Introduction
Gastric carcinoma is one of the most deadly types of
cancer worldwide (1,2), especially in China (3). Despite making advances in treatment
and putting effort into research over the past few decades, the
outcome of gastric cancer remains unsatisfactory, and the overall
5-year survival rate of advanced gastric adenocarcinoma patients is
low. Therefore, improvement in the therapy of gastric cancer now
depends on improving our understanding of the complex molecular
mechanisms governing the progression and aggressiveness of the
disease. Uncontrolled proliferation, invasion and metastasis as a
whole is a major poor prognostic factor for advanced gastric cancer
(4). It is well known that there is
a close correlation between inflammation and cancer; early in 1863,
Virchow hypothesized that the origin of cancer was at sites of
chronic inflammation (5).
Non-resolving inflammation plays a critical role in the development
and progression of gastric cancer (6,7),
including in the dialectical correlation between inflammation and
tumor progression, chemokine receptors and their ligands, an
important class of non-resolving inflammatory factors, are involved
in carcinogenic, proliferative, growth, invasive, metastatic and
drug resistance processes (8–11).
C-X-C chemokine receptor types 1/2 (CXCR1/2) belong
to the chemokine receptor family, which consists of G
protein-coupled receptors containing 7 transmembrane domains.
CXCR1/2 are receptors for interleukin-8 (IL-8) and transduce the
signal through a G protein-activating second messenger system.
CXCR1 and CXCR2 proteins have a single poly-peptide chain which is
350 and 355 or 360 amino acids in length, respectively, which share
76% amino acid identity to one another with the highest homology
over the membrane-spanning regions and significant divergence at
both N- and C-termini (12,13). CXCR1/2 are expressed mainly on
neutrophils and were originally characterized by their ability to
induce the chemotaxis of leukocytes. Recently, it was found that
CXCR1/2 are overexpressed in numerous solid tumors, and the studies
revealed a close correlation with proliferation, angiogenesis,
invasion, metastasis and drug resistance of the tumor (14–19).
Although there have been some studies on CXCR1/2 in several cancer
types and there have been a few reports on the role of CXCR1/2 in
gastric carcinoma (20), to date,
the significance of CXCR1/2 expression in gastric cancer
progression has not been evaluated in detail.
To determine the functional role of CXCR1/2 in the
progression of gastric carcinoma, based on the literature review
and our previous study (21), in
the present study, we investigated CXCR1/2 expression in tumors of
patients diagnosed with primary gastric carcinoma and in
corresponding non-neoplastic mucosa. We preliminarily discuss the
correlation between the immunohistochemical expression of CXCR1/2
and clinicopathological features, phosphorylation of ERK1/2 and AKT
and the expression of relevant indicators of proliferation, growth
and apoptosis (Bcl-2, Bax, Cyclin D1, EGFR and Ki-67), angiogenesis
(VEGF and CD34), invasion and metastasis (MMP-9, MMP-2, TIMP-2 and
E-cadherin).
Materials and methods
Patients and specimens
This study was conducted on 69 primary and sporadic
gastric adenocarcinoma tissue samples and their corresponding
non-neoplastic mucosa specimens retrieved from the archives at the
Department of Pathology of Xiang-ya Hospital of Central South
University (Changsha, China) between 2008 and 2010. The protocol
followed the ethical guidelines of the Declaration of Helsinki, and
informed consent was obtained from all patients before the study.
No patients had received chemotherapy or radiotherapy prior to
surgery. Tissue blocks of non-neoplastic mucosa (>5 cm away from
the edge of tumor) were obtained. The clinicopathological findings
were determined according to the AJCC tumor-node-metastasis (TNM)
staging system (22). The patients'
data and histopathological characteristics of the tumors are
summarized in Table I.
 | Table I.Patient data and tumor
characteristics. |
Table I.
Patient data and tumor
characteristics.
| Factor | Value |
|---|
| No. of
patients | 69 |
| Gender, n (%) | |
| Male | 55 (73.5) |
| Female) | 14 (26.5) |
| Age (years), median
(range) | 55 (31–79) |
| TNM stage, n
(%) | |
| T stage | |
| T1 | 3 (4.3) |
| T2 | 13 (18.8) |
| T3 | 36 (52.2) |
| T4 | 17 (24.6) |
| N stage | |
| N0 | 22 (31.9) |
| N1 | 21 (30.4) |
| N2 | 12 (17.4) |
| N3 | 14 (20.3) |
| Overall
stage | |
| I | 8 (11.6) |
| II | 33 (47.8) |
| III | 27 (39.1) |
| IV | 1 (1.4) |
|
Differentiation | |
| Good | 7 (10.1) |
| Moderate | 24 (34.8) |
| Poor | 38 (55.1) |
Antibodies
Phosphorylated antibodies (pAKT-Ser473,
anti-AKT, pERK-Thr202/Tyr204 and anti-ERK)
were obtained from Anbo Biotechnology Co., Ltd. (San Francisco, CA,
USA) and the following antibodies were purchased from Santa Cruz
Biotechnology, Inc. (Santa Cruz, CA, USA): CXCR1/2, Bcl-2, Bax,
Cyclin D1, EGFR, Ki-67, VEGF, CD34, MMP-9, MMP-2, TIMP-2 and
E-cadherin. The StreptAvidin Biotin Complex (SABC) kit (Wuhan
Boster Bio-Engineering Ltd. Co., China) was used according to the
manufacturer's instructions.
Immunohistochemical analysis
Immunohistochemistry (IHC) was performed as
previously described (21). More
than 10 serial thin (4 μm) sections were cut from each
paraffin block. The sections were deparaffinized and endogenous
peroxidase activity was blocked. The sections were then pre-treated
in antigen retrieval buffer (citrate buffer, pH 6.0, at 100°C, 2
min in a pressure cooker) and stained with primary antibodies
CXCR1/2, pAKT-Ser473, AKT,
pERK-Thr202/Tyr204, ERK, Bcl-2, Bax, Cyclin
D1, EGFR, Ki-67, VEGF, CD34, MMP-9, MMP-2, TIMP-2 and E-cadherin
(diluted 1:200). IgG2b-stained sections were used as negative
controls. Slides were then washed and incubated for 1 h with the
appropriate horseradish peroxidase-conjugated secondary antibody.
Diaminobenzidine (DAB) was used as the chromogen and sections were
counterstained with hematoxylin.
Clinicopathological and
immunohistochemical assessment
The tumors were staged by two observers who had no
prior knowledge of the results of the assays, according to the 7th
edition of the AJCC tumor-node-metastasis (TNM) classifications.
The immunohistochemical expression of the indicators was
independently assessed by two pathologists, without knowledge of
the clinical data. The distribution of the immunohistochemical
expression of the indicators was semi-quantitatively assessed by
estimating the proportion and intensity of positively stained tumor
cells. According to previous studies (23,24),
in brief, the adjusted Allred scoring system was applied to
evaluate each entire slide using light microscopy. First, the
proportion score (PS) was assigned using a 0-to-4 scale: 0 for 0–5%
positive tumor cells, 1 for 6–25% positive tumor cells, 2 for
26–50% positive tumor cells, 3 for 51–75% positive tumor cells and
4 for >75% positive tumor cells. The intensity score (IS) was
based on a 4-point system: 0, 1, 2 and 3 (for no, light, medium or
dark staining, respectively). The proportion and intensity scores
were added to obtain a total score. When a total score was 0 or 1,
the intensity of immunostaining in the tissue was considered
negative; the intensity was weak when a total score was between 2
and 4; and the intensity was strong when a total score was ≥5.
Clinicopathological factors, including age, gender, staging, ERK1/2
and AKT phosphorylation and the expression of indicators of
proliferation, growth and apoptosis (Bcl-2, Bax, Cyclin D1, EGFR
and Ki-67), angiogenesis (VEGF and CD34), invasion and metastasis
(MMP-9, MMP-2, TIMP-2 and E-cadherin) were analyzed for an
association with CXCR1/2 expression.
Statistical analysis
The SPSS 13.0 software system (SPSS, Inc., Chicago,
IL, USA) was used for statistical analysis. The Spearman
correlation was used, when appropriate, to analyze the significance
of the correlation between CXCR1 protein expression and tumor
characteristics, including age, gender, staging, ERK1/2 and AKT
phosphorylation and expression of indicators of proliferation,
growth and apoptosis, invasion and metastasis. Uni- and
multivariate logistic regression analysis was performed to
determine factors associated with tumor stage. P<0.05 was
considered to indicate a statistically significant result.
Results
Association between CXCR1/2 expression
and clinicopathological factors of gastric carcinoma
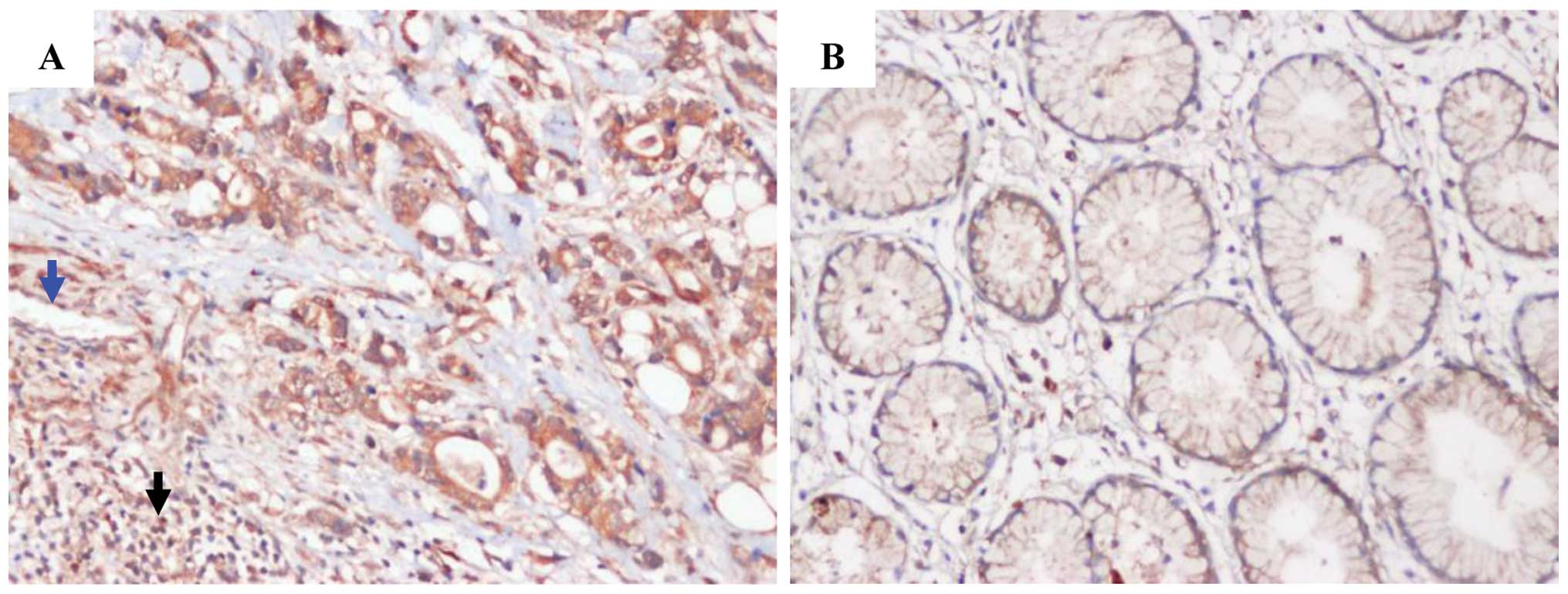
Positive staining for CXCR1/2 was shown in 68
(98.6%) of the 69 tumor specimens (Table II). CXCR1/2 showed membrane and
cytoplasmic expression in tumor cells and also in some leukocytes
and vascular endothelial cells (Fig.
1). Based on CXCR1/2 expression levels, demographic
characteristics and tumor status were analyzed (Table II). Table II shows that as CXCR1/2 expression
increased in the tumor, so did the overall tumor stage. Of 68
tumors with positive CXCR1/2 expression, 60 (88.2%) cases were
stage II, III and IV, but only 8 (11.8%) were stage I. According to
the evaluation of the CXCR1/2 immnunostaining, CXCR1/2 expression
was significantly correlated with TNM stage, T stage and N stage
(P<0.001). However, no correlation was observed between CXCR1/2
expression and gender, age and tumor differentiation.
| Table II.Association between the expression of
CXCR1/2 and clinicopathological factors of gastric carcinoma. |
Table II.
Association between the expression of
CXCR1/2 and clinicopathological factors of gastric carcinoma.
| Expression
| |
|---|
|
Characteristics | Negative (n=1) | Weak (n=45) | Strong (n=23) | P-value |
|---|
| Male:female | 0:1 | 37:8 | 18:5 | 0.452 |
| Age (years), mean ±
SD | 53.0±0 | 52.3±20.0 | 56.0±27.3 | 0.501 |
| Cancer cell
differentiation | | | | 0.357 |
| Good | 0 | 5 | 2 | |
| Moderate | 0 | 17 | 7 | |
| Poor | 1 | 23 | 14 | |
| T stage | | | | <0.001 |
| T1 | 0 | 3 | 0 | |
| T2 | 0 | 13 | 0 | |
| T3 | 1 | 20 | 15 | |
| T4 | 0 | 9 | 8 | |
| N stage | | | | <0.001 |
| N0 | 1 | 20 | 1 | |
| N1 | 0 | 17 | 4 | |
| N2 | 0 | 7 | 5 | |
| N3 | 0 | 1 | 13 | |
| Overall stage | | | | <0.001 |
| I | 0 | 8 | 0 | |
| II | 1 | 30 | 2 | |
| III | 0 | 6 | 21 | |
| IV | 0 | 1 | 0 | |
Association between expression of CXCR1/2
and indicators of phosphorylation, proliferation, growth,
apoptosis, angiogenesis, invasion and metastasis
Correlation analysis between the expression of
CXCR1/2 and the indicators of phosphorylation (AKT, ERK, pAKT and
pERK), proliferation, growth and apoptosis (Bcl-2, Bax, Cyclin D1,
EGFR and Ki-67), angiogenesis (VEGF and CD34), invasion and
metastasis (MMP-9, MMP-2, TIMP-2 and E-cadherin) using the Spearman
correlation test revealed that CXCR1/2 expression was significantly
correlated with pAKT, pERK, Cyclin D1, EGFR, Bcl-2, microvessel
density (MVD), MMP-9 and MMP-2 (P=0.032, P<0.001, P=0.049,
P=0.013, P=0.003, P=0.001, P=0.013 and P=0.027, respectively), but
CXCR1/2 and AKT, ERK, Ki-67, Bax, VEGF, TIMP-2 and E-cadherin
expression were not significantly correlated in gastric carcinoma
(Fig. 2 and Table III).
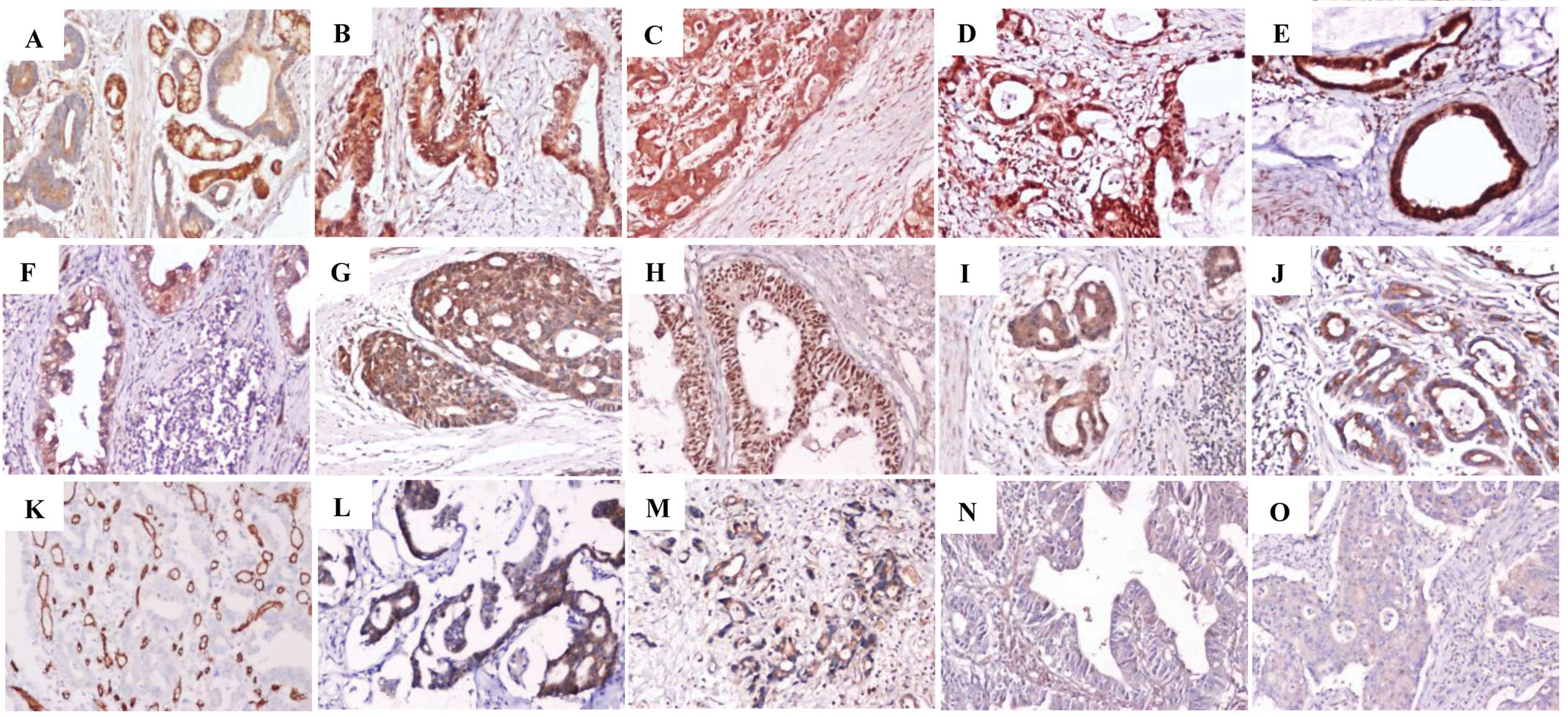 | Figure 2.In gastric carcinoma, representative
immunostaining for phosphorylation indicators: (A) AKT, (B) pAKT,
(C) ERK, (D) pERK; proliferation, growth and apoptosis indicators:
(E) Bcl-2, (F) Bax, (G) Ki-67, (H) Cyclin D1, (I) EGFR;
angiogenesis indicators: (J) VEGF, (K) CD34 to calculate
microvessel density; invasion and metastasis indicators: (L) MMP-2,
(M) MMP-9, (N) TIMP-2, (O) E-cadherin. Original magnification,
x200. IgG staining was used as a negative control. |
| Table III.Association between the expression of
CXCR1/2 and indicators of proliferation, growth, apoptosis,
angiogenesis, invasion and metastasis. |
Table III.
Association between the expression of
CXCR1/2 and indicators of proliferation, growth, apoptosis,
angiogenesis, invasion and metastasis.
| CXCR1/2 expression
| |
|---|
| Indicator
expression | Negative (n=1) | Weak (n=45) | Strong (n=23) | P-value |
|---|
|
Phosphorylation | | | | |
| AKT | | | | 0.339 |
| Negative | 0 | 5 | 0 | |
| Weak | 1 | 25 | 13 | |
| Strong | 0 | 15 | 10 | |
| pAKT | | | | 0.032 |
| Negative | 1 | 1 | 1 | |
| Weak | 0 | 15 | 6 | |
| Strong | 0 | 29 | 16 | |
| ERK | | | | 0.725 |
| Negative | 0 | 0 | 0 | |
| Weak | 1 | 9 | 6 | |
| Strong | 0 | 36 | 17 | |
| pERK | | | | <0.001 |
| Negative | 0 | 2 | 0 | |
| Weak | 1 | 19 | 1 | |
| Strong | 0 | 24 | 22 | |
| Proliferation and
growth | | | | |
| Ki-67 | | | | 0.456 |
| Negative | 1 | 6 | 5 | |
| Weak | 0 | 28 | 11 | |
| Strong | 0 | 11 | 7 | |
| Cyclin D1 | | | | 0.049 |
| Negative | 0 | 8 | 2 | |
| Weak | 1 | 32 | 13 | |
| Strong | 0 | 5 | 8 | |
| EGFR | | | | 0.013 |
| Negative | 1 | 14 | 3 | |
| Weak | 0 | 25 | 12 | |
| Strong | 0 | 6 | 8 | |
| Apoptosis | | | | |
| Bcl-2 | | | | 0.003 |
| Negative | 0 | 4 | 0 | |
| Weak | 1 | 21 | 10 | |
| Strong | 0 | 20 | 13 | |
| Bax | | | | 0.103 |
| Negative | 1 | 6 | 3 | |
| Weak | 0 | 34 | 15 | |
| Strong | 0 | 5 | 5 | |
| Angiogenesis | | | | |
| VEGF | | | | 0.678 |
| Negative | 0 | 2 | 1 | |
| Weak | 1 | 23 | 12 | |
| Strong | 0 | 20 | 10 | |
| MVD | | | | 0.001 |
| <20 | 1 | 31 | 9 | |
| ≥20 | 0 | 14 | 14 | |
| Invasion and
metastasis | | | | |
| MMP-9 | | | | 0.013 |
| Negative | 1 | 11 | 1 | |
| Weak | 0 | 29 | 16 | |
| Strong | 0 | 5 | 6 | |
| MMP-2 | | | | 0.027 |
| Negative | 1 | 14 | 6 | |
| Weak | 0 | 30 | 15 | |
| Strong | 0 | 1 | 2 | |
| TIMP-2 | | | | 0.843 |
| Negative | 0 | 24 | 11 | |
| Weak | 1 | 21 | 11 | |
| Strong | 0 | 0 | 1 | |
| E-cadherin | | | | 0.414 |
| Negative | 0 | 12 | 4 | |
| Weak | 1 | 28 | 17 | |
| Strong | 0 | 5 | 2 | |
Association between expression of pAKT
and pERK and indicators of proliferation, growth, apoptosis,
angiogenesis, invasion and metastasis
Positive immunohistochemical reaction for AKT, pAKT,
ERK and pERK in tumor cells was characterized by positive staining
in the membrane and cytoplasm (Fig.
2A–D). Based on the immnunostaining evaluation, the expression
of pAKT was significantly correlated with Ki-67, EGFR, Bcl-2, VEGF
and MMP-2 expression (P=0.001, P=0.029, P<0.001, P=0.003 and
P=0.041, respectively), but not with Cyclin D1, Bax, MVD, MMP-9,
TIMP-2 and E-cadherin expression. pERK expression was significantly
correlated with Ki-67, EGFR, Bcl-2, MMP-9 and MMP-2 expression
(P=0.013, P=0.002, P<0.001, P=0.003 and P=0.010, respectively),
and tended to correlate with Cyclin D1, Bax, MVD and TIMP-2
expression (P=0.098, P=0.081, P=0.073 and P=0.084, respectively),
but not with VEGF and E-cadherin expression (Table IV).
| Table IV.Association between the expression of
indicators of phosphorylation and those of proliferation, growth,
apoptosis, angiogenesis, invasion and metastasis. |
Table IV.
Association between the expression of
indicators of phosphorylation and those of proliferation, growth,
apoptosis, angiogenesis, invasion and metastasis.
| P-value
|
|---|
| Indicator
expression | AKT | pAKT | ERK | pERK |
|---|
| Proliferation and
growth | | | | |
| Ki-67 | 0.125 | 0.001 | 0.020 | 0.013 |
| Cyclin D1 | 0.889 | 0.349 | 0.596 | 0.098 |
| EGFR | 0.296 | 0.029 | 0.370 | 0.002 |
| Apoptosis | | | | |
| Bcl-2 | 0.051 | <0.001 | 0.003 | <0.001 |
| Bax | 0.031 | 0.451 | 0.012 | 0.081 |
| Angiogenesis | | | | |
| VEGF | 0.086 | 0.003 | 0.048 | 0.102 |
| MVD | 0.079 | 0.841 | 0.560 | 0.073 |
| Invasion and
metastasis | | | | |
| MMP-9 | 0.427 | 0.161 | 0.275 | 0.003 |
| MMP-2 | 0.572 | 0.041 | 0.086 | 0.010 |
| TIMP-2 | 0.167 | 0.456 | 0.587 | 0.084 |
| E-cadherin | 0.014 | 0.202 | 0.110 | 0.391 |
Factors associated with tumor stage
Based on a univariate analysis, CXCR1/2, pERK and
MVD expression were significantly associated with high TNM stage,
and the odds ratios (ORs) were 39.291, 5.186 and 13.383,
respectively, which suggested that cases with strong CXCR1
expression, strong ERK phosphorylation and high MVD had a 39.291-,
5.186- and 13.383-fold higher risk for high TNM stage, compared
with negative and weak CXCR1 expression and ERK phosphorylation and
low MVD, respectively. The other detected indicators were not
significantly associated with high TNM stage. The multivariate
analysis indicated that only CXCR1/2 and MVD expression were
significantly associated with high TNM stage, with ORs of 204.793
and 28.905, respectively (Table
V).
| Table V.Univariate and multivariate analyses
of clinicopathological variables and the expression of CXCR1/2 with
regard to TNM stage. |
Table V.
Univariate and multivariate analyses
of clinicopathological variables and the expression of CXCR1/2 with
regard to TNM stage.
| Univariate analysis
| Multivariate
analysis
|
|---|
| Variables | OR | 95% CI | P-value | OR | 95% CI | P-value |
|---|
| Gender (male vs.
female) | 0.754 | 0.246–2.312 | 0.062 | 0.610 | 0.074–5.053 | 0.646 |
| Age (<60 vs. ≥60
years) | 1.022 | 0.405–2.581 | 0.963 | 0.806 | 0.167–3.900 | 0.789 |
| Differentiation
(poor vs. moderate, good) | 0.570 | 0.229–1.422 | 0.228 | 0.549 | 0.108–2.804 | 0.471 |
| CXCR1/2 (negative,
weak vs. strong) | 39.291 | 9.061–169.864 | <0.001 | 204.793 |
14.850–2827.081 | <0.001 |
| pAKT (negative,
weak vs. strong) | 1.193 | 0.412–3.463 | 0.744 | 5.435 | 0.775–38.081 | 0.089 |
| pERK (negative,
weak vs. strong) | 5.186 | 1.786–15.059 | 0.002 | 2.049 | 0.336–12.516 | 0.437 |
| Ki-67 (negative,
weak vs. strong) | 1.111 | 0.400–3.089 | 0.840 | 0.849 | 0.082–8.837 | 0.891 |
| Cyclin D1
(negative, weak vs. strong) | 1.506 | 0.474–4.783 | 0.488 | 1.563 | 0.166–14.688 | 0.697 |
| EGFR (negative,
weak vs. strong) | 1.091 | 0.357–3.330 | 0.879 | 0.149 | 0.013–1.766 | 0.131 |
| Bcl-2 (negative,
weak vs. strong) | 1.560 | 0.631–3.857 | 0.336 | 3.436 | 0.481–24.582 | 0.219 |
| Bax (negative, weak
vs. strong) | 1.127 | 0.315–4.039 | 0.854 | 0.677 | 0.071–6.449 | 0.734 |
| VEGF (negative,
weak vs. strong) | 0.604 | 0.242–1.507 | 0.280 | 0.499 | 0.072–3.483 | 0.483 |
| MVD (<20 vs.
≥20) | 13.383 | 4.280–41.846 | <0.001 | 28.905 | 4.092–204.384 | 0.001 |
| MMP-9 (negative,
weak vs. strong) | 0.988 | 0.290–3.367 | 0.985 | 0.288 | 0.020–4.166 | 0.361 |
| MMP-2 (negative,
weak vs. strong) | 0.419 | 0.045–3.881 | 0.443 | 0.260 | 0.003–26.050 | 0.566 |
| E-cadherin
(negative, weak vs. strong) | 0.245 | 0.052–1.121 | 0.075 | 0.067 | 0.003–1.697 | 0.101 |
A univariate analysis showed that poor tumor
differentiation, strong CXCR1/2 expression and high MVD were
significant risk factors for T stage, with ORs of 3.534 (1/0.283),
4.039 and 3.855, respectively. Tumor differentiation, CXCR1/2,
pAKT, Ki-67 and EGFR expression were associated with high T stage
by the multivariate analysis (Table
VI). A univariate analysis indicated that CXCR1/2, pERK, EGFR
and MVD expression were significant risk factors for T stage; and
the significance of CXCR1/2, pERK, EGFR, VEGF and MVD expression
was preserved using multivariate analysis (Table VII). Taken together, strong CXCR1/2
expression is a significant risk factor for T stage, N stage and
TNM stage in gastric carcinoma.
| Table VI.Uni- and multivariate analyses of
clinicopathological variables and the expression of CXCR1/2 with
regard to T stage. |
Table VI.
Uni- and multivariate analyses of
clinicopathological variables and the expression of CXCR1/2 with
regard to T stage.
| Univariate analysis
| Multivariate
analysis
|
|---|
| Variables | OR | 95% CI | P-value | OR | 95% CI | P-value |
|---|
| Differentiation
(poor vs. moderate, good) | 0.283 | 0.108–0.745 | 0.011 | 0.268 | 0.072–0.997 | 0.049 |
| CXCR1/2 (negative,
weak vs. strong) | 4.039 | 1.448–11.257 | 0.008 | 8.101 | 1.861–35.269 | 0.005 |
| pAKT (negative,
weak vs. strong) | 1.579 | 0.614–4.063 | 0.343 | 5.382 | 1.203–24.095 | 0.028 |
| Ki-67 (negative,
weak vs. strong) | 0.396 | 0.140–1.123 | 0.081 | 0.149 | 0.026–0.843 | 0.031 |
| EGFR (negative,
weak vs. strong) | 0.451 | 0.146–1.387 | 0.165 | 0.126 | 0.020–0.787 | 0.027 |
| MVD (<20 vs.
≥20) | 3.855 | 1.448–10.433 | 0.007 | 3.040 | 0.904–10.237 | 0.072 |
| Table VII.Uni- and multivariate analyses of
clinicopathological variables and the expression of CXCR1/2 with
regard to N stage. |
Table VII.
Uni- and multivariate analyses of
clinicopathological variables and the expression of CXCR1/2 with
regard to N stage.
| Univariate analysis
| Multivariate
analysis
|
|---|
| Variables | OR | 95% CI | P-value | OR | 95% CI | P-value |
|---|
| CXCR1/2 (negative,
weak vs. strong) | 23.571 | 7.121–77.945 | <0.001 | 29.108 | 5.807–146.057 | <0.001 |
| pERK (negative,
weak vs. strong) | 5.155 | 1.910–13.902 | 0.001 | 5.523 | 1.283–23.807 | 0.022 |
| EGFR (negative,
weak vs. strong) | 2.983 | 1.012–8.802 | 0.047 | 7.243 | 1.022–51.367 | 0.048 |
| VEGF (negative,
weak vs. strong) | 0.610 | 0.257–1.449 | 0.262 | 0.106 | 0.022–0.514 | 0.005 |
| MVD (<20 vs.
≥20) | 5.686 | 2.201–14.673 | <0.001 | 6.398 | 1.779–23.035 | 0.004 |
Discussion
Previous studies have shown that cancer cells from
numerous types of cancer express higher levels of the chemokine
receptors (25–27). Chemokine receptors and their ligands
were believed to be involved in all stages of certain types of
cancer, including influencing the tumor microenvironment (28,29),
malignant cell survival and growth (30), angiogenesis (28), invasion (31) and metastasis (10,11,32). A
greater understanding of the chemokine receptor system in
malignancy would not only add to our knowledge of the pathogenesis
of cancer, but may also suggest new treatment targets for
development. CXCR1/2, members of the chemokine receptor family,
have been studied in several types of cancer, showing a close
correlation with drug resistance, survival, growth, angiogenesis,
invasion and metastasis in breast cancer (16), melanoma (17), pancreatic cancer (19,33)
and colon cancer (18). In
melanoma, knockdown of the receptors or the use of antagonists or
neutralizing antibodies against CXCR1/2 affected cell
proliferation, migration and tumor growth, strongly indicating the
involvement of these receptors in melanoma progression (34).
In gastric carcinoma there is little information
concerning the expression of CXCR1/2 proteins, which are generally
believed to play a role in tumor progression by interacting with
their ligands. In the present study, we examined CXCR1/2 protein
expression in gastric carcinoma, and CXCR1/2 expression was
immunohistochemically detected in 68 (98.6%) of the 69 tumor
specimens. The expression level of CXCR1/2 was higher in gastric
carcinoma than in the corresponding non-neoplastic mucosa in
certain cases.
Previous studies have indicated that CXCR1/2
expression is significantly correlated with invasion, metastasis
and advanced TNM stage in patients with malignant melanoma
(35) and prostate cancer (36). Our current data show that the
membrane and cytoplasmic expression of CXCR1/2 in gastric carcinoma
cells was positively correlated with advanced T stage, N stage and
overall TNM stage. T stage and N stage represent invasion and
metastasis degree, respectively (22). These data indicate that CXCR1/2 may
be involved in the invasion and metastasis of gastric carcinoma.
Univariate and multivariate analysis revealed that strong CXCR1/2
expression was a significant risk factor for T stage, N stage and
TNM stage, from which CXCR1/2 expression appears to play an
overlooked role in the development and progression of gastric
carcinoma, as does MVD. Our findings further support the hypothesis
that there is an association between CXCR1/2 expression and cancer
cell invasion and metastasis in certain cancer types (14,16,37,38).
Several studies have indicated that chemokine
receptors play multiple roles in the development and progression of
a number of tumors via various mechanisms (14,39–42).
To investigate the possible mechanisms of CXCR1/2 involvement in
the progression of gastric carcinoma, we examined the
immunohistochemical expression of ERK1/2 and AKT phosphorylation
and the expression of relevant indicators of proliferation, growth
and apoptosis (Bcl-2 and Bax, Cyclin D1, EGFR and Ki-67),
angiogenesis (VEGF and CD34), invasion and metastasis (MMP-9,
MMP-2, TIMP-2 and E-cadherin) in primary gastric carcinoma and its
corresponding nonneoplastic mucosa, which were involved in the
regulation of tumor proliferation, growth, angiogenesis, invasion
and metastasis. Evaluation of the correlation between the
expression of CXCR1/2 and the indicators using the Spearman
correlation analysis revealed that CXCR1/2 expression was
positively correlated with Cyclin D1, EGFR, Bcl-2, MVD, MMP-9 and
MMP-2. CD34 is a marker of MVD and reflects angiogenesis, which
plays an important role in the growth and invasion of tumors
(43). The cell cycle regulatory
protein Cyclin D1 may contribute to TNM classification,
histological differentiation, perineural invasion, DNA ploidy,
S-phase fraction, expression of Ki-67 and mitotic index. EGFR has
been shown to be associated with tumor proliferation and growth,
Bcl-2 inhibits tumor apoptosis and MMP-9 and MMP-2 play an
indispensable role in tumor invasion and metastasis (44,45).
Based on our results, it is possible that via the upregulation of
Cyclin D1, EGFR, Bcl-2, MMP-9 and MMP-2 expression and MVD, CXCR1/2
and their ligands are involved in mediating proliferation, growth,
angiogenesis, invasion and metastasis of gastric carcinoma.
Other studies (14,15)
have found that abnormal phosphorylation of ERK1/2 and AKT was
closely associated with proliferation, growth, angiogenesis,
invasion and metastasis of tumors, and played as an intermediary
between CXCR1/2 and their downstream molecular indicators.
Following stimulation of CXCR1/2 receptors with the ligands, for
example IL-8, heterotrimeric small G proteins are activated and
promote the activation of the primary effector, such as
phosphatidyl-inositol-3-kinase, one of the principal targets of the
CXCR1/2 subunits. Activation of the phosphatidyl-inositol-3-kinase
may result in increased phosphorylation of its substrate
serine/threonine kinase, PKB/AKT (46), promoting the activation of AKT or
MAPK signaling cascades. These signaling pathways have been shown
to promote protein translation and regulate the activity of a range
of transcription factors, and are likely to induce the
transcription of multiple genes involved in angiogenesis, cell
cycle regulation, migration, invasion and the evasion of apoptosis
(14). Increased AKT expression and
activity by CXCR1/2 receptor/ligand signaling have been detected in
multiple forms of cancer, which is consistent with poor tumor
progression (47). A study
conducted by one group suggests that CXCR1/2 receptor/ligand
signaling not only induces activation of AKT but also increases the
expression of AKT in androgen-independent prostate cancer cell
lines (48). The CXCR1/2
receptor/ligand pathway also regulates the activity of the
activation of MAPK signaling cascade, with downstream
phosphorylation of ERK1/2 detected in cancer cells (48–50).
Certain studies conducted in ovarian and lung cancer cell lines
showed that the CXCR1/2 receptor/ligand pathway transactivates
EGFR, promoting the downstream activation of MAPK signaling and
mediating cell proliferation and survival (49,50).
Our data showed that strong CXCR1/2 expression was positively
associated with the phosphorylation of AKT and ERK. Further
analysis indicated that the expression of pAKT was significantly
correlated with Ki-67, EGFR, Bcl-2, VEGF and MMP-2 expression, and
pERK expression was significantly correlated with Ki-67, EGFR,
Bcl-2, MMP-9 and MMP-2 expression and tended to correlate with
Cyclin D1, Bax, MVD and TIMP-2 expression. Therefore, these
results, to a certain extent, suggest that CXCR1/2 receptor/ligand
signaling plays a significant role in the progression of gastric
carcinoma by means of ERK1/2 and AKT phosphorylation, two important
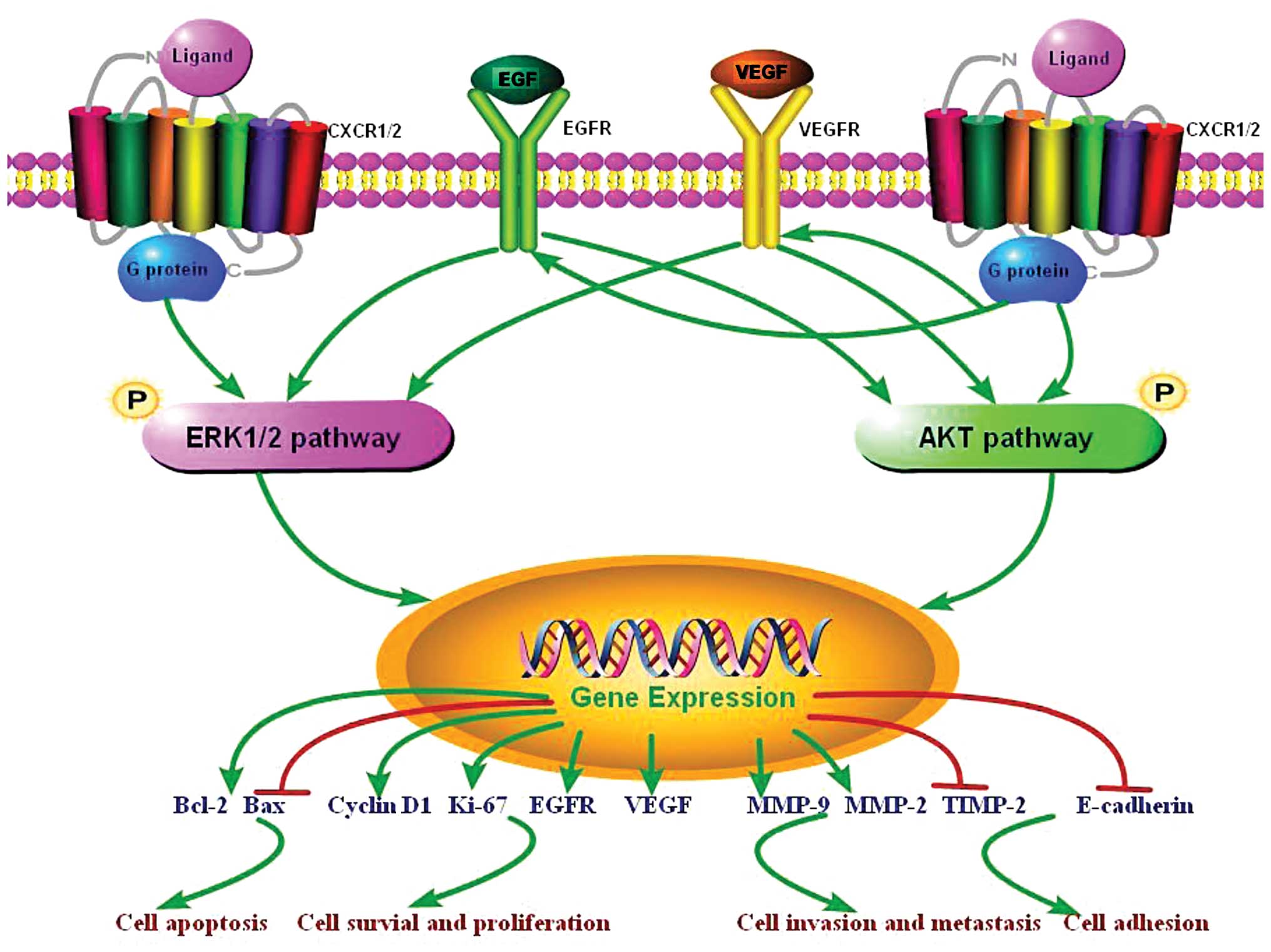
pathways (Fig. 3).
In conclusion, the results of the current study
suggest that the overexpression of CXCR1/2 was associated with the
malignant progression of gastric carcinoma, and simultaneously with
the expression of certain indicators of phosphorylation,
proliferation, growth, apoptosis, angiogenesis, invasion and
metastasis. It is possible that CXCR1/2, interacting with their
ligands, activate ERK1/2 and AKT phosphorylation, which in turn
mediates the expression of indicators of proliferation, growth,
apoptosis, angiogenesis, invasion and metastasis; and activation of
the signaling pathway results in poor progression of gastric
carcinoma (Fig. 3). Therefore,
CXCR1/2 may be a useful predictive marker and promising therapeutic
target in gastric carcinoma. Further research is required to
confirm the relevance of CXCR1/2 expression to gastric carcinoma
progression in vitro and in vivo.
Acknowledgements
This study was partially supported by
the Hunan Provincial Innovation Foundation For Postgraduates (No.
CX2011B046), the Graduate Degree Thesis Innovation Foundation of
Central South University (No. 2009ssxt062), the Science and
Technology Program Foundation of Changsha City (Nos. K1005005-31
and K1106041-31), the Open-end Fund for the Valuable and Precision
Instruments of Central South University, the Key Program of Natural
Science Fund of Hunan Province (No. 09JJ3040) and the National
Natural Science Fund of China (No. 81001080).
References
|
1.
|
Ferlay J, Shin HR, Bray F, Forman D,
Mathers C and Parkin DM: GLOBOCAN 2008 v2.0, Cancer Incidence and
Mortality Worldwide: IARC CancerBase No 10 [Internet]. Lyon,
France: International Agency for Research on Cancer; 2010,
http://globocan.iarc.fr.
accessed on February 27, 2012.
|
|
2.
|
Alberts SR, Cervantes A and van de Velde
CJ: Gastric cancer: epidemiology, pathology and treatment. Ann
Oncol. 14(Suppl 2): ii31–36. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Yang L: Incidence and mortality of gastric
cancer in China. World J Gastroenterol. 12:17–20. 2006.
|
|
4.
|
Hyung WJ, Noh SH, Yoo CH, et al:
Prognostic significance of metastatic lymph node ratio in T3
gastric cancer. World J Surg. 26:323–329. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Balkwill F and Mantovani A: Inflammation
and cancer: back to Virchow? Lancet. 357:539–545. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Nathan C and Ding A: Nonresolving
inflammation. Cell. 140:871–882. 2010. View Article : Google Scholar
|
|
7.
|
Mantovani A: Cancer: Inflaming metastasis.
Nature. 457:36–37. 2009. View
Article : Google Scholar
|
|
8.
|
Righi E, Kashiwagi S, Yuan J, et al:
CXCL12/CXCR4 blockade induces multimodal antitumor effects that
prolong survival in an immunocompetent mouse model of ovarian
cancer. Cancer Res. 71:5522–5534. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Wendel C, Hemping-Bovenkerk A, Krasnyanska
J, et al: CXCR4/CXCL12 participate in extravasation of
metastasizing breast cancer cells within the liver in a rat model.
PLoS One. 7:e300462012. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Balkwill FR: The chemokine system and
cancer. J Pathol. 226:148–157. 2012. View Article : Google Scholar
|
|
11.
|
Lazennec G and Richmond A: Chemokines and
chemokine receptors: new insights into cancer-related inflammation.
Trends Mol Med. 16:133–144. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Murphy PM: The molecular biology of
leukocyte chemoattractant receptors. Annu Rev Immunol. 12:593–633.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Kelvin DJ, Michiel DF, Johnston JA, et al:
Chemokines and serpentines: the molecular biology of chemokine
receptors. J Leukoc Biol. 54:604–612. 1993.PubMed/NCBI
|
|
14.
|
Waugh DJ and Wilson C: The interleukin-8
pathway in cancer. Clin Cancer Res. 14:6735–6741. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Zhang Y, Wang L, Zhang M, Jin M, Bai C and
Wang X: Potential mechanism of interleukin-8 production from lung
cancer cells: an involvement of EGF-EGFR-PI3K-Akt-Erk pathway. J
Cell Physiol. 227:35–43. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Ginestier C, Liu S, Diebel ME, et al:
CXCR1 blockade selectively targets human breast cancer stem cells
in vitro and in xenografts. J Clin Invest. 120:485–497. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Singh S, Nannuru KC, Sadanandam A, Varney
ML and Singh RK: CXCR1 and CXCR2 enhances human melanoma
tumourigenesis, growth and invasion. Br J Cancer. 100:1638–1646.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Varney ML, Singh S, Li A, Mayer-Ezell R,
Bond R and Singh RK: Small molecule antagonists for CXCR2 and CXCR1
inhibit human colon cancer liver metastases. Cancer Lett.
300:180–188. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Matsuo Y, Raimondo M, Woodward TA, et al:
CXC-chemokine/CXCR2 biological axis promotes angiogenesis in vitro
and in vivo in pancreatic cancer. Int J Cancer. 125:1027–1037.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Eck M, Schmausser B, Scheller K, Brändlein
S and Müller-Hermelink HK: Pleiotropic effects of CXC chemokines in
gastric carcinoma: differences in CXCL8 and CXCL1 expression
between diffuse and intestinal types of gastric carcinoma. Clin Exp
Immunol. 134:508–515. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Wang JP, Hu WM, Wang KS, et al:
Upregulation of C-X-C chemokine receptor type 1 expression is
associated with late-stage gastric adenocarcinoma. Exp Ther Med.
4:55–60. 2012.PubMed/NCBI
|
|
22.
|
Washington K: 7th edition of the AJCC
cancer staging manual: stomach. Ann Surg Oncol. 17:3077–3079. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Allred DC, Harvey JM, Berardo M and Clark
GM: Prognostic and predictive factors in breast cancer by
immunohistochemical analysis. Mod Pathol. 11:155–168.
1998.PubMed/NCBI
|
|
24.
|
Harvey JM, Clark GM, Osborne CK and Allred
DC: Estrogen receptor status by immunohistochemistry is superior to
the ligand-binding assay for predicting response to adjuvant
endocrine therapy in breast cancer. J Clin Oncol. 17:1474–1481.
1999.PubMed/NCBI
|
|
25.
|
Raman D, Baugher PJ, Thu YM and Richmond
A: Role of chemokines in tumor growth. Cancer Lett. 256:137–165.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Ali S and Lazennec G: Chemokines: novel
targets for breast cancer metastasis. Cancer Metastasis Rev.
26:401–420. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27.
|
Vindrieux D, Escobar P and Lazennec G:
Emerging roles of chemokines in prostate cancer. Endocr Relat
Cancer. 16:663–673. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28.
|
Orimo A, Gupta PB, Sgroi DC, et al:
Stromal fibroblasts present in invasive human breast carcinomas
promote tumor growth and angiogenesis through elevated SDF-1/CXCL12
secretion. Cell. 121:335–348. 2005. View Article : Google Scholar
|
|
29.
|
Colmone A, Amorim M, Pontier AL, Wang S,
Jablonski E and Sipkins DA: Leukemic cells create bone marrow
niches that disrupt the behavior of normal hematopoietic progenitor
cells. Science. 322:1861–1865. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30.
|
Singh S, Varney M and Singh RK: Host
CXCR2-dependent regulation of melanoma growth, angiogenesis, and
experimental lung metastasis. Cancer Res. 69:411–415. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
31.
|
Kitamura T, Kometani K, Hashida H, et al:
SMAD4-deficient intestinal tumors recruit CCR1+ myeloid cells that
promote invasion. Nat Genet. 39:467–475. 2007.
|
|
32.
|
Buonamici S, Trimarchi T, Ruocco MG, et
al: CCR7 signalling as an essential regulator of CNS infiltration
in T-cell leukaemia. Nature. 459:1000–1004. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
33.
|
Maxwell PJ, Gallagher R, Seaton A, et al:
HIF-1 and NF-kappa B-mediated upregulation of CXCR1 and CXCR2
expression promotes cell survival in hypoxic prostate cancer cells.
Oncogene. 26:7333–7345. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34.
|
Varney ML, Li A, Dave BJ, Bucana CD,
Johansson SL and Singh RK: Expression of CXCR1 and CXCR2 receptors
in malignant melanoma with different metastatic potential and their
role in interleukin-8 (CXCL-8)-mediated modulation of metastatic
phenotype. Clin Exp Metastasis. 20:723–731. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
35.
|
Varney ML, Johansson SL and Singh RK:
Distinct expression of CXCL8 and its receptors CXCR1 and CXCR2 and
their association with vessel density and aggressiveness in
malignant melanoma. Am J Clin Pathol. 125:209–216. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
36.
|
Murphy C, McGurk M, Pettigrew J, et al:
Nonapical and cytoplasmic expression of interleukin-8, CXCR1, and
CXCR2 correlates with cell proliferation and microvessel density in
prostate cancer. Clin Cancer Res. 11:4117–4127. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
37.
|
Müller A, Homey B, Soto H, et al:
Involvement of chemokine receptors in breast cancer metastasis.
Nature. 410:50–56. 2001.PubMed/NCBI
|
|
38.
|
Tanaka T, Bai Z, Srinoulprasert Y, Yang
BG, Hayasaka H and Miyasaka M: Chemokines in tumor progression and
metastasis. Cancer Sci. 96:317–322. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
39.
|
Koizumi K, Hojo S, Akashi T, Yasumoto K
and Saiki I: Chemokine receptors in cancer metastasis and cancer
cell-derived chemokines in host immune response. Cancer Sci.
98:1652–1658. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
40.
|
Balakin KV, Ivanenkov YA, Tkachenko SE,
Kiselyov AS and Ivachtchenko AV: Regulators of chemokine receptor
activity as promising anticancer therapeutics. Curr Cancer Drug
Targets. 8:299–340. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
41.
|
Ruffini PA, Morandi P, Cabioglu N,
Altundag K and Cristofanilli M: Manipulating the
chemokine-chemokine receptor network to treat cancer. Cancer.
109:2392–2404. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
42.
|
Kakinuma T and Hwang ST: Chemokines,
chemokine receptors, and cancer metastasis. J Leukoc Biol.
79:639–651. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
43.
|
Gabellini C, Trisciuoglio D, Desideri M,
et al: Functional activity of CXCL8 receptors, CXCR1 and CXCR2, on
human malignant melanoma progression. Eur J Cancer. 45:2618–2627.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
44.
|
Roomi MW, Monterrey JC, Kalinovsky T, Rath
M and Niedzwiecki A: Comparative effects of EGCG, green tea and a
nutrient mixture on the patterns of MMP-2 and MMP-9 expression in
cancer cell lines. Oncol Rep. 24:747–757. 2010.PubMed/NCBI
|
|
45.
|
Roomi MW, Monterrey JC, Kalinovsky T, Rath
M and Niedzwiecki A: Patterns of MMP-2 and MMP-9 expression in
human cancer cell lines. Oncol Rep. 21:1323–1333. 2009.PubMed/NCBI
|
|
46.
|
Knall C, Worthen GS and Johnson GL:
Interleukin 8-stimulated phosphatidylinositol-3-kinase activity
regulates the migration of human neutrophils independent of
extracellular signal-regulated kinase and p38 mitogen-activated
protein kinases. Proc Natl Acad Sci USA. 94:3052–3057. 1997.
View Article : Google Scholar
|
|
47.
|
Cheng GZ, Park S, Shu S, et al: Advances
of AKT pathway in human oncogenesis and as a target for anti-cancer
drug discovery. Current Cancer Drug Targets. 8:2–6. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
48.
|
MacManus CF, Pettigrew J, Seaton A, et al:
Interleukin-8 signaling promotes translational regulation of cyclin
D in androgen-independent prostate cancer cells. Mol Cancer Res.
5:737–748. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
49.
|
Venkatakrishnan G, Salgia R and Groopman
JE: Chemokine receptors CXCR-1/2 activate mitogen-activated protein
kinase via the epidermal growth factor receptor in ovarian cancer
cells. J Biol Chem. 275:6868–6875. 2000. View Article : Google Scholar
|
|
50.
|
Luppi F, Longo AM, de Boer WI, Rabe KF and
Hiemstra PS: Interleukin-8 stimulates cell proliferation in
non-small cell lung cancer through epidermal growth factor receptor
transactivation. Lung Cancer. 56:25–33. 2007. View Article : Google Scholar : PubMed/NCBI
|