized by CD163 and CD206 expression) (71–77). This reciprocal interaction establishes a positive feedback loop: M2-polarized TAMs further recruit Tregs via chemokine axes [e.g., C-C motif chemokine ligand (CCL)17/C-C motif chemokine receptor (CCR)4] and promote iTreg differentiation via TGF-β and PD-1/programmed death ligand 1 (PD-L1) interactions (78,79) (Fig. 2).
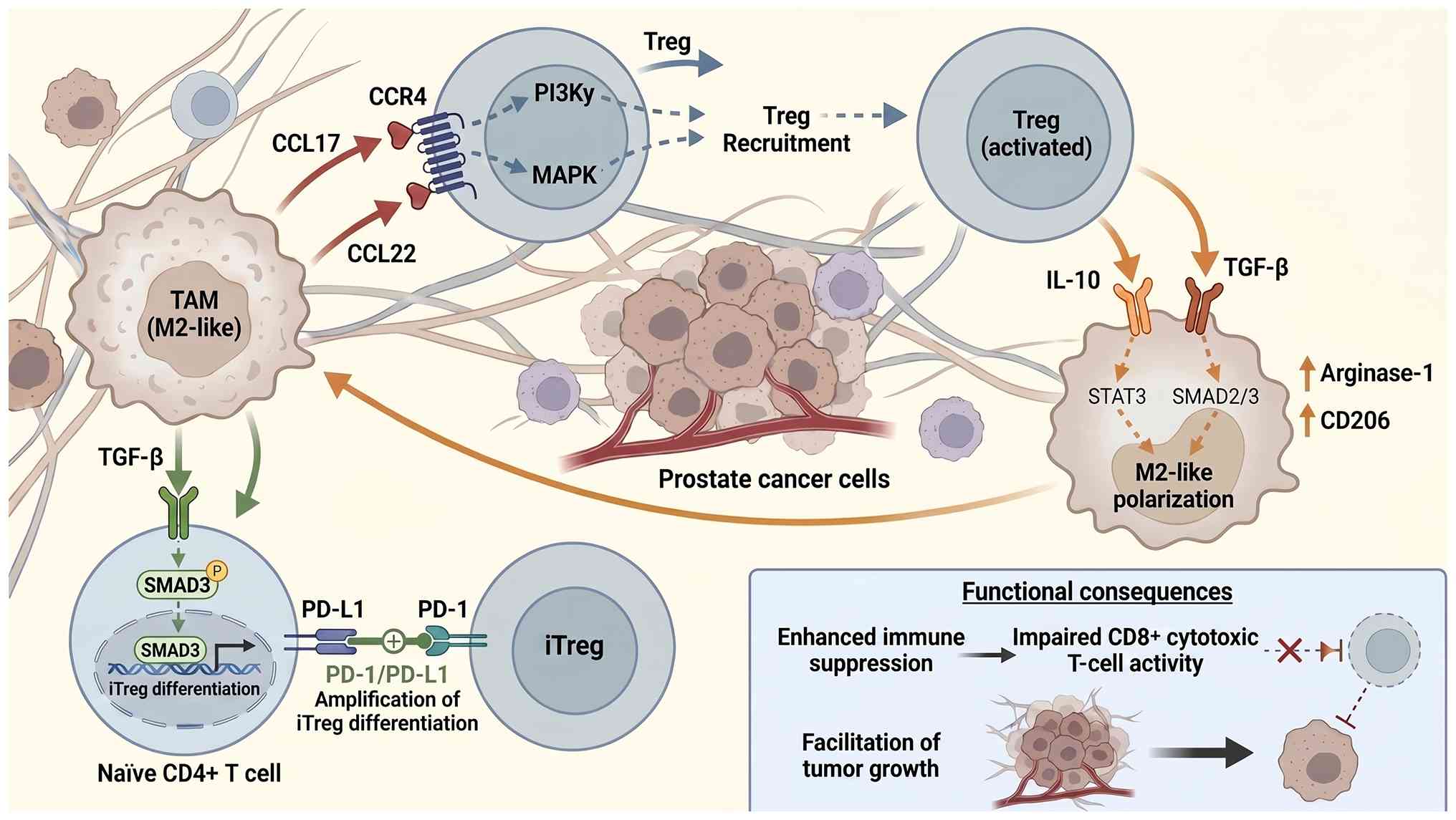 |
Figure 2.
The TAM immunosuppressive feedback loop in the prostate cancer microenvironment. TAMs release CCL17/CCL22, which bind to CCR4 on Tregs, recruiting them into the tumor site via PI3Kγ and MAPK signaling pathways. TAM-derived TGF-β activates SMAD3 in naïve CD4+ T cells, driving their differentiation into iTregs. This process is further augmented by PD-1/PD-L1 interactions. Reciprocally, Tregs secrete IL-10 and TGF-β, which act on macrophages via STAT3 and SMAD2/3 signaling, driving their polarization towards a pro-tumor M2-like phenotype (characterized by arginase-1 and CD206 expression). This reciprocal crosstalk establishes a self-reinforcing loop that enhances overall immune suppression, impairs CD8+ cytotoxic T-cell activity and facilitates tumor growth. CCL, C-C motif chemokine ligand; CCR4, C-C motif chemokine receptor 4; CD4, cluster of differentiation 4; CD8, cluster of differentiation 8; CD25, cluster of differentiation 25; CD206, cluster of differentiation 206; FoxP3, forkhead box P3; IL-10, interleukin-10; iTreg, induced regulatory T cell; MAPK, mitogen-activated protein kinase; PD-1, programmed cell death protein 1; PD-L1, programmed death-ligand 1; PI3Kγ, phosphoinositide 3-kinase γ; SMAD2/3, mothers against decapentaplegic homolog 2/3; SMAD3, mothers against decapentaplegic homolog 3; STAT3, signal transducer and activator of transcription 3; TAM, tumor-associated macrophage; TGF-β, transforming growth factor-β; Treg, regulatory T cell.
|
Heterogeneity of suppressive Treg subsets in the PCa TME
Tregs are not a uniform population, and single-cell analyses have begun to dissect the specific subsets driving immunosuppression in PCa (51,52). The most suppressive subset identified in the PCa TME is the CD45 isoform RA-Foxp3 activated effector Treg (eTreg) population. These cells exhibit a highly activated transcriptional program characterized by the upregulation of co-inhibitory molecules (CTLA-4 ‘high’, ICOS ‘high’, T cell immunoreceptor with Ig and ITIM domains ‘high’), TNF receptor family members (tumor necrosis factor receptor superfamily, member 18 ‘high’, 4-1BB ‘high’) and cytokines (IL-32) (51). Spatially, these highly suppressive eTregs are often localized in the tumor stroma, frequently in close proximity to M2-polarized TAMs, creating an immunosuppressive niche associated with CD8+ T-cell exclusion and exhaustion (52,79). Other subsets, such as tissue-resident Tregs marked by the transcription factors BATF and PRDM1, have also been implicated in therapy resistance, as silencing these factors can abrogate Treg suppression (58). The presence of these specific subsets, rather than the total Treg count, is strongly linked to biochemical recurrence and poor prognosis, highlighting the need for subset-specific targeting strategies (51–53).
Tregs as determinants of prognosis in PCa
The presence and activity levels of Tregs in the tumor immune microenvironment play a vital role in determining clinical outcomes in PCa. This section examines the potential of Tregs as indicators of prognosis and prediction, as well as how the immunosuppressive environment to which they contribute to is linked to disease recurrence and advancement.
Tregs as prognostic and predictive biomarkers
The presence of Foxp3+ Tregs is a significant factor affecting patient prognosis in different types of cancer (80). In PCa, a higher concentration of these Tregs is often linked to lower survival rates, suggesting their potential role as biomarkers for disease categorization (46,81). This predictive significance is consistent across various cancers; for example, elevated levels of Foxp3+ Tregs in the peripheral blood are associated with unfavorable outcomes in hepatocellular carcinoma, and in triple-negative breast cancer, their prevalence is inversely related to the effectiveness of neoadjuvant chemotherapy (82–85).
Both transcriptomic and immunological studies have consistently revealed the immunosuppressive functions of Tregs in PCa (45). Advanced machine learning techniques have been utilized to create prognostic tools, including tumor-infiltrating lymphocytes (TIL) TregSig, which can accurately forecast patient outcomes and responses to immunotherapy by analyzing the characteristics of tumor-infiltrating Tregs (61). Additionally, genes associated with the cell cycle, such as the origin recognition complex 6, demonstrate a positive relationship with Treg infiltration in PCa, and their elevated expression correlates with an unfavorable patient prognosis, indicating that gene expression linked to Tregs may act as a valuable molecular prognostic indicator (86–88).
The relationship between Tregs and immune checkpoints has significant prognostic value. In solid tumors, the presence of PD-L1 is frequently associated with Foxp3 + Treg infiltration (89). A comparable mechanism may be present in PCa, in which pathways associated with Tregs foster an immunosuppressive environment that influences both patient survival and treatment response (88). Importantly, Foxp3-high Tregs that infiltrate tumors can be drawn from the bloodstream through the CCR5-CCL5 pathway, and their levels in the peripheral blood may serve as indicators of survival and early recurrence, underscoring their potential as non-invasive prognostic markers (90).
The immunosuppressive microenvironment and clinical outcomes
The density of Tregs infiltrating the PCa microenvironment is a significant prognostic factor (91). Analyses of various datasets, including the Cancer Genome Atlas and Gene Expression Omnibus, have indicated that elevated Treg levels in PCa tissues correlate with reduced disease-free survival and a heightened likelihood of biochemical recurrence (92). Prognostic models that focus on different biological mechanisms, such as ferroptosis and pyroptosis, consistently highlight the role of Tregs, with high-risk patient cohorts showing increased Treg infiltration and the activation of immunosuppressive pathways (48,93,94).
The arrangement of immune cells in tumors plays a vital role. In cases of high-risk PCa, there is a notable increase in Tregs and M2 macrophages within both the tumor stroma and epithelial areas, contributing to an immunosuppressive environment linked to increased recurrence rates (55,95). Single-cell sequencing data indicate that tissues from high-grade, high-Gleason score PCa show a marked increase in Tregs, which is associated with a phenotype of T-cell exhaustion characterized by elevated levels of PD-1 and CTLA-4 (96).
Multiple independent studies, including single-cell RNA-sequencing and spatial transcriptomics, have conclusively demonstrated that high Treg infiltration is associated with CD8+ T cell exhaustion [as measured by increased PD-1 and hepatitis A virus cellular receptor 2 (HAVCR2, also known as T-cell immunoglobulin and mucin domain containing 3) expression] and a 2- to 3-fold higher risk of biochemical recurrence in patients with PCa (51,52,96). These data establish Tregs as a clinically detrimental component of the anti-tumor immune response. Treatments, such as ADT, which promote the infiltration of various immune cells, can also lead to an increase in the population of immunosuppressive Tregs. This results in complex and often negative alterations in the immune environment (23,97). Furthermore, a high presence of Tregs is frequently associated with increased levels of immune checkpoint proteins, such as PD-L1 and lymphocyte-activation gene 3, implying that patients with this profile may experience reduced efficacy of immune checkpoint inhibitors (ICIs) (98). Therefore, focusing on Tregs and their related pathways is viewed as a promising approach to enhance the effectiveness of immunotherapy and improve survival rates in patients with PCa (99,100).
Modulation of Tregs by conventional PCa therapies
Standard approaches for managing PCa, particularly hormone therapy and radiation treatment, have intricate and sometimes contradictory effects on the immune environment, notably influencing Treg cell populations. Understanding these treatment-induced immune changes is essential for developing successful combination therapies.
Effects of endocrine therapy on Tregs
Hormonal treatment, a fundamental aspect of PCa management that disrupts androgen signaling, plays a crucial role in altering the immune landscape of tumors, particularly by affecting the presence and activity of Tregs (101,102). In cases of PCa that are resistant to hormonal therapy, the TME becomes significantly immunosuppressive, marked by a heightened presence of Tregs (10). This phenomenon is partially driven by the flightless I homolog (FLII)/Y-box binding protein (YBX1)/PD-L1 signaling pathway; enhancing FLII levels can counteract this effect, diminish Treg presence and reactivate CD8+ T cells, suggesting that hormonal therapy indirectly affects Tregs through this mechanism (103).
Hormonal treatments also influence Tregs via various immune modulation mechanisms (104). The enzyme cyclooxygenase-2 and its byproduct, prostaglandin E2 (PGE2), facilitate the ability of tumors to evade the immune system by interacting with the EP4 receptor. PGE2 aids in the development and proliferation of MDSCs and Tregs, while simultaneously suppressing the activity of natural killer cells (105). Blocking the EP4 receptor can reduce the functions of MDSCs and Tregs, while enhancing the maturation of effector T cells. This indicates that pairing hormonal therapy with EP4 blockers may enhance treatment effectiveness by targeting Tregs (24).
While PCa primarily relies on androgens, the role of estrogen signaling also plays a significant role in immune modulation (106). In different scenarios, like endometriosis, the estrogen-estrogen receptor α pathway facilitates the growth and immunosuppressive characteristics of Tregs (107). Blocking this pathway decreases both the quantity and effectiveness of Tregs. This indicates that hormonal treatments can affect Treg behavior by modifying extensive hormone receptor signaling.
The dual role of radiotherapy in shaping Treg dynamics
Radiotherapy is a key localized treatment for PCa and causes notable alterations in the immune microenvironment of tumors, often resulting in complex and at times counterproductive effects on Tregs (108,109). Research using preclinical models indicates that high-dose fractionated radiotherapy initiates dynamic immune reactions. This process begins with an increase in the number of MDSCs, followed by an increase in the number of active CD8+ TILs. Nevertheless, there is frequent concurrent growth of Tregs, which can create an immunosuppressive setting that hinders the overall effectiveness of the antitumor immune response (110).
Research has indicated that RT parameters have a significant effect on systemic immune responses (111). Factors, such as the clinical target volume and the amount of bone marrow exposed to 20 Gy, are linked to variations in peripheral immune cell counts. Increased volumes of radiation tend to lead to an early decline in antitumor immune activity, resulting in negative alterations in Tregs and CD8+ T-cell populations (112,113). Even sophisticated techniques, such as carbon ion radiotherapy, which can stimulate lymphocyte growth and activity in patients with PCa, are associated with an increase in Treg levels, underscoring the simultaneous activation of immune suppression mechanisms (114,115).
The processes facilitating Treg growth after radiotherapy are complex and varied. They involve the secretion of immunosuppressive agents, such as TGF-β and IL-10 (whose roles in Treg development and suppression are detailed further above), along with the attraction of Tregs by TAMs and MDSCs through chemokine pathways (79,116). Furthermore, radiotherapy has the potential to transform standard CD4+ T cells into Tregs, a phenomenon observed in models of head and neck cancer, and blocking the complement C3a/C5a pathway enhances this transformation (117).
Research is currently focused on methods to address the accumulation of Tregs caused by radiotherapy (118). Using low-dose cyclophosphamide to deplete Tregs, in conjunction with immune checkpoint blockers and radiation treatment, has been shown to improve the overall antitumor activity in mouse studies (119). Additional strategies involve modifying Treg behavior, such as inhibiting STAT3 and using stimulator of interferon response cGAMP interactor agonists aimed at TAMs to stimulate local immune responses and postpone resistance (120,121).
Emerging therapeutic strategies to target Tregs in PCa
The constraints of traditional treatments, coupled with the pivotal function of Tregs in immune regulation, have driven the development of innovative methods focused on directly or indirectly influencing Tregs to enhance anti-tumor immune responses. These strategies can be classified into several main categories, as outlined in Table I.
 |
Table I.
Therapeutic strategies targeting Tregs in PCa.
|
Table I.
Therapeutic strategies targeting Tregs in PCa.
| Strategy category |
Target |
Mechanism of action |
Representative examples/status in PCa |
(Refs.) |
| Monoclonal antibodies |
CCR4 |
Depletes CCR4+ Tregs, reduces tumor infiltration |
Mogamulizumab; preclinical (canine PCa model) & clinical (other cancers) |
(49,126) |
| |
CTLA-4 |
Depletes intratumoral Tregs via ADCC; blocks inhibitory signaling |
Ipilimumab; clinical trial (mCRPC, limited efficacy as mono); fc-enhanced anti-CTLA-4; preclinical (PCa models) |
(12,78,124) |
| |
CD25 (IL-2rα) |
Targets high-affinity IL-2 receptor to deplete/inhibit Tregs |
Basiliximab; preclinical & clinical (limited PCa-specific data; risk of depleting activated Teffs) |
(44,63) |
| |
GARP |
Depletes highly suppressive GARP+ Tregs |
Ds-1055a; preclinical (in vitro/in vivo; GARP+ Tregs identified in PCa patient samples) |
(18) |
| Combination immunotherapy |
PD-1/PD-L1 + Treg-targeting |
Reinvigorates effector T cells while attenuating Treg-mediated suppression |
Anti-PD-1 + anti-CTLA-4; clinical trial (MCRPC); anti-PD-1 + anti-CCR4; preclinical (PCa models). |
(126,131) |
| |
Immune checkpoints + adenosine pathway |
Dual blockade of immunosuppressive pathways |
Anti-PD-1 + A2AR antagonist/CD73 antibody; preclinical (solid tumors) |
(13,118) |
| |
Immunotherapy + radiotherapy/ADT |
Radiotherapy/ADT remodels TME; combined with immunotherapy for synergy |
HIFU + ICIs; ADT + anti-CTLA-4; preclinical & clinical trials (PCa) |
(61,110,138) |
| Novel modalities |
Metabolic pathways (oxphos) |
Inhibits Treg energy metabolism, impairing survival/function |
Oxphos inhibitors (e.g., Gboxin analogs); preclinical (in vitro/in vivo PCa models) |
(152,153) |
| |
Transcription factors |
Modulates Treg stability and function via siRNA |
SiRNA targeting BATF/PRDM1 (nanoparticle-delivered); preclinical (PCa models) |
(58) |
| |
Bispecific antibodies |
Simultaneously depletes Tregs and activates effector cells |
Frp303 (anti-CCR8/4-1bb); preclinical (PCa models) |
(126) |
| |
Cell therapy |
Engineers CAR-T cells resistant to Treg suppression or targeting TME |
TME-iCAR-T; preclinical (solid tumors) |
(157) |
mAbs for Treg depletion and function blockade
Therapies utilizing mAbs targeting Tregs offer a promising method to mitigate immune suppression in PCa (122). As CD4+CD25+FoxP3+ Tregs are found in increased numbers in the lymph nodes and bloodstream of individuals with PCa, and their presence is linked to the advancement of the disease, employing mAbs to eliminate or inhibit the activity of Tregs is a logical approach (46,123).
Focusing on chemokine receptors and immune checkpoints. The mAb mogamulizumab, which targets CCR4, has been shown to reduce Tregs and enhance survival rates in a naturally occurring canine model of PCa, thereby providing a strong preclinical rationale (49). This is supported by evidence that the CCR4-CCL17 pathway is active in attracting Tregs within human PCa tissues (49). By contrast, although anti-CTLA-4 antibodies, such as ipilimumab, have shown promise in pre-clinical PCa models by depleting intratumoral Tregs via ADCC, their clinical efficacy as monotherapy in PCa has been limited, highlighting the need for combination strategies (12,78,124). Similarly, although anti-PD-1/PD-L1 antibodies have had limited success as monotherapies for PCa, they are being actively investigated as combination regimens (125).
Innovative antibody designs
New bispecific antibodies are being engineered to focus more accurately on the TME. For instance, bispecific antibodies that target both 4-1BB and CCR8, such as FRP303, can specifically reduce tumor-infiltrating Tregs while stimulating CD8+ T cells, demonstrating enhanced effects when used alongside PD-1 inhibitors (126). Additionally, antibodies targeting different pathways, such as CD6-CD318, can further boost the effectiveness of cytotoxic lymphocytes present within tumors (127,128).
Radionuclide conjugates for radioimmunotherapy
Antibody-linked radionuclides, such as prostate-specific membrane antigen-targeted 225Ac or 177Lu, have demonstrated significant clinical effectiveness in PCa (129,130). This method utilizes the precision of mAbs to specifically target and administer radiation to cancerous and surrounding immunosuppressive cells.
While CD25 (IL-2Rα) is highly expressed on Tregs, it is also transiently upregulated on activated effector T cells (63). This dual expression poses a significant therapeutic challenge, as strategies aimed at depleting CD25+ cells risk collateral depletion of anti-tumor CD8+ T cells. To mitigate this risk, several innovative approaches are being explored (44,64). First, the use of non-depleting anti-CD25 antibodies that block IL-2 signaling without inducing antibody-dependent cell-mediated cytotoxicity can inhibit Treg function without eliminating them or activated effector T cells (63,64). Second, optimized dosing schedules, such as lower doses or cyclical administration, may allow for preferential or transient Treg modulation while preserving effector T-cell activity (40,44). Third, combining CD25 targeting with agents that selectively boost effector T cells, such as IL-2 superkines engineered to bind the IL-2 receptor complex on effector T cells (IL-2Rβγ) rather than Tregs (IL-2Rαβγ), can shift the immune balance away from suppression (63,64). These strategies represent a shift from indiscriminate depletion to more nuanced modulation of the IL-2 pathway.
The rationale for combination immunotherapy
Due to the complex immunosuppressive environment present in PCa, where Tregs, MDSCs and TAMs collaborate to promote immune evasion, it is crucial to implement strategies that address multiple mechanisms simultaneously (21,61). A significant area of research involves the combination of ICIs and therapies that disrupt additional immunosuppressive pathways (131–134). For example, inhibitors targeting the adenosine signaling pathway, such as those affecting CD39, CD73 or the adenosine A2A receptor, can reduce the suppression of effector T cells caused by adenosine (116,135). When used alongside checkpoint blockers, these inhibitors effectively counteract immune evasion.
Collaboration with regional modalities
Nanotechnology is a cutting-edge delivery method (136). Exosomes sourced from fully developed dendritic cells, infused with the DC1-targeted chemokine XCL1, can successfully attract and stimulate CD8+ T cells while diminishing the levels of Tregs when used alongside chemotherapy-induced immunogenic cell death (137). Techniques for local ablation, such as high-intensity focused ultrasound, can trigger immunogenic cell death, lower the activity of Tregs and MDSCs, and function in conjunction with ICIs (138).
Combining with standard-of-care
According to the above, integrating Treg-targeting approaches with ADT is important. Although ADT effectively slows tumor progression, it simultaneously increases the populations of Tregs and MDSCs, which restricts its effectiveness in immunotherapy. Consequently, the strategic combination of ADT with immunotherapies targeting Tregs is currently a focus of research (23,139). Additionally, addressing prevalent genetic mutations found in tumors, such as those in phosphatase and tensin homolog or tumor protein p53 (TP53), could potentially counteract inherent immunosuppression and improve immune monitoring (140,141).
Charting the future: Overcoming challenges in Treg-targeted therapy
Implementing Treg-targeting approaches in clinical settings encounters multiple obstacles, such as variations in tumors, the emergence of adaptive resistance and potential autoimmune reactions. This section explores the journey towards tailored immunotherapy and the development of advanced techniques to address these issues.
Lessons from clinical failures: The need for patient stratification
Despite a strong preclinical rationale, Treg-targeting monotherapies have shown limited efficacy in unselected PCa patient populations. The failure of ipilimumab (anti-CTLA-4) in phase III trials for metastatic castration-resistant PCa (CRPC) serves as a cautionary example (125). Post-hoc analyses suggested that insufficient intratumoral Treg depletion, compensatory upregulation of other immunosuppressive mechanisms, such as MDSCs and TAMs, and immune-related adverse events contributed to these outcomes (21,78). These failures underscore the critical lessons for future trial design: i) Agent potency and specificity: Depletion of intratumoral Tregs by anti-CTLA-4 may be Fc-dependent, and standard ipilimumab may be inadequate. Agents engineered for enhanced Fc function or those targeting more Treg-restricted markers, such as CCR8, are required. ii) Combination context: The TME of immunosuppressive PCa is shaped by multiple redundant pathways. Treg-directed therapies must be combined with modalities, such as ADT or radiotherapy, to reduce the overall immunosuppressive burden, rather than being used as a monotherapy. iii) Patient selection: The benefit of Treg depletion may be confined to patients with a TME dominated by Treg-mediated suppression. Biomarkers, such as the TIL TregSig or spatial Treg/M2 macrophage indices, are needed to prospectively identify these patients.
Towards personalized immunotherapy: Decoding Treg heterogeneity and patient stratification
An essential avenue for future research is the development of targeted immunotherapy methods based on the molecular profiling of Tregs and the immune microenvironment associated with PCa (142,143). The significant variability in PCa, which is evident in the different immune cell types and genetic profiles of tumors, requires a tailored strategy (144).
The use of multi-omics approaches is essential for this purpose. By combining genomic, transcriptomic and epigenomic information, it is possible to identify immune subtypes unique to each patient that are associated with varying clinical outcomes and treatment sensitivities (145). For example, the transmembrane protease serine 2-ETS-related gene fusion, frequently observed in PCa, has been linked to the recruitment of Tregs, indicating that this genetic change may guide the choice of immunotherapy (146). Beyond genetic fusions, recent research has explored copper-dependent cell death (cuproptosis) as a mechanism to influence the PCa immune microenvironment, and cuproptosis-related gene signatures have been used to stratify patients for prognosis and potential immunotherapy response (144). Additionally, scoring frameworks that focus on particular biological mechanisms, such as patterns of RNA N6-methyladenosine modifications, have also been effective in categorizing patients according to their immune cell density, prognosis and anticipated responses to immunotherapy (147).
The genetic makeup of tumors significantly influences the immune environment. Changes, such as the amplification of myelocytomatosis viral oncogene homolog and the inactivation of TP53, not only enhance the tumor's aggressiveness but also create a microenvironment that suppresses the immune response by promoting vascular endothelial growth factor (VEGF) production, which hampers the activity of CD8+ T cells (148,149). Recognizing these genetic variations enables the strategic pairing of targeted therapies, such as VEGF inhibitors, with immunotherapies to counteract immune suppression (150).
Future studies should utilize cutting-edge technologies, such as single-cell sequencing and spatial transcriptomics, to advance past traditional bulk tissue analysis. These methodologies enable detailed mapping of the spatial arrangement, functional characteristics and clonality of Tregs and various immune cells within the TME. Gaining a high-resolution understanding is essential for crafting targeted interventions that focus on immunosuppressive cells without compromising overall immune function, thereby facilitating the creation of genuinely personalized treatment strategies (141).
Unresolved questions: Tregs in CRPC and metabolic vulnerabilities
A critical gap lies in the current understanding of the functional evolution of Tregs during disease progression. The role and phenotype of Tregs in CRPC may differ significantly from those in hormone-sensitive prostate cancer (HSPC) (10). In the untreated HSPC setting, Treg infiltration, while present, is often lower and their suppressive function may be more dependent on the initial recruitment cues from the primary tumor. By contrast, emerging evidence suggests that in CRPC, particularly following therapies such as enzalutamide treatment, Tregs become more abundant and exhibit an enhanced immunosuppressive capacity, paradoxically driven by treatment itself. For instance, enzalutamide has been shown to enhance Treg infiltration and activity through mechanisms such as the FLII/YBX1/PD-L1 axis, contributing to acquired resistance (10,103). This suggests a phenotypic and functional shift of Tregs under therapeutic pressure. Understanding whether distinct Treg subsets (e.g., the highly suppressive eTregs described in the above chapter) dominate in CRPC and how they co-opt metabolic pathways (e.g., enhanced fatty acid oxidation vs. glycolysis) to survive in the therapy-remodeled TME is a crucial area for future investigations.
Exploiting Treg metabolic dependencies
A promising approach to overcome Treg-mediated resistance is to exploit the unique metabolic vulnerabilities of Tregs. While effector T-cells rely heavily on glycolysis, intratumoral Tregs are highly dependent on OXPHOS and fatty acid oxidation for their survival and suppressive functions (151,152). This metabolic dependence presents a potential therapeutic window. Combining ICIs with OXPHOS inhibitors is a strategy currently under pre-clinical investigation with the aim of selectively depriving Tregs of energy while preserving or even enhancing the glycolytic capacity of effector T cells (53,153). Further research on the metabolic interplay between Tregs and other cells in the TME is essential for the development of targeted metabolic interventions.
Developing next-generation therapeutic modalities
To address the resistance posed by Tregs, it is essential to develop innovative treatments that focus on the core biology of these cells, especially their exceptional ability to adapt metabolically and their survival strategies in the TME.
Exploiting metabolic vulnerabilities
A potential strategy involves leveraging the metabolic pathways of Tregs. PCa cells, along with immunosuppressive cells, such as Tregs, frequently rely on mitochondrial OXPHOS for their energy needs (151,152). By using targeted inhibitors of OXPHOS, impairing energy resources essential for Treg activity is applicable, which can diminish their ability to suppress the immune response and enhance the effectiveness of ICIs (53,153).
Sophisticated combination approaches
Given the intricate nature of the TME, it is improbable that therapies targeting a single agent will be effective. Future treatment protocols should incorporate strategically designed multi-target combinations. This may involve the use of ICIs alongside i) metabolic modulators, such as OXPHOS inhibitors (154) and ii) nanotechnology solutions aimed at altering the TME (155). For instance, polymeric lipid manganese dioxide nanoparticles can help mitigate tumor hypoxia, decrease the recruitment of Tregs and myeloid-derived suppressor cells and improve the effectiveness of radiotherapy (156).
Advanced cell therapies
The latest advancements in cell therapy are aimed at improving safety and target accuracy. Inducible chimeric antigen receptor T-cell (CAR-T) systems, such as TME-iCAR-T, are designed to be activated exclusively within the TME, allowing for the precise destruction of cancer cells and potentially harmful stromal components, while reducing off-target effects. This represents a major advancement in cellular immunotherapy (157).
Conclusion
A growing body of research has identified Tregs as key controllers of the immunosuppressive environment found in PCa. Through the direct inhibition of effector T-cell activity and intricate interactions with various immune cells, Tregs create an immune tolerance that promotes tumor growth and helps the cancer cells avoid detection by the host's immune system. Understanding these processes has deepened our insight into the immunobiology of PCa and laid a strong foundation for the development of innovative immunotherapeutic approaches.
To progress in this field, it is essential to reconcile the contradictory findings. While numerous studies have linked a high density of Tregs to unfavorable outcomes, new evidence indicates that the functional characteristics and diversity of Treg subsets could play a more crucial role in immune suppression than their shear numbers. These perspectives are not opposing; rather, they underscore the intricate nature of Treg biology. Therefore, future research should extend beyond mere counting to thoroughly analyze Treg subsets and evaluate their functional roles in the context of individual tumors. Additionally, the balance between Tregs and other immune elements is vital for determining the success of treatment. The primary challenge is to achieve accurate immunomodulation: Effectively reducing Treg-induced suppression to enhance anti-tumor immunity while steering clear of excessive immune responses and autoimmunity.
To address these issues, future studies should focus on clarifying the fundamental molecular networks that regulate Treg activity, particularly in relation to signaling pathways, epigenetic modifications and metabolic changes. Employing advanced technologies such as single-cell multi-omics and spatial profiling will be crucial for unraveling the complex spatiotemporal variations within the immune environment of PCa at an unmatched level of detail. Simultaneously, there is a need to expedite clinical applications by focusing on the strategic development of combination trials that merge Treg-targeting treatments, such as depleting antibodies and metabolic inhibitors with ICIs, standard therapies and other immunomodulatory agents.
In conclusion, Tregs play a crucial and actionable role within the immunosuppressive mechanism of PCa. Achieving breakthroughs against Treg-driven resistance requires a comprehensive approach that integrates thorough mechanistic insights into cutting-edge clinical trial methodologies. This research suggests a move towards tailored combination treatments that effectively counteract Treg suppression, ultimately enhancing long-lasting anti-tumor responses and benefiting patient results.
Acknowledgements
Not applicable.
Funding
This research was funded by the Medical Research Project of Sichuan Medical Association (grant no. S2024047).
Availability of data and materials
Not applicable.
Authors' contributions
HL was responsible for the study conception and design, literature search and selection, figure generation, and manuscript drafting and editing. Data authentication is not applicable. The author has read and approved the final manuscript.
Ethics approval and consent to participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The author declares to have no competing interests.
References
|
1
|
Xu MY, Zeng N, Ma S, Hua ZJ, Zhang SH, Xiang JC, Xiong YF, Xia ZY, Sun JX, Liu CQ, et al: A clinical evaluation of robotic-assisted radical prostatectomy (RARP) in located prostate cancer: A systematic review and network meta-analysis. Crit Rev Oncol Hematol. 204:1045142024. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Genitourinary Oncology Committee of Chinese Anti-Cancer Association, . Expert consensus on whole-course management of prostate cancer (2025 edition). Zhonghua Zhong Liu Za Zhi. 47:617–634. 2025.(In Chinese). PubMed/NCBI
|
|
3
|
Hussain Y, Mirzaei S, Ashrafizadeh M, Zarrabi A, Hushmandi K, Khan H and Daglia M: Quercetin and its Nano-scale delivery systems in prostate cancer therapy: Paving the way for cancer elimination and reversing chemoresistance. Cancers (Basel). 13:16022021. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Manfredi C, Ditonno F, Franco A, Bologna E, Licari LC, Arcaniolo D, Tubaro A, De Nunzio C, Antonelli A, De Sio M, et al: Prostate cancer in transgender women: Epidemiology, clinical characteristics, and management challenges. Curr Oncol Rep. 25:1431–1443. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ciccarese C, Nobili E, Grilli D, Casolari L, Rihawi K, Gelsomino F, Tortora G and Massari F: The safety and efficacy of enzalutamide in the treatment of advanced prostate cancer. Expert Rev Anticancer Ther. 16:681–696. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wei J, Li D, Long H and Han M: Immune microenvironment of tumor-draining lymph nodes: Insights for immunotherapy. Front Immunol. 16:15627972025. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Sugiyama D, Hinohara K and Nishikawa H: Significance of regulatory T cells in cancer immunology and immunotherapy. Exp Dermatol. 32:256–263. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bergerhoff K and Pedersen M: Isolation and analysis of Tumor-infiltrating treg. Methods Mol Biol. 2559:51–63. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chen BJ, Zhao JW, Zhang DH, Zheng AH and Wu GQ: Immunotherapy of cancer by targeting regulatory T cells. Int Immunopharmacol. 104:1084692021. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ruan H, Bao L, Tao Z and Chen K: Flightless I homolog reverses enzalutamide resistance through PD-L1-mediated immune evasion in prostate cancer. Cancer Immunol Res. 9:838–852. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kania E, Janica M, Nesterowicz M, Modzelewski W, Cybulski M and Janica J: Advances and challenges in prostate cancer diagnosis: A comprehensive review. Cancers (Basel). 17:21372025. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Fu J, Mao L, Jiao Y, Mei D and Chen Y: Elucidating CTLA-4′s role in tumor immunity: A comprehensive overview of targeted antibody therapies and clinical developments. Mol Divers. 29:5075–5084. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Xing J, Zhang J and Wang J: The immune regulatory role of adenosine in the tumor microenvironment. Int J Mol Sci. 24:149282023. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhang L, Kuca K, You L, Zhao Y, Musilek K, Nepovimova E, Wu Q, Wu W and Adam V: Signal transducer and activator of transcription 3 signaling in tumor immune evasion. Pharmacol Ther. 230:1079692021. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lu J, Liang T, Li P and Yin Q: Regulatory effects of IRF4 on immune cells in the tumor microenvironment. Front Immunol. 14:10868032023. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhan DT and Xian HC: Exploring the regulatory role of lncRNA in cancer immunity. Front Oncol. 13:11919132023. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Liu YN, Zhang H, Zhang L, Cai TT, Huang DJ, He J, Ni HH, Zhou FJ, Zhang XS and Li J: Sphingosine 1 phosphate receptor-1 (S1P1) promotes tumor-associated regulatory T cell expansion: Leading to poor survival in bladder cancer. Cell Death Dis. 10:502019. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Satoh K, Kobayashi Y, Fujimaki K, Hayashi S, Ishida S, Sugiyama D, Sato T, Lim K, Miyamoto M, Kozuma S, et al: Novel anti-GARP antibody DS-1055a augments anti-tumor immunity by depleting highly suppressive GARP+ regulatory T cells. Int Immunol. 33:435–446. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Liu Y, Zhao L, Liu J and Wang L: Artificial intelligence-based personalized clinical decision-making for patients with localized prostate cancer: Surgery versus radiotherapy. Oncologist. 29:e1692–e1700. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Felici A, Peduzzi G, Pellungrini R and Campa D: Artificial intelligence to predict cancer risk, are we there yet? A comprehensive review across cancer types. Eur J Cancer. 222:1154402025. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Stultz J and Fong L: How to turn up the heat on the cold immune microenvironment of metastatic prostate cancer. Prostate Cancer Prostatic Dis. 24:697–717. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Movassaghi M, Chung R, Anderson CB, Stein M, Saenger Y and Faiena I: Overcoming immune resistance in prostate cancer: Challenges and advances. Cancers (Basel). 13:47572021. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Qin C, Wang J, Du Y and Xu T: Immunosuppressive environment in response to androgen deprivation treatment in prostate cancer. Front Endocrinol (Lausanne). 13:10558262022. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ching MM, Reader J and Fulton AM: Eicosanoids in Cancer: Prostaglandin E2 receptor 4 in cancer therapeutics and immunotherapy. Front Pharmacol. 11:8192020. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kawano Y: The role of regulatory T cells in multiple myeloma progression. Rinsho Ketsueki. 62:299–304. 2021.(In Japanese). PubMed/NCBI
|
|
26
|
Ge J, Yin X and Chen L: Regulatory T cells: Masterminds of immune equilibrium and future therapeutic innovations. Front Immunol. 15:14571892024. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Cheng J, Qian W, Chen F, Liu X, Fu M, Cao W and Zhou Y: Function of epigenetic modifications in wound healing and potential therapies (Review). Int J Mol Med. 56:1902025. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yadav M, Stephan S and Bluestone JA: Peripherally induced tregs-role in immune homeostasis and autoimmunity. Front Immunol. 4:2322013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ohkura N and Sakaguchi S: Transcriptional and epigenetic basis of Treg cell development and function: Its genetic anomalies or variations in autoimmune diseases. Cell Res. 30:465–474. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Xiang Y, Wang J, Li JP, Guo W, Huang F, Zhang HM, Li HH, Dai ZT, Zhang ZJ, Li H, et al: MKL-1 is a coactivator for STAT5b, the regulator of Treg cell development and function. Cell Commun Signal. 18:1072020. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Yang F, Yanes A, Li M, Heizer P, Linatoc I, Stephens ME, Song Y, Ort T, Bednar KJ, Ikeda Y, et al: Differential regulation of Treg stability in human naïve and effector Treg subsets by TGFβ-signaling via ARKADIA-SKI axis. Front Immunol. 16:16364342025. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Bagheri Y, Babaha F, Falak R, Yazdani R, Azizi G, Sadri M, Abolhassani H, Shekarabi M and Aghamohammadi A: IL-10 induces TGF-β secretion, TGF-β receptor II upregulation, and IgA secretion in B cells. Eur Cytokine Netw. 30:107–113. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kessel A, Haj T, Peri R, Snir A, Melamed D, Sabo E and Toubi E: Human CD19(+) CD25(high) bregulatory cells suppress proliferation of CD4(+) T cells and enhance Foxp3 and CTLA-4 expression in T-regulatory cells. Autoimmun Rev. 11:670–677. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Jin H, Zhong X, Zhang C, Wu Y, Sun J, Wang X, Wang Z, Zhu J, Jiang Y, Du X, et al: CD73 promotes the immunoregulatory functions of hepatic Tregs through enzymatic and nonenzymatic pathways in MASLD development. Mol Metab. 96:1021312025. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Jiang Z, Zhu H, Wang P, Que W, Zhong L, Li XK and Du F: Different subpopulations of regulatory T cells in human autoimmune disease, transplantation, and tumor immunity. MedComm (2020). 3:e1372022. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Ma D, Alizadeh H, Comerford SA, Gething MJ, Sambrook JF, Anand R and Niederkorn JY: Rejection of intraocular tumors from transgenic mice by tumor-infiltrating lymphocytes. Curr Eye Res. 13:361–369. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Lu J, Liang Y, Meng H, Zhang A, Zhao J and Zhang C: Metabolic controls on epigenetic reprogramming in regulatory T cells. Front Immunol. 12:7287832021. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Singh AK, Al Qureshah F, Drow T, Hou B and Rawlings DJ: Activated PI3Kδ specifically perturbs mouse regulatory T cell homeostasis and function leading to immune dysregulation. J Immunol. 213:135–147. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Singh AK, Qureshah FA, Drow T, Hou B and Rawlings DJ: Activated PI3Kδ specifically perturbs mouse Treg homeostasis and function leading to immune dysregulation. bioRxiv. 23:5696652023.
|
|
40
|
Li J, Zhang L, Liu R, Xu C, Tang H, Zou Y, Cao Q and Huang W: CXCL12/CXCR4 axis governs Treg spatial dominance over CD8+ T cells via IL-2 sequestration: A dual therapeutic target in prostate cancer. Front Immunol. 16:16267082025. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Jovanovic I, Zivkovic M, Jesic S and Stankovic A: Non-coding RNA and cholesteatoma. Laryngoscope Investig Otolaryngol. 7:60–66. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Luo Y and Wang H: Effects of Non-coding RNA on regulatory T cells and implications for treatment of immunological diseases. Front Immunol. 11:6120602020. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Qiu R, Zhou L, Ma Y, Zhou L, Liang T, Shi L, Long J and Yuan D: Regulatory T cell plasticity and stability and autoimmune diseases. Clin Rev Allergy Immunol. 58:52–70. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Dees S, Ganesan R, Singh S and Grewal IS: Regulatory T cell targeting in cancer: Emerging strategies in immunotherapy. Eur J Immunol. 51:280–291. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Bian X, Wang W, Abudurexiti M, Zhang X, Ma W, Shi G, Du L, Xu M, Wang X, Tan C, et al: Integration analysis of Single-cell Multi-Omics reveals prostate cancer heterogeneity. Adv Sci (Weinh). 11:e23057242024. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Karpisheh V, Mousavi SM, Naghavi Sheykholeslami P, Fathi M, Mohammadpour Saray M, Aghebati-Maleki L, Jafari R, Majidi Zolbanin N and Jadidi-Niaragh F: The role of regulatory T cells in the pathogenesis and treatment of prostate cancer. Life Sci. 284:1191322021. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Feriz AM, Khosrojerdi A, Lotfollahi M, Shamsaki N, GhasemiGol M, HosseiniGol E, Fereidouni M, Rohban MH, Sebzari AR, Saghafi S, et al: Single-cell RNA sequencing uncovers heterogeneous transcriptional signatures in tumor-infiltrated dendritic cells in prostate cancer. Heliyon. 9:e156942023. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Wang H, Fang D, Zhu J, Liu L, Xue L, Wang L, Karzai F, Antonarakis ES, Urabe F, Ma W and Wei W: Ferroptosis-related gene signature predicts prognosis and immune microenvironment in prostate cancer. Transl Androl Urol. 13:2092–2109. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Maeda S, Motegi T, Iio A, Kaji K, Goto-Koshino Y, Eto S, Ikeda N, Nakagawa T, Nishimura R, Yonezawa T and Momoi Y: Anti-CCR4 treatment depletes regulatory T cells and leads to clinical activity in a canine model of advanced prostate cancer. J Immunother Cancer. 10:e0037312022. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Huen NY, Pang AL, Tucker JA, Lee TL, Vergati M, Jochems C, Intrivici C, Cereda V, Chan WY, Rennert OM, et al: Up-regulation of proliferative and migratory genes in regulatory T cells from patients with metastatic castration-resistant prostate cancer. Int J Cancer. 133:373–382. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Adorno Febles VR, Hao Y, Ahsan A, Wu J, Qian Y, Zhong H, Loeb S, Makarov DV, Lepor H, Wysock J, et al: Single-cell analysis of localized prostate cancer patients links high Gleason score with an immunosuppressive profile. Prostate. 83:840–849. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Andersen LB, Nørgaard M, Rasmussen M, Fredsøe J, Borre M, Ulhøi BP and Sørensen KD: Immune cell analyses of the tumor microenvironment in prostate cancer highlight infiltrating regulatory T cells and macrophages as adverse prognostic factors. J Pathol. 255:155–165. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Akalin I, Erol B, Aslan E, Ozkanli SS, Efiloglu O, Yildirim S, Caskurlu T, Yildirim A and Karaman MI: A New promising pathway in aggressive prostate cancer: Treg/mir-let8c/lin28b. Arch Esp Urol. 75:459–466. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Wong RL and Yu EY: Refining Immuno-oncology approaches in metastatic prostate cancer: Transcending current limitations. Curr Treat Options Oncol. 22:132021. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Meng F, Han X, Min Z, He X and Zhu S: Prognostic signatures associated with high infiltration of Tregs in bone metastatic prostate cancer. Aging (Albany NY). 13:17442–17461. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Davidsson S, Carlsson J, Greenberg L, Wijkander J, Söderquist B and Erlandsson A: Cutibacterium acnes induces the expression of immunosuppressive genes in macrophages and is associated with an increase of regulatory T-Cells in prostate cancer. Microbiol Spectr. 9:e01497212021. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Li S, Liu R, Hao X and Liu X: The role of gut microbiota in prostate cancer progression: A Mendelian randomization study of immune mediation. Medicine (Baltimore). 103:e388252024. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Zhao Z, An R, Tang W, Chen J, Xu R and Kan L: Modulating Treg cell activity in prostate cancer via chitosan nanoparticles loaded with si-BATF/PRDM1. Int Immunopharmacol. 144:1134452024. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Witt K, Evans-Axelsson S, Lundqvist A, Johansson M, Bjartell A and Hellsten R: Inhibition of STAT3 augments antitumor efficacy of anti-CTLA-4 treatment against prostate cancer. Cancer Immunol Immunother. 70:3155–3166. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Wang Z, Wang Y, Peng M and Yi L: UBASH3B is a novel prognostic biomarker and correlated with immune infiltrates in prostate cancer. Front Oncol. 9:15172019. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Kajikawa H, Hirata M, Haruna M, Ueyama A, Hirose K, Kawashima A, Iwahori K, Matsunaga K, Toyosawa S, Uzawa N and Wada H: Tumor-infiltrating ICOS+ effector regulatory T-Cells in oral squamous cell carcinoma as a promising biomarker for prognosis and ‘Hot’ tumor. Anticancer Res. 42:2383–2393. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Ju M, Fan J, Zou Y, Yu M, Jiang L, Wei Q, Bi J, Hu B, Guan Q, Song X, et al: Computational recognition of a regulatory T-cell-specific signature with potential implications in prognosis, immunotherapy, and therapeutic resistance of prostate cancer. Front Immunol. 13:8078402022. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
de la Rosa M, Rutz S, Dorninger H and Scheffold A: Interleukin-2 is essential for CD4+CD25+ regulatory T cell function. Eur J Immunol. 34:2480–2488. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Lahusen A, Minhöfer N, Lohse KA, Blechner C, Lindenmayer J, Eiseler T, Wellstein A, Kleger A, Seufferlein T, Windhorst S and Lin YN: Pancreatic cancer cell-intrinsic transglutaminase-2 promotes T cell suppression through microtubule-dependent secretion of immunosuppressive cytokines. J Immunother Cancer. 13:e0105792025. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Chatterjee S, Chatterjee A, Jana S, Dey S, Roy H, Das MK, Alam J, Adhikary A, Chowdhury A, Biswas A, et al: Transforming growth factor beta orchestrates PD-L1 enrichment in tumor-derived exosomes and mediates CD8 T-cell dysfunction regulating early phosphorylation of TCR signalome in breast cancer. Carcinogenesis. 42:38–47. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Araujo Furlan CL, Boccardo S, Rodriguez C, Mary VS, Gimenez CMS, Robson SC, Gruppi A, Montes CL and Acosta Rodríguez EV: CD39 expression by regulatory T cells participates in CD8+ T cell suppression during experimental Trypanosoma cruzi infection. PLoS Pathog. 20:e10121912024. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Zagorulya M, Yim L, Morgan DM, Edwards A, Torres-Mejia E, Momin N, McCreery CV, Zamora IL, Horton BL, Fox JG, et al: Tissue-specific abundance of interferon-gamma drives regulatory T cells to restrain DC1-mediated priming of cytotoxic T cells against lung cancer. Immunity. 56:386–405.e10. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Cederbom L, Hall H and Ivars F: CD4+CD25+ regulatory T cells down-regulate co-stimulatory molecules on antigen-presenting cells. Eur J Immunol. 30:1538–1543. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Lv Y, Tian W, Teng Y, Wang P, Zhao Y, Li Z, Tang S, Chen W, Xie R, Lü M and Zhuang Y: Tumor-infiltrating mast cells stimulate ICOS+ regulatory T cells through an IL-33 and IL-2 axis to promote gastric cancer progression. J Adv Res. 57:149–162. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Salminen A: The role of the immunosuppressive PD-1/PD-L1 checkpoint pathway in the aging process and age-related diseases. J Mol Med (Berl). 102:733–750. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Faria AM and Weiner HL: Oral tolerance and TGF-beta-producing cells. Inflamm Allergy Drug Targets. 5:179–190. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Kos K, Salvagno C, Wellenstein MD, Aslam MA, Meijer DA, Hau CS, Vrijland K, Kaldenbach D, Raeven EAM, Schmittnaegel M, et al: Tumor-associated macrophages promote intratumoral conversion of conventional CD4+ T cells into regulatory T cells via PD-1 signalling. Oncoimmunology. 11:20632252022. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Chen J, Feng W, Sun M, Huang W, Wang G, Chen X, Yin Y, Chen X, Zhang B, Nie Y, et al: TGF-β1-Induced SOX18 elevation promotes hepatocellular carcinoma progression and metastasis through transcriptionally upregulating PD-L1 and CXCL12. Gastroenterology. 167:264–280. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Audun Klingen T, Chen Y, Aas H and Akslen LA: DDR2 expression in breast cancer is associated with blood vessel invasion, basal-like tumors, tumor associated macrophages, regulatory T cells, detection mode and prognosis. Hum Pathol. 150:29–35. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Xing Y, Ruan G, Ni H, Qin H, Chen S, Gu X, Shang J, Zhou Y, Tao X and Zheng L: Tumor immune microenvironment and its related miRNAs in tumor progression. Front Immunol. 12:6247252021. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Jayaraman Rukmini S, Bi H, Sen P, Everhart B, Jin S and Ye K: Inducing tumor suppressive microenvironments through genome Edited CD47-/-Syngeneic cell vaccination. Sci Rep. 9:200572019. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Zhou K, Zhong Q, Wang YC, Xiong XY, Meng ZY, Zhao T, Zhu WY, Liao MF, Wu LR, Yang YR, et al: Regulatory T cells ameliorate intracerebral hemorrhage-induced inflammatory injury by modulating microglia/macrophage polarization through the IL-10/GSK3β/PTEN axis. J Cereb Blood Flow Metab. 37:967–979. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Ager CR, Obradovic A, McCann P, Chaimowitz M, Wang ALE, Shaikh N, Shah P, Pan SS, Laplaca CJ, Virk RK, et al: Fc-enhanced anti-CTLA-4 depletes tumor-infiltrating regulatory T cells to augment immune effects of androgen ablation in high-risk prostate cancer. medRxiv. 31:243133082025.
|
|
79
|
Chiang Y, Lu LF, Tsai CL, Tsai YC, Wang CC, Hsueh FJ, Huang CY, Chen CH, Pu YS and Cheng JC: C-C chemokine receptor 4 (CCR4)-positive regulatory T cells interact with tumor-associated macrophages to facilitate metastatic potential after radiation. Eur J Cancer. 198:1135212023. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Zhuo C, Xu Y, Ying M, Li Q, Huang L, Li D, Cai S and Li B: FOXP3+ Tregs: Heterogeneous phenotypes and conflicting impacts on survival outcomes in patients with colorectal cancer. Immunol Res. 61:338–347. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Lv D, Wu X, Chen X, Yang S, Chen W, Wang M, Liu Y, Gu D and Zeng G: A novel immune-related gene-based prognostic signature to predict biochemical recurrence in patients with prostate cancer after radical prostatectomy. Cancer Immunol Immunother. 70:3587–3602. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Su TH and Shin EC: Peripheral blood Foxp3-high Tregs: A novel prognostic biomarker in hepatocellular carcinoma. Hepatology. Jul 7–2025.(Epub ahead of print). doi: 10.1097/HEP.0000000000001464.
|
|
83
|
Huang CH, Ku WT, Teng W, Jeng WJ and Lin CY: Letter to the editor: Peripheral Foxp3-high Tregs as a dual biomarker for HCC prognosis and immunotherapy response. Hepatology. 83:E13–E14. 2026. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Wang Y, Qin Y, Wu C, Chen J, Zhang Y, Chen Y, Xie X, Gao X, Sun C and Liu S: OSU-T315 overcomes immunosuppression in triple-negative breast cancer by targeting the ILK/NF-κB signaling pathway to enhance immunotherapeutic efficacy. Int Immunopharmacol. 143:1135302024. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Oshi M, Asaoka M, Tokumaru Y, Angarita FA, Yan L, Matsuyama R, Zsiros E, Ishikawa T, Endo I and Takabe K: Abundance of regulatory T Cell (Treg) as a predictive biomarker for neoadjuvant chemotherapy in Triple-negative breast cancer. Cancers (Basel). 12:30382020. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Lin Y, Zhang Y, Tuo Z, Gao L, Ding D, Bi L, Yu D, Lv Z, Wang J and Chen X: ORC6, a novel prognostic biomarker, correlates with T regulatory cell infiltration in prostate adenocarcinoma: A pan-cancer analysis. BMC Cancer. 23:2852023. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Kampan NC, Kartikasari AER, Deceneux C, Madondo MT, McNally OM, Flanagan KL, Aziz NA, Stephens AN, Reynolds J, Quinn MA and Plebanski M: Combining TNFR2-Expressing Tregs and IL-6 as superior diagnostic biomarkers for high-grade serous ovarian cancer masses. Cancers (Basel). 15:6672023. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Cheng Y, Li L, Wei X, Xu F, Huang X, Qi F, Zhang Y and Li X: HNRNPC suppresses tumor immune microenvironment by activating Treg cells promoting the progression of prostate cancer. Cancer Sci. 114:1830–1845. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Zhao L and Cao Y: PD-L1 expression level displays a positive correlation with immune response in pancreatic cancer. Dis Markers. 2020:88431462020. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Huang CH, Ku WT, Mahalingam J, Wu CH, Wu TH, Fan JH, Su CW, Lin PT, Peng CW, Yang CK, et al: Tumor-migrating peripheral Foxp3-high regulatory T cells drive poor prognosis in hepatocellular carcinoma. Hepatology. Jul 1–2025.doi: 10.1097/HEP.0000000000001428 (Epub ahead of print).
|
|
91
|
Tian Y, Yu Q, Qiao J, Tao Y, Li Y and Li T: Landscape analysis of matrix metalloproteinases reveals key prognostic markers for prostate cancer. Front Immunol. 16:15829922025. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Shao N, Tang H, Mi Y, Zhu Y, Wan F and Ye D: A novel gene signature to predict immune infiltration and outcome in patients with prostate cancer. Oncoimmunology. 9:17624732020. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Okamoto T, Mizuta R, Demachi-Okamura A, Muraoka D, Sasaki E, Masago K, Yamaguchi R, Teramukai S, Otani Y, Date I, et al: Immune prognostic model for glioblastoma based on the ssGSEA enrichment score. Cancer Genet. 294-295:32–41. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Zhang G, Luo Y, Dong W and Zhong W: Characterization of a Pyroptosis-related signature for prognosis prediction and immune microenvironment infiltration in prostate cancer. Comput Math Methods Med. 2022:82338402022.PubMed/NCBI
|
|
95
|
Wang PC, Hu ZQ, Zhou SL, Yu SY, Mao L, Su S, Li J, Ren N and Huang XW: The spatial distribution of immune cell subpopulations in hepatocellular carcinoma. Cancer Sci. 113:423–431. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Liu Z, Zhong J, Cai C, Lu J, Wu W and Zeng G: Immune-related biomarker risk score predicts prognosis in prostate cancer. Aging (Albany NY). 12:22776–22793. 2020.PubMed/NCBI
|
|
97
|
Arai M, Watanabe K, Takeda T, Matsumoto K, Yamashita M, Kitano S and Oya M: Dynamics in the prostate immune microenvironment induced by androgen deprivation therapy. Prostate. 85:308–314. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Anwaier A, Zhu SX, Tian X, Xu WH, Wang Y, Palihati M, Wang WY, Shi GH, Qu YY, Zhang HL and Ye DW: Large-scale proteomics data reveal integrated Prognosis-related protein signatures and role of SMAD4 and RAD50 in prognosis and immune infiltrations of prostate cancer microenvironment. Phenomics. 2:404–418. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Pan Y, Zhou H, Sun Z, Zhu Y, Zhang Z, Han J, Liu Y and Wang Q: Regulatory T cells in solid tumor immunotherapy: Effect, mechanism and clinical application. Cell Death Dis. 16:2772025. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Song P, Song F, Shao T, Wang P, Li R, Chen ZS, Zhang Z and Xue G: Natural products: Promising therapeutics for targeting regulatory immune cells in the tumor microenvironment. Front Pharmacol. 15:14818502024. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Alqathama A: Natural products as promising modulators of breast cancer immunotherapy. Front Immunol. 15:14103002024. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Hibino S, Chikuma S, Kondo T, Ito M, Nakatsukasa H, Omata-Mise S and Yoshimura A: Inhibition of Nr4a receptors enhances antitumor immunity by breaking Treg-mediated immune tolerance. Cancer Res. 78:3027–3040. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Zhong S, Peng S, Chen Z, Chen Z and Luo JL: Choosing kinase inhibitors for androgen deprivation Therapy-resistant prostate cancer. Pharmaceutics. 14:4982022. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Brennan L, Brouwer-Visser J, Nüesch E, Karpova M, Heller A, Gaire F, Schneider M, Gomes B and Korski K: T-Cell heterogeneity in baseline tumor samples: Implications for early clinical trial design and analysis. Front Immunol. 13:7607632022. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Zheng X, Wang J, OuYang Y, Yao K, Zheng J, Zeng L, Wang J, Chen H, Du H, Fu D, et al: Breaking immune evasion in breast cancer by targeting COX-2/PGE2 pathway. Mol Cell Endocrinol. 608:1126172025. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Osborne CK: Aromatase inhibitors in relation to other forms of endocrine therapy for breast cancer. Endocr Relat Cancer. 6:271–276. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Tong D: Selective estrogen receptor modulators contribute to prostate cancer treatment by regulating the tumor immune microenvironment. J Immunother Cancer. 10:e0029442022. View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Ollivier L, Labbé M, Fradin D, Potiron V and Supiot S: Interaction between modern radiotherapy and immunotherapy for metastatic prostate cancer. Front Oncol. 11:7446792021. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Muroyama Y, Nirschl TR, Kochel CM, Lopez-Bujanda Z, Theodros D, Mao W, Carrera-Haro MA, Ghasemzadeh A, Marciscano AE, Velarde E, et al: Stereotactic radiotherapy increases functionally suppressive regulatory T cells in the tumor microenvironment. Cancer Immunol Res. 5:992–1004. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Lin L, Kane N, Kobayashi N, Kono EA, Yamashiro JM, Nickols NG and Reiter RE: High-dose per fraction radiotherapy induces both antitumor immunity and immunosuppressive responses in prostate tumors. Clin Cancer Res. 27:1505–1515. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Hoffmann E, Paulsen F, Schaedle P, Zips D, Gani C, Rammensee HG, Gouttefangeas C and Eckert F: Radiotherapy planning parameters correlate with changes in the peripheral immune status of patients undergoing curative radiotherapy for localized prostate cancer. Cancer Immunol Immunother. 71:541–552. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Wang C, Yuan M, Gao Y, Hou R, Song D and Feng Y: Changes in tumor immune microenvironment after radiotherapy resistance in colorectal cancer: A narrative review. Oncol Res Treat. 46:177–191. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
113
|
Hu W, Pei Y, Ning R, Li P, Zhang Z, Hong Z, Bao C, Guo X, Sun Y and Zhang Q: Immunomodulatory effects of carbon ion radiotherapy in patients with localized prostate cancer. J Cancer Res Clin Oncol. 149:4533–4545. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
114
|
Zhang F, Zheng Z, Barman AK, Wang Z, Wang L, Zeng W, Wang L, Qin Y, Pandey A, Zhang C and Liang W: Optimal combination treatment regimens of vaccine and radiotherapy augment tumor-bearing host immunity. Commun Biol. 4:782021. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Erlandsson A, Lundholm M, Watz J, Bergh A, Petrova E, Alamdari F, Helleday T, Davidsson S, Andren O and Tarish F: Infiltrating immune cells in prostate cancer tissue after androgen deprivation and radiotherapy. Int J Immunopathol Pharmacol. 37:39463202311580252023. View Article : Google Scholar : PubMed/NCBI
|
|
116
|
Zhang C, Wang K and Wang H: Adenosine in cancer immunotherapy: Taking off on a new plane. Biochim Biophys Acta Rev Cancer. 1878:1890052023. View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Gadwa J, Bickett TE, Darragh LB, Knitz MW, Bhatia S, Piper M, Van Court B, Bhuvane S, Nguyen D, Nangia V, et al: Complement C3a and C5a receptor blockade modulates regulatory T cell conversion in head and neck cancer. J Immunother Cancer. 9:e0025852021. View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Ji D, Song C, Li Y, Xia J, Wu Y, Jia J, Cui X, Yu S and Gu J: Combination of radiotherapy and suppression of Tregs enhances abscopal antitumor effect and inhibits metastasis in rectal cancer. J Immunother Cancer. 8:e0008262020. View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Luo X and Zeng M: Combination low-dose cyclophosphamide with check-point blockade and ionizing radiation promote an abscopal effect in mouse models of melanoma. J Cancer Res Ther. 20:718–725. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
120
|
Al-Janabi H, Moyes K, Allen R, Fisher M, Crespo M, Gurel B, Rescigno P, de Bono J, Nunns H, Bailey C, et al: Targeting a STING agonist to perivascular macrophages in prostate tumors delays resistance to androgen deprivation therapy. J Immunother Cancer. 12:e009362024. View Article : Google Scholar
|
|
121
|
Piper M, Van Court B, Mueller A, Watanabe S, Bickett T, Bhatia S, Darragh LB, Mayeda M, Nguyen D, Gadwa J, et al: Targeting Treg-expressed STAT3 enhances NK-Mediated surveillance of metastasis and improves therapeutic response in pancreatic adenocarcinoma. Clin Cancer Res. 28:1013–1026. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
122
|
Kurose K, Ohue Y and Oka M: Anti-CCR4 mAb and regulatory T cells. Gan To Kagaku Ryoho. 40:1150–1155. 2013.(In Japanese). PubMed/NCBI
|
|
123
|
Sugiyama D, Nishikawa H, Maeda Y, Nishioka M, Tanemura A, Katayama I, Ezoe S, Kanakura Y, Sato E, Fukumori Y, et al: Anti-CCR4 mAb selectively depletes effector-type FoxP3+CD4+ regulatory T cells, evoking antitumor immune responses in humans. Proc Natl Acad Sci USA. 110:17945–17950. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
124
|
Watanabe T, Ishino T, Ueda Y, Nagasaki J, Sadahira T, Dansako H, Araki M and Togashi Y: Activated CTLA-4-independent immunosuppression of Treg cells disturbs CTLA-4 blockade-mediated antitumor immunity. Cancer Sci. 114:1859–1870. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
125
|
Burbach BJ, O'Flanagan SD, Shao Q, Young KM, Slaughter JR, Rollins MR, Street TJL, Granger VE, Beura LK, Azarin SM, et al: Irreversible electroporation augments checkpoint immunotherapy in prostate cancer and promotes tumor antigen-specific tissue-resident memory CD8+ T cells. Nat Commun. 12:38622021. View Article : Google Scholar : PubMed/NCBI
|
|
126
|
Xu J, Wang R, Cheng S, Wangmo S, Yang J, Jin F, Lu X, Ma L, Zhu Y, Sun H, et al: Bispecific targeting of 4-1BB and CCR8 boosts antitumor immunity via Ti-Treg depletion and CD8+ activation. iScience. 28:1128292025. View Article : Google Scholar : PubMed/NCBI
|
|
127
|
Gurrea-Rubio M, Wu Q, Amin MA, Sule G, Carmona-Rivera C, Lucotti S, Ikari Y, Wu Q, Campbell PL, Gurrea-Rubio M, et al: Activation of cytotoxic lymphocytes through CD6 enhances killing of cancer cells. Cancer Immunol Immunother. 73:342024. View Article : Google Scholar : PubMed/NCBI
|
|
128
|
Nyalali AMK, Leonard AU, Xu Y, Li H, Zhou J, Zhang X, Rugambwa TK, Shi X and Li F: CD147: An integral and potential molecule to abrogate hallmarks of cancer. Front Oncol. 13:12380512023. View Article : Google Scholar : PubMed/NCBI
|
|
129
|
Alati S, Singh R, Pomper MG, Rowe SP and Banerjee SR: Preclinical development in radiopharmaceutical therapy for prostate cancer. Semin Nucl Med. 53:663–686. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
130
|
Frantellizzi V, Cosma L, Brunotti G, Pani A, Spanu A, Nuvoli S, De Cristofaro F, Civitelli L and De Vincentis G: Targeted alpha therapy with Thorium-227. Cancer Biother Radiopharm. 35:437–445. 2020.PubMed/NCBI
|
|
131
|
Dong L, Myers KV and Pienta KJ: Understanding the tumor-immune microenvironment in prostate cancer. Curr Opin Oncol. 33:231–237. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
132
|
Rathi N, McFarland TR, Nussenzveig R, Agarwal N and Swami U: Evolving role of immunotherapy in metastatic castration refractory prostate cancer. Drugs. 81:191–206. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
133
|
Wang X, Tan B, Liu J, Wang J, Chen M, Yang Q, Zhang X, Li F, Wei Y, Wu K, et al: Echinacoside inhibits tumor immune evasion by downregulating inducible PD-L1 and reshaping tumor immune landscape in breast and colorectal cancer. Phytomedicine. 135:1561882024. View Article : Google Scholar : PubMed/NCBI
|
|
134
|
Qi Z, Xu Z, Zhang L, Zou Y, Li J, Yan W, Li C, Liu N and Wu H: Overcoming resistance to immune checkpoint therapy in PTEN-null prostate cancer by intermittent anti-PI3Kα/β/δ treatment. Nat Commun. 13:1822022. View Article : Google Scholar : PubMed/NCBI
|
|
135
|
Ma R, Hu X, Zhang X, Wang W, Sun J, Su Z and Zhu C: Strategies to prevent, curb and eliminate biofilm formation based on the characteristics of various periods in one biofilm life cycle. Front Cell Infect Microbiol. 12:10030332022. View Article : Google Scholar : PubMed/NCBI
|
|
136
|
Shen AN, Lin YL, Zhao XH, Li JG, Monteiro MJ and Gu WY: Bone targeted nano-drug and nano-delivery. Bone Res. 12:512024. View Article : Google Scholar : PubMed/NCBI
|
|
137
|
Fan Z, Wang Z, Zhang H, Zhang H, Zhao R, Zhu SM and Liu XQ: Extracellular vesicles derived from mature dendritic cells loaded with cDC1-specific chemokine XCL1 combined with chemotherapy-induced ICD for the treatment of castration-resistant prostate cancer. Cancer Immunol Immunother. 74:2422025. View Article : Google Scholar : PubMed/NCBI
|
|
138
|
Silvestri I, Cattarino S, Giantulli S, Nazzari C, Collalti G and Sciarra A: A perspective of immunotherapy for prostate cancer. Cancers (Basel). 8:642016. View Article : Google Scholar : PubMed/NCBI
|
|
139
|
Melo CM, Vidotto T, Chaves LP, Lautert-Dutra W, Reis RBD and Squire JA: The role of somatic mutations on the immune response of the tumor microenvironment in prostate cancer. Int J Mol Sci. 22:95502021. View Article : Google Scholar : PubMed/NCBI
|
|
140
|
Murphy KC, DeMarco KD, Zhou L, Peura J, Giwa HK, Lopez-Diaz Y, Ho YJ, Li J, Bai S, Simin K, et al: MYC and p53 alterations cooperate through VEGF signaling to repress cytotoxic T cell and immunotherapy responses in prostate cancer. Cancer Res. 85:4359–4379. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
141
|
De Velasco MA, Kura Y, Fujita K and Uemura H: Moving toward improved immune checkpoint immunotherapy for advanced prostate cancer. Int J Urol. 31:307–324. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
142
|
Ren C, Li J, Zhou Y, Zhang S and Wang Q: Typical tumor immune microenvironment status determine prognosis in lung adenocarcinoma. Transl Oncol. 18:1013672022. View Article : Google Scholar : PubMed/NCBI
|
|
143
|
Zhao B, Lu W, Chen Y and Cai X: Predictive model for prognosis, immune microenvironment and drug sensitivity of colon carcinoma based on cuproptosis-related genes. Int J Clin Exp Pathol. 18:148–165. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
144
|
Li C, Xiao Y, Cao H, Chen Y, Li S and Yin F: Cuproptosis regulates microenvironment and affects prognosis in prostate cancer. Biol Trace Elem Res. 202:99–110. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
145
|
Xu J, Gao D, Ren C, Wang Z, Yuan F and Shen Y: Emerging implications of N6-methyladenosine in prostate cancer progression and treatment. Cell Death Discov. 11:3912025. View Article : Google Scholar : PubMed/NCBI
|
|
146
|
Song Q, Zhou R, Shu F and Fu W: Cuproptosis scoring system to predict the clinical outcome and immune response in bladder cancer. Front Immunol. 13:9583682022. View Article : Google Scholar : PubMed/NCBI
|
|
147
|
Zhao Y, Sun H, Zheng J and Shao C: Analysis of RNA m6A methylation regulators and tumour immune cell infiltration characterization in prostate cancer. Artif Cells Nanomed Biotechnol. 49:407–435. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
148
|
Liu Z, Zhong J, Zeng J, Duan X, Lu J, Sun X, Liu Q, Liang Y, Lin Z, Zhong W, et al: Characterization of the m6A-associated tumor immune microenvironment in prostate cancer to aid immunotherapy. Front Immunol. 12:7351702021. View Article : Google Scholar : PubMed/NCBI
|
|
149
|
Ramirez CFA, Taranto D, Ando-Kuri M, de Groot MHP, Tsouri E, Huang Z, de Groot D, Kluin RJC, Kloosterman DJ, Verheij J, et al: Cancer cell genetics shaping of the tumor microenvironment reveals myeloid cell-centric exploitable vulnerabilities in hepatocellular carcinoma. Nat Commun. 15:25812024. View Article : Google Scholar : PubMed/NCBI
|
|
150
|
Boufaied N, Chetta P, Hallal T, Cacciatore S, Lalli D, Luthold C, Homsy K, Imada EL, Syamala S, Photopoulos C, et al: Obesogenic High-Fat diet and MYC cooperate to promote lactate accumulation and tumor microenvironment remodeling in prostate cancer. Cancer Res. 84:1834–1855. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
151
|
Huang WB, Lai HZ, Long J, Dai ZL, Ma Q, Xiao C and You FM: Biomechanics of the tumor extracellular matrix and regulatory T cells: Regulatory mechanisms and potential therapeutic targets. Cell Commun Signal. 23:3752025. View Article : Google Scholar : PubMed/NCBI
|
|
152
|
Sooi K, Walsh R, Kumarakulasinghe N, Wong A and Ngoi N: A review of strategies to overcome immune resistance in the treatment of advanced prostate cancer. Cancer Drug Resist. 6:656–673. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
153
|
Xue D, Xu Y, Kyani A, Roy J, Dai L, Sun D and Neamati N: Discovery and lead optimization of benzene-1,4-disulfonamides as oxidative phosphorylation inhibitors. J Med Chem. 65:343–368. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
154
|
Kawuribi V, Xie Y, Xu H, Zhang Y and Zheng S: Nano-omics and nanomedicine target microbial carcinogenesis: Tumor microenvironment reprograming to clinical translation. Crit Rev Oncol Hematol. 213:1048662025. View Article : Google Scholar : PubMed/NCBI
|
|
155
|
Singh DD, Haque S, Kim Y, Han I and Yadav DK: Remodeling of tumour microenvironment: Strategies to overcome therapeutic resistance and innovate immunoengineering in triple-negative breast cancer. Front Immunol. 15:14552112024. View Article : Google Scholar : PubMed/NCBI
|
|
156
|
Alradwan I, Ahmed T, He C, Henderson JT, Rauth AM and Wu XY: Remodeling tumor immune microenvironment by using polymer-Lipid-manganese dioxide nanoparticles with radiation therapy to boost immune response of castration-Resistant Prostate Cancer. Research (Wash D C). 6:02472023.PubMed/NCBI
|
|
157
|
Garcia-Robledo JE, Cabrera-Salcedo S, Michael Brandauer A, Romano F, Rengifo-Martinez J, Toro-Pedroza A, Sebastián Victoria A, Rios-Serna LJ, Loukanov A, Cardona AF, et al: Engineering the next generation of CAR T-cells: Precision modifications, logic gates and universal strategies to overcome exhaustion and tumor resistance. Front Oncol. 15:16984422026. View Article : Google Scholar : PubMed/NCBI
|














