Introduction
Clear cell renal carcinoma (RCC) is a rare tumor
accounting for 3% of all malignancies in adults and 85% of primary
renal tumors (1). Currently, its
incidence is on the increase due to the increased number of
incidental findings in imaging tests (2). RCC frequently metastasizes in the
lungs, bones, lymph nodes and liver. Gallbladder metastasis is
extremely rare, being found in approximately 0.6% of cases at
autopsy (3). We report a case of
gallbladder and metachronous contralateral adrenal metastasis. The
study was approved by the ethics committee of La Fe University
Hospital, and consent was obtained from the patient.
Case report
A 75-year-old female was incidentally diagnosed with
right RCC following radiological tests requested for benign
anorectal disease in March 2010. Computed tomography (CT) revealed
a right renal mass of 11.3×8.6×12.2 cm with areas of necrosis,
calcification, increased neovascularization and exophytic growth
towards the liver. In addition, lymph nodes were detected in the
renal hilum and retroperitoneum, with uncertain infiltration of the
renal vein and inferior vena cava without distant metastases. The
tumor markers CEA and CA19.9 were within the normal range. A
radical right nephrectomy was carried out through a right subcostal
incision without demonstrable vascular invasion or metastases
intraoperatively. Macroscopically, the renal lesion was yellowish
in appearance, with undefined limits and a confluent nodular
pattern with fibrous areas.
The patient's postoperative course was uneventful
and systemic adjuvant therapy was not administered. The
pathological study revealed a typical RCC with a solid growth
pattern without invasion of the renal pelvic wall and tumor
thrombosis in the renal vein. Surgical margins were tumor-free and
all lymph nodes dissected were free of tumor infiltration, with
stage pT3N0M0.
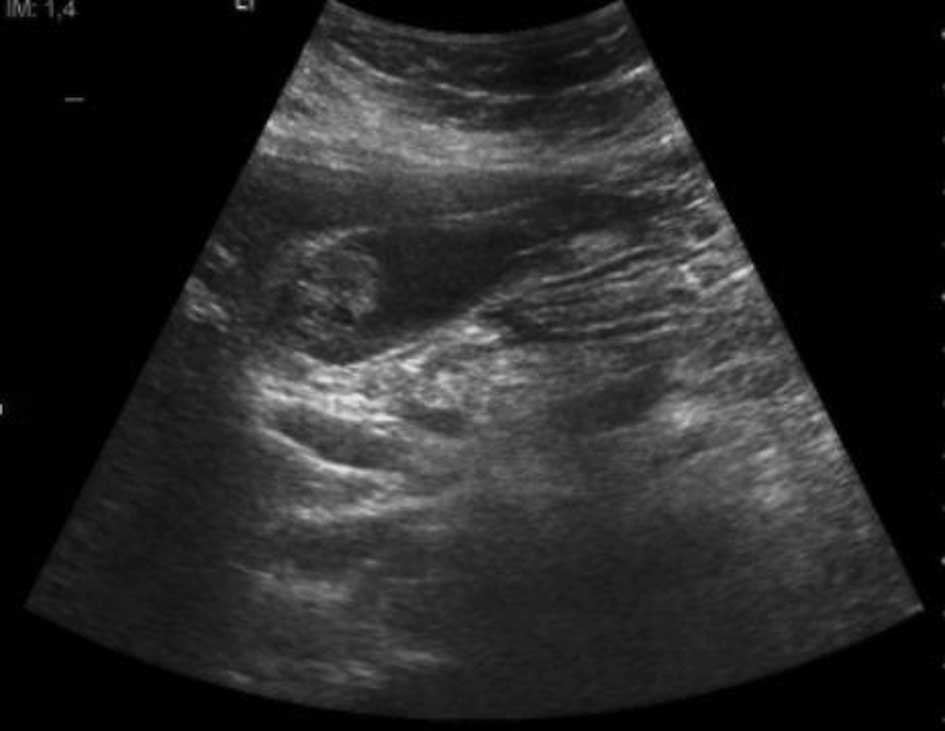
A CT scan was performed at 6 months which showed a
nodular lesion of 3 cm in the left adrenal gland and a lobulated
lesion in the gallbladder wall, with the suspected diagnosis of
metastasis. Ultrasonography (US) revealed a heterogeneous solid
nodular structure of 2 cm with poor delineation of the gallbladder
wall. It was not possible to exclude infiltration of the liver
parenchyma (Fig. 1). The extension
study was completed with a thoracic CT, which revealed no
pathological findings. Tumor markers were also within normal
ranges.
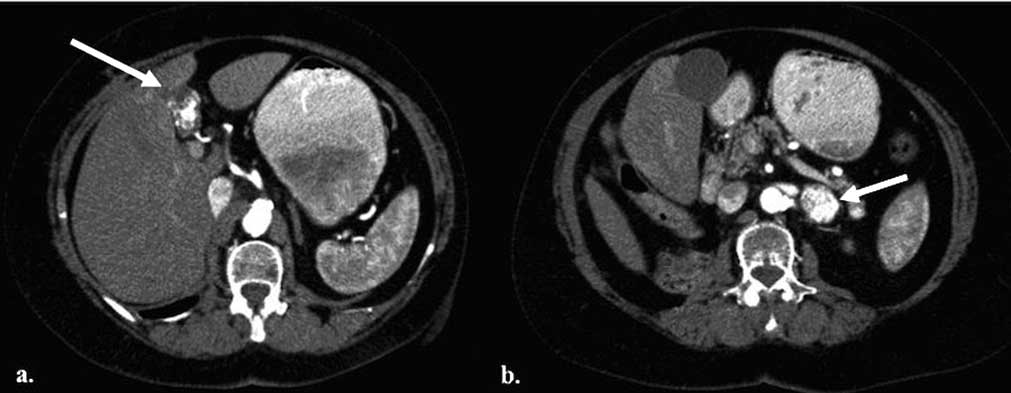
A midline laparotomy was carried out and the patient
underwent left adrenalectomy and cholecystectomy, with no
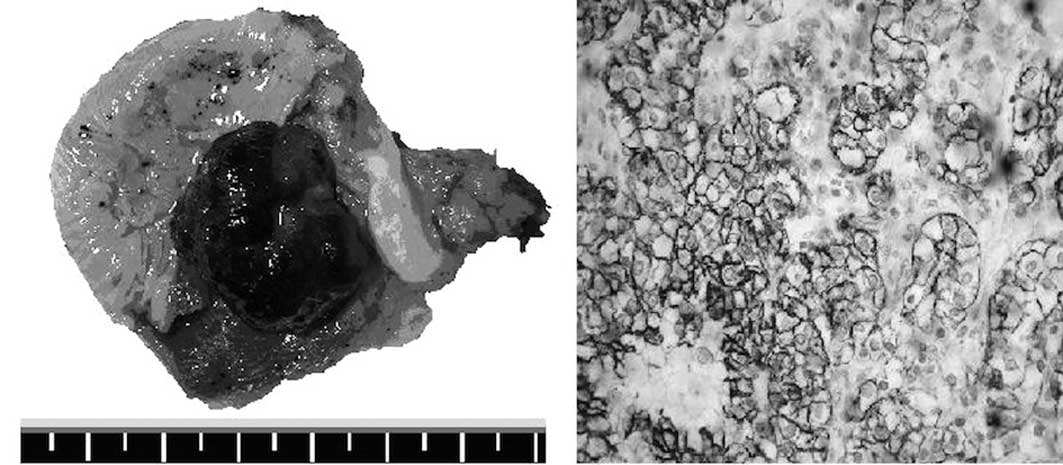
complications during the postoperative period (Fig. 2). There was a polypoid lesion of the
gallbladder without infiltration of the wall and the left adrenal
nodule had a yellowish appearance with areas of cystic hemorrhage
(Fig. 3A). Histological examination
of the two specimens showed metastases of RCC.
At present, the patient is receiving corticosteroid
replacement therapy with no adjuvant treatment. A CT scan four
months after the surgery showed no signs of recurrence.
Discussion
Metastatic gallbladder lesions are infrequent;
melanoma, stomach, pancreas, ovary, small bowel, biliary duct and
breast carcinomas are those that have the highest probability of
metastasis (4). Half of the cases
are synchronic. However, RCC is the primary renal tumor that
metastasizes most frequently in the gallbladder (5).
Clinical findings are not specific enough to arrive
at a final diagnosis. Primary tumors prevail in women over 65 years
of age with biliary lithiasis (6).
Metastatic tumors usually appear in 39 to 84-year-old males, who
have a personal history of cancer without previous biliary
pathology (4).
Imaging diagnosis may not be conclusive in making a
differential diagnosis between primary and secondary tumors. US is
the initial approach in the diagnosis of gallbladder tumors, and
this may be further improved with contrast US. Metastases can
appear under different hyperechoic masses bigger than 1 cm in
diameter, close to the gallbladder wall without posterior acoustic
shadowing (7). In primary tumors, a
solid mass is observed, occupying the entire wall thickness, or a
polypoid lesion with increased vascularization (8). A radiological finding that can help to
differentiate between a primary gallbladder tumor and metastasis in
the CT scan is the invasion of the mucosal layer. If the mucosa is
not infiltrated, indicating an invasion from the serosa layer, the
primary gallbladder tumor can be excluded. In tumoral gallbladder
invasion by contiguous tumors, a great mass without clear limits is
observed (7).
There is no evidence to suggest any benefit from
using positron emission tomography-computed tomography (PET-CT) to
detect gallbladder metastases, which may be due to the low number
of cases reported (9). The utility
of this test for future diagnoses and follow-up should be
validated.
The specific diagnosis of polypoid gallbladder
masses is problematic. It is necessary to make differential
diagnosis between cholesterol polyps, gallbladder clear cell tumor,
carcinoid and paragangliomes (4).
Immunohistochemistry is also necessary to differentiate between
primary and secondary metastatic tumors. In primary tumors,
extremely high CEA and CK7 levels, and moderately raised levels of
CK10 are found, with an absence of vimentin. Moreover, in the case
of RCC metastases, we find high vimentin levels, whereas CK7
testing yields negative results (Fig.
3B) (3).
In all gallbladder findings with suspected
malignancy, or benign lesions larger than 1 cm, a cholecystectomy
should be performed to obtain a definitive diagnosis (5). Cholecystectomy with R0 resection has
been demonstrated to be the only factor that increases survival,
mainly in isolated cases of metastasis (4,10).
Acute cholecystitis as a clinical presentation is associated with
poor prognosis (10).
The five-year survival rate following
cholecystectomy for RCC is 35–50%. According to Chung et al
(5), 63% of patients with one
gallbladder metastasis have a two-year survival, while in the case
of multiple metastases this rate decreases to 23% following
cholecystectomy. In conclusion, gallbladder metastasis of RCC
tumors is a rare entity, but should be borne in mind in the case of
diagnosis of a gallbladder lesion during the diagnosis and/or
follow-up of a primary tumor. Although radiological tests may raise
clinical suspicion, a cholecystectomy should be carried out to
determine the definitive diagnosis and improve survival.
References
|
1
|
Choi JB, Yoon BI, Kim SJ, Cho HJ, Hong SH,
Choi YJ, Kim SW, Hwang TK and Lee JY: Changes in
clinicopathological characteristics of renal cell carcinoma in the
past 25 years: a single-center experience. Korean J Urol.
52:110–114. 2011.PubMed/NCBI
|
|
2
|
Kim WJ, Chung JI, Hong JH, Kim CS, Jung SI
and Yoon DK: Epidemiological study for urologic cancer in Korea
(1998–2002). Korean J Urol. 45:1081–1088. 2004.
|
|
3
|
Nojima H, Cho A, Yamamoto H, Nagata M,
Takiguchi N, Kainuma O, Souda H, Gunji H, Miyazaki A, Ikeda A, et
al: Renal cell carcinoma with unusual metastasis to the
gallbladder. J Hepatobiliary Pancreat Surg. 15:209–212. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Fang X, Gupta N, Shen SS, Tamboli P,
Charnsangavej C, Rashid A and Wang H: Intraluminal polypoid
metastasis of renal cell carcinoma in gallbladder mimicking
gallbladder polyp. Arch Pathol Lab Med. 134:1003–1009.
2010.PubMed/NCBI
|
|
5
|
Chung PH, Srinivasan R, Linehan WM, Pinto
PA and Bratslavsky G: Renal cell carcinoma with metastases to the
gallbladder: Four cases from the National Cancer Institute and
review of the literature. Urol Oncol. 28:2011.(Epub ahead of
print).
|
|
6
|
Limani K, Matos C, Hut F, Gelin M and
Closset J: Metastatic carcinoma of the gallbladder after a renal
cell carcinoma. Acta Chir Belg. 103:233–234. 2003.PubMed/NCBI
|
|
7
|
Barretta ML, Catalano O, Setola SV,
Granata V, Marone U and D'Errico Gallipoli A: Gallbladder
metastasis: spectrum of imaging findings. Abdom Imaging.
36:729–734
|
|
8
|
Xie XH, Xu HX, Xie XY, Lu MD, Kuang M, Xu
ZF, Liu GJ, Wang Z, Liang JY, Chen LD and Lin MX: Differential
diagnosis between benign and malignant gallbladder diseases with
real-time contrast-enhanced ultrasound. Eur Radiol. 20:239–248.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kawahara T, Ohshiro H, Sekiguchi Z, Furuya
M, Namura K, Itoh H, Sano F, Kawaji K, Hayashi N, Makiyama K, et
al: Gallbladder metastasis from renal cell carcinoma. Case Rep
Oncol. 29:30–34. 2010. View Article : Google Scholar
|
|
10
|
Yoon WJ, Yoon YB, Kim YJ, Ryu JK and Kim
YT: Metastasis to the gallbladder: a single-center experience of 20
cases in South Korea. World J Gastroenterol. 15:4806–4809. 2009.
View Article : Google Scholar : PubMed/NCBI
|