Introduction
Thymoma is a rare anterior mediastinal tumor with
complicated processing mechanisms. The pathological classifications
were based on the WHO classification system. Thymomas were
classified into types A, B and C (1). On the other hand, the current clinical
diagnosis is predominantly based on the estimate of surgical
management established by Masaoka et al (2). However, pathologically indolent cases
occasionally show malignancy as invasion, recurrence or metastasis
(3). For this reason, discrepancies
are noted between clinical stages and the current pathological
classifications. Therefore, certain markers should be defined as a
complement of clinicopathological parameters to evaluate malignancy
and outcome. Surgical resection is the optimal standard therapy.
Based on the large-sample analysis of 1,320 cases in Japan,
surgical treatment was shown to be an independent factor affecting
prognosis, but the value of adjuvant chemotherapy and radiotherapy
is uncertain (4). However, in terms
of the unresectable or relapsed cases, a non-surgical therapeutic
approach is the last recourse. Thus, alternative therapeutic
molecular targets are required.
As a key indicator, mutant p53 is predisposed to
cancer (5). Certain authors studied
the accumulation of an abnormal form of the protein in the cell
nucleus, the normal p53 protein with a half-life that was too short
to be detected, while most, but not all, mutant p53 proteins
possess a prolonged half-life, accumulate in tissues, and are able
to be directly detected by immunohistochemical assays (6,7). To
exclude false-positive and false-negative results, the analysis was
performed a number of times according to the most frequently used
method, i.e., immunohistochemistry with certain specific
antibodies, such as DO-7. p53 protein accumulation is interpreted
as being indicative of the presence of p53 mutations. As such, the
immunohistochemical evaluation of p53 revealed its prognostic
significance in the tumor (8,9).
Epidermal growth factor receptor (EGFR), a cellular
surface membrane glycoprotein receptor, plays a key role in the
regulation of key normal cellular processes and in the
hyperproliferation, infiltration, invasion and metastasis of
epithelium-derived tumors. Thus, gene and biological therapies
targeting EGFR were extensively applied to the treatment of certain
solid tumors (10,11).
Studies previously reported p53 and EGFR in thymoma
(12–20). However, the majority of these
studies lack a control group with benign thymic tissues or a
long-term follow-up study due to low morbidity. In this study, the
expression of p53 and EGFR in thymoma was tested using an
immunohistochemical assay. Correlations between p53 and EGFR and
clinicopathological characteristics were analyzed and the survival
rate was investigated.
Materials and methods
Patients and samples
A total of 16 thymic hyperplasia and 43 thymoma
patients were recruited in the First Affiliated Hospital of
Guangzhou Medical College and the First Affiliated Hospital of
Nanjing Medical University, China. The patients were pathologically
diagnosed between 2002 and 2005, and the 43 thymoma patients were
available for a 5-year follow-up study. Standards were adhered to
according to the ? Ethics Committee, and written informed consent
was obtained from the patients. In the thymoma patients, ages
ranged from 12–72 years (mean 45.16), with 27 females and 16 males
(Table I). The pathological
classification was in accordance with the WHO 1999 pathological
classification criteria. The distribution was: 2 with type A, 5
with type AB, 7 with type B1, 14 with type B2, 11 with type B3 and
4 with type C. The clinical staging was based on Masaoka's staging
system as follows: 11 patients in stage I, 25 in stage II, 4 in
stage III and 3 in stage IV (Table
II).
 | Table IThe clinicopathological
characteristics of epidermal growth factor receptor (EGFR) and
p53. |
Table I
The clinicopathological
characteristics of epidermal growth factor receptor (EGFR) and
p53.
| EGFR | p53 |
|---|
|
|
|
|---|
| Positive (%) | Negative (%) | p-value | Positive (%) | Negative (%) | p-value |
|---|
| Age (years) | | | 1.000 | | | 1.000 |
| <50 | 17 (68.0) | 8 (32.0) | | 21 (84.0) | 4 (16.0) | |
| ≥50 | 13 (72.2) | 5 (27.2) | | 15 (83.3) | 3 (16.7) | |
| Gender | | | 0.307 | | | 0.229 |
| Male | 13 (81.3) | 3 (18.7) | | 15 (93.4) | 1 (6.6) | |
| Female | 17 (63.0) | 10 (37.0) | | 21 (77.8) | 6 (22.2) | |
| Myasthenia
gravis | | | 0.727 | | | 0.652 |
| Positive | 9 (75.0) | 3 (25.0) | | 11 (91.6) | 1 (8.4) | |
| Negative | 21 (67.7) | 10 (22.3) | | 25 (80.7) | 6 (29.3) | |
| Tumor size (cm) | | | 0.011 | | | 0.082 |
| <6 | 8 (47.1) | 9 (53.9) | | 11 (68.8) | 5 (31.2) | |
| ≥6 | 22 (84.6) | 4 (15.4) | | 25 (92.6) | 2 (7.4) | |
| Histology | | | 0.001 | | | 0.030 |
| Thymoma | 30 (70.0) | 13 (30.0) | | 37 (86.0) | 6 (14.0) | |
| Thymus
hyperplasia | 3 (18.8) | 13 (81.2) | | 9 (56.3) | 7 (43.7) | |
| Table IIEpidermal growth factor receptor
(EGFR) and p53 with pathological classifications and clinical
stages. |
Table II
Epidermal growth factor receptor
(EGFR) and p53 with pathological classifications and clinical
stages.
| EGFR | p53 |
|---|
|
|
|
|---|
| 0 | 1+ | 2+ | 3+ | Statistical
value | 0 | 1+ | 2+ | 3+ | Statistical
value |
|---|
| Pathological
classification | | | | | p<0.001
r=0.515 | | | | | p<0.001
r=0.471 |
| A | 1 | 1 | 0 | 0 | | 1 | 1 | 0 | 0 | |
| AB | 3 | 2 | 0 | 0 | | 2 | 2 | 1 | 0 | |
| B1 | 2 | 2 | 3 | 0 | | 1 | 6 | 0 | 0 | |
| B2 | 6 | 2 | 3 | 3 | | 2 | 4 | 5 | 3 | |
| B3 | 1 | 1 | 5 | 4 | | 1 | 4 | 3 | 3 | |
| C | 0 | 1 | 1 | 2 | | 0 | 1 | 1 | 2 | |
| Total | 13 | 9 | 12 | 9 | | 7 | 18 | 10 | 8 | |
| Clinical stage | | | | | p=0.003
r=0.443 | | | | | p=0.289
N/A |
| I | 6 | 4 | 0 | 1 | | 1 | 6 | 4 | 0 | |
| II | 6 | 5 | 9 | 5 | | 6 | 9 | 4 | 6 | |
| III | 1 | 0 | 1 | 2 | | 0 | 2 | 2 | 0 | |
| IV | 0 | 0 | 2 | 1 | | 0 | 1 | 0 | 2 | |
| Total | 13 | 9 | 12 | 9 | | 7 | 18 | 10 | 8 | |
Immunohistochemical assay
The protein expression of EGFR and p53 were
evaluated immunohistochemically in representative paraffin-embedded
sections. The staining was performed with mouse monoclonal antibody
(clones EGFR 111.6, and p53 DO-7), purchased from Thermo Fisher
Scientific, Inc. (Waltham, MA, USA). The procedure was performed in
accordance with the manual's instructions. The diaminobenzidine
(DAB) immunohistochemistry kit with antimouse secondary antibody
(Invitrogen, USA) was used to visualize the antibody binding. The
p53-positive expression was considered to be the nuclear staining,
while the EGFR expression was assessed visually as indicating the
tumor cell membrane, cytoplasm or both. p53 scores were assigned:
0, negative; 1+, 10% nuclei staining positively; 2+, 10–50% nuclei;
3+, >50% nuclei (21). The
EGFR-positive expression was scored as 0, 1+, 2+ and 3+ in
accordance with Henley's system (15).
Follow-up study
A follow-up study was conducted for the thymoma
cases that were diagnosed between 2002 and 2005. Six patients were
lost at follow-up and 3 patients succumbed to diseases of other
systems. A total of 43 cases were available for the 5-year
survival, and the overall survival was defined as the time from
diagnosis to succumbing to disease. A total of 21 stage II cases,
who had undergone a complete resection without adjuvant chemo- or
radiotherapy, were selected to calculate the relapse-free time. The
relapse-free time was defined as the period of time from surgery
until relapse or progress. The patients were either contacted
through routine outpatient services or telephone interviews were
conducted. The follow-up time was 48.326±21.646 months in the
overall survival study.
Statistical analysis
The data were analyzed by software SPSS 17.0. The
Chi-square test was used to compare the variations between the two
groups. The Spearman's model was performed to analyze the
correlation coefficient. Follow-up was obtained in 43 cases and was
terminated in August 2010. A number of factors, including
pathological classification, clinical stage, EGFR expression, p53
expression and completed resection, were considered for the
multivariate analysis. The multivariate analysis, conducted with
the application of Cox regression, was used to evaluate the effect
of the selected prognostic factors on survival. Relapse-free curves
were analyzed by the Kaplan-Meier method and compared using the
log-rank test. P<0.05 was considered to be statistically
significant.
Results
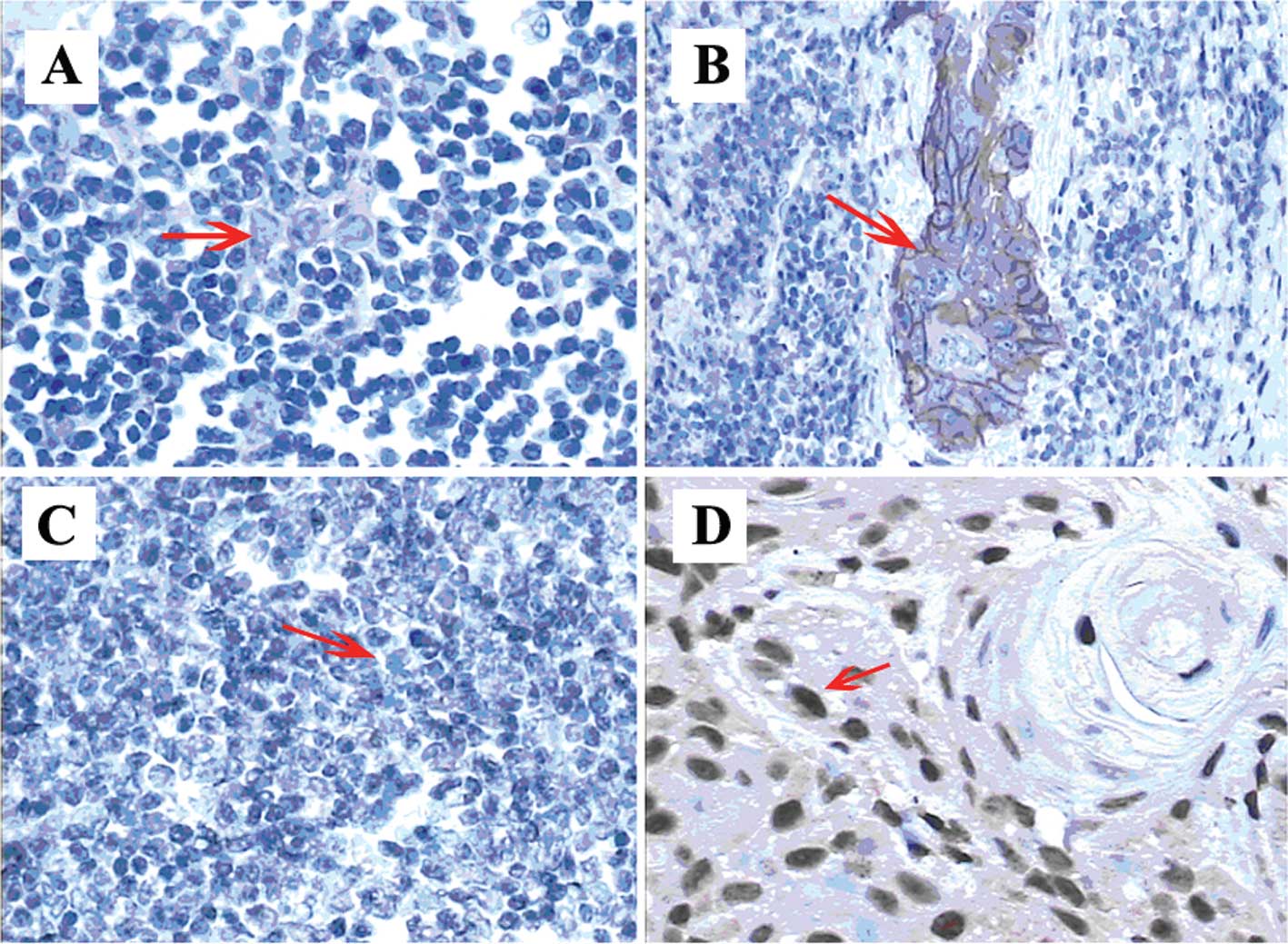
Fig. 1 shows the
expression of EGFR and p53 in immunohistochemical assays.
Patient characteristics are shown in Table I. Neither p53 nor EGFR correlated
with age, gender or myasthenia gravis morbidity (p>0.05).
Table I also shows the p53-positive
rates (56.3 vs. 86%, p<0.05) in thymic hyperplasia and thymoma;
the EGFR-positive rate was 18 and 70%, respectively (p<0.05).
The results of thymic hyperplasia and thymoma were significantly
different from those of EGFR. However, EGFR was found to correlate
with tumor size, whereas p53 did not.
p53 expression
Table II shows the
distribution of p53 expression with WHO 1999 classification in 64
patients: type A/AB 57.1%, type B1 85.7%, type B2 85.7%, type B3
90.9% and type C 100% (p<0.05, r=0.471). The positive rates of
p53 expression in the various clinical stages were analyzed (stage
I 90.9%, stage II 90.9%, stage III 100% and stage IV 100%,
p=0.289>0.05). As a result, no significance was noted between
positive and negative groups in p53 expression.
Epidermal growth factor receptor
expression
Table II shows the
positive distribution of thymoma pathological types. The positive
rates vs. pathological types were: 42.9% for type A/AB, 71.4% for
type B1, 57.1% for type B2, 90.9% for type B3 and 100% for type C.
The positive rates in the various types of thymoma were
significantly different (p<0.05, r=0.515). Regarding the rank
correlation between the positive rates and different clinical
stages (stage I 45.5%, stage II 76%, stage III 75% and stage IV
100%), a statistical significance was noted among the respective
stages (p<0.05) with a moderate relativity (r=0.443).
Follow-up results
Table III shows
the results of the multivariate analysis with a variety of factors,
including pathological classification, clinical stage, p53
expression, EGFR expression, completed resection, tumor size
(cutoff 6 cm) and myasthenia gravis. The Cox regression model
showed that only clinical stage significantly affected overall
survival (p=0.048<0.05) among the potential factors. Neither p53
(p=0.128>0.05) nor EGFR (p=0.933>0.05) was shown to be an
independent prognostic factor.
| Table IIIMultivariate analysis of several
potential factors with overall survival (43 cases). |
Table III
Multivariate analysis of several
potential factors with overall survival (43 cases).
| No. of cases | Survival (%) | p-value |
|---|
| Pathological
classification | | | 0.072 |
| A | 2 | 2 (100.0) | |
| AB | 5 | 5 (100.0) | |
| B1 | 7 | 5 (71.4) | |
| B2 | 14 | 12 (85.7) | |
| B3 | 11 | 7 (63.6) | |
| C | 4 | 1 (25.0) | |
| Clinical stage | | | 0.048 |
| I | 11 | 11 (100.0) | |
| II | 25 | 20 (80.0) | |
| III | 4 | 2 (50.0) | |
| IV | 3 | 0 (0.0) | |
| EGFR
expression | | | 0.933 |
| Positive | 30 | 21 (70.0) | |
| Negative | 13 | 12 (92.3) | |
| p53 expression | | | 0.128 |
| Positive | 36 | 27 (75.0) | |
| Negative | 7 | 6 (85.7) | |
| Completed
resection | | | 0.678 |
| Yes | 38 | 32 (84.2) | |
| No | 5 | 1 (20.0) | |
| Tumor size
(cm) | | | 0.954 |
| <6 | 17 | 16 (94.1) | |
| ≥6 | 26 | 17 (65.4) | |
| Myasthenia
gravis | | | 0.437 |
| Positive | 12 | 10 (83.3) | |
| Negative | 31 | 23 (74.2) | |
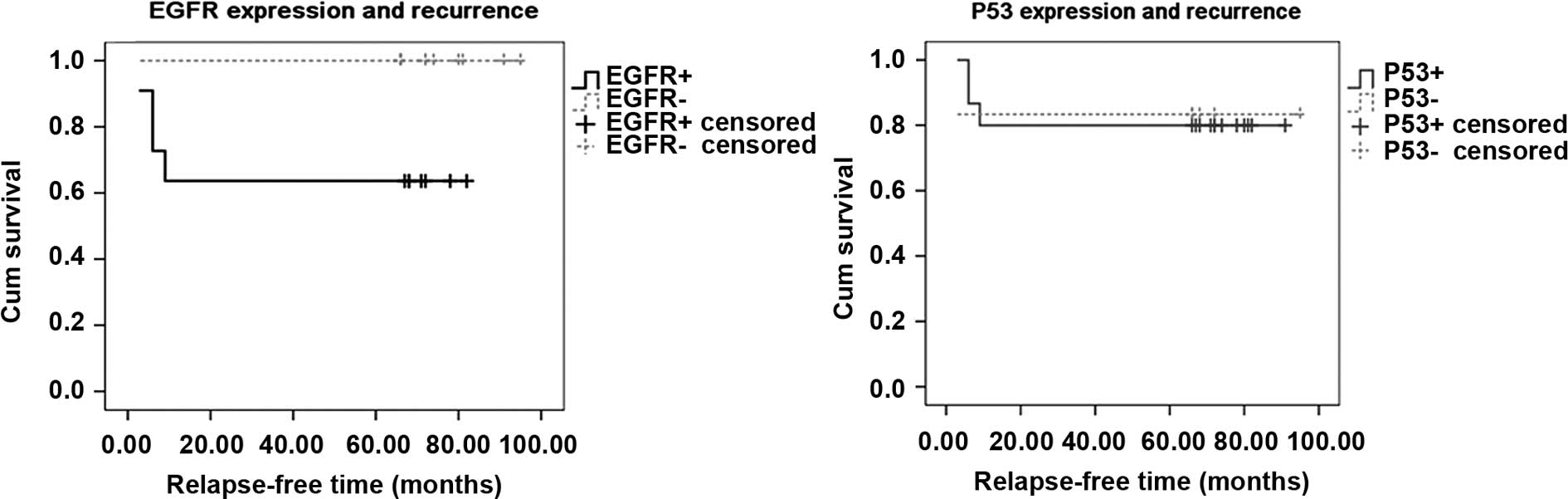
In the 21 radically resected cases with stage II, a
significant difference was noted in the relapse-free survival time
between the EGFR-negative and EGFR-positive groups (76.3±10.339 vs.
48.182±33.757 months, p=0.039<0.05). No relapse was noted in the
negative group, but a recurrence was noted in 4 cases in the
positive group within 1 year. No difference was noted between the
p53-positive and p53-negative groups (74.2±8.677 vs. 79.667±13.997
months, p=0.942>0.05). The relapse-free curves are shown in
Fig. 2.
Discussion
Thymoma is a controversial issue. Previous studies
have shown the prognostic significances of pathological
classification, clinical stage and completed resection (4,22–24).
Nevertheless, the results were inconsistent due to the rare
incidence and complicated mechanisms of thymoma. For example, our
present study showed that only clinical stage is an independent
prognostic factor, as compared to pathological classification and
completed resection. In addition, although thymoma is basically
indolent in its early stage, certain investigators asssert that
occasionally benign-appearing thymoma is potentially malignant
(25,26). Furthermore, clinical doctors have
not achieved a standardized solution to classify thymoma into
typical TMN classifications. The above phenomena in thymoma makes
it difficult to evaluate patient outcome. Therefore, numerous
checkpoint proteins were examined in thymoma in order to prove
their prognostic or predictive value, and their contribution to the
outcome evaluation (20). However,
few studies have investigated multiple factors in these tumors, due
to the fact that they lacked a control group from normal thymoma
tissues or the follow-up study had insufficient data.
The present study focused on the significance
between p53 and EGFR, and clinicopathological characteristics and
thymic hyperplasia. Furthermore, the potential factors, including
pathological classification, clinical stage, p53 expression, EGFR
expression, completed resection, tumor size and myasthenia gravis,
were subject to a multivariate analysis. We found that p53 rarely
correlated with the pathological classifications and differed in
thymic hyperplasia and thymoma. Consequently, the value of protein
accumulation in p53 is limited, since the protein accumulation did
not accurately express the status of p53 mutation. Therefore,
combining p53 genetic analysis with the immunohistochemical assay
is required in order to clarify its significance in thymoma
(27). The prevalence of EGFR is
more valuable in thymoma in that it is well-correlated with the
above pathological typing, clinical staging and tumor size and
contributes to distinguishing between thymic hyperplasia and
thymoma. The overexpression of EGFR in invasive thymoma was
previously reported, but the significance of the survival rates was
not determined. Although findings of the multivariate analysis did
not confirm whether EGFR was an independent prognostic factor, the
present follow-up data indicated that the completely resected cases
with EGFR expression showed a significantly higher relapse rate
than the negative group in stage II, suggesting that EGFR plays a
key role in thymoma progression. Therefore, if the internal
relationships between EGFR expression and thymoma and the
accompanying mechanism are clarified, an approach may be developed
that contributes to the evaluation of patient outcome with EGFR
testing (ELISA and pre-operative biopsy). Moreover, in the event
that positive results are obtained, a specific therapy may be
developed.
The role of surgery in thymoma is crucial. However,
rapidly developing non-surgical approaches have currently become
the major treatment for cases which are unresectable or in which
relapse occurs. Since EGFR is much more valuable than p53, the
former is considered a potential aim for targeted agents.
Furthermore, various trials have been conducted on the application
of EGFR-targeted agents in advanced thymoma cases (28,29). A
number of these trials showed a favorable response, indicating that
these drugs can be applied for malignant thymoma. Notably, the
results of our study did not reveal the clinical significance of
p53 and EGFR in thymoma, but a rational approach for the
application of targeted therapies. Subsequently, if the
significances of EGFR-targeted agents are confirmed in invasive
thymoma, particularly for pre-operative neo-adjuvant chemotherapy,
tumor size may be reduced and complete resection or even survival
rates may increase.
Acknowledgements
We thank Yingying Gu for the technical assistance on
immunohistochemistry assay and Yan Zhong for the data
collection.
References
|
1
|
Marx A and Muller-Hermelink H: From basic
immunobiology to the upcoming WHO-classification of tumors of the
thymus. The Second Conference on Biological and Clinical Aspects of
Thymic Epithelial Tumors and related recent developments. Pathol
Res Pract. 195:515–533. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Masaoka A, Monden Y, Nakahara K and
Tanioka T: Follow-up study of thymomas with special reference to
their clinical stages. Cancer. 48:2485–2492. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Suster S: Diagnosis of thymoma. J Clin
Pathol. 59:1238–1244. 2006. View Article : Google Scholar
|
|
4
|
Kondo K and Monden Y: Therapy for thymic
epithelial tumors: a clinical study of 1,320 patients from Japan.
Ann Thorac Surg. 76:878–884. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Vousden KH: Outcomes of p53 activation –
spoilt for choice. J Cell Sci. 119:5015–5020. 2006.
|
|
6
|
Tominaga O, Hamelin R, Remvikos Y, Salmon
R and Thomas G: p53 from basic research to clinical applications.
Crit Rev Oncog. 3:257–282. 1992.PubMed/NCBI
|
|
7
|
Shiao YH, Palli D, Caporaso NE, et al:
Genetic and immunohistochemical analyses of p53 independently
predict regional metastasis of gastric cancers. Cancer Epidemiol
Biomarkers Prev. 9:631–633. 2000.PubMed/NCBI
|
|
8
|
Steels E, Paesmans M, Berghmans T, et al:
Role of p53 as a prognostic factor for survival in lung cancer: a
systematic review of the literature with a meta-analysis. Eur
Respir J. 18:705–719. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pectasides D, Papaxoinis G, Nikolaou M, et
al: Analysis of 7 immunohistochemical markers in male germ cell
tumors demonstrates the prognostic significance of p53 and MIB-1.
Anticancer Res. 29:4151–4156. 2009.PubMed/NCBI
|
|
10
|
Carpenter G and Cohen S: Epidermal growth
factor. J Biol Chem. 265:7709–7712. 1990.
|
|
11
|
Fischer O, Hart S, Gschwind A and Ullrich
A: EGFR signal transactivation in cancer cells. Biochem Soc Trans.
31:1203–1208. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ionescu D, Sasatomi E, Cieply K, Nola M
and Dacic S: Protein expression and gene amplification of epidermal
growth factor receptor in thymomas. Cancer. 103:630–636. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hayashi Y, Ishii N, Obayashi C, et al:
Thymoma: tumour type related to expression of epidermal growth
factor (EGF), EGF-receptor, p53, v-erb B and ras p21. Virchows
Arch. 426:43–50. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sasaki H, Yukiue H, Sekimura A, et al:
Elevated serum epidermal growth factor receptor level in stage IV
thymoma. Surg Today. 34:477–479. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Henley J, Koukoulis G and Loehrer PL Sr:
Epidermal growth factor receptor expression in invasive thymoma. J
Cancer Res Clin Oncol. 167–170. 2002. View Article : Google Scholar
|
|
16
|
Aisner SC, Hameed MR, Wang W, et al: EGFR
and C-Kit immuno-staining in advanced or recurrent thymic
epithelial neoplasms staged according to the WHO: an Eastern
Cooperative Oncology Group Study. American Society of Clinical
Oncology. 22:96372004.
|
|
17
|
Girard N, Shen R, Guo T, et al:
Comprehensive genomic analysis reveals clinically relevant
molecular distinctions between thymic carcinomas and thymomas. Clin
Cancer Res. 15:6790–6799. 2009. View Article : Google Scholar
|
|
18
|
Suzuki E, Sasaki H, Kawano O, et al:
Expression and mutation statuses of epidermal growth factor
receptor in thymic epithelial tumors. Jpn J Clin Oncol. 36:351–356.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Tomita M, Matsuzaki Y and Onitsuka T:
Relationship between expression of cancer-related proteins and
tumor invasiveness in thymoma. Eur J Cardiothorac Surg. 21:595–598.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Baldi A, Ambrogi V, Mineo D, et al:
Analysis of cell cycle regulator proteins in encapsulated thymomas.
Clin Cancer Res. 11:5078–5083. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Landolfi JA and Terio KA: Transitional
cell carcinoma in fishing cats (Prionailurus viverrinus):
pathology and expression of cyclooxygenase-1, -2 and p53. Vet
Pathol. 43:674–681. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Detterbeck FC: Clinical value of the WHO
classification system of thymoma. Ann Thorac Surg. 81:2328–2334.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Detterbeck FC and Parsons AM: Thymic
tumors. Ann Thorac Surg. 77:1860–1869. 2004. View Article : Google Scholar
|
|
24
|
Yin H, Du J, Lu Z, Jiao X, Wang J and Zhou
X: The correlation of the World Health Organization histologic
classification of thymic epithelial tumors and its prognosis: a
clinicopathologic study of 108 patients from China. Int J Surg
Pathol. 17:255–261. 2009. View Article : Google Scholar
|
|
25
|
Riedel RF and Burfeind WR Jr: Thymoma:
benign appearance, malignant potential. Oncologist. 11:887–894.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Reddy RHV, Shah R, Kumar B and Thorpe JAC:
Recurrence of stage I thymoma in sternum, 13 years after ‘complete’
excision. Eur J Cardiothorac Surg. 23:134–135. 2003.PubMed/NCBI
|
|
27
|
Shiao Y-H, Palli D, Caporaso NE, et al:
Genetic and immunohistochemical analyses of p53 independently
predict regional metastasis of gastric cancers. Cancer Epidemiol
Biomarkers Prev. 9:631–633. 2000.PubMed/NCBI
|
|
28
|
Bedano PM, Perkins S, Burns M, et al: A
phase II trial of erlotinib plus bevacizumab in patients with
recurrent thymoma or thymic carcinoma. American Society of Clinical
Oncology. 26:190872008.
|
|
29
|
Christodoulou C, Murray S, Dahabreh J, et
al: Response of malignant thymoma to erlotinib. Ann Oncol.
19:1361–1362. 2006. View Article : Google Scholar : PubMed/NCBI
|