Introduction
Multiple myeloma (MM) is a malignant neoplasm of
plasma cells that accumulate in the bone marrow, and accounts for
approximately 10% of all hematological malignancies (1). Multiple myeloma is characterized by
skeletal destruction, renal failure, hypercalcemia and monoclonal
immunoglobulin (M protein) accumulation in the serum or urine. The
solitary extramedullary plasmacytoma (SEP) is a rare form of tumor,
accounting for less than 3% of all plasma cell neoplasms. SEPs are
localized mainly in the the submucosa of various organs in the head
and neck; however, epidural space involvement is relatively rare
(2). The diagnosis of SEP is based
on histological confirmation of a single extramedullary mass of
plasma cells with no evidence of multiple myeloma (3). The SEP size has been reported to be a
poor prognostic factor (4).
Therefore, the treatment of large SEP remains a challenge. In the
present study, we report the case of a previously untreated patient
with a large epidural plasmacytoma who achieved an excellent
clinical response and sustained remission following bortezomib
treatment. The study was approved by the ethics committee of Fujian
Medical University. Informed consent was obtained from the patient
who participated in the study.
Case report
This report presents the case of a 35-year-old male
with no significant clinical background. At the time of referral to
The First Affiliated Hospital of Fujian Medical University (China),
the patient had suffered from thoracic back pain for 2 months and
progressively ascending bilateral numbness and weakness of the
lower extremities for 1 month. Shortly following a visit to the
neurology clinic, the patient became unable to walk independently
and developed urinary incontinence. Neurological examination
revealed that muscular strength was normal in the upper limbs, but
decreased in the lower limbs (grade 1/5 strength in the left and
grade 2/5 in the right). Muscular tension increased in the lower
limbs. Superficial and deep sensation disturbance was found below
the level of T5 for the left side and T6 for the right side,
respectively. The reflexes did not exist in the two sides,
including cremaster, patellar tendon and abdominal wall at the
upper, middle and lower level. Signs of Babinski, Oppenheim,
Chaddock and Gordon were positive in the two sides. Cranial
computed tomography (CT) and magnetic resonance imaging (MRI) were
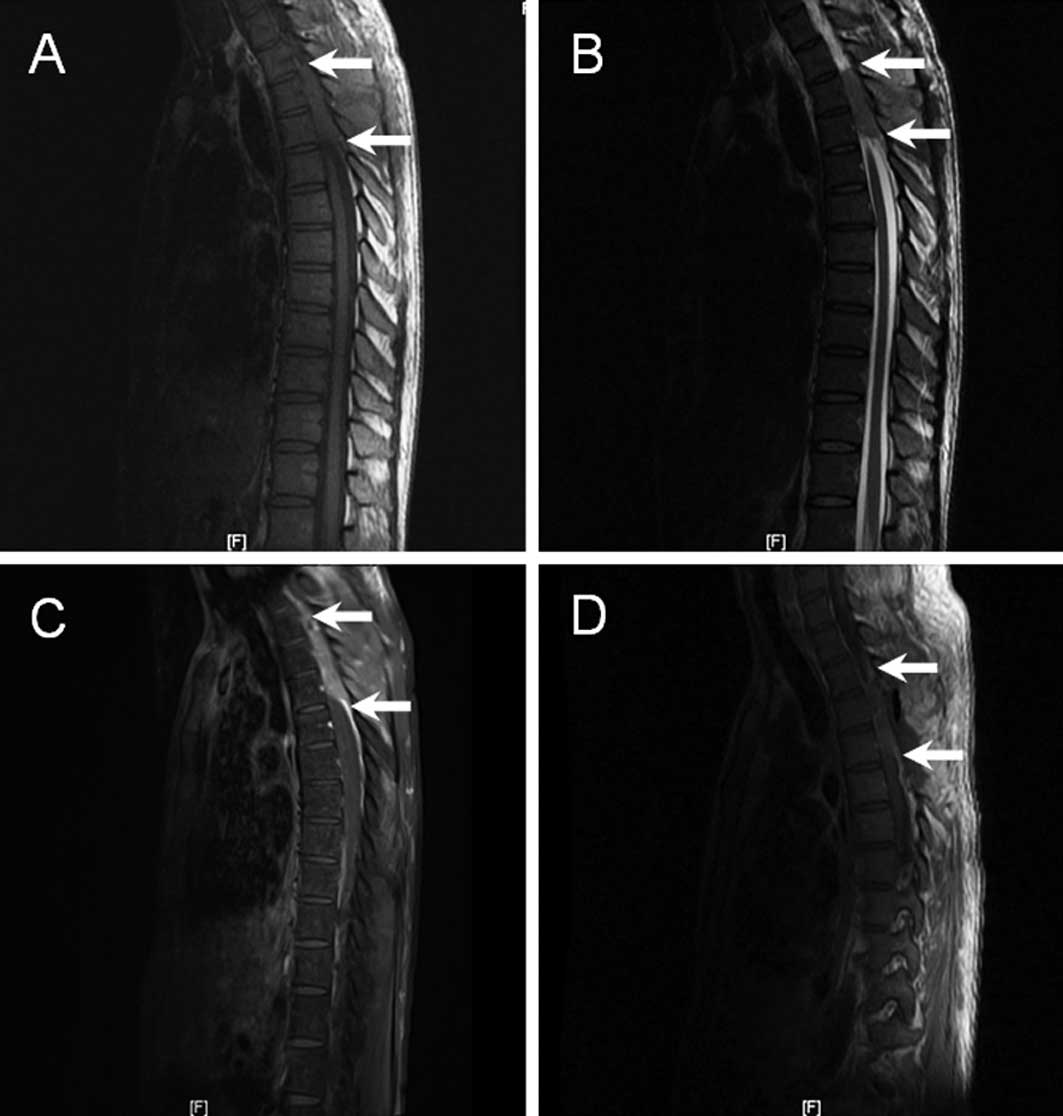
normal. Plain MRI of the thoracic spine revealed an epidural mass
(6.4×1.4×4.2 cm), which was located at the T2–T4 level where it
compressed the spinal cord. The mass was isointense to the spinal
cord on the T1-weighted image (Fig.
1A) and hyperintense on the T2-weighted image (Fig. 1B), with a moderate and homogenous
contrast enhancement (Fig. 1C).
Bone destruction was observed in the corresponding spinal and
vertebral plate. The right lateral neighboring muscles were not
well organized.
The patient underwent neurosurgical intervention
with T2–T4 vertebral canal decompression and excision of the
extradural tumour. However, a postoperative MRI of the thoracic
spine revealed that only part of the epidural mass had been
removed. Slight contrast enhancement showed that the remaining mass
had been maintained in the same position (Fig. 1D). Histopathological analysis of the
tumour tissue revealed that the cells expressed CD38 and CD138,
which were markers of plasma cells. However, CD20, a typical
immunophenotype for B lymphocytes, was negative. The patient was
referred to the hematology department for further investigation
following the announcement of the histopathology report. At that
time, laboratory work-up findings revealed an erythrocyte
sedimentation rate (ESR) of 20 mm/h, C-reactive protein of 5.76
mg/l, white blood cell count of 11.48×109/l, hemoglobin
of 129 g/l and platelets 175×1012/l. The serum renal and
liver function tests were within normal ranges. The
β2-microglobulin level was 1.74 mg/l (reference range:
0.7–1.8 mg/l). Bence-Jones protein was negative. The serum
concentrations of immunoglobulins were as follows: IgG 10.6 g/l,
IgA 2.62 g/l, IgM 0.86 g/l, κ 2.5 g/l and λ 1.9 g/l. Serum protein
electrophoresis revealed no abnormal spike, and immunofixation
electrophoresis revealed polyclonal bands. Bone marrow examination
revealed 7.5% well-differentiated plasma cells. These findings were
utilized in making the diagnosis of extraosseous epidural
plasmacytoma.
The patient received bortezomib at a dose of 1.0
mg/m2 on days 1, 4, 8 and 11 of a 21-day cycle in
combination with a dose of 40 mg dexamethasone intravenously on
days 1, 2, 4, 5, 8, 9 and 11 and 12 of each cycle, as well as a
dose of 75 mg thalidomide daily. Following completion of the first
cycle of combination chemotherapy, the automatic micturition
function returned to normal. Back pain was significantly reduced
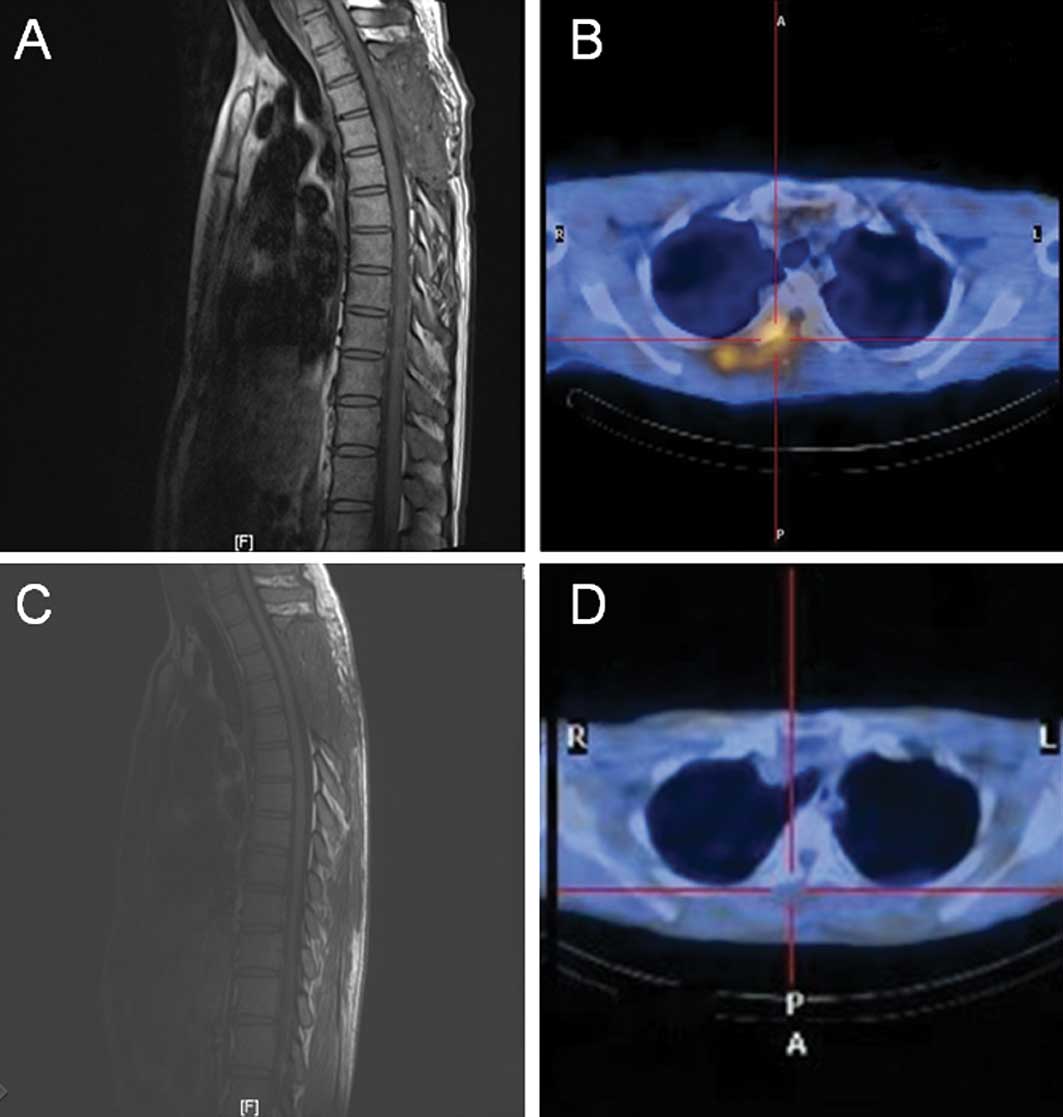
and the strength in the patient’s lower limbs gradually improved. A
repeat MRI revealed complete remission of the epidural mass with
decompression of the spinal cord (Fig.
2A); however, 18F-fluorodeoxyglucose
(18F-FDG) positron emission tomography (PET)/CT scan
revealed focal areas of increased 18F-FDG uptake
(Fig. 2B). The patient experienced
4 cycles of chemotherapy, which were well tolerated and no side
effects were documented. Over 1 year following the initial
diagnosis, there was no evidence of relapse in the repeat MRI
(Fig. 2C) and 18F-FDG
PET/CT (Fig. 2D). No evidence was
found of evolution to multiple myeloma. The muscle strength of the
legs improved to grade 5 and the patient was able to walk.
Discussion
SEP is a rare clinical entity of plasma cell
neoplasms, particularly when located in the epidural region. Since
SEP may be confused with non-Hodgkin’s lymphoma, careful
histopathological evaluation of the infiltrated cells is crucial
for diagnosis. Furthermore, multiple myeloma should be excluded. In
this case, histopathology revealed a typical immunophenotype of
plasma cells. There were no signs of multiple myeloma following
hematological analysis, serum chemistry, serum protein
electrophoresis and bone imaging. Thus, a diagnosis of SEP was
confirmed.
The optimal management of SEP remains unclear. The
generally applied treatment is radiotherapy as SEP is highly
radiosensitive. Certain studies report that local radiotherapy may
achieve excellent local control (5–6).
However, failure to respond is frequent for bulky SEP of >5.0
cm, which is considered to be a poor prognosis factor for survival
(4–5,7). Since
in this case the tumor was >5.0 cm, we treated the patient with
bortezomib, based on the fact that bortezomib is effective for
relapsed/refractory myeloma, as well as extramedullary relapses of
multiple myeloma (1,8–9).
This is the first case of a previously untreated
epidural plasmacytoma that was successfully treated with
bortezomib-containing chemotherapy. The combination of
bortezomib/dexamethasone/thalidomide was well tolerated and no side
effects were documented. The patients achieved complete and
sustained remission. Additionally, we found that MRI is useful in
follow-up examinations during therapy, since the images may
document a reduction in tumor size. PET/CT scans are also capable
of providing additional information to MRI if problems with the MRI
technique arise.
In conclusion, this case provides evidence that the
use of bortezomib in combination with dexamethasone and thalidomide
may be a reliable, safe and effective alternative for treating
previously untreated epidural plasmcytomas.
References
|
1
|
Kyle RA and Rajkumar SV: Multiple myeloma.
Blood. 111:2962–2972. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Okacha N, Chrif E, Brahim E, et al:
Extraosseous epidural multiple myeloma presenting with thoracic
spine compression. Joint Bone Spine. 75:70–72. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zazpe I, Caballero C, Cabada T, Guerrero
D, Gallo-Ruiz A and Portillo E: Solitary thoracic intradural
extramedullary plasmacytoma. Acta Neurochir (Wien). 149:529–532.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Soutar R, Lucraft H, Jackson G, Reece A,
Bird J, Low E and Samson D: Guidelines on the diagnosis and
management of solitary plasmacytoma of bone and solitary
extramedullary plasmacytoma. Br J Haematol. 124:717–726. 2004.
View Article : Google Scholar
|
|
5
|
Tsang RW, Gospodarowicz MK, Pintilie M,
Bezjak A, Wells W, Hodgson D and Stewart A: Solitary plasmacytoma
treated with radiotherapy: impact of tumor size on outcome. Int J
Radiat Oncol Biol Phys. 50:113–120. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Galieni P, Cavo M, Pulsoni A, et al:
Clinical outcome of extramedullary plasmacytoma. Haematologica.
85:47–51. 2000.
|
|
7
|
Holland J, Trenkner DA, Wasserman TH and
Fineberg B: Plasmacytoma. Treatment results and conversion to
myeloma. Cancer. 69:1513–1517. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Espanol I, Martinez A, Lopez MD, et al:
First report of a medullar cord compression secondary to osseous
plasmacytoma successfully treated with bortezomib and
dexamethasone. Leuk Res. 34:E97–E99. 2010. View Article : Google Scholar
|
|
9
|
Laura R, Cibeira MT, Uriburu C, Yantorno
S, Salamero O, Blade J and Montserrat E: Bortezomib: an effective
agent in extramedullary disease in multiple myeloma. Eur J
Haematol. 76:405–408. 2006. View Article : Google Scholar : PubMed/NCBI
|