Introduction
Gastric cancer is one of the most common
malignancies worldwide and remains a leading cause of death in Asia
(1). The association between
gastric cancer and chronic inflammation has generally been
recognized, and chronic Helicobacter pylori (H. pylori)
infection has been found to be a significant risk factor for
gastric cancer (2,3). Only a small proportion of chronic
H. pylori-infected individuals develop malignancies
(2), suggesting that other factors,
particularly host genetic factors, modulate the effects of
inflammation in carcinogenesis.
The transforming growth factor-β (TGFβ) pathway
plays an important role in inflammatory responses in the tumor
microenvironment (4). TGFβ uniquely
promotes the differentiation of human naive CD4+ T cells
into TH17 cells, thereby becoming involved in the modulation of
complicated inflammation pathways (5,6). As a
multifunctional cytokine, TGFβ1 regulates a number of important
cellular responses, in addition to its role in cell
differentiation, including apoptosis, cell migration, immune
responses and angiogenesis. TGFβ1 initiates downstream signaling
events by binding to the transforming growth factor β receptor 2
(TGFβR2), a constitutively active kinase which activates type 1
receptors by the phosphorylation of serine and threonine residues
in the GS box and downstream signaling (7).
TGFB1 -509C/T (rs1800469) and TGFBR2
-875A/G polymorphisms (rs3087465) have been reported to be
associated with gastric cancer risk (8–10).
However, the results of studies from different geographical
regions, ethnic groups and study groups are controversial (8–12). For
example, certain studies found that carriers of TGFB1 -509T
were associated with a decreased (8) or increased risk of gastric cancer
(9). On the other hand, other
studies have reported that the TGFB1 -509 C/T polymorphism
has no association with the risk of gastric cancer or patient
survival (11,12). The limitations of these studies
should be considered when interpreting their findings. The majority
of studies dismissed potential confounding factors such as age,
gender, H. pylori status, tumor location and histological
subtype, which may result in the bias and inaccuracy of results. In
addition, it is known that TGFB1 and TGFBR2 map to
different chromosomes, i.e., 19q13.2 and 3p24.1, respectively,
indicating that TGFB1 and TGFBR2 are independently
inherited. Subsequently, variants of TGFB1 -509C/T and
TGFBR2 -875A/G exhibit a potential interaction with respect
to gastric cancer risk.
This study aimed to investigate whether the
TGFB1 -509C/T and TGFBR2 -875A/G polymorphisms are
correlated to the susceptibility of gastric cancer with respect to
clinical and pathologic parameters. The combination of the
genotypes of TGFB1 -509 and TGFBR2 -875 was also
evaluated for their association with the risk of gastric
cancer.
Materials and methods
Subjects
A population-based case-control study was conducted
between 1999 and 2006 in Guangdong Province, China. The case series
included 1,010 Chinese gastric cancer patients, newly diagnosed at
the First Affiliated Hospital and Cancer Center of Sun Yat-Sen
University, Guangzhou, China, from January 1999 to December 2006.
The control series included 1,500 Cantonese healthy subjects from
the general population of Guangzhou in southern China. Diagnosis
was confirmed histologically as gastric cancer. The median duration
of follow-up was 14 months (ranging from 0 to 98 months). Clinical
data of the patients were collected from medical records and
structured interviews were conducted using questionnaires. Patients
diagnosed with gastric cancer received surgical resection of the
tumors. Patients and control subjects provided written informed
consent for participation in this study, and the study protocol was
approved by the Clinical Research Ethics Committee of the Sun
Yat-Sen University of Medical Sciences.
DNA extraction
Genomic DNA was extracted from paraffin-embedded
tissues of 1,010 gastric cancer patients using QIAamp DNA Mini kit
(Qiagen, Hilden, Germany). Of these patients, 963 were included as
the case group due to good DNA quality. Genomic DNA was also
extracted from 2 ml of peripheral blood of 1,500 healthy subjects
using the Gentra Puregene Blood kit (Gentra Systems, Minneapolis,
MN, USA). Of these, 787 subjects were selected as healthy controls
frequency matched to the case group by age and gender. There were
655 males (68%) and 308 females (32%) in the gastric cancer case
group, whereas the control group included 512 males (65%) and 275
females (35%). Frequency matching by age and gender was not
complete, and thus these factors were further regulated in the
multivariate data analysis stage. Extracted DNA was resuspended in
UltraPure RNAse/DNAse-free distilled water (Invitrogen, Hong Kong,
China).
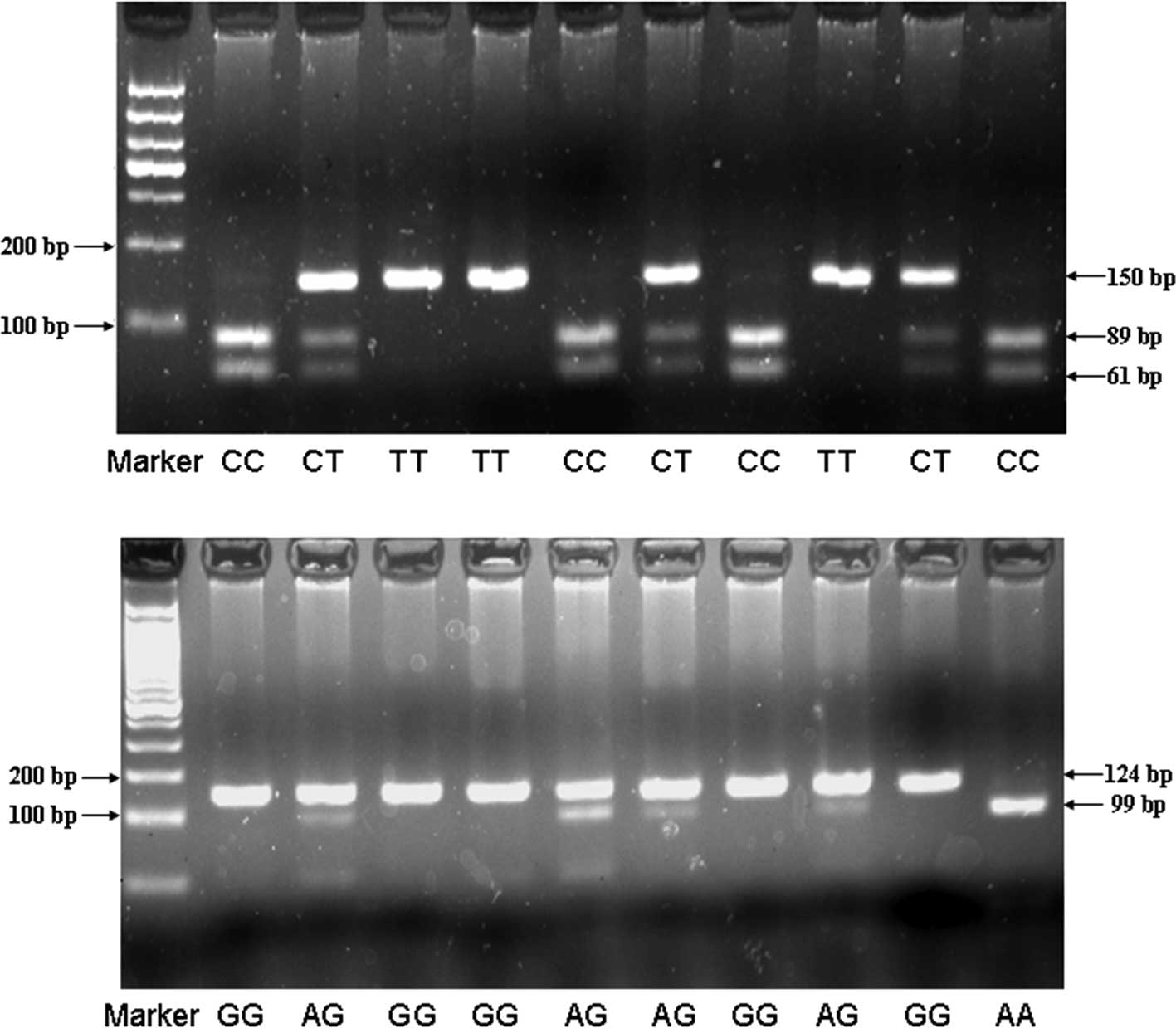
Genotyping analysis
TGFB1 -509C/T and TGFBR2 -875A/G
genotyping was performed by polymerase chain reaction-restriction
fragment length polymorphism (PCR-RFLP). Primer sequences for
TGFB1 -509C/T and TGFBR2 -875A/G were: sense
5′-GAGACGCCTTGAAGTAACTG-3′ and anti-sense
5′-AACCAAAGATGTTCTGAACTGA-3′ for TGFB1 -509C/T; and sense
5′-GCAAGAAAGGAAATTTGAAAGTT TGT-3′ and anti-sense
5′-TCACCTGAATGCTTGTGTTTT-3′ for TGFBR2 -875A/G. PCR was
performed under the conditions: denaturation at 94°C for 10 min,
followed by 94°C (30 sec), 65°C (30 sec), and 72°C (30 sec) for 38
cycles, followed by a final extension at 72°C for 7 min. PCR
products were digested overnight at 37°C with Bsu36I (New
England BioLabs, Ipswich, MA, USA) for TGFB1 -509C/T and
RsaI (New England BioLabs) for TGFBR2 -875A/G
genotypes, and then separated by electrophoresis on 3% agarose gel
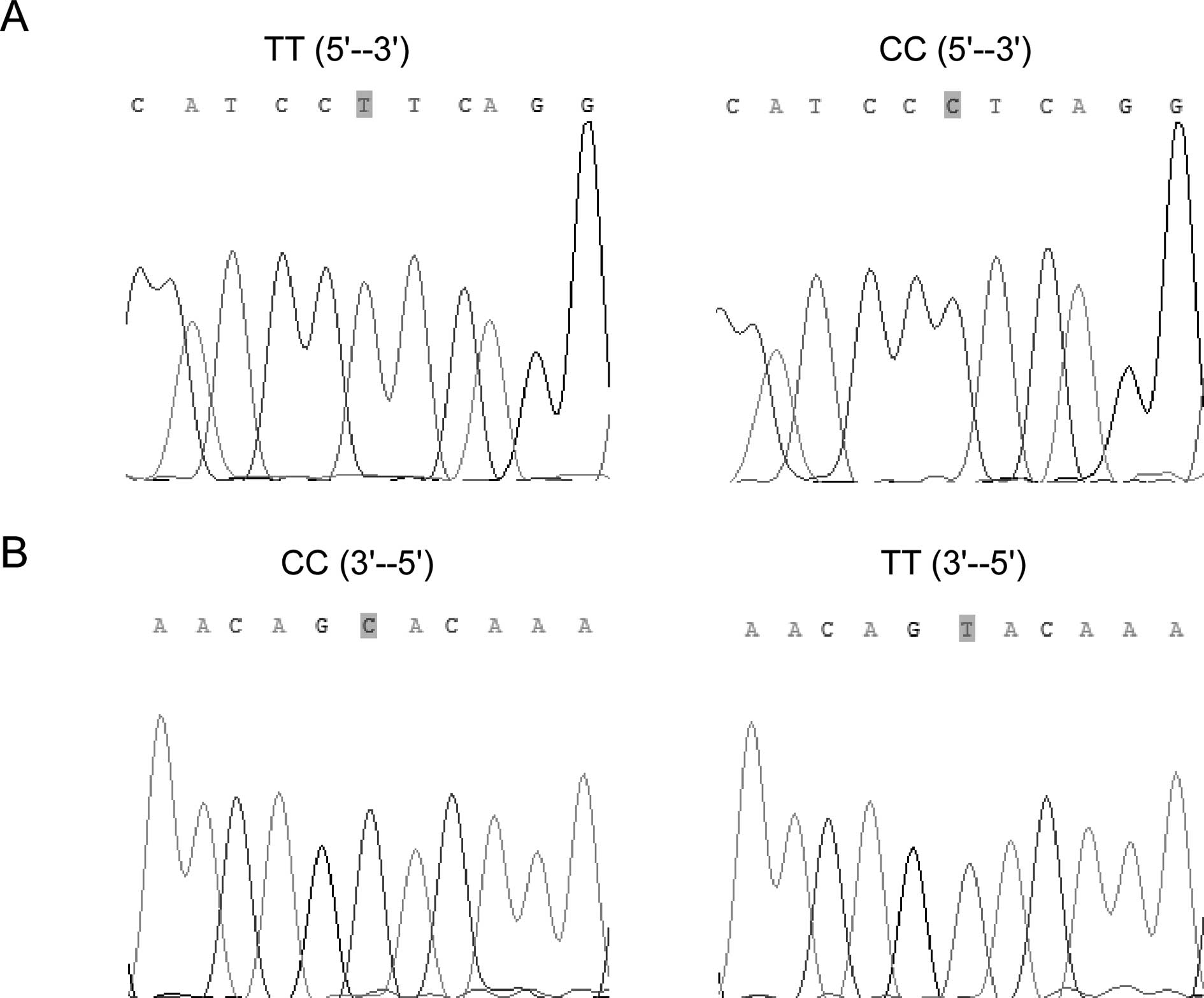
with ethidium bromide staining. PCR products were shown to be
digested into 3 types of fragments (Fig. 1). To confirm the genotyping results,
randomly selected PCR samples were examined by DNA sequencing
(Fig. 2).
Statistical analysis
Hardy-Weinberg equilibrium in the controls was
assessed using the χ2 test. The effects of the genotypes
on the risk of gastric cancer were represented as odds ratios (OR)
with 95% confidence interval (CI) by logistic regression.
Relationships between the two polymorphisms and clinicopathological
characteristics of the gastric cancer patients were compared using
contingency tables and the Pearson’s χ2 test. Since
frequency matching was not complete, age and gender were included
in all of the multiple logistic regression models. Kaplan-Meier
survival curves and the log-rank test for trend were used to
evaluate the relationship between the two polymorphisms and the
prognosis from the date of primary diagnosis to the end of
follow-up. The multivariate Cox regression analysis was performed
to assess the prognostic value of the two polymorphisms with
adjustment for age, gender, tumor size, grade, lymph node status
and distant metastasis. Hazard ratios (HR) and 95% confidence
interval (CI) for each factor in the multivariate analysis were
calculated from the Cox regression model. Differences were regarded
as significant at P<0.05. The above statistical analyses were
performed using SPSS 13.0 software package (SPSS Inc, Chicago, IL,
USA).
Results
Association of TGFB1 -509C/T and TGFBR2
-875A/G polymorphisms with gastric cancer susceptibility
Among the controls, the genotype distribution for
each SNP was in Hardy-Weinberg equilibrium (P>0.05). The
frequencies of the polymorphisms in the cases and controls are
shown in Table I. Compared with the
TGFB1 -509 TT genotype, the CC and CT genotypes
significantly decreased gastric cancer risk with odds ratios (ORs)
of 0.70 (95% CI, 0.53–0.94) and 0.72 (95% CI, 0.58–0.89),
respectively. Overall, the C carriers (CT or CC) were also
associated with a lower gastric cancer risk when compared with the
TT carriers (OR, 0.71; 95% CI, 0.58–0.87; P=0.001). Analysis of the
TGFBR2 -875A/G genotype polymorphisms showed a significant
difference between the gastric cancer patients and controls
(P<0.001). The AG genotype was associated with a lower gastric
cancer risk when compared with the GG genotype (OR, 0.56; 95% CI,
0.45–0.70; P<0.001) (Table
I).
 | Table IAdjusted odds ratios (ORs) and 95%
confidence intervals (CIs) for gastric cancer in relation to the
TGFB1 -509C/T and TGFBR2 -875A/G genotypes. |
Table I
Adjusted odds ratios (ORs) and 95%
confidence intervals (CIs) for gastric cancer in relation to the
TGFB1 -509C/T and TGFBR2 -875A/G genotypes.
| Genotype | Control (%) | Cases (%) | ORa (95% CI) | P-value |
|---|
| TGFB1
-509C/T |
| CT/CC | 536 (69) | 578 (61) | 0.71
(0.58–0.87) | 0.001 |
| CC | 133 (17) | 142 (15) | 0.70
(0.53–0.94) | 0.016 |
| CT | 403 (52) | 436 (46) | 0.72
(0.58–0.89) | 0.002 |
| TT | 245 (31) | 367 (39) | 1 | |
| TGFBR2
-875A/G |
| AG/AA | 305 (39) | 261 (27) | 0.58
(0.62–0.91) | <0.001 |
| AA | 38 (5) | 39 (4) | 0.69
(0.43–1.09) | 0.114 |
| AG | 268 (34) | 222 (23) | 0.56
(0.45–0.70) | <0.001 |
| GG | 478 (61) | 702 (73) | 1 | |
Association of the TGFB1 -509C/T and
TGFBR2 -875A/G polymorphisms with clinicopathological
parameters
Stratified by the Lauren classification, the
presence of the TGFB1 -509 C allele genotypes (CC or CT) was
significantly associated with intestinal-type gastric cancer with
an OR of 0.70 (95% CI, 0.57–0.87; P=0.001), but not with diffuse-
or mixed-type gastric cancer, as compared with the TT genotype. In
contrast, the association between the TGFBR2 -875
polymorphism and gastric cancer was not modified by the Lauren
classification. Carriers of the AG genotype had a significantly
decreased risk of intestinal-, diffuse- and mixed-type gastric
cancer, compared to carriers of the GG genotype (Table II).
| Table IIAdjusted odds ratios (ORs) and 95%
confidence intervals (CIs) for gastric cancer, stratified by Lauren
classification, in relation to the TGFB1 -509C/T and
TGFBR2 -875A/G genotypes. |
Table II
Adjusted odds ratios (ORs) and 95%
confidence intervals (CIs) for gastric cancer, stratified by Lauren
classification, in relation to the TGFB1 -509C/T and
TGFBR2 -875A/G genotypes.
| | Intestinal | Diffuse | Mixed |
|---|
| |
|
|
|
|---|
| Genotype | Control | Case | ORa (95% CI) | P-value | Case | ORa (95% CI) | P-value | Case | ORa (95% CI) | P-value |
|---|
| TGFB1-509C/T |
| CT/CC | 536 | 448 | 0.70
(0.57–0.87) | 0.001 | 30 | 0.62
(0.35–1.09) | 0.099 | 90 | 0.78
(0.54–1.13) | 0.192 |
| CC | 133 | 106 | 0.66
(0.49–0.90) | 0.009 | 8 | 0.67
(0.29–1.56) | 0.353 | 26 | 0.89
(0.53–1.49) | 0.665 |
| CT | 403 | 342 | 0.72
(0.57–0.90) | 0.004 | 22 | 0.60
(0.32–1.11) | 0.104 | 64 | 0.74
(0.49–1.11) | 0.142 |
| TT | 245 | 285 | 1 | | 22 | 1 | | 54 | 1 | |
| TGFBR2 -875A/G |
| AG/AA | 305 | 203 | 0.58
(0.46–0.72) | <0.001 | 15 | 0.64
(0.34–1.19) | 0.158 | 36 | 0.53
(0.35–0.79) | 0.002 |
| AA | 38 | 26 | 0.59
(0.35–0.99) | 0.049 | 5 | 1.81
(0.67–4.93) | 0.244 | 6 | 0.61
(0.23–1.58) | 0.304 |
| AG | 267 | 177 | 0.57
(0.46–0.72) | <0.001 | 10 | 0.48
(0.24–0.99) | 0.047 | 30 | 0.51
(0.33–0.79) | 0.003 |
| GG | 478 | 552 | 1 | | 36 | 1 | | 105 | 1 | |
When the gastric cancers were stratified according
to tumor differentiation, the effect of the TGFB1 -509 CC
and CT genotypes remained significant on poorly differentiated
gastric cancer with ORs of 0.63 (95% CI, 0.45–0.88; P=0.006) and
0.69 (95% CI, 0.54–0.88; P=0.002), respectively, but not on
moderately or well-differentiated gastric cancer. However, the
association between the TGFBR2 -875 polymorphism and gastric
cancer was not modified by tumor differentiation. The TGFBR2
-875AG genotype was found to be associated with both poorly
differentiated and moderately or well-differentiated gastric cancer
(Table III).
| Table IIIAdjusted odds ratios (ORs) and 95%
confidence intervals (CIs) for gastric cancer, stratified by tumor
differentiation, in relation to the TGFB1 -509C/T and
TGFBR2 -875A/G genotypes. |
Table III
Adjusted odds ratios (ORs) and 95%
confidence intervals (CIs) for gastric cancer, stratified by tumor
differentiation, in relation to the TGFB1 -509C/T and
TGFBR2 -875A/G genotypes.
| | Poor | Moderate or
well-differentiated |
|---|
| |
|
|
|---|
| Genotype | Control | Cases | ORa (95% CI) | P-value | Cases | ORa (95% CI) | P-value |
|---|
| TGFB1 -509C/T |
| CT/CC | 536 | 335 | 0.67
(0.54–0.85) | 0.001 | 147 | 0.79
(0.58–1.09) | 0.156 |
| CC | 133 | 78 | 0.63
(0.45–0.88) | 0.006 | 40 | 0.86
(0.55–1.35) | 0.512 |
| CT | 403 | 257 | 0.69
(0.54–0.88) | 0.002 | 107 | 0.77
(0.55–1.08) | 0.133 |
| TT | 245 | 225 | 1 | | 83 | 1 | |
| TGFBR2 -875A/G |
| AG/AA | 305 | 167 | 0.63
(0.50–0.79) | <0.001 | 53 | 0.44
(0.31–0.63) | <0.001 |
| AA | 38 | 27 | 0.83
(0.49–1.38) | 0.470 | 5 | 0.36
(0.14–0.94) | 0.037 |
| AG | 267 | 140 | 0.61
(0.47–0.77) | <0.001 | 48 | 0.46
(0.32–0.65) | <0.001 |
| GG | 478 | 410 | 1 | | 180 | 1 | |
When the gastric cancer patients were divided into
two subgroups according to TNM stage, the TGFB1 -509 CT
genotype was found to be associated with TNM III/IV stage gastric
cancer with an OR of 0.71 (95% CI, 0.56–0.91; P=0.007), but not
with TNM I/II stage gastric cancer, when compared with the TT
genotype. In addition, the association between the TGFBR2
-875 polymorphism and gastric cancer was not modified by TNM stage.
The TGFBR2 -875AG genotype was associated with both TNM I/II
and TNM III/IV stage gastric cancer when compared to the GG
genotype (Table IV).
| Table IVAdjusted odds ratios (ORs) and 95%
confidence intervals (CIs) for gastric cancer, stratified by TNM
stage, in relation to the TGFB1 -509C/T and TGFBR2
-875A/G genotypes. |
Table IV
Adjusted odds ratios (ORs) and 95%
confidence intervals (CIs) for gastric cancer, stratified by TNM
stage, in relation to the TGFB1 -509C/T and TGFBR2
-875A/G genotypes.
| | TNM I+II | TNM III+IV |
|---|
| |
|
|
|---|
| Genotype | Control | Cases | ORa (95% CI) | P-value | Cases | ORa (95% CI) | P-value |
|---|
| TGFB1 -509C/T |
| CT/CC | 536 | 143 | 0.83
(0.61–1.15) | 0.260 | 339 | 0.73
(0.58–0.92) | 0.008 |
| CC | 133 | 30 | 0.70
(0.44–1.13) | 0.146 | 91 | 0.78
(0.56–1.08) | 0.138 |
| CT | 403 | 113 | 0.88
(0.63–1.22) | 0.436 | 248 | 0.71
(0.56–0.91) | 0.007 |
| TT | 245 | 77 | 1 | | 210 | 1 | |
| TGFBR2 -875A/G |
| AG/AA | 305 | 64 | 0.59
(0.43–0.82) | 0.002 | 141 | 0.54
(0.43–0.69) | <0.001 |
| AA | 38 | 7 | 0.53
(0.23–1.22) | 0.137 | 21 | 0.66
(0.38–1.14) | 0.134 |
| AG | 267 | 57 | 0.60
(0.43–0.84) | 0.003 | 120 | 0.53
(0.41–0.68) | <0.001 |
| GG | 478 | 61 | 1 | | 409 | 1 | |
Association of the TGFB1 -509C/T and
TGFBR2 -875A/G polymorphisms with the survival of gastric cancer
patients
Overall survival of the gastric cancer patients was
analyzed using Kaplan-Meier survival curves for dependence on the
TGFB1 -509C/T (P=0.859) and TGFBR2 -875A/G genotypes (P=0.652),
respectively. In the multivariate Cox regression analysis, the
survival of gastric cancer patients was significantly associated
with age (p=0.03), tumor staging (p=0.013), lymph node status
(P<0.001) and distant metastasis (P<0.001). However, the
TGFB1 -509C/T and TGFBR2 -875A/G genotypes were not
associated with outcome in gastric cancer patients (Table V).
| Table VThe Cox multivariate regression
analysis of potential factors for overall survival in the gastric
cancer patients. |
Table V
The Cox multivariate regression
analysis of potential factors for overall survival in the gastric
cancer patients.
| Variable | HR (95% CI) | P-value |
|---|
| Age | 1.02
(1.00–1.03) | 0.030 |
| Gender |
| Female | 1 | |
| Male | 1.12
(0.81–1.53) | 0.430 |
| Tumor staging |
| T1 | 1 | |
| T2 | 2.11
(0.40–10.16) | 0.350 |
| T3 | 4.26
(0.995–18.26) | 0.050 |
| T4 | 6.52
(1.49–28.50) | 0.013 |
| Lymph node |
| Negative | 1 | |
| Positive | 2.60
(1.59–4.26) | <0.001 |
| Metastasis |
| Negative | 1 | |
| Positive | 3.55
(2.50–5.02) | <0.001 |
| Lauren
classification |
| Intestinal | 1 | |
| Diffuse or
mixed | 1.14
(0.71–1.82) | 0.600 |
|
Differentiation |
| Poor | 1 | |
| Moderate or
well | 0.90
(0.62–1.31) | 0.590 |
| TGFB1
-509C/T |
| TT | 1 | |
| CT | 0.93
(0.67–1.23) | 0.630 |
| CC | 0.79
(0.47–1.31) | 0.360 |
| TGFBR2
-875A/G |
| GG | 1 | |
| AG | 0.88
(0.39–1.98) | 0.750 |
| AA | 0.87
(0.40–1.90) | 0.730 |
Combination of the TGFB1 -509C/T and
TGFBR2 -875A/G polymorphisms
We further investigated the effect of the
combination of the TGFB1 -509C/T and TGFBR2 -875A/G
genotypes. As shown in Table VI,
compared with the TGFB1 -509 TT and TGFBR2 -875 GG
genotypes, the combination of the TGFB1 -509CC/CT and
TGFBR2 -875AA/AG genotypes was significantly associated with
a decreased risk of gastric cancer (OR, 0.42; 95% CI, 0.32–0.57;
P<0.001) (Table VI).
| Table VICombined distribution of the
TGFB1 -509C/T and TGFBR2 -875A/G genotypes in the
controls and gastric cancer patients. |
Table VI
Combined distribution of the
TGFB1 -509C/T and TGFBR2 -875A/G genotypes in the
controls and gastric cancer patients.
| Genotypea | Control (%) | Cases (%) | ORb (95% CI) | P-value |
|---|
| 3 and 4 | 213 (57) | 158 (43) | 0.42
(0.32–0.57) | <0.001 |
| 1 and 2 | 153 (37) | 266 (63) | 1 | |
Overall survival of the gastric cancer patients was
analyzed using Kaplan-Meier survival curves. No statistical
difference was noted between the variant combination of the
TGFB1 -509 and TGFBR2 -875 genotypes (P=0.459). In
the multivariate Cox regression analysis, age, tumor size, tumor
grade, lymph node status and distant metastasis were significantly
associated with the survival of gastric cancer patients. However,
the combination of the TGFB1 -509 and TGFBR2 -875
genotypes was not associated with the outcome of the gastric cancer
patients (P=0.766) (data not shown).
Discussion
In the present study, we investigated the
relationship between polymorphisms of the TGFB1 and
TGFBR2 genes and the risk of gastric cancer in a low-risk
Chinese population. TGFB1 -509 C (heterozygote or
homozygote) and TGFBR2 AG genotypes were found to be
associated with a reduced risk of gastric cancer, and this risk was
particularly lower among subjects who carried the TGFB1 -509
C and TGFBR2 -875 A allele genotypes, suggesting that the
TGFB1 -509C/T and TGFBR2 -875A/G polymorphisms were
significant host protective biological factors that affected the
risk of gastric carcinogenesis in southern China.
Previous studies on the association of the
TGFB1 -509C/T polymorphism and gastric cancer are
controversial. Li et al found that carriers of TGFB1
-509T were more susceptible to gastric cancer in northern China
(9), which was consistent with our
results (Table I). Jin et al
reported that among a high-risk Chinese population in Nanjing,
carriers of TGFB1 -509 T or TGFBR2 -875 A had a
decreased risk of gastric cancer (8). On the other hand, no association was
found between the TGFB1 -509C/T polymorphism and gastric
cancer in a US population (12).
Allele frequency patterns of the TGFB1 -509C/T polymorphism
vary greatly between different geographical regions and ethnic
groups. For example, the frequencies of the -509 T allele among
healthy controls were 0.468, 0.461 and 0.212 in Nanjing, Shandong
and the US population, respectively (8,9,12),
while the -509 T allele frequency in our healthy controls was
0.572. As a result, the -509 T allele acted as a major allele in
our region, but as a minor allele in the above-mentioned regions.
Ethnic differences in TGFB1 allele frequencies may be an
explanation for the discrepancies in the findings between the
present study and the study in the US population. However, findings
of the latter study cannot explain the inconsistency in our study
and that by Jin et al, where only minor differences in the
-509 T allele frequencies were noted in the control subjects. The
discrepancy may be explained due to the different compositions of
patients with various clinicopathological characteristics in the
two studies. For the allele frequency of TGFBR2 -875A,
similar frequencies were observed between Nanjing (0.197 in
controls) and our population group (0.155 in controls) (8).
We further demonstrated that the TGFB1 -509 C
allele was associated with a decreased risk of intestinal-type
cancer. It has been widely accepted that intestinal- and
diffuse-type gastric cancer differ with regards to age, gender and
the process of carcinogenesis (13). The development of intestinal-type
malignancy is a longer multistep process via gastric atrophy,
intestinal metaplasia, dysplasia and ultimately intestinal-type
carcinoma, which is initiated by H. pylori infection and by
exposure to environmental toxins (14). TGFB1, as a regulator of
inflammation, may be involved in this multistep process. Messa
et al reported that patients with H. pylori infection
had elevated TGFβ1 levels in the gastric antrum, while TGFβ1
expression levels decreased following eradicating treatment
(15). Kandulski et al
reported that H. pylori-induced gastritis is associated with
a recruitment of naturally occurring FOXP3(+) Treg cells that
correlate with higher bacterial colonization and increased mucosal
TGFβ1 expression, suggesting that H. pylori infection
suppresses the maintenance and aggravation of gastric inflammation
by activating the TGFβ1-FoxP-CD4+CD25highTreg
pathway (16). A similar phenomenon
was observed in other animal studies (17,18).
Based on the above studies, we inferred that TGFβ1 plays an
important role in the inhibition of H. pylori-induced
gastritis. It has been reported that presence of the TGFB1
-509 C allele is related to a higher production of TGFβ1 in the
Chinese (19). Elevated TGFβ1 may
in turn affect the multistep process of gastric cancer initiated by
H. pylori infection by activating
CD4+CD25highTregs, which contribute to a
reduced incidence of intestinal-type gastric cancer.
This study showed that the TGFB1 -509 C
allele was associated with poorly differentiated gastric cancer,
but not with moderately or well-differentiated gastric cancer.
Studies have shown that the p38 MAPK pathway is involved in the
development of poorly differentiated gastric cancer (20–22). A
specific p38 inhibitor was found to reduce the irregular dense
membranous accumulation of F-actin in poorly differentiated gastric
cancer cell lines (22). Moreover,
activation of the phosphatidylinostiol 3-kinase (PI3K) via the p38
MAPK cascade caused the loss of cell-cell contact in poorly
differentiated signet-ring cell carcinoma (20,21).
TGFB1 together with the IL1B gene are involved in a complex
signal network. Therefore, the TGFB1 polymorphism may be
partially associated with poorly differentiated gastric cancer
through inhibition of the p38 MAPK pathway.
In contrast, the TGFBR2 -875A/G polymorphism
was found to be associated with decreased gastric cancer risk, and
the association was not modified by pathological types, degrees of
differentiation or TNM stages. A possible explanation for this
phenomenon is that TGFβ suppresses carcinogenesis by suppressing
tumorigenic inflammation and stroma-derived mitogens (23). In the TGFβ pathway, seven type I and
five type II receptors paired in different combinations provide the
receptor system for the entire TGFβ family. However, among the type
II receptors, only TGFβR2 is able to bind to TGFβ to activate
downstream signaling (23). Thus,
TGFβR2 acts as a key regulator in the TGFβ pathway. The
TGFBR2 -875A/G polymorphism may have an extensive effect in
reducing the risk of gastric cancer by altering the protein
expression of the TGFBR2 gene to affect signal
transduction.
Another noteworthy finding of this study was that
TGFB1 -509C/T and TGFBR2 -875A/G gene polymorphisms
acted synergistically on the decreased risk of gastric cancer. The
risk of gastric cancer was particularly lower among subjects who
carried both the TGFB1 -509 C and TGFBR2 -875 A
allele genotypes. TGFB1 and TGFBR2 map to different
chromosomes but are essential components of the same signaling
pathway. TGFβ signaling initiates carcinoma-immune cell cross-talk
within the carcinoma cell and is involved in carcinogenesis,
invasion and metastasis (24). TGFβ
activation is induced by a number of mechanisms, including the
expression of calpain and cathepsin D (24). Once activated, TGFβ binds to TGFβR2
to activate downstream signaling (24). Thus, it is feasible that the
combination of the TGFB1 -509C/T and TGFBR2 -875A/G
gene polymorphisms confer a synergistic effect on gastric cancer
initiation and progression. This result confirmed the hypothesis
that a combined assessment of functionally relevant common variants
may aid in the characterization of cancer risk and prediction of
disease aggressiveness (25).
Although studies have shown that TGFβ1 expression is
closely linked to the prognosis of gastric cancer (26,27),
neither the polymorphisms of TGFB1 -509C/T and TGFBR2
-875A/G nor the combination of the two SNPs revealed a correlation
with patient survival in this study, consistent with the study in
the US population (11). A possible
explanation is that overall survival is determined, not only by
factors involved in gastric cancer disease activity, but also by
underlying diseases and other complications. Thus, SNPs alone may
not be enough to affect the complex outcome.
In conclusion, our study provides evidence that the
TGFB1 -509 CC, CT and TGFBR2 AG genotypes are
significantly associated with a decreased risk of gastric
carcinoma. The TGFB1 -509 C allele was found to be
associated with a reduced risk of intestinal-type, poorly
differentiated and TNM III/IV stage gastric cancer. Moreover, the
combination of the TGFB1 -509C/T and TGFBR2 -875A/G
polymorphisms exhibited a synergistically decreased risk of gastric
cancer in a southern Chinese population. These findings may provide
clues to the biological mechanisms that underline tumor
heterogeneity; thus, further studies are warranted.
Acknowledgements
This study was supported by the ‘Doctoral Natural
Science Foundation of Guangdong Province, China’ (Grant no.
04300361) and ‘Research Fund for the Doctoral Program of Higher
Education of China’ (Grant no. 20070558230).
References
|
1
|
Parkin DM, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108. 2005.
View Article : Google Scholar
|
|
2
|
Moss SF and Blaser MJ: Mechanisms of
disease: inflammation and the origins of cancer. Nat Clin Pract
Oncol. 2:90–97. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mantovani A, Allavena P, Sica A and
Balkwill F: Cancer-related inflammation. Nature. 454:436–444. 2008.
View Article : Google Scholar
|
|
4
|
Bierie B and Moses HL: Tumour
microenvironment: TGFbeta: the molecular Jekyll and Hyde of cancer.
Nat Rev Cancer. 6:506–520. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yang L, Anderson DE, Baecher-Allan C, et
al: IL-21 and TGF-beta are required for differentiation of human
T(H)17 cells. Nature. 454:350–352. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Veldhoen M, Hocking RJ, Atkins CJ,
Locksley RM and Stockinger B: TGFbeta in the context of an
inflammatory cytokine milieu supports de novo differentiation of
IL-17-producing T cells. Immunity. 24:179–189. 2006. View Article : Google Scholar
|
|
7
|
Massague J, Blain SW and Lo RS: TGFbeta
signaling in growth control, cancer, and heritable disorders. Cell.
103:295–309. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Jin G, Wang L, Chen W, et al: Variant
alleles of TGFB1 and TGFBR2 are associated with a decreased risk of
gastric cancer in a Chinese population. Int J Cancer.
120:1330–1335. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Li T, Cao BW, Dai Y, Cui H, Yang HL and Xu
CQ: Correlation of transforming growth factor beta-1 gene
polymorphisms C-509T and T869C and the risk of gastric cancer in
China. J Gastroenterol Hepatol. 23:638–642. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zhang P, Di JZ, Zhu ZZ, et al: Association
of transforming growth factor-beta 1 polymorphisms with genetic
susceptibility to TNM stage I or II gastric cancer. Jpn J Clin
Oncol. 38:861–866. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Guan X, Zhao H, Niu J, Tan D, Ajani JA and
Wei Q: Polymorphisms of TGFB1 and VEGF genes and survival of
patients with gastric cancer. J Exp Clin Cancer Res. 28:942009.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Guan X, Zhao H, Niu J, Tang D, Ajani JA
and Wei Q: The VEGF -634G>C promoter polymorphism is associated
with risk of gastric cancer. BMC Gastroenterol. 9:772009.
|
|
13
|
Yamaguchi N and Kakizoe T: Synergistic
interaction between Helicobacter pylori gastritis and diet
in gastric cancer. Lancet Oncol. 2:88–94. 2001.
|
|
14
|
Kountouras J, Zavos C, Chatzopoulos D and
Katsinelos P: New aspects of Helicobacter pylori infection
involvement in gastric oncogenesis. J Surg Res. 146:149–158.
2008.
|
|
15
|
Messa C, Di Leo A, Greco B, et al:
Successful eradicating treatment of Helicobacter pylori in
patients with chronic gastritis: gastric levels of cytokines,
epidermal growth factor and polyamines before and after therapy.
Immunopharmacol Immunotoxicol. 18:1–13. 1996.
|
|
16
|
Kandulski A, Wex T, Kuester D, et al:
Naturally occurring regulatory T cells (CD4+,
CD25high, FOXP3+) in the antrum and cardia
are associated with higher H. pylori colonization and
increased gene expression of TGF-beta1. Helicobacter. 13:295–303.
2008.
|
|
17
|
Rad R, Brenner L, Bauer S, et al:
CD25+/Foxp3+ T cells regulate gastric
inflammation and Helicobacter pylori colonization in vivo.
Gastroenterology. 131:525–537. 2006.
|
|
18
|
Raghavan S, Fredriksson M, Svennerholm AM,
Holmgren J and Suri-Payer E: Absence of
CD4+CD25+ regulatory T cells is associated
with a loss of regulation leading to increased pathology in
Helicobacter pylori-infected mice. Clin Exp Immunol.
132:393–400. 2003.
|
|
19
|
Qi P, Chen YM, Wang H, et al: -509C>T
polymorphism in the TGF-beta1 gene promoter, impact on the
hepatocellular carcinoma risk in Chinese patients with chronic
hepatitis B virus infection. Cancer Immunol Immunother.
58:1433–1440. 2009.
|
|
20
|
Kobayashi M, Nagata S, Iwasaki T, et al:
Dedifferentiation of adenocarcinomas by activation of
phosphatidylinositol 3-kinase. Proc Natl Acad Sci USA.
96:4874–4879. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Xu Q, Karouji Y, Kobayashi M, Ihara S,
Konishi H and Fukui Y: The PI 3-kinase-Rac-p38 MAP kinase pathway
is involved in the formation of signet-ring cell carcinoma.
Oncogene. 22:5537–5544. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Atsumi T, Kato K, Uno K, et al:
Pathophysiological role of the activation of p38 mitogen-activated
protein kinases in poorly differentiated gastric cancer. Pathol
Int. 57:635–644. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Massague J: TGFbeta in cancer. Cell.
134:215–230. 2008. View Article : Google Scholar
|
|
24
|
Bierie B and Moses HL: Transforming growth
factor beta (TGF-beta) and inflammation in cancer. Cytokine Growth
Factor Rev. 21:49–59. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kaklamani VG, Baddi L, Liu J, et al:
Combined genetic assessment of transforming growth factor-beta
signaling pathway variants may predict breast cancer risk. Cancer
Res. 65:3454–3461. 2005.PubMed/NCBI
|
|
26
|
Nakamura M, Katano M, Kuwahara A, et al:
Transforming growth factor beta1 (TGF-beta1) is a preoperative
prognostic indicator in advanced gastric carcinoma. Br J Cancer.
78:1373–1378. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Vagenas K, Spyropoulos C, Gavala V and
Tsamandas AC: TGFbeta1, TGFbeta2, and TGFbeta3 protein expression
in gastric carcinomas: correlation with prognostic factors and
patient survival. J Surg Res. 139:182–188. 2007. View Article : Google Scholar : PubMed/NCBI
|