Introduction
Gastric or gastroesophageal junction (GEJ)
adenocarcinoma represents a global health problem. In
industrialized countries, the incidence of GEJ and gastric cardial
cancers continues to rise, while noncardial gastric cancers have
declined over the past few decades. In Israel, the incidence of
gastric cancer has remained stable throughout the last decade,
annually affecting 650–700 new patients. The incidence trend,
described as the age standardized rate (ASR/100,000), is declining
in the Jewish population, while rising in the Arab population
(1).
The human epidermal growth factor 2 (HER2) gene is a
well-described proto-oncogene. High amplification of this gene
induces protein overexpression in the cellular membrane, conferring
oncogenic properties to a malignant cell (2). Although HER2 gene amplification and
protein overexpression have been mostly studied in breast cancer, a
wide overexpression variation has been demonstrated in other
malignancies (3). HER2
overexpression, measured using immunohistochemistry (IHC), was
reported in 4–53% of gastric adenocarcinoma cases, with a median of
18% (4). In a previous study, the
incidence of HER2/neu gene amplification was revealed to be higher
in GEJ tumors compared with other gastric tumors, and in an
intestinal histologic subtype compared with a diffused subtype
(5). A recently published
systematic review was inconclusive with regard to the prognostic
association between HER2 overexpression and poorer survival in
patients who underwent curative surgery (4).
The standard of care in advanced gastric carcinoma
patients has changed recently, due to a phase III trial adding
trastuzumab to chemotherapy in patients with overexpression of HER2
(ToGA trial). The study indicated that this subgroup of patients
would benefit from an improvement in overall survival of almost
three months (6).
The retinoblastoma (Rb) protein is a tumor
suppressor protein that is dysfunctional in many cancers, including
gastric adenocarcinoma. One function of phosphorylated Rb (pRb) is
to prevent excessive cell growth by inhibiting cell cycle
progression in the G1-S checkpoints. Cyclin D1 is a component of
this pathway, and it stimulates phosphorylation of the Rb protein
by associating with cyclin-dependent kinases (CDKs). Overexpression
of cyclin D1 causes pRb pathway dysfunction and stimulation of cell
proliferation (7). Upregulation of
cyclin D1 has been described in gastric cancer; however, its
prognostic value is not fully clear. A possible correlation between
HER2 and cyclin D1, both suggested to be poor prognostic tissue
markers, had not been examined prior to this study.
The aim of the current study was to evaluate the
incidence and the prognostic value of HER2 overexpression among an
Israeli population with gastric or GEJ adenocarcinoma. In addition,
the correlation between HER2 and cyclin D1 in this patient
population was also investigated.
Materials and methods
Patients
The records and histological specimens of
consecutive gastric or GEJ adenocarcinoma patients who had
undergone surgery or biopsies, and were treated in the Division of
Oncology at Rambam Healthcare Campus (Haifa, Israel) from June 2005
to March 2009, were evaluated. Clinical and demographical data were
retrospectively collected from the computerized hospital medical
charts. Data included location of the primary tumor, TNM staging,
histological subtype, perineural or vascular invasion, type of
surgery, adjuvant chemotherapy and/or radiotherapy, time to
recurrence, site of metastases, chemotherapy regimens, response to
treatment, time to tumor progression and survival. The study was
conducted in accordance with the Helsinki declaration and approved
by the Rambam Health Care Campus Ethics Committee, Bat-Galim,
Haifa, Israel.
Immunohistochemical staining
All specimens were fixed in buffered formalin and
were immunohistochemically stained for HER2 using the polyclonal
antibody anti c-erbB-2 (dilution 1:1400; Dako; Glostrup, Denmark).
Immunoreactivity was determined according to the scoring system for
gastric carcinoma. For validation, certain cases were evaluated
with the Ventana PATHWAY anti-HER-2/neu (4B5) rabbit monoclonal
primary antibody (Ventana Medical Systems, Inc., Tucson, AZ, USA).
Cases that scored 2+ were further evaluated using the HER2 CISH
pharmDx kit (Dako). Additionally, cases were evaluated for cyclin
D1 immunoreactivity using the rabbit monoclonal anti-cyclin D1
(SP4) antibody (dilution 1:90; Lab Vision/Neomarkers; Fremont, CA,
USA). All immunostaining was performed in the Ventana Benchmark XT
immunostainer (Ventana Medical Systems, Inc.). Positive controls,
for HER2 (breast cancer) and cyclin D1 (mantel cell lymphoma), and
negative controls were run in parallel. A total of 24 biopsy
specimens (16%) were compared with surgical specimens.
Statistical methodology
To identify parameters associated with HER2
overexpression, binary logistic regression was implemented,
including calculation of odds ratios (OR) with 95% confidence
intervals (CI) and P-values in the bivariate analysis. Survival
analysis was performed by the Kaplan-Meier method for overall
survival (OS), according to HER2 in locoregional and metastatic
diseases. To identify parameters associated with the OS bi-variant,
Cox regression was used. P-values, hazard ratios (HR) and 95% CI
were presented.
All variables with P<0.2 in bivariate analyses
were included in a multivariable explanatory model. A multivariate
analysis (Cox regression model) was utilized to determine the
independent effects of variables on overall survival. The
likelihood ratio was used as a measure of model discrimination.
To analyze the difference between biopsy and surgery
histology parameter results, the κ-coefficient was used. A
two-tailed P≤0.05 was considered to indicate a statistically
significant difference. Statistical analyses were performed with
Statistics Products Solutions Services (SPSS) 18.0 software for
Windows (SPSS, Inc.; Chicago, IL, USA).
Results
General remarks
The key demographic and clinical characteristics of
patients are summarized in Table I
One hundred and fifty patients, 59% of which were male, were
included in the study. The median age at diagnosis was 65 years and
52 (30%) patients were over the age of 70. Arabs constituted 23% of
the study population. Poorly differentiated or signet ring cell
carcinoma was present in 65% of patients. The disease was
metastatic in 68 (45%) patients and signet ring cell carcinoma was
the most common histological subtype.
 | Table I.Associations between patient
demographics, clinicopathological parameters and HER2 status in 150
gastric adenocarcinoma cases. |
Table I.
Associations between patient
demographics, clinicopathological parameters and HER2 status in 150
gastric adenocarcinoma cases.
| Variable | No. of patients | HER2 | Odds ratio | 95% confidence
interval | P-value |
|---|
| Gender | | | | | |
| Male | 89 (59%) | 10 (11%) | 1.00 | Reference | 0.34 |
| Female | 61 (41%) | 4 (6.6%) | 0.55 | 0.16–1.85 | |
| Age (years) | | | | | |
| ≤50 | 27 (18%) | 3 (11%) | 1.00 | Reference | 0.13 |
| 51–70 | 71 (47%) | 3 (4.2%) | 0.35 | 0.67–1.87 | 0.22 |
| ≥71 | 52 (35%) | 8 (15.4%) | 1.45 | 0.30–6.00 | 0.60 |
| Ethnicity | | | | | |
| Jewish | 116 (77%) | 12 (10.4%) | 1.00 | Reference | 0.48 |
| Arab | 34 (23%) | 2 (6.3%) | 0.57 | 0.12–2.67 | |
| Histology | | | | | |
| Well diff. | 10 (7%) | 0 | | 0.16 | |
| Moderate diff. | 31 (21%) | 7 (22.6%) | | | |
| Signet ring and
poor diff. | 96 (65%) | 7 (7.2%) | | | |
| Mucinous | 13 (8%) | 0 | | | |
| Stage | | | | | |
| I | 19 (13%) | 1 (5.3%) | 1.00 | Reference | 0.80 |
| II and III | 63 (42%) | 6 (9.5%) | 1.90 | 0.21–16.8 | 0.56 |
| IV | 68 (45%) | 7 (10.3%) | 2.06 | 0.24–17.91 | 0.51 |
| Location | | | | | |
| GEJ and cardia | 47 (31%) | 5 (10.4%) | 1.20 | 0.38–3.80 | 0.75 |
| Body | 52 (35%) | 4 (7.3%) | 0.66 | 0.20–2.25 | 0.51 |
| Antrum | 46 (31%) | 5 (10.6%) | 1.24 | 0.39–3.93 | 0.71 |
| Entire stomach | 5 (3%) | 0 | 0.999 | | |
| Cyclin D1 | | | | | |
| ≤5% | 15 (10%) | 0 | | 0.69 | |
| 6–49% | 72 (48%) | 9 (12.5%) | | | |
| ≥50% | 63 (42%) | 5 (8%) | | | |
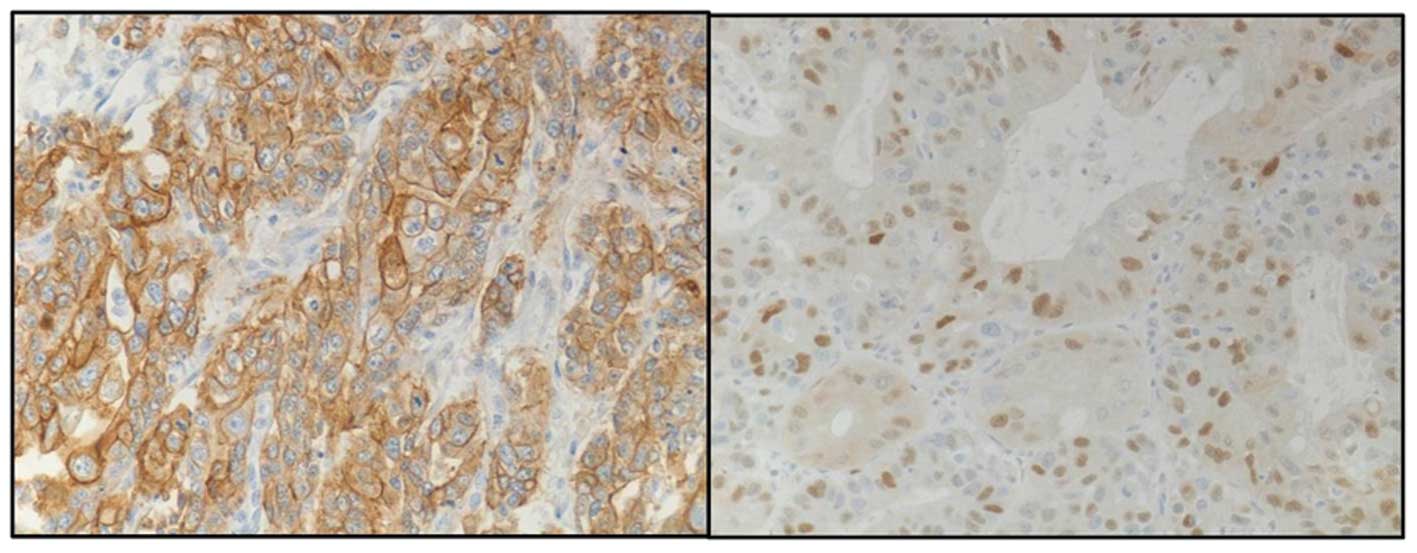
All 150 histological specimens of gastric carcinoma
were immunohistochemically stained for HER2 and cyclin D1
immunoreactivity, as described previously (Fig. 1). In 24 cases, the biopsy specimens
were compared to the surgical specimens. Only 14 (9.4%) specimens
were HER2-positive (HER2+). Among the positive
specimens, 11 exhibited an IHC HER2 score of +3, while three out of
six cases with an IHC score of +2 demonstrated HER2 amplification
in the CISH test. All demographic, histopathological and clinical
parameters were tested for association with HER2+;
however, no significant correlation was identified between HER2+
tumors and any of the parameters evaluated (Table I).
HER2 status in association with stage and
survival
HER2+ status was identified in 7/82
(8.5%) patients with stage I–III adenocarcinoma who were treated
with curative intent, and in 7/68 (10.3%) cases with stage IV
adenocarcinoma. In the metastatic group, median survival was 9.5
and 2.5 months for HER2-negative (HER2−)and
HER2+ patients, respectively (P=0.041). First-line
therapy consisted of platinum and 5FU/capecitabine, with or without
taxanes. No HER2+ patients were treated with
trastuzumab. In the non-metastatic group, median survival time was
59 months for HER2− and 42 months for HER2+
patients, and this difference was not statistically different. In
this group, 63 patients were in stage II–III and 19 in stage I of
the disease. Adjuvant chemo-radiotherapy was given to 53 out of 63
patients.
Prognostic factors for survival
A Cox regression model was utilized to determine the
independent effects of variables on overall survival. In a
bivariate analysis (Table II),
stage level was included in the model with P<0.001 (HR, 4.1).
The other variables, with P<0.2 in the bivariate analyses, were
HER2+ (P=0.10; HR, 1.7) and age over 70 years (P=0.19;
HR, 1.45). These parameters were also included in the multivariable
explanatory model. For illustration of the model, 1- and 2-year
mortality were added to Table II.
In the Cox regression multivariant analysis, together with stage
(stage II–III: HR, 3.38; 95% CI, 1.2–9.5 and stage IV: HR, 1.73;
95% CI, 4.25–32.50), HER2+ was also revealed to be an
independent negative prognostic factor for survival (HR, 1.2; 95%
CI,1.03–3.58; P=0.046), although the positive HER2 group was a
small sample size.
| Table II.Associations between patient
demographics, histology parameters and mortality. |
Table II.
Associations between patient
demographics, histology parameters and mortality.
| Variable | No. of patients | 1-year mortality
(%) | 2-year mortality
(%) | Hazard ratio | 95% confidence
interval | P-value |
|---|
| Gender | | | | | | |
| Male | 89 | 39 (43.8%) | 51 (57.3%) | 1 | Ref. | |
| Female | 61 | 23 (37.7%) | 39 (54.1%) | 0.75 | 0.50–1.13 | |
| Age (years) | | | | | | |
| ≤50 | 27 | 7 (26%) | 15 (55.6%) | 1 | Ref. | 0.17 |
| 51–70 | 71 | 25 (35.2%) | 36 (50.7%) | 0.99 | 0.57–1.71 | 0.98 |
| ≥71 | 52 | 30 (57.7%) | 33 (63.5%) | 1.45 | 0.83–2.54 | 0.19 |
| Stage | | | | | | |
| I–III | 82 | 16 (19.5%) | 26 (31.7%) | 1 | Ref. |
>0.0001 |
| IV | 68 | 46 (67.6%) | 58 (85.5%) | 4.14 | 2.76–6.21 | |
| Histology | | | | | | |
| Well diff. | 10 | 3 (30%) | 3 (30%) | 1 | Ref. | 0.43 |
| Moderate
diff. | 31 | 10 (32.3%) | 15 (48.4%) | 1.14 | 0.46–2.84 | 0.77 |
| Signet ring and
poorly diff. | 97 | 46 (47.4%) | 61 (63%) | 1.47 | 0.64–3.40 | 0.36 |
| Mucinous | 12 | 3 (25%) | 5 (41.7% | 0.90 | 0.30–2.68 | 0.85 |
| HER2 status | | | | | | |
| Negative | 136 | 53 (39%) | 74 (54.4%) | 1 | Ref. | 0.10 |
| Positive | 14 | 9 (64%) | 10 (71.4%) | 1.68 | 0.90–3.15 | |
| Cyclin D1 | | | | | | |
| ≤5% | 15 | 7 (46.7%) | 10 (66.7%) | 1 | Ref. | 0.88 |
| 6–49% | 72 | 28 (39%) | 38 (52.8%) | 0.89 | 0.45–1.76 | 0.73 |
| ≥50% | 63 | 27 (43%) | 36 (57%) | 0.97 | 0.49–1.93 | 0.94 |
Cyclin D1 and validation tests
Due to the low incidence of HER2+ in the
study population when the anti-c-erbB2 oncoprotein antibody was
used, a sample of 15 cases with an HER2 score of +1 or +2 was also
evaluated with the Ventana PATHWAY anti-HER-2/neu (4B5) rabbit
monoclonal primary antibody, for validation. Although the staining
with the Ventana PATHWAY anti-HER2/neu (4B5) antibody was clearer
for evaluation, no difference in the scoring level was observed
between the two staining antibodies.
The majority of cases (89.3%) were cyclin
D1-positive (>5% staining of tumor cells). Only 16 cases had ≤5%
cell staining; all of which were HER2−, and only 2 of which had a
weak HER2 staining score of +1. No association was identified
between HER2 status and cyclin D1. A threshold of 50% cell staining
was used to differentiate between positive and highly positive
cyclin D1 staining. No correlation was observed between the level
of cyclin D1 positive staining and any of the clinicopathological
parameters or survival. Among the 134 positive cases, 71 (47.3%)
cases exhibited positive staining (5%<cyclin D1<50%) and 63
(42%) were highly positive (>50% of the tumor cells).
The possibility of a difference in HER2 score or
cyclin D1 staining between primary biopsies and surgical specimens
was evaluated in 24 cases. No significant differences were observed
in HER2 status or score between specimens. Heterogeneity was
observed in the cyclin D1 level, while 52% of duplicated cases were
not in the same cyclin D1 level group, with a κ value of 0.14 that
indicated a slight degree of association.
Discussion
The prognostic value of HER2 gene amplification and
protein overexpression in gastric adenocarcinoma is not as
established as it is in breast cancer. In a retrospective study in
Singapore, the rate of HER2 overexpression in patients who
underwent curative surgery was 9.4% and was inversely correlated
with survival in intestinal-type gastric cancer (8). However, a large retrospective study of
over 900 cases identified similar rates of positive HER2 cases
(<10%), but no correlation with survival was observed (9). A review of 35 published studies, which
evaluated the prognostic value of HER2, indicated no differences in
the majority of studies, with regard to overall survival (OS). Two
studies identified a longer OS, while 13 (37%) observed a
significantly poorer OS (4). The
current study supports the data indicating that HER2 overexpression
in gastric cancer is a poor prognostic sign.
A retrospective study involving 461 consecutive
patients with gastric cancer evaluated the clinical and
pathological characteristics of gastric cancer in Israel, in
comparison to with a Western population. The authors indicated that
results unique to the Israeli population were increased incidence
of gastric cancer in Ashkenazi Jews and a high incidence of second
primary malignancy and family history of cancer. In both study
populations, there was no predominance of proximal gastric cancer
(10). In the current study, no
significant differences were identified between Jewish and Arab
populations, or between gastric and GEJ adenocarcinoma patients,
with regard to HER2 expression. The median age at diagnosis was
similar to that observed in other studies (10,11).
However, HER2 positivity in Ashkenazi Jews was not evaluated due to
the small number of patients. The rate of HER2 positivity
identified in the current study is within the lower range published
in the literature (11–13). Tumor heterogeneity is more common in
gastric cancer patients than in breast cancer patients, with regard
to HER2 scoring. Therefore, a significant number of patients may be
missed, as was demonstrated in a previous validation study
(12).
Further examination of uncertain cases in relation
to tumor heterogeneity, type, grade, location and distribution of
polysomy did not provide valuable information for the validation of
HER2 status (12). In the current
study, all histological specimens were immunohistochemically
stained for HER2 using anti c-erB2 oncoprotein antibody (Dako).
Several cases were further evaluated by the Ventana PATHWAY
anti-HER-2/neu (4B5) antibody. Cases that demonstrated an IHC score
of +2 were further evaluated using the HER2CISH pharmDx kit (Dako).
This was conducted similarly to the recommendations by Rüschoff
et al, which suggest that IHC should be the initial testing
methodology and FISH/silver in situ hybridization should be
used to re-evaluate samples with an IHC score of +2 (14).
The clinical significance of cyclin D1
overexpression in gastric cancer is inconclusive (7); it has been demonstrated to be
associated with poor differentiation, diffuse type lesions, signet
ring cell carcinoma or lymph node involvement, and depth of
invasion (15,16). In the present study, the majority of
samples were cyclin D1-positive. Even when a threshold of 50% cell
staining was applied to differentiate between positive and highly
positive cyclin D1 staining, no correlation was identified between
cyclin D1-positive staining and survival. Also, no correlation was
demonstrated between HER2 status and cyclin D1. There were certain
differences in the extent of cyclin D1 staining between the primary
biopsy and the full surgical specimen; we propose this was a
consequence of heterogeneity for cyclin D1 staining in the full
surgical specimen. Therefore, in this case, a primary biopsy
specimen taken from a limited location within the tumor may not
accurately represent the extent of cyclin D1 staining. Differences
in immunostaining between the primary biopsy and the full surgical
specimen may also be attributed to differences in fixation between
smaller and larger sized tissue samples (17). However, this is less likely in our
case, since no differences in the interpretation of HER2
immunostaining were noted.
According to the ToGA trial (a large, multicenter,
phase III, randomized controlled trial), trastuzumab in combination
with chemotherapy is the new standard option for patients with
HER2+ advanced gastric and GEJ adenocarcinoma, due to
its survival benefit (6). The
independent prognostic value of HER2 overexpression, as identified
in the current study as well as in others (4), raises the need for clinical evaluation
of anti-HER2 monoclonal antibodies as a part of the adjuvant
treatment protocol for gastric adenocarcinoma.
In conclusion, the rate of positive HER2 status in
the current group of unselected Israeli patients with gastric and
GEJ adenocarcinoma was relatively low, compared with that noted in
the literature. Nevertheless, positive HER2 was associated with a
poor prognosis in Cox regression multivariate analysis.
References
|
1.
|
Israel National Cancer Registry: Cancer
Incidence Tables: Stomach. http://abush.health.gov.il/download/sartan/trends/Stomach.pdf.
Accessed August 2009.
|
|
2.
|
Slamon DJ, Godolphin W, Jones LA, et al:
Studies of the HER-2/neu proto-oncogene in human breast and ovarian
cancer. Science. 244:707–712. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Scholl S, Beuzeboc P and Pouillart P:
Targeting HER2 in other tumor types. Ann Oncol. 12(Suppl 1):
S81–87. 2001. View Article : Google Scholar
|
|
4.
|
Chua TC and Merrett ND: Clinicopathologic
factors associated with HER2-positive gastric cancer and its impact
on survival outcomes - a systematic review. Int J Cancer.
130:2845–2856. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Tanner M, Hollmén M, Junttila TT, et al:
Amplification of HER-2 in gastric carcinoma: association with
Topoisomerase IIalpha gene amplification, intestinal type, poor
prognosis and sensitivity to trastuzumab. Ann Oncol. 16:273–278.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Bang YJ, Van Cutsem E, Feyereislova A, et
al: ToGA Trial Investigators: Trastuzumab in combination with
chemotherapy versus chemotherapy alone for treatment of
HER2-positive advanced gastric or gastro-oesophageal junction
cancer (ToGA): a phase 3, open-label, randomised controlled trial.
Lancet. 376:687–697. 2010. View Article : Google Scholar
|
|
7.
|
Weinberg RA: The retinoblastoma protein
and cell cycle control. Cell. 81:323–330. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Yan B, Yau EX, Bte Omar SS, et al: A study
of HER2 gene amplification and protein expression in gastric
cancer. J Clin Pathol. 63:839–842. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Grabsch H, Sivakumar S, Gray S, Gabbert HE
and Müller W: HER2 expression in gastric cancer: Rare,
heterogeneous and of no prognostic value - conclusions from 924
cases of two independent series. Cell Oncol. 32:57–65.
2010.PubMed/NCBI
|
|
10.
|
Dreznik A, Purim O, Idelevich E, et al:
Gastric cancer: biology and clinical manifestations in Israel. J
Surg Oncol. 105:316–322. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Giuffrè G, Ieni A, Barresi V, Caruso RA
and Tuccari G: HER2 status in unusual histological variants of
gastric adenocarcinomas. J Clin Pathol. 65:237–241. 2012.PubMed/NCBI
|
|
12.
|
Hofmann M, Stoss O, Shi D, et al:
Assessment of a HER2 scoring system for gastric cancer: results
from a validation study. Histopathology. 52:797–805. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Rüschoff J, Dietel M, Baretton G, et al:
HER2 diagnostics in gastric cancer-guideline validation and
development of standardized immunohistochemical testing. Virchows
Arch. 457:299–307. 2010.PubMed/NCBI
|
|
14.
|
Rüschoff J, Hanna W, Bilous M, et al: HER2
testing in gastric cancer: a practical approach. Mod Pathol.
25:637–650. 2012.PubMed/NCBI
|
|
15.
|
Feakins RM, Nickols CD, Bidd H and Walton
SJ: Abnormal expression of pRb, p16, and cyclin D1 in gastric
adenocarcinoma and its lymph node metastases: relationship with
pathological features and survival. Hum Pathol. 34:1276–1282. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Kishimoto I, Mitomi H, Ohkura Y, Kanazawa
H, Fukui N and Watanabe M: Abnormal expression of p16(INK4a),
cyclin D1, cyclin-dependent kinase 4 and retinoblastoma protein in
gastric carcinomas. J Surg Oncol. 98:60–66. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Werner M, Chott A, Fabiano A and Battifora
H: Effect of formalin tissue fixation and processing on
immunohistochemistry. Am J Surg Pathol. 24:1016–1019. 2000.
View Article : Google Scholar : PubMed/NCBI
|