Glioma currently represents the most common and
aggressive primary brain tumor in adults and has been associated
with a poor prognosis (1). Despite
the progress achieved by research on glioma treatments, the median
survival time of patients with glioma remains <15 months
(2,3). One of the primary drivers of
therapeutic resistance in glioma is the markedly complex and
immunosuppressive tumor microenvironment (TME), which has been
shown to not only support tumor growth but also to actively subvert
antitumor immunity (4–6).
Tumor-associated microglia and tumor-associated
macrophages (collectively termed TAMs) constitute dominant
components of the TME of glioma (4,7,8).
Notably, TAMs can be manipulated by glioma cells to adopt an
immunosuppressive phenotype that facilitates tumor progression,
angiogenesis and treatment resistance (8–13).
However, the simplistic binary classification of TAMs into
pro-inflammatory or anti-inflammatory phenotypes that was employed
previously is no longer adequate; these cells have now been
recognized to exhibit multifaceted and context-dependent roles in
the TME (8–13).
Triggering receptor expressed on myeloid cells
(TREM)2 is an important immunoregulatory receptor that governs key
microglial functions, such as phagocytosis, lipid metabolism,
viability and inflammatory responses (14,15).
Although the protective effects of TREM2 in Alzheimer's disease
(AD) remain well-documented (16,17),
the dual function of TREM2 in glioma has been a notable source of
research and debate. On one hand, notable evidence has positioned
TREM2 as a promoter of glioma; the pro-tumor activity of TREM2 is
primarily mediated by its ability to foster an immunosuppressive
microenvironment and enhance angiogenesis, which in turn promotes
glioma progression (18–20). However, emerging evidence has also
suggested that, under specific conditions, TREM2 can play an
immunoprotective role in glioma. Recently, a key study revealed
that TREM2 deficiency in glioma models accelerates tumor
progression, and this effect was linked to impaired
myeloid-mediated phagocytosis of tumor cells and reduced major
histocompatibility complex class II (MHCII) expression, which
subsequently resulted in a loss of CD4+ T cells
(21). In addition, another recent
study identified TREM2 as an immunoprotective factor in
glioblastoma (GBM), and its deficiency has been shown to accelerate
tumor progression, directly contrasting with its established
immunosuppressive role in peripheral cancers (22–25).
These findings illustrate the complex mechanistic role of TREM2 in
glioma, reflecting the intricacy of the TME in the central nervous
system (CNS) and highlighting the importance of further research
into the role of this receptor in glioma.
Given the notable role of TAMs in the glioma
microenvironment, these cells have become a central research focus
within glioma oncology, with numerous studies aiming to understand
their interactions with key pathological processes, such as tumor
progression, recurrence and immunotherapy responses. Within the
context of glioma, TREM2 has emerged as an important molecular
regulator of tumor progression, exhibiting the dual capacity to
both protect against and contribute to glioma pathology (22–25).
This duality underscores the notable complexity of TREM2 activity
in glioma, as well as the requirement for further in-depth
investigations into the multifaceted roles of TREM2 in glioma
pathogenesis within the CNS.
TREM2 is an important immunoregulatory receptor that
is predominantly expressed on microglial cells, which are resident
macrophages of the CNS (26,27).
Notably, TREM2 has been shown to form a signaling complex with the
adaptor protein TYRO protein tyrosine kinase-binding protein
(DAP12), which is important for transducing signals that govern key
myeloid functions, such as phagocytosis, cell survival, lipid
metabolism and the modulation of inflammatory responses (28). As such, TREM2 is a central
regulator of immune homeostasis in the CNS and has been shown to
play an important, albeit context-dependent, role across a spectrum
of pathological conditions, ranging from neurodegenerative diseases
to cancer (16,29).
TREM2 activity is initiated by its interaction with
a diverse array of ligands, such as lipids, apolipoproteins and
amyloid-β (Aβ). These interactions trigger downstream signaling
that is important for maintaining CNS integrity (30–32).
Notably, TREM2 activity is important for a number of fundamental
neural processes. For example, during development, TREM2 is
required for synaptic pruning, and TREM2 deficiency has been shown
to lead to impaired synapse elimination and altered neural
connectivity (33). Another core
function exhibited by TREM2 is the regulation of phagocytic
clearance, enabling microglia to remove apoptotic neurons, myelin
debris and protein aggregates, thereby supporting CNS tissue
homeostasis and neuronal health (32,34–37).
In AD, TREM2 has been shown to bind to Aβ oligomers, facilitating
their clearance and modulating microglial responses to amyloid
plaques. This interaction is important as it mitigates the
progression of AD by influencing microglial activation and
viability (38,39). However, TREM2 exhibits a dual role
in inflammation in the CNS; although it can promote the resolution
of inflammation, TREM2 signaling has also been shown to exacerbate
neuropathic pain by driving the release of pro-inflammatory
cytokines from microglia (40).
Conversely, in models of ischemic stroke, TREM2 activity has been
shown to partially attenuate neuroinflammation and CNS injury,
highlighting its therapeutic potential in mitigating neural
inflammation (41,42).
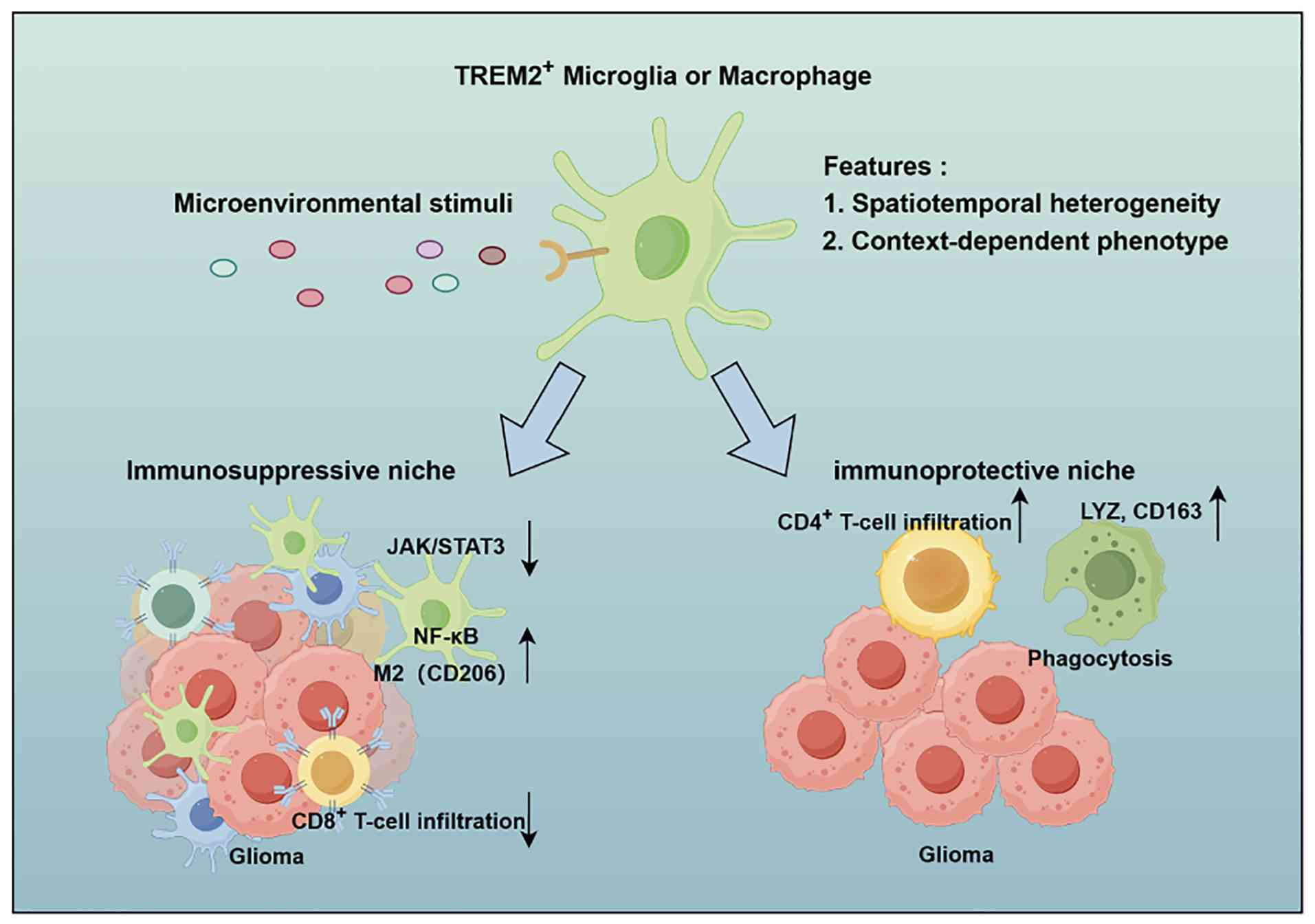
In the TME of glioma, the TREM2 signaling pathway is
activated in myeloid cells by numerous ligands. However, the
functional outcome of this activation is notably context-dependent,
embodying a dual role that can either promote tumor progression or
support antitumor immunity. Although TREM2 signaling is frequently
activated by glioma cells to foster an immunosuppressive niche and
support tumor growth (18,19), the TREM2-regulated capacity of
microglia for phagocytosis and antigen presentation is important
for T-cell activation (21,22).
This inherent duality makes TREM2 a central but complex signaling
hub in glioma pathology. Hijacked TREM2 signaling has been shown to
regulate the TME in glioma through the mechanisms discussed in this
section (Fig. 1).
In glioma, TREM2 knockdown in microglia has been
shown to promote a pro-inflammatory microglial phenotype and
suppress tumor progression by increasing the activity of the Janus
kinase/STAT signaling pathway and suppressing the NF-κB pathway.
Consequently, the transcriptional program that sustains an
immunosuppressive niche in the glioma TME is suppressed (43–47).
These findings indicate that TREM2 contributes to the development
of an immunosuppressive microenvironment, which is a characteristic
feature of glioma pathology (7,48,49).
TREM2 expression has also been strongly associated with the M2
polarization of microglia and macrophages, which has been linked to
a higher glioma grade and a poorer prognosis for patients (18,19,50).
Notably, inhibition of TREM2 signaling reprograms myeloid cells
toward a pro-inflammatory phenotype, promoting CD8+
T-cell infiltration and activity in the TME. Furthermore, TREM2
inhibition has been shown to synergize with anti-programmed cell
death protein 1 immunotherapy to improve patient survival in
preclinical glioma models (20).
Collectively, these findings underscore the concept that the
TREM2-dependent immunosuppressive niche contributed to by TAMs is
markedly involved in promoting tumor advancement and treatment
failure in glioma.
Studies have demonstrated that TREM2 signaling
enhances the uptake of glioma cells by myeloid cells; this increase
in phagocytic function has been associated with changes in the
levels of canonical phagocytosis markers, for example, lysozyme and
CD163. TREM2 has also been shown to trigger the phosphorylation of
DAP12 and activate downstream spleen tyrosine kinase (Syk), which
is an important event for the efficient phagocytosis of tumor
cells, acting through cytoskeletal remodeling, calcium
mobilization, and activation of PI3K-AKT and MAPK signaling
pathways (51–54).
Notably, this TREM2-mediated regulation of
phagocytosis extends beyond the clearance of tumor cells to
influence the direct interactions of microglial cells with adaptive
immunity. This functional link is important for regulating
efficient antigen presentation. Notably, TREM2 deficiency impairs
MHCII expression on TAMs, leading to a reduction in CD4+
T-cell tumor infiltration and diminished antitumor immune responses
(21). By applying integrated
single-cell and spatial transcriptomics, a recent study redefined
the role of TREM2 in GBM. In contrast to its established role as a
key immunosuppressive target in peripheral tumors, the
aforementioned study reported that TREM2 appears to exert an
immunoprotective function in GBM; its deficiency was shown to
accelerate tumor progression and to associate with
immunosuppressive signatures (22). Collectively, these findings
underscore that TREM2 plays a central yet complex role in
phagocytosis and immune reprogramming, challenging simplistic
strategies for therapeutic inhibition of TREM2 and demanding
context-specific strategies.
A central dilemma to be elucidated concerns the
mechanisms that prime TREM2-expressing myeloid cells toward a
pro-tumor vs. an antitumor state. The determination of these
phenotypes likely involves spatial, metabolic and temporal factors
within the glioma microenvironment. Regarding molecular triggers,
TREM2-ligand identity represents an important determinant of
myeloid phenotype. TREM2 has been shown to bind to a diverse range
of molecules, including oxidized lipids, myelin debris and
apolipoproteins (30–32), although the ligand repertoire for
TREM2 likely varies across tumor models. Notably, redundant
pathways, such as those mediated by T-cell immunoglobulin and
mucin-domain containing-3 or AXL, may compensate for TREM2 loss.
Competitive ligand binding further complicates TREM2 signaling
(55,56).
Metabolic reprogramming of the glioma
microenvironment also shapes TREM2-mediated immune responses. TREM2
expression is closely linked to enhanced lipid metabolism in TAMs,
and the hypoxia-driven shift in lipid metabolism observed within
the tumor core may enhance TREM2 signaling to foster an
immunosuppressive TAM phenotype (57,58).
At the invasive margin of glioma, damage-associated molecules, for
example phosphatidylserine and gangliosides, are released from
disrupted neuronal architecture and activate TREM2 signaling; this
creates a functional gradient from pro-inflammatory signaling at
the tumor-neuron interface to an increasingly immunosuppressive
microenvironment toward the glioma core (59). Within this hypoxic core,
TREM2+ cells exhibit reduced antigen presentation
(59). Temporally, TREM2 does not
exert protective effects in the early stages of TAM
differentiation; instead, its expression peaks at the terminal
phase of monocyte-to-TAM differentiation, in parallel with
immunosuppressive hallmarks such as arginase 1, CD274 and
glycoprotein NMB (10).
Another overlooked layer of complexity regarding the
function of TREM2 is the heterogeneity observed between preclinical
glioma models themselves. The commonly used orthotopic glioma cell
lines, namely the GL261, CT2A, NPA C54B and SB28 cell lines, harbor
distinct genetic backgrounds and origins (60,61).
Consequently, their responses to immune checkpoint blockade are
notably different; for example, GL261 cells are immune checkpoint
blockade-responsive, whereas SB28 cells demonstrate resistance to
this treatment (60). These
divergent responses may consequently influence the specific
mechanisms underlying TREM2-mediated responses in these models. In
the GL261 glioma model, TREM2 expression has been associated with a
shift from a pro-inflammatory to an immunosuppressive immune
microenvironment (10). The
aforementioned factors, including glioma model immunogenicity,
ligand availability, receptor redundancy, spatial niche and
temporal stage of differentiation, converge in a context-dependent
manner to influence the outcomes of TREM2 activity in glioma.
Future studies using spatial transcriptomics, lineage tracing,
metabolic profiling and glioma-model comparisons are required to
identify therapeutically targetable switches.
The dual nature of TREM2 notably reflects the
heterogeneity of high-grade glioma and the complex interplay of
TREM2 with the TME (61). This
interaction-based heterogeneity results in the marked
context-dependency of the immune functions of TREM2; its intrinsic
phagocytic and antigen-presenting capacity can, under specific
conditions, support antitumor immunity (21), whereas hijacking TREM2 activity to
induce its immunosuppressive function has been shown to promote
immune evasion and tumor progression in glioma. Consequently,
within this complex microenvironment, TREM2 emerges as a central,
yet multilayered, immune-signaling hub. Therapeutic targeting of
TREM2 therefore requires precise modulation to effectively block
the activity of its pro-tumor pathways whilst preserving its
residual or inducible protective functions, making it a compelling
but challenging axis for TME reprogramming (15).
Studies have indicated that TREM2 holds notable
potential for the diagnosis and prognosis of glioma; its expression
is markedly higher in tumor tissues from patients with GBM compared
with that in normal tissues or low-grade glioma cases (19). Furthermore, this elevated
expression has been shown to associate markedly with molecular
features linked to the aggressive behavior of the tumor, including
the mesenchymal subtype, isocitrate dehydrogenase (IDH) wild-type
status and lack of 1p/19q codeletion (19). Supporting its functional role,
TREM2 deficiency in mouse glioma models has been shown to result in
a reduction in the proportion of M2-polarized microglia within
tumors, underscoring the key role of TREM2 in remodeling the
immunosuppressive TME (43).
Notably, emerging single-cell resolution data have revealed that a
TREM2-high lipid-metabolic macrophage subset is linked to poorer
survival outcomes for patients with glioma (50). However, high TREM2 expression,
specifically within tumor-infiltrating myeloid cells, has
paradoxically been associated with improved survival outcomes and
an antitumor immune signature in a study by Zhong et al
(22). The expression profile of
TREM receptors in the peripheral circulation also carries
prognostic importance. Research has shown that a higher TREM1/TREM2
ratio on circulating CD14+ monocytes is an independent
predictor of reduced overall survival, whereas a higher percentage
of TREM2+ monocytes has been associated with improved
patient outcomes specifically in the GBM subgroup (62). Furthermore, this relationship may
be modulated by a number of factors, such as vitamin D levels,
which are positively associated with the proportion of
TREM2+ monocytes in low-grade glioma (63). These results indicate that
composite indicators incorporating TREM2 and other biological
markers possess superior potential for guiding clinical prognosis
assessment relative to single markers.
A study has demonstrated that soluble TREM2 (sTREM2)
levels are markedly elevated in the cerebrospinal fluid (CSF) of
patients with multiple sclerosis but return to normal following
treatment. By extension, TREM2 shows promise as a diagnostic
biomarker in the CSF of patients with glioma (64). Similarly, elevated sTREM2 levels
observed in the CSF of patients with neuromyelitis optica spectrum
disorder, which is also a type of neuroinflammatory condition, have
been genetically and clinically associated with disease risk and
severity. Notably, elevated sTREM2 levels have been shown to result
in microglial dysfunction and NF-κB pathway activation. This
pathological state is characterized by excessive activation,
enhanced phagocytosis and metabolic reprogramming (65). In another study of 205 patients
with GBM, AD-associated neuropathological changes were present in
the tumor-adjacent cortex of 52% of patients, and the degree of
this pathology was positively associated with microglial activation
(66). However, the cross-disease
robustness of sTREM2 levels as a biomarker for CNS pathology
presents a notable challenge for glioma-specific diagnosis.
Therefore, sTREM2 alone is unlikely to reliably differentiate
high-grade glioma from other neuroinflammatory or neurodegenerative
conditions in a clinical setting.
To enhance its specificity as a biomarker, sTREM2
should be: i) Incorporated into a multi-analyte panel that includes
multiple tumor-derived markers, such as glial fibrillary acidic
protein, matrix metalloproteinases, IDH mutation status or
O-6-methylguanine-DNA methyltransferase promoter methylation; or
ii) combined with advanced imaging features. Furthermore,
establishing disease-specific sTREM2 cut-off values and dynamically
monitoring sTREM2 changes over time may improve its clinical
utility as a biomarker of glioma. Future studies should directly
compare CSF-derived sTREM2 levels between patients with glioma and
well-matched control groups with other neurological diseases to
define its specificity and diagnostic accuracy. Together, these
findings suggest the potential of sTREM2 as a diagnostic and
prognostic biomarker for brain tumors (67,68).
Targeting the TREM2 signaling pathway represents a
promising therapeutic strategy for reprogramming microglia within
the glioma TME. Preclinical studies, primarily those using the
murine GBM cell line GL261, have demonstrated that TREM2 deficiency
or knockdown markedly inhibits tumor growth and angiogenesis
(18,43). This antitumor effect is linked to
the inhibition of key pro-survival and inflammatory pathways in the
microglia, such as the Wnt/β-catenin and NF-κB pathways, which can
in turn enhance antitumor immune responses (43,69).
In AD research, targeting TREM2 on microglia has achieved notable
therapeutic progress toward mitigating AD-associated pathological
changes. For example, a phase I clinical trial using the
TREM2-targeting antibody AL002 demonstrated target engagement and
pharmacodynamic effects in the CNS of patients with AD (70). Although, to the best of our
knowledge, clinical trials targeting TREM2 have not yet been
launched in glioma, the progress made in the phase 2 trial of AL002
in AD (70) offers important
preliminary evidence for pharmacologically modulating TREM2 in the
human brain for glioma therapy.
Beyond direct receptor inhibition, a recent study
has explored TREM2 as a target for precision drug delivery using an
innovative strategy. This study designed TREM2-specific
peptide-conjugated nanoliposomes to deliver doxorubicin
specifically to glioma cells; this approach demonstrated enhanced
drug accumulation in brain tumors and improved antitumor efficacy
compared with untargeted PLD (non-modified PEGylated nanoliposomal
doxorubicin) in preclinical models, validating the effectiveness of
TREM2-targeting strategies in glioma therapy (71).
The findings of the aforementioned studies have
offered valuable insights for future therapeutic directions in
glioma research, including direct TREM2 inhibition or precision
drug delivery leveraging the TREM2 signaling pathway. Examples of
potential therapeutic strategies targeting TREM2 in neuro-oncology
include the use of precision-targeted nanotechnology, antibody
engineering and the development of novel inhibitor designs; these
strategies may be combined with existing therapies to modulate the
immunosuppressive glioma TME and improve immunotherapeutic
outcomes. However, the role of TREM2 in glioma is marked by notable
functional heterogeneity; this functional duality highlights the
requirement for further research in order to elucidate the complex
mechanisms of TREM2 in glioma, thereby providing a solid foundation
for the development of future clinical therapeutic strategies.
Preclinical studies have demonstrated that
strategies targeting TREM2 show notable promise for glioma therapy,
yet there remain numerous challenges to realizing the clinical
potential of these strategies. A primary challenge lies in the
complexity of the ligand-receptor interactions of TREM2. As a
multiligand receptor, TREM2 binds to a diverse array of molecules
(55), which in turn trigger
multiple downstream effects, complicating its therapeutic targeting
(22). This characteristic of
TREM2 may be a contributing factor to the clinical failure of some
ligand-dependent TREM2 inhibitors (56). Such clinical failure highlights the
translational gap between promising preclinical data and clinical
outcomes. The dynamic nature of ligand binding, along with the
existence of multiple known and unknown ligands competing for the
receptor in human biology, makes it difficult to achieve effective
and specific TREM2 blockade with conventional approaches (56). To overcome this challenge, a shift
in therapeutic development toward innovative ligand-independent
inhibition strategies would enable the blockade of downstream
signaling from a novel perspective, permitting TREM2 blockade
irrespective of which ligand is bound. Such an approach could
diminish the impact of competitive ligands and reduce the
off-target effects of inhibitors, consequently allowing inhibitors
to function more effectively (56,72,73).
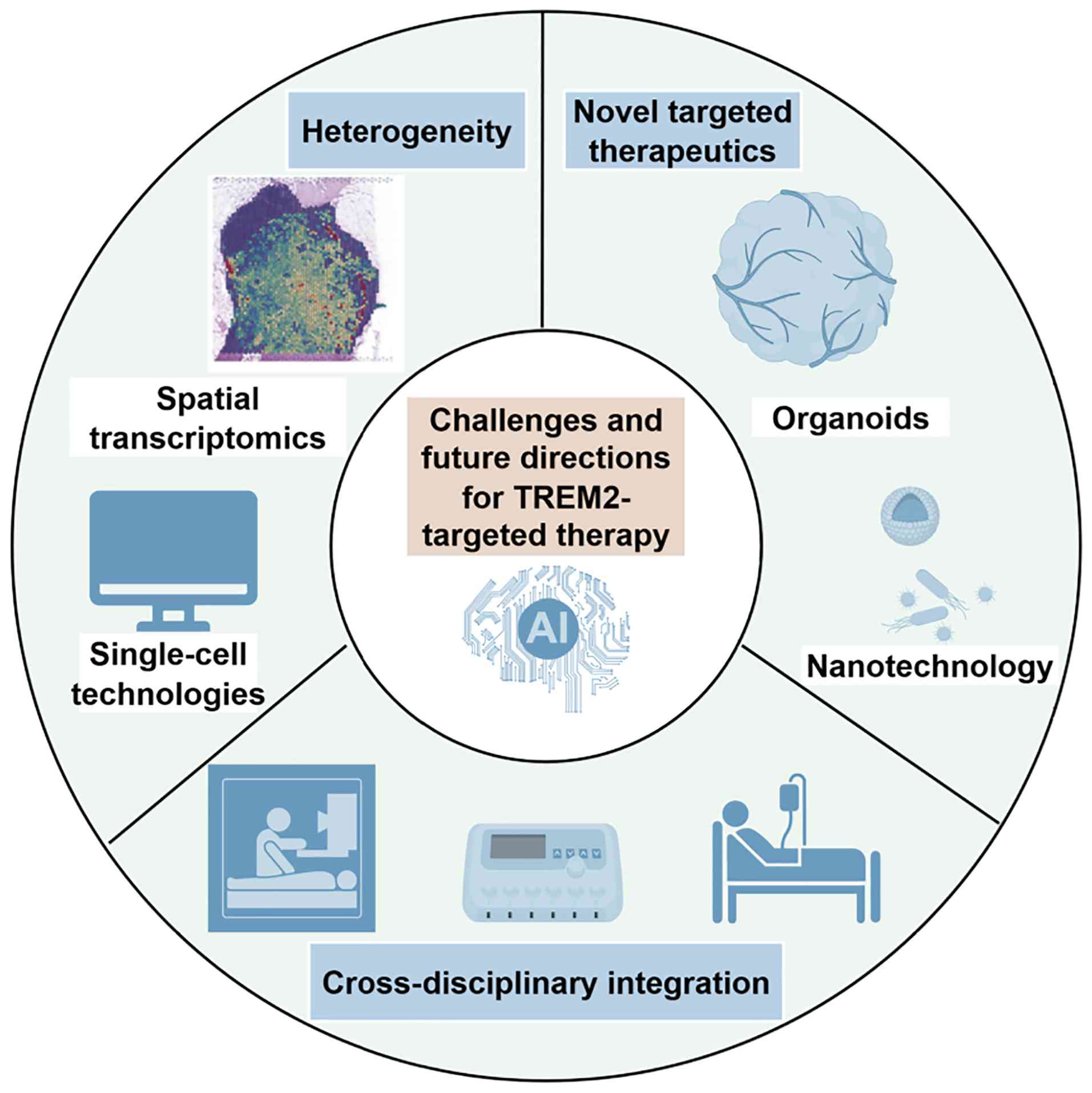
Future research should focus on developing precision
medicine and multidimensional strategies to effectively advance
targeted drug development and immunotherapy (Fig. 2). The dual functionality of TREM2
is highly context-dependent within the glioma microenvironment. The
integration of single-cell and spatial multi-omics technologies
will enable future research to move beyond bulk analyses and to
precisely assess the functional heterogeneity of TREM2-expressing
microglia and macrophages across different tumor regions and
disease stages (10,22,59).
For example, single-cell RNA sequencing has revealed that myeloid
cell states in glioma are driven more by microenvironmental signals
than by cellular origin, identifying distinct immunosuppressive and
inflammatory programs (8,48,74).
Notably, spatial transcriptomic technologies are now enabling
researchers to map these cellular states within the intact tissue
architecture (75,76). As such, spatial transcriptomics has
proven effective in resolving cellular heterogeneity and spatial
organization within tumors. For example, a study in GBM employed
spatial transcriptomic technologies to highlight the heterogeneous
infiltration patterns of immune cells from the tumor core to the
invasive margin (75). The
application of single-cell and spatial transcriptomic technologies
in future studies will help to elucidate the spatial localization,
temporal dynamics and specific interactions of TREM2+
TAMs in glioma (10,21,22,59),
including interactions with glioma cells, various immune cells and
TME components, such as vascular endothelial cells.
Determining whether TREM2 inhibition or activation
associates with an immunosuppressive or immunoprotective
microenvironment in patients with specific genetic backgrounds is
important for glioma therapy. Furthermore, understanding whether
variations in these spatiotemporal interactions (TREM2+
TAM interactions with glioma cells, various immune cells and TME
components) enhance or undermine immunotherapeutic efficacy, or
whether these interactions associate with therapeutic resistance,
is important for designing optimal clinical interventions and
achieving precision medicine goals; the elucidation of mechanisms
responsible for these clinical features is also necessary for
improving therapeutic outcomes. Notably, exploring the differential
metabolic regulation of TREM2+ TAMs at specific
spatiotemporal nodes, including lipid metabolism pathways analogous
to those in AD models, presents another promising option for
deciphering the function of these cells and identifying novel
therapeutic targets (69).
Nanotechnology has been shown to provide robust
technical support for effective TREM2-targeted therapy, enabling
the precise delivery of targeted drugs and supporting their
regulation of the TME through highly specific and controlled drug
release (77–79). One notable study investigated the
therapeutic efficacy of a novel strategy integrating synthetic
immunology and protein-engineering designed myeloid-targeted
immunocytokines (MiTEs), which can bind to TREM2 on
immunosuppressive TAMs. After being cleaved by a specific protease
present in TAMs, MiTEs released an IL-2 signal that activated
cytotoxic T cells and natural killer cells, thereby initiating an
antitumor immune response. This strategy achieved notable efficacy
in preclinical models by orchestrating a multi-axis antitumor
immune response while minimizing systemic toxicity, indicating the
promising potential of TREM2-targeted immunotherapy (80).
Concurrently, a recent study developed PEGylated
nanoliposomes conjugated with TREM2-targeting peptides for use in
glioma therapy. Although this construct delivered a conventional
chemotherapeutic agent, doxorubicin, rather than directly
modulating immunity, this therapeutic strategy validated the
effectiveness of TREM2-targeting nanocarriers. By leveraging
localized TREM2 expression, these nanoparticles achieved specific
targeting to glioma tissues and enhanced the accumulation of
antitumor drugs in targeted brain tumors, promoting their notable
tumor-killing effects. These findings demonstrate the potential of
TREM2-targeted nanodrug delivery for future integration with
immunotherapy or chemotherapy strategies in the treatment of glioma
(71).
Notably, advanced and reliable preclinical models
are important for discovering and validating the therapeutic
effects of nanodrugs or advanced biologics, such as MiTEs. This
highlights the advantages of optimized conditional-knockout mice
and patient-derived organoid co-culture models (81–83);
these models are valuable for studying the functions and mechanisms
of TREM2-associated TAMs, conducting high-throughput drug
screenings and investigating the dynamic interactions between
TREM2+ TAMs and other cells (81,84,85).
A notable and often underappreciated challenge to
therapeutic drug delivery is the blood-brain barrier (BBB), which
markedly restricts the delivery of systemically administered
biologics and nanoparticles into the brain parenchyma. Although the
BBB is locally disrupted at the GBM core, it remains largely intact
at the infiltrating tumor margin, which is a primary site of
recurrence (86,87). Therefore, even TREM2-targeted
nanoliposomes (71) or MiTEs
(80) that show robust efficacy in
preclinical intracranial models are hindered in clinical settings
by their large size, which limits passive diffusion across the
intact or partially intact BBB. Strategies to overcome this
size-limitation may include receptor-mediated transcytosis, for
example via transferrin or low-density lipoprotein receptor-related
protein 1 targeting, focused ultrasound-induced BBB disruption or
alternative drug delivery routes, such as intranasal administration
(88,89). Future TREM2-directed therapeutic
designs should incorporate such BBB-crossing mechanisms from the
outset for effective clinical translation.
The ultimate translation of TREM2-directed
strategies into clinical application will also be guided by notable
cross-disciplinary collaboration (Fig.
2). The convergence of neurosurgery, neuropathology and
molecular diagnostics is important for obtaining and analyzing
high-quality, spatially annotated tumor specimens (90). The data generated from these
specimens can span genomics, transcriptomics, proteomics and
digital pathology, collectively creating a complex and integrated
big-data network; as such, artificial intelligence (AI) and
big-data analytics may serve important roles in the clinical
translation of TREM2-targeted therapies (91–95).
AI can accelerate the design of novel
TREM2-targeting compounds at the drug discovery stage by modeling
protein-protein interactions, enabling virtual drug screening and
facilitating de novo molecular design to optimize drug
efficacy and safety, thereby reducing the reliance of drug
development on costly and resource-intensive traditional wet-lab
experiments. Furthermore, AI can integrate multi-omics data with
clinical imaging data to build predictive models that identify
patients harboring TREM2-driven immunosuppressive tumor niches,
thereby informing personalized therapy selection (96–100). In clinical development, AI can
optimize trial design and patient stratification by analyzing
real-world data, improving patient recruitment efficiency and
predicting patient survival outcomes, which is important for
efficiently testing the next generation of TREM2-directed therapies
(101–103). Furthermore, machine-learning
techniques such as federated learning can enable privacy-preserving
institutional collaboration by allowing AI models to be trained on
clinical data distributed across multiple institutions without the
raw data ever leaving its source. This is important for building
robust, generalizable models while adhering to strict data-security
and patient-privacy regulations (94,104). Harnessing AI-driven clinical-data
analysis in the future will be an important component for
deciphering the context-specific roles of TREM2 and translating
preclinical research findings into effective treatment methods for
glioma.
TREM2-associated TAMs represent a notable regulatory
node within the immune microenvironment of glioma. They are notable
mediators of the glioma TME and possess promising therapeutic
potential. Previous research has highlighted the dual role of TREM2
in glioma, encompassing both immunosuppressive and immunoprotective
functions; this duality reflects the complex biology of the brain
TME. Future research and therapeutic success will require the
stratification of patients based on the microenvironmental features
that determine whether the TREM2 signaling axis sustains tumor
growth or supports antitumor immunity in specific spatial and
temporal contexts. Subsequently, targeted precision medicine can be
developed based on the heterogeneity of these features. This will
require deeper investigation into TREM2 activity in glioma and the
integration of these research findings with innovative clinical
practices. Notably, interdisciplinary integration that incorporates
AI offers a promising possibility for elucidating the complexity of
TREM2 signaling and improving treatment outcomes for high-grade
glioma.
Not applicable.
Funding was received from the Key Specialist Fund (grant no.
41C41B26), the Medical Research Project of Chengdu City (grant no.
2024097) and the Military Center of Neuroanesthesia.
Not applicable.
JF conceptualized the study and contributed toward
performing the literature investigation, generating the figures and
writing the original draft of the manuscript. QH was responsible
for editing and reviewing the manuscript. DL contributed to
performing the literature investigation and reviewing and editing
the manuscript. SL contributed toward performing the literature
investigation and writing the original draft of the manuscript. HS
contributed to writing the original draft of the manuscript and
generating the figures. YW supervised the study and contributed to
writing the original draft of the manuscript. LY supervised the
study, conceptualized the study, reviewed and edited the manuscript
and acquired the funding. Data authentication is not applicable.
All authors read and approved the final version of the
manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Price M, Ballard C, Benedetti J, Neff C,
Cioffi G, Waite KA, Kruchko C, Barnholtz-Sloan JS and Ostrom QT:
CBTRUS statistical report: primary brain and other central nervous
system tumors diagnosed in the United States in 2017–2021. Neuro
Oncol. 26 (Suppl 6):vi1–vi85. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Schaff LR and Mellinghoff IK: Glioblastoma
and other primary brain malignancies in adults: A review. JAMA.
329:574–587. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tan AC, Ashley DM, López GY, Malinzak M,
Friedman HS and Khasraw M: Management of glioblastoma: State of the
art and future directions. CA Cancer J Clin. 70:299–312.
2020.PubMed/NCBI
|
|
4
|
Klemm F, Maas RR, Bowman RL, Kornete M,
Soukup K, Nassiri S, Brouland JP, Iacobuzio-Donahue CA, Brennan C,
Tabar V, et al: Interrogation of the microenvironmental landscape
in brain tumors reveals disease-specific alterations of immune
cells. Cell. 181:1643–1660.e17. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kloosterman DJ, Erbani J, Boon M, Farber
M, Handgraaf SM, Ando-Kuri M, Sánchez-López E, Fontein B, Mertz M,
Nieuwland M, et al: Macrophage-mediated myelin recycling fuels
brain cancer malignancy. Cell. 187:5336–5356.e30. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
White J, White MPJ, Wickremesekera A, Peng
L and Gray C: The tumour microenvironment, treatment resistance and
recurrence in glioblastoma. J Transl Med. 22:5402024. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Khan F, Pang L, Dunterman M, Lesniak MS,
Heimberger AB and Chen P: Macrophages and microglia in
glioblastoma: Heterogeneity, plasticity, and therapy. J Clin
Invest. 133:e1634462023. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Miller TE, El Farran CA, Couturier CP,
Chen Z, D'Antonio JP, Verga J, Villanueva MA, Gonzalez Castro LN,
Tong YE, Saadi TA, et al: Programs, origins and immunomodulatory
functions of myeloid cells in glioma. Nature. 640:1072–1082. 2025.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Li J, Ross JL, Hambardzumyan D and Brat
DJ: Immunopathology of glioblastoma. Annu Rev Pathol. 21:135–162.
2026. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kirschenbaum D, Xie K, Ingelfinger F,
Katzenelenbogen Y, Abadie K, Look T, Sheban F, Phan TS, Li B,
Zwicky P, et al: Time-resolved single-cell transcriptomics defines
immune trajectories in glioblastoma. Cell. 187:149–165.e23. 2024.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Pombo Antunes AR, Scheyltjens I, Lodi F,
Messiaen J, Antoranz A, Duerinck J, Kancheva D, Martens L, De
Vlaminck K, Van Hove H, et al: Single-cell profiling of myeloid
cells in glioblastoma across species and disease stage reveals
macrophage competition and specialization. Nat Neurosci.
24:595–610. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wang W, Li T, Cheng Y, Li F, Qi S, Mao M,
Wu J, Liu Q, Zhang X, Li X, et al: Identification of hypoxic
macrophages in glioblastoma with therapeutic potential for
vasculature normalization. Cancer Cell. 42:815–832.e12. 2024.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Waibl Polania J, Hoyt-Miggelbrink A,
Tomaszewski WH, Wachsmuth LP, Lorrey SJ, Wilkinson DS, Lerner E,
Woroniecka K, Finlay JB, Ayasoufi K and Fecci PE: Antigen
presentation by tumor-associated macrophages drives T cells from a
progenitor exhaustion state to terminal exhaustion. Immunity.
58:232–246.e6. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pocock J, Vasilopoulou F, Svensson E and
Cosker K: Microglia and TREM2. Neuropharmacology. 257:1100202024.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Molgora M, Liu YA, Colonna M and Cella M:
TREM2: A new player in the tumor microenvironment. Semin Immunol.
67:1017392023. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Deczkowska A, Weiner A and Amit I: The
physiology, pathology, and potential therapeutic applications of
the TREM2 signaling pathway. Cell. 181:1207–1217. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hou J, Chen Y, Grajales-Reyes G and
Colonna M: TREM2 dependent and independent functions of microglia
in Alzheimer's disease. Mol Neurodegener. 17:842022. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Chen X, Zhao Y, Huang Y, Zhu K, Zeng F,
Zhao J, Zhang H, Zhu X, Kettenmann H and Xiang X: TREM2 promotes
glioma progression and angiogenesis mediated by microglia/brain
macrophages. Glia. 71:2679–2695. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yu M, Chang Y, Zhai Y, Pang B, Wang P, Li
G, Jiang T and Zeng F: TREM2 is associated with tumor immunity and
implies poor prognosis in glioma. Front Immunol. 13:10892662023.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sun R, Han R, McCornack C, Khan S, Tabor
GT, Chen Y, Hou J, Jiang H, Schoch KM, Mao DD, et al: TREM2
inhibition triggers antitumor cell activity of myeloid cells in
glioblastoma. Sci Adv. 9:eade35592023. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zheng J, Wang L, Zhao S, Zhang W, Chang Y,
Bosco DB, Huang T, Dheer A, Gao S, Xu S, et al: TREM2 mediates
MHCII-associated CD4+ T-cell response against gliomas. Neuro Oncol.
26:811–825. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhong J, Xing X, Gao Y, Pei L, Lu C, Sun
H, Lai Y, Du K, Xiao F, Yang Y, et al: Distinct roles of TREM2 in
central nervous system cancers and peripheral cancers. Cancer Cell.
42:968–984.e9. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Park MD, Reyes-Torres I, LeBerichel J,
Hamon P, LaMarche NM, Hegde S, Belabed M, Troncoso L, Grout JA,
Magen A, et al: TREM2 macrophages drive NK cell paucity and
dysfunction in lung cancer. Nat Immunol. 24:792–801. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Chu T, Zhu G, Tang Z, Qu W, Yang R, Pan H,
Wang Y, Tian R, Chen L, Guan Z, et al: Metabolism archetype cancer
cells induce protumor TREM2+ macrophages via
oxLDL-mediated metabolic interplay in hepatocellular carcinoma. Nat
Commun. 16:67702025. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sun R, Lei C, Xu Z, Gu X, Huang L, Chen L,
Tan Y, Peng M, Yaddanapudi K, Siskind L, et al: Neutral ceramidase
regulates breast cancer progression by metabolic programming of
TREM2-associated macrophages. Nat Commun. 15:9662024. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lin M, Yu JX, Zhang WX, Lao FX and Huang
HC: Roles of TREM2 in the pathological mechanism and the
therapeutic strategies of Alzheimer's disease. J Prev Alzheimers
Dis. 11:1682–1695. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yin P, Su Z, Shu X, Dong Z and Tian Y:
Role of TREM2 in immune and neurological diseases: Structure,
function, and implications. Int Immunopharmacol. 143:1132862024.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhao Y, Guo Q, Tian J, Liu W and Wang X:
TREM2 bridges microglia and extracellular microenvironment:
Mechanistic landscape and therapeutical prospects on Alzheimer's
disease. Ageing Res Rev. 103:1025962025. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Painter MM, Atagi Y, Liu CC, Rademakers R,
Xu H, Fryer JD and Bu G: TREM2 in CNS homeostasis and
neurodegenerative disease. Mol Neurodegener. 10:432015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Vijayan N, Thanikachalam PV and Patel S:
Decoding of the role of TREM2 in neuropathic pain: Molecular
pathway and neuroinflammatory mechanism. Drug Dev Res.
86:e701112025. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Yang H, Kim D, Yang Y, Bagyinszky E and An
SSA: TREM2 in neurodegenerative disorders: Mutation spectrum,
pathophysiology, and therapeutic targeting. Int J Mol Sci.
26:70572025. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Atagi Y, Liu CC, Painter MM, Chen XF,
Verbeeck C, Zheng H, Li X, Rademakers R, Kang SS, Xu H, et al:
Apolipoprotein E is a ligand for triggering receptor expressed on
myeloid cells 2 (TREM2). J Biol Chem. 290:26043–26050. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Filipello F, Morini R, Corradini I, Zerbi
V, Canzi A, Michalski B, Erreni M, Markicevic M, Starvaggi-Cucuzza
C, Otero K, et al: The microglial innate immune receptor TREM2 is
required for synapse elimination and normal brain connectivity.
Immunity. 48:979–991.e8. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Konishi H and Kiyama H: Non-pathological
roles of microglial TREM2/DAP12: TREM2/DAP12 regulates the
physiological functions of microglia from development to aging.
Neurochem Int. 141:1048782020. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Cignarella F, Filipello F, Bollman B,
Cantoni C, Locca A, Mikesell R, Manis M, Ibrahim A, Deng L, Benitez
BA, et al: TREM2 activation on microglia promotes myelin debris
clearance and remyelination in a model of multiple sclerosis. Acta
Neuropathol. 140:513–534. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
McCray TJ, Bedford LM, Bissel SJ and Lamb
BT: Trem2-deficiency aggravates and accelerates age-related myelin
degeneration. Acta Neuropathol Commun. 12:1542024. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Xue T, Ji J, Sun Y, Huang X, Cai Z, Yang
J, Guo W, Guo R, Cheng H and Sun X: Sphingosine-1-phosphate, a
novel TREM2 ligand, promotes microglial phagocytosis to protect
against ischemic brain injury. Acta Pharm Sin B. 12:1885–1898.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Zhao Y, Wu X, Li X, Jiang LL, Gui X, Liu
Y, Sun Y, Zhu B, Piña-Crespo JC, Zhang M, et al: TREM2 is a
receptor for β-amyloid that mediates microglial function. Neuron.
97:1023–1031.e7. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Zhong L, Wang Z, Wang D, Wang Z, Martens
YA, Wu L, Xu Y, Wang K, Li J, Huang R, et al: Amyloid-beta
modulates microglial responses by binding to the triggering
receptor expressed on myeloid cells 2 (TREM2). Mol Neurodegener.
13:152018. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Kobayashi M, Konishi H, Sayo A, Takai T
and Kiyama H: TREM2/DAP12 signal elicits proinflammatory response
in microglia and exacerbates neuropathic pain. J Neurosci.
36:11138–11150. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Wei W, Zhang L, Xin W, Pan Y, Tatenhorst
L, Hao Z, Gerner ST, Huber S, Juenemann M, Butz M, et al: TREM2
regulates microglial lipid droplet formation and represses
post-ischemic brain injury. Biomed Pharmacother. 170:1159622024.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Kawabori M, Kacimi R, Kauppinen T,
Calosing C, Kim JY, Hsieh CL, Nakamura MC and Yenari MA: Triggering
receptor expressed on myeloid cells 2 (TREM2) deficiency attenuates
phagocytic activities of microglia and exacerbates ischemic damage
in experimental stroke. J Neurosci. 35:3384–3396. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Yan Y, Bai S, Han H, Dai J, Niu L, Wang H,
Dong Q, Yin H, Yuan G and Pan Y: Knockdown of trem2 promotes
proinflammatory microglia and inhibits glioma progression via the
JAK2/STAT3 and NF-κB pathways. Cell Commun Signal. 22:2722024.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Liu T, Gao H, Xi Z, Yu T, Gu Y, Mai H,
Yuan H, Liu Y, Liu H, Zhang Q, et al: CAR-T triggers TAM
reeducation and adaptive anti-tumor response via TREM2 deficiency
or CD40 agonist. Cell Rep Med. 7:1025392026. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Ruganzu JB, Zheng Q, Wu X, He Y, Peng X,
Jin H, Zhou J, Ma R, Ji S, Ma Y, et al: TREM2 overexpression
rescues cognitive deficits in APP/PS1 transgenic mice by reducing
neuroinflammation via the JAK/STAT/SOCS signaling pathway. Exp
Neurol. 336:1135062021. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Wang M, Zhao R, Su Y, Zhai D, Liang H,
Zhang L, Wang W, Wang Z, Qi M, Jiang X, et al:
4,4′-Dimethoxychalcone mitigates neuroinflammation following
traumatic brain injury through modulation of the
TREM2/PI3K/AKT/NF-κB signaling pathway. Inflammation. 48:3487–3505.
2025. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Yang D, Sun X, Wang H, Wistuba II, Wang H,
Maitra A and Chen Y: TREM2 depletion in pancreatic cancer elicits
pathogenic inflammation and accelerates tumor progression via
enriching IL-1β+ macrophages. Gastroenterology.
168:1153–1169. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Lin H, Liu C, Hu A, Zhang D, Yang H and
Mao Y: Understanding the immunosuppressive microenvironment of
glioma: Mechanistic insights and clinical perspectives. J Hematol
Oncol. 17:312024. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Elguindy MM, Young JS, Ho WS and Lu RO:
Co-evolution of glioma and immune microenvironment. J Immunother
Cancer. 12:e0091752024. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Li J, Yu X, Yang D, Chen S, Xu J, Ma X,
Huang C, Xu B, Xue L and Wang Y: Lipid-metabolically active
TREM2high microglia-derived macrophages predict poor
prognosis and represent an immunotherapeutic target in glioma. J
Neuroimmune Pharmacol. 20:922025. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Peshoff MM, Gupta P, Oberai S, Trivedi R,
Katayama H, Chakrapani P, Dang M, Migliozzi S, Gumin J, Kadri DB,
et al: Triggering receptor expressed on myeloid cells 2 (TREM2)
regulates phagocytosis in glioblastoma. Neuro Oncol. 26:826–839.
2024. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Li P, Sun Z, Chen Y, Fang Z, Yu D, Wang L,
Ren Y and Gong P: Role of eCIRP in mediating post-ischemia
microglial phagocytosis via TREM-2 receptor: insights from porcine
and mouse cellular models. Mol Neurobiol. 63:4832026. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Zhang Z, Yu K, Cao Y, Xie P, Wang L, Shen
Z and Qin J: TREM2 facilitates gastric cancer progression and
immune evasion via inhibiting TRIM21-mediated STAT1 degradation in
tumor-associated macrophages. Cell Death Dis. 16:8452025.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Zhao Y, Hu H, Wang J, Hu Y, Yang L, Wu Z,
Zhao S, Wang X, Mu Y, Zheng M, et al: SYK-dependent lipid handling
in monocyte-derived macrophages governs functional recovery after
spinal cord injury. Brain Res Bull. 237:1118232026. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Colonna M: The biology of TREM receptors.
Nat Rev Immunol. 23:580–594. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Sigalov AB: TREM-1 and TREM-2 as
therapeutic targets: Clinical challenges and perspectives. Front
Immunol. 15:14989932024. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Lu J, Chu S, Wang S, Wang S, Yu Z, Yan Z,
Ji G, Zhou H, Wang J and Zhu C: Spatiotemporal and metabolic
heterogeneity of tumor-associated macrophages in glioblastoma: From
single-cell insights to therapeutic targeting. Front Cell Dev Biol.
14:17742152026. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Cheng Y, Zhao W, Xie M, Zheng X, Ding F
and Du J: Decoding myeloid heterogeneity in glioblastoma: Spatial
insights from transcriptomics. J Transl Med. 24:4322026. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Villa G, Delev D and Heiland DH: Mapping
myeloid cell function: Spatial diversity in tumor and neuronal
microenvironment. Cancer Cell. 42:934–936. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Genoud V, Marinari E, Nikolaev SI, Castle
JC, Bukur V, Dietrich PY, Okada H and Walker PR: Responsiveness to
anti-PD-1 and anti-CTLA-4 immune checkpoint blockade in SB28 and
GL261 mouse glioma models. Oncoimmunology. 7:e15011372018.
View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Ghosh S and Rothlin CV: TREM2 function in
glioblastoma immune microenvironment: Can we distinguish reality
from illusion? Neuro Oncol. 26:840–842. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Kluckova K, Kozak J, Szaboova K, Rychly B,
Svajdler M, Suchankova M, Tibenska E, Filova B, Steno J, Matejcik
V, et al: TREM-1 and TREM-2 expression on blood monocytes could
help predict survival in high-grade glioma patients. Mediators
Inflamm. 2020:17981472020. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Kluckova K, Kozak J, Szaboova K,
Suchankova M, Svajdler M, Blazickova S, Makohusova M, Steno J,
Matejcik V and Bucova M: Low serum vitamin D levels are associated
with a low percentage of TREM-2+ monocytes in low-grade gliomas and
poorer overall survival in patients with high-grade gliomas.
Bratisl Lek Listy. 122:172–178. 2021.PubMed/NCBI
|
|
64
|
Ohrfelt A, Axelsson M, Malmestrom C,
Novakova L, Heslegrave A, Blennow K, Lycke J and Zetterberg H:
Soluble TREM-2 in cerebrospinal fluid from patients with multiple
sclerosis treated with natalizumab or mitoxantrone. Mult Scler.
22:1587–1595. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Qin C, Chen M, Dong MH, Yang S, Zhang H,
You YF, Zhou LQ, Chu YH, Tang Y, Pang XW, et al: Soluble TREM2
triggers microglial dysfunction in neuromyelitis optica spectrum
disorders. Brain. 147:163–176. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Greutter L, Miller-Michlits Y, Klotz S,
Reimann R, Nenning KH, Platzek S, Krause E, Kiesel B, Widhalm G,
Langs G, et al: Frequent Alzheimer's disease neuropathological
change in patients with glioblastoma. Neurooncol Adv.
6:vdae1182024.PubMed/NCBI
|
|
67
|
Zhong L, Chen XF, Wang T, Wang Z, Liao C,
Wang Z, Huang R, Wang D, Li X, Wu L, et al: Soluble TREM2 induces
inflammatory responses and enhances microglial survival. J Exp Med.
214:597–607. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Zhang L, Xiang X, Li Y, Bu G and Chen XF:
TREM2 and sTREM2 in Alzheimer's disease: From mechanisms to
therapies. Mol Neurodegener. 20:432025. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Zheng H, Jia L, Liu CC, Rong Z, Zhong L,
Yang L, Chen XF, Fryer JD, Wang X, Zhang YW, et al: TREM2 promotes
microglial survival by activating Wnt/β-catenin pathway. J
Neurosci. 37:1772–1784. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Ma YN, Hu X, Karako K, Song P, Tang W and
Xia Y: The potential and challenges of TREM2-targeted therapy in
Alzheimer's disease: Insights from the INVOKE-2 study. Front Aging
Neurosci. 17:15760202025. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Li H, Xu D, Cai W, Liu J, Bing Z and Zhang
Q: PEGylated nanoliposomal doxorubicin conjugated with specific
TREM2 peptides for glioma-targeting therapy. Adv Healthc Mater.
14:e24030962025. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Sigalov AB: Inhibition of TREM-2 markedly
suppresses joint inflammation and damage in experimental arthritis.
Int J Mol Sci. 23:88572022. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Gallop D, Scanlon KM, Ardanuy J, Sigalov
AB, Carbonetti NH and Skerry C: Triggering receptor expressed on
myeloid cells-1 (TREM-1) contributes to bordetella pertussis
inflammatory pathology. Infect Immun. 89:e00126212021. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Zhou F, Mukherjee P, Mu J and Chen P:
Therapeutic potential of targeting macrophages and microglia in
glioblastoma. Trends Pharmacol Sci. 46:848–862. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Harwood DSL, Artzi SB, Pedersen V, Locallo
A, Lü MJS, Scheie D, Nørøxe DS, Hammouda NM, Lassen U,
Weischenfeldt J and Kristensen BW: Genomic heterogeneity drives
distinct infiltration patterns in glioblastoma. Acta Neuropathol
Commun. 14:52025. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Lemoine C, Da Veiga MA, Rogister B, Piette
C and Neirinckx V: An integrated perspective on single-cell and
spatial transcriptomic signatures in high-grade gliomas. NPJ Precis
Oncol. 9:442025. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Kim J, Zhu Y, Chen S, Wang D, Zhang S, Xia
J, Li S, Qiu Q, Lee H and Wang J: Anti-glioma effect of
ginseng-derived exosomes-like nanoparticles by active
blood-brain-barrier penetration and tumor microenvironment
modulation. J Nanobiotechnology. 21:2532023. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Wang C, Feng W, Li J, Wang J, Liu L, Ye
SH, Zhang Y, Fu J, Zheng H, Chen E, et al: Enhanced nano-vaccine
utilizing biomineralized virus-like particles for efficient
glioblastoma immunotherapy via the nose-to-brain delivery pathway.
ACS Nano. 19:21154–21168. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Kuang L, Han M, Wu X, Deng Z, Liu T, Yin
Y, Tang Y, Dong Z, Hu X, Zhu S, et al: Starting the engine and
releasing the brakes of T-cell responses: A biomimetic dendritic
cell nanoplatform for improved glioblastoma immunotherapy. ACS
Nano. 19:21365–21384. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
von Locquenghien M, Zwicky P, Xie K,
Jaitin DA, Sheban F, Yalin A, Uhlitz F, Gur C, Eshed RS, David E,
et al: Macrophage-targeted immunocytokine leverages myeloid, T, and
NK cell synergy for cancer immunotherapy. Cell. 188:7099–7117.e26.
2025. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Lago C, Gianesello M, Santomaso L, Leva G,
Ballabio C, Anderle M, Antonica F and Tiberi L: Medulloblastoma and
high-grade glioma organoids for drug screening, lineage tracing,
co-culture and in vivo assay. Nat Protoc. 18:2143–2180. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Pasupuleti V, Vora L, Prasad R, Nandakumar
DN and Khatri DK: Glioblastoma preclinical models: Strengths and
weaknesses. Biochim Biophys Acta Rev Cancer. 1879:1890592024.
View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Correia CD, Calado SM, Matos A, Esteves F,
De Sousa-Coelho AL, Campinho MA and Fernandes MT: Advancing
glioblastoma research with innovative brain organoid-based models.
Cells. 14:2922025. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Wen J, Liu F, Cheng Q, Weygant N, Liang X,
Fan F, Li C, Zhang L and Liu Z: Applications of organoid technology
to brain tumors. CNS Neurosci Ther. 29:2725–2743. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Zheng C, Wang P, Zhang D, Fang Z, Feng Y,
Chen J, Chen J, Fu Y, Yang B, Yu S, et al: A novel organoid model
retaining the glioma microenvironment for personalized drug
screening and therapeutic evaluation. Bioact Mater. 53:205–217.
2025.PubMed/NCBI
|
|
86
|
Schupper AJ and Hadjipanayis CG: Novel
approaches to targeting gliomas at the leading/cutting edge. J
Neurosurg. 139:760–768. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Gampa G, Vadlakonda R, Stefanich E, Kamath
AV, Sadekar S and Shivva V: Bridging the blood-brain barrier:
Strategies to improve delivery of biologics to tumors in the brain.
Fluids Barriers CNS. 23:252026. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Wang N, Qing Q, Xue Y, Cai S, Zheng M,
Zhang D and Ismail M: Enhancing lipid nanoparticles-mediated RNA
delivery to glioblastoma via targeted strategies. J Control
Release. 389:1144722026. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Arjmand B, Mojavezi AR, Kamroo A, Yazdi
RK, Rezaei-Tavirani M and Vahedi MS: Advances in intranasal
delivery of exosomes for central nervous system disorders. Mol
Neurobiol. 63:1932025. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Pai B, Ramos SI, Cheng WS, Joshi T, Özen
E, Kulumani Mahadevan LS, Silva-Hurtado TJ, Price GA, Tome-Garcia
J, Nudelman G, et al: Spatial multiomics defines a shared tumor
infiltrative signature at the resection margin in high-grade
gliomas. Cancer Res. 85:4233–4250. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Fan H, Luo Y, Gu F, Tian B, Xiong Y, Wu G,
Nie X, Yu J, Tong J and Liao X: Artificial intelligence-based MRI
radiomics and radiogenomics in glioma. Cancer Imaging. 24:362024.
View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Luo J, Pan M, Mo K, Mao Y and Zou D:
Emerging role of artificial intelligence in diagnosis,
classification and clinical management of glioma. Semin Cancer
Biol. 91:110–123. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Wang YRJ, Wang P, Yan Z, Zhou Q, Gunturkun
F, Li P, Hu Y, Wu WE, Zhao K, Zhang M, et al: Advancing presurgical
non-invasive molecular subgroup prediction in medulloblastoma using
artificial intelligence and MRI signatures. Cancer Cell.
42:1239–1257.e7. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Morello G, La Cognata V, Guarnaccia M,
Gentile G and Cavallaro S: Artificial intelligence-driven
multi-omics approaches in glioblastoma. Int J Mol Sci. 26:93622025.
View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Lin B, Tan Z, Mo Y, Yang X, Liu Y and Xu
B: Intelligent oncology: The convergence of artificial intelligence
and oncology. J Natl Cancer Cent. 3:83–91. 2022.PubMed/NCBI
|
|
96
|
Li H, Nithin C, Kmiecik S and Huang SY:
Computational methods for modeling protein-protein interactions in
the AI era: Current status and future directions. Drug Discov
Today. 30:1043822025. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Sarvepalli S and Vadarevu S: Role of
artificial intelligence in cancer drug discovery and development.
Cancer Lett. 627:2178212025. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Zhang K, Yang X, Wang Y, Yu Y, Huang N, Li
G, Li X, Wu JC and Yang S: Artificial intelligence in drug
development. Nat Med. 31:45–59. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Ocana A, Pandiella A, Privat C, Bravo I,
Luengo-Oroz M, Amir E and Gyorffy B: Integrating artificial
intelligence in drug discovery and early drug development: A
transformative approach. Biomark Res. 13:452025. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Vecchietti LF, Wijaya BN, Armanuly A,
Hangeldiyev B, Jung H, Lee S, Cha M and Kim HM: Artificial
intelligence-driven computational methods for antibody design and
optimization. MAbs. 17:25289022025. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Wang Z, Zhang RY, Ji C, Zhang JY, Yue BT
and Wang F: Revolutionizing gastrointestinal cancer research with
artificial intelligence: From precision patient stratification to
real-world evidence. World J Gastrointest Oncol. 17:1113392025.
View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Jin D, Shmatko A, Patel A, Rutz S,
Friedrich L, Banan R, Rahmanzade R, Sievers P, Hamelmann S,
Schrimpf D, et al: Hetairos is a histology-based artificial
intelligence model for predicting central nervous system tumor
methylation subtypes. Nat Cancer. Jun 10–2026.(Epub ahead of
print). View Article : Google Scholar
|
|
103
|
Zapaishchykova A, Zielke J, Tak D, Climent
Pardo JC, Mojahed-Yazdi R, Soto-Rivera CL, Liu KX, Saraf A, Ye Z,
Wang W, et al: Artificial intelligence analysis of temporalis
muscle thickness for monitoring sarcopenia and clinical outcomes in
individuals with paediatric brain tumours: A retrospective cohort
study. Lancet Digit Health. 1009732026.(Epub ahead of print).
View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Ning Y, Teixayavong S, Shang Y, Savulescu
J, Nagaraj V, Miao D, Mertens M, Ting DSW, Ong JCL, Liu M, et al:
Generative artificial intelligence and ethical considerations in
health care: A scoping review and ethics checklist. Lancet Digit
Health. 6:e848–e856. 2024. View Article : Google Scholar : PubMed/NCBI
|