Introduction
Lung cancer is a leading cause of cancer-related
mortality worldwide and is expected to remain a major public health
problem for the foreseeable future. Numerous phase III studies have
been conducted aiming at validating therapeutic impact on patient
survival among patients with advanced non-small cell lung cancer
(NSCLC) (?).
The heart is a sophisticated endocrine gland that
synthesizes a family of peptide hormones using three genes. These
cardiac hormones are stored as three prohormones: atrial
natriuretic peptide (ANP), brain natriuretic peptide (BNP) and
C-type natriuretic peptide (1–4). The
ANP prohormones comprise four peptide hormones: ANP, vessel
dilator, kaliuretic peptide and long-acting natriuretic peptide.
These peptides decrease up to 97% of human pancreatic, breast,
colon, prostate, kidney and ovarian carcinomas as well as
small-cell and squamous cell lung cancer cells within 24 h in cell
culture (5). In vivo the
four cardiac hormones eliminate up to 80% of human pancreatic
adenocarcinomas, 66% of human breast cancers and up to 86% of human
small-cell lung cancers in athymic mice. The anticancer mechanisms
of these hormones target the Ras-MEK 1/2-ERK 1/2 kinase cascade in
cancer cells. The four cardiac hormones also inhibit up to 95% of
the basal activity of Ras, 98% of the phosphorylation of MEK 1/2
and 97% of the basal activity of ERK 1/2. They also block the
activity of mitogens, such as the ability of epidermal growth
factor to stimulate ERK (5).
ANP and BNP plasma concentrations were elevated in
patients with congestive heart failure (6,7). The
level of BNP was shown to be sufficiently accurate for diagnosing,
monitoring and predicting prognosis in those patients (8). Of the six hormones, BNP had no
antitumor effect against various tumor cell lines, including
pancreatic, breast and small cell lung cancer (9,10).
However, to the best of our knowledge, no reports exist on the
prognostic effect of these peptide hormones or the relationship
between clinicopathological factors and plasma levels in advanced
NSCLC patients who are anticipated to have a high cardiac
burden.
In this study, the concentration of plasma BNP
levels in NSCLC patients was measured and the relationship between
these levels and clinicopathological factors was investigated.
Patients and methods
Patients and methods
A total of 133 patients admitted to Kyoto University
Hospital with advanced NSCLC between September 2007 and May 2009
were included in this study. Plasma samples were collected from all
133 patients.
The level of BNP was determined at the time of
diagnosis. Venous blood (4 ml) was obtained from each patient and
transferred to tubes containing aprotinin and
ethylene-diamine-tetra-acetic acid, and stored at −20°C until the
measurements were taken. Plasma concentration of BNP was measured
using a chemiluminescent enzyme immunoassay kit (MI02 Shionogi BNP;
Shionogi Co. Ltd., Osaka, Japan) and an immunoassay system (MI02;
A&T Co. Ltd., Yokohama, Japan). The minimum quantity of a human
BNP detectable using this system is 4 pg/ml.
Statistical analysis
The univariate relationship between each independent
clinicopathological variable and plasma BNP was examined using the
Chi-square test. The survival curves were determined using the
Kaplan-Meier method. The log-rank test was used to evaluate the
differences between the survival curves. The data were analysed
using JMP 6 software (SAS Institute, Cary, NC, USA).
Results
Patient characteristics
Table I shows the
characteristics of the 133 advanced NSCLC patients who were
admitted to our institution between June 2007 and May 2009. The
patients were Japanese, and included 95 (71.4%) males and 38
(28.6%) females, with a median age of 61 years (range 34–88). The
pathological diagnoses are listed in Table I and the number of dominant
adenocarcinomas was 85 (63.9%). A total of 44 (33.1%) patients were
non-smokers and 89 (66.9%) patients were former or current smokers.
The Eastern Cooperative Oncology Group performance status was 0–1
for 104 patients and 2–3 for 29 patients. Of the 133 patients, 62
(46.6%) had been treated with platinum doublets, 30 (22.6%) with
cytotoxic agent monotherapy, 7 (5.3%) with epidermal growth factor
receptor tyrosine kinase inhibitors as the first-line regimen, 5
(3.8%) with chemo-radiotherapy, 3 (2.2%) with thoracic radiotherapy
and 26 (19.5%) with best supportive care.
 | Table IPatient characteristics and treatment
(n=133). |
Table I
Patient characteristics and treatment
(n=133).
| Characteristics | n (%) |
|---|
| Age (years) |
| Range | 34–88 |
| Median | 61 |
| Gender |
| Female | 38 (28.6) |
| Male | 95 (71.4) |
| Smoking status |
| Non-smoker | 44 (33.1) |
| Smoker | 89 (66.9) |
| Former | 46 (34.6) |
| Current | 43 (32.3) |
| Performance
status |
| 0–1 | 104 (78.2) |
| >2 | 29 (21.8) |
| Tumor histology |
| Adenocarcinoma | 85 (63.9) |
| Squamous cell
carcinoma | 24 (18.0) |
| NSCLC | 22 (16.5) |
| Large | 2 (0.6) |
| Pathological
stage |
| IIIB | 55 (41.4) |
| IV | 78 (58.6) |
| Therapy |
| Platinum
doublet | 62 (46.6) |
| Cytotoxic agent
monotherapy | 30 (22.6) |
| EGFR TKIs | 7 (5.3) |
|
Chemo-radiotherapy | 5 (3.8) |
| Radiation | 3 (2.2) |
| Best supportive
care | 26 (19.5) |
Plasma brain natriuretic peptide
The mean and median concentration of plasma BNP was
11.5 and 22.4 pg/ml, respectively. A statistical comparison of the
plasma BNP in our study population showed significantly lower
levels in patients with metastasis compared to those without
metastasis (two-tailed t=1.969, df=9.177, p=0.05, Fig. 1). According to the cut-off level of
plasma BNP (11.5 and 22.4 pg/ml), plasma BNP negativity correlates
with the presence of metastases (Table
II-A and B) (Chi-square test, p=0.0374 and p=0.0098,
respectively).
| Table IICorrelation between metastases and
serum BNP according to the cut-off BNP levels. |
Table II
Correlation between metastases and
serum BNP according to the cut-off BNP levels.
| A, 11.5 pg/ml |
|---|
|
|---|
| No. of cases | Metastases |
|---|
| |
|
|---|
| | Positive | Negative |
|---|
| Negative (<11.5
pg/ml) | 34 | 25 | 9 |
| Positive (>11.5
pg/ml) | 99 | 53 | 46 |
| Total | 133 | 78 | 55 |
| B, 22.4 pg/ml |
|---|
|
|---|
| No. of cases | Metastases |
|---|
| |
|
|---|
| | Positive | Negative |
|---|
| Negative (<22.4
pg/ml) | 66 | 46 | 20 |
| Positive (>22.4
pg/ml) | 67 | 32 | 35 |
| Total | 133 | 78 | 55 |
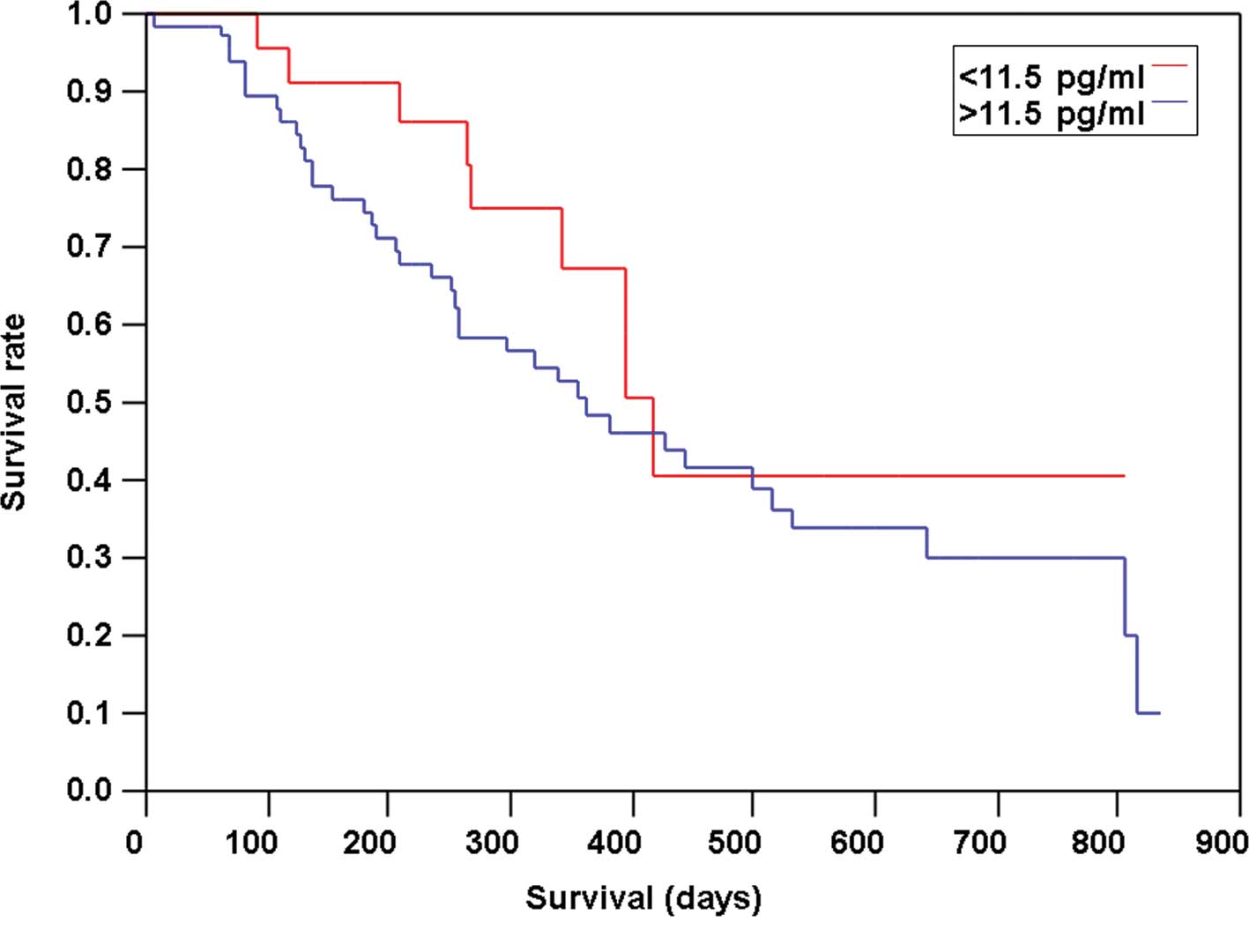
Plasma brain natriuretic peptide and
survivals
Positive or negative plasma BNP was determined by
the cut-off values of 11.5 and 22.4 pg/ml, which are the 25 and 50%
percentiles, respectively. No significant association between
patient survival time and plasma BNP level was noted (Figs. 2 and 3).
Discussion
In this study, reduced plasma BNP levels were noted
in advanced NSCLC patients with metastases. We also found that
plasma BNP levels did not affect the survival of patients with or
without chemotherapy.
The most recently-discovered property of the cardiac
natriuretic peptides is their ability to inhibit the growth of
cancers in vitro and in vivo (9–13). In
any cancer cell line that has been examined in vitro
(9–11,13)
and in vivo (12), including
that of human pancreatic adenocarcinoma cells, human breast
adenocarcinoma, human squamous cell lung cancer and human small
lung cancer cells, vessel dilator has had the strongest anticancer
effects, whereas BNP had no effect on the cancer cells. However, in
our study, the plasma BNP level was significantly lower in patients
with metastasis, indicating that BNP decreases distant metastases
in patients with NSCLC.
We hypothesized that plasma BNP inhibits the
profibrotic action of tumor growth factor-β (TGF-β) (14), thereby decreasing distant
metastases. TGF-β promotes an epithelial to mesenchymal transition
that is associated with increased tumor cell motility, invasion and
metastasis (15,16).
Moreover, BNP promotes vessel growth by increasing
the number of endothelial progenitors and enhancing their
functional properties (17). The
provasculogenic properties of BNP may account for certain
beneficial effects in NSCLC patients in terms of normal
vasculogenesis in the tumor bed which differs from plasma vascular
endothelial growth factor (VEGF). Subsequently, the association
between plasma BNP and VEGF in vivo should be
investigated.
No prognostic significance of plasma BNP was found
whether or not chemotherapy was administered. The level of BNP has
been shown to be sufficiently accurate to predict prognosis in
those patients (7). To the best of
our knowledge, no reports exist regarding the relationship between
prognosis and the levels of cardiac peptide hormones, including
BNP, although advanced NSCLC patients anticipate to have a high
cardiac burden. The reason is that in many cohorts dealing with
advanced NSCLC patients, clinical stage is not always considered to
be a prognostic factor.
The limitations of our study include the small
sample size, the heterogeneity of the treatment regimens and its
retrospective nature. However, we showed reduced plasma BNP levels
in advanced NSCLC patients with metastases, suggesting that BNP
decreases the distant metastases of advanced NSCLC patients. In
conclusion, whether BNP is a potential therapeutic option for
inhibiting distant metastases of advanced NSCLC patients remains to
be determined.
References
|
1
|
Gardner DG, Chen S, Glenn DJ and Grigsby
CL: Molecular biology of the natriuretic peptide system:
implications for physiology and hypertension. Hypertension.
49:419–426. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Gardner DG, Kovacic-Milivojevic BK and
Garmai M: Atrial natriuretic peptides. Molecular Biology of the
Natriuretic Peptides. Vesely DL: Research Signpost; Trivandrum: pp.
15–38. 1977
|
|
3
|
Vesely DL: Atrial natriuretic peptide
prohormone gene expression: hormones and diseases that upregulate
its expression. IUBMB Life. 53:153–159. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Vesely DL: Natriuretic hormones. The
Kidney: Physiology and Pathophysiology. 4th edition. Alpern RJ:
Elsevier/Academic Press; San Diego, CA: 2006
|
|
5
|
Vesely DL: Metabolic targets of cardiac
hormones' therapeutic anti-cancer effects. Curr Pharm Des.
16:1159–1166. 2010. View Article : Google Scholar
|
|
6
|
Burnett JC Jr, Kao PC, Hu DC, et al:
Atrial natriuretic peptide elevation in congestive heart failure in
the human. Science. 231:1145–1147. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yoshimura M, Yasue H, Okumura K, et al:
Different secretion patterns of atrial natriuretic peptide and
brain natriuretic peptide in patients with congestive heart
failure. Circulation. 87:464–469. 1993. View Article : Google Scholar
|
|
8
|
Cowie MR, Struthers AD, Wood DA, et al:
Value of natriuretic peptides in assessment of patients with
possible new heart failure in primary care. Lancet. 350:1349–1353.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Vesely BA, Song S, Sanchez-Ramos J, et al:
Five cardiac hormones decrease the number of human small-cell lung
cancer cells. Eur J Clin Invest. 35:388–398. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Vesely BA, Song S, Sanchez-Ramos J, et al:
Four peptide hormones decrease the number of human breast
adenocarcinoma cells. Eur J Clin Invest. 35:60–69. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Vesely BA, McAfee Q, Gower WR Jr and
Vesely DL: Four peptides decrease the number of human pancreatic
adenocarcinoma cells. Eur J Clin Invest. 33:998–1005. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Vesely DL, Clark LC, Garces AH, McAfee QW,
Soto J and Gower WR Jr: Novel therapeutic approach for cancer using
four cardiovascular hormones. Eur J Clin Invest. 34:674–682. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Vesely BA, Fitz SR, Gower WR Jr and Vesely
DL: Vessel dilator: most potent of the atrial natriuretic peptides
in decreasing the number and DNA synthesis of human squamous lung
cancer cells. Cancer Lett. 233:226–231. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kapoun AM, Liang F, O'Young G, et al:
B-type natriuretic peptide exerts broad functional opposition to
transforming growth factor-beta in primary human cardiac
fibroblasts: fibrosis, myofibroblast conversion, proliferation, and
inflammation. Circ Res. 94:453–461. 2004. View Article : Google Scholar
|
|
15
|
Bierie B and Moses HL: Transforming growth
factor beta (TGF-beta) and inflammation in cancer. Cytokine Growth
Factor Rev. 21:49–59. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tian M and Schiemann WP: The TGF-beta
paradox in human cancer: an update. Future Oncol. 5:259–271. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Shmilovich H, Ben-Shoshan J, Tal R, et al:
B-type natriuretic peptide enhances vasculogenesis by promoting
number and functional properties of early endothelial progenitor
cells. Tissue Eng Part A. 15:2741–2749. 2009. View Article : Google Scholar : PubMed/NCBI
|