Introduction
Certain types of soft tissue tumor are positive for
CD99. CD99 is a membranous protein that is expressed in most cases
of Ewing sarcoma (EWS), synovial sarcoma (SS) and low-grade
fibromyxoid sarcoma (LGFMS), although its involvement in these
diseases is unknown. However, knocking down CD99 expression in
human EWS cell lines reduced their ability to form tumors and bone
metastases when xenografted into immunodeficient mice, and
diminished their tumorigenic characteristics in vitro
(1). Therefore, CD99 may be a
marker of aggressiveness. Some of these cancer types have a
well-known specific chromosomal translocation, such as t(11;22) in
EWS, or t(18;X) in SS (2,3). However, this is the first case of
CD99-positive soft tissue sarcoma with t(1;16) and inv(5).
This study was approved by the local Ethics
Committee of the University of Toyama. The patient was informed
that his data would be submitted for publication, and gave
consent.
Case report
The patient was a 31-year-old Japanese male with
normal growth and development who presented with a mass located on
the right thigh. He had noted a rapidly enlarging mass two months
previously. On examination, there was a 15×13 cm firm and
non-tender tumor of the postero-medial thigh. The clinical history
of the patient was normal.
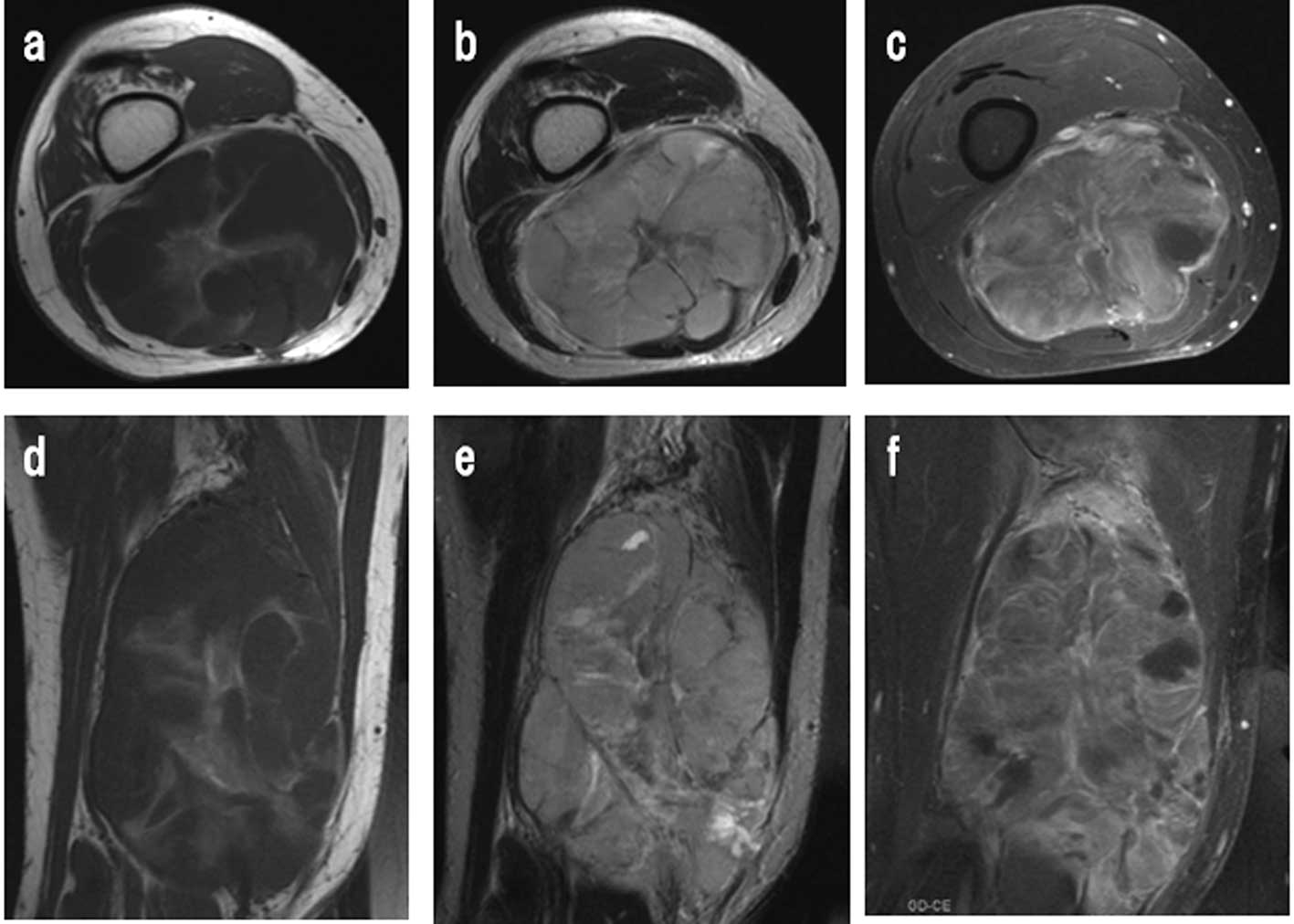
Radiographs showed a non-mineralized soft tissue
mass without bone involvement. T1- and T2-weighted MRI revealed a
multi-lobulated heterogeneous large mass involving most of the
flexor muscles, suggestive of a soft tissue sarcoma (Fig. 1). An angiogram revealed the
hypervascularity of the tumor (Fig.
2). No other tumor or inguinal lymphadenopathy was present.
Distal neurovascular examination was normal and laboratory findings
were almost normal.
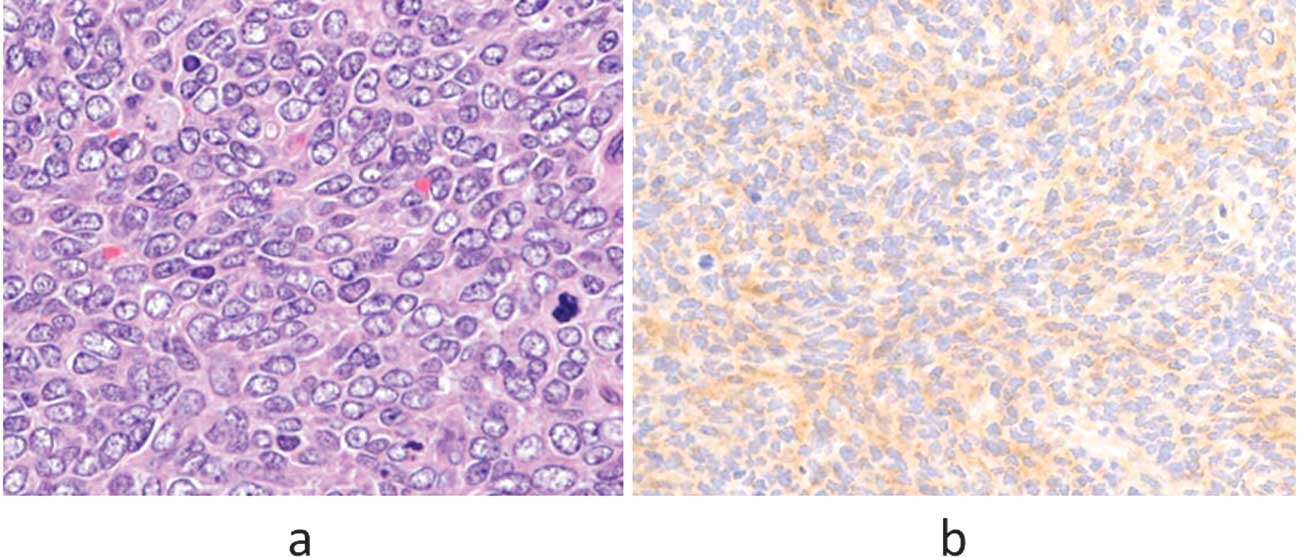
A needle biopsy of the tumor was carried out and the
pathology was reviewed to be unclassified high-grade sarcoma
(Fig. 3). The tumor was then
surgically removed. However, the evaluation of the resected margin
of the tumor was intralesional, since the mass had existed in the
intermuscular space and lacked any capsule. Gross appearance of the
resected specimen showed a non-capsulated, soft-to-firm,
tan-to-pink mass (15 cm in maximum dimension) with foci of cysts
and hemorrhage.
Microscopically, the tumor was composed of
well-formed and variably sized vessels with proliferative ovoid or
short- spindle atypical cells. Numerous mitotic figures were
present. The tumor cells were immunoreactive to CD99, vimentin, and
bcl-2. However, they had no reactivity to desmin, S-100, CD34,
AE1/AE3, EMA and CK7.
Following surgery, the patient repeatedly received
intensive multidrug chemotherapy, including combination
chemotherapy VDC (vincristine 2 mg/day, doxorubicin 50 mg/day × 2
days, and cyclophosphamide 1800 mg/day), IE (ifosfamide 3 g × 3
days, etoposide 100 mg/day × 3 days) and MAID (doxorubicin 30
mg/day, ifosfamide 3 g/day, dacarbazine 450 mg/day) × 3 days
(4). However, multiple lung
metastatic tumors developed during postoperative chemotherapy.
Moreover, the tumor recurred and metastasized to the
retroperitoneal space at 2 years after surgery, and the patient
suddenly succumbed to tumor-related septic shock 4 years after
surgery.
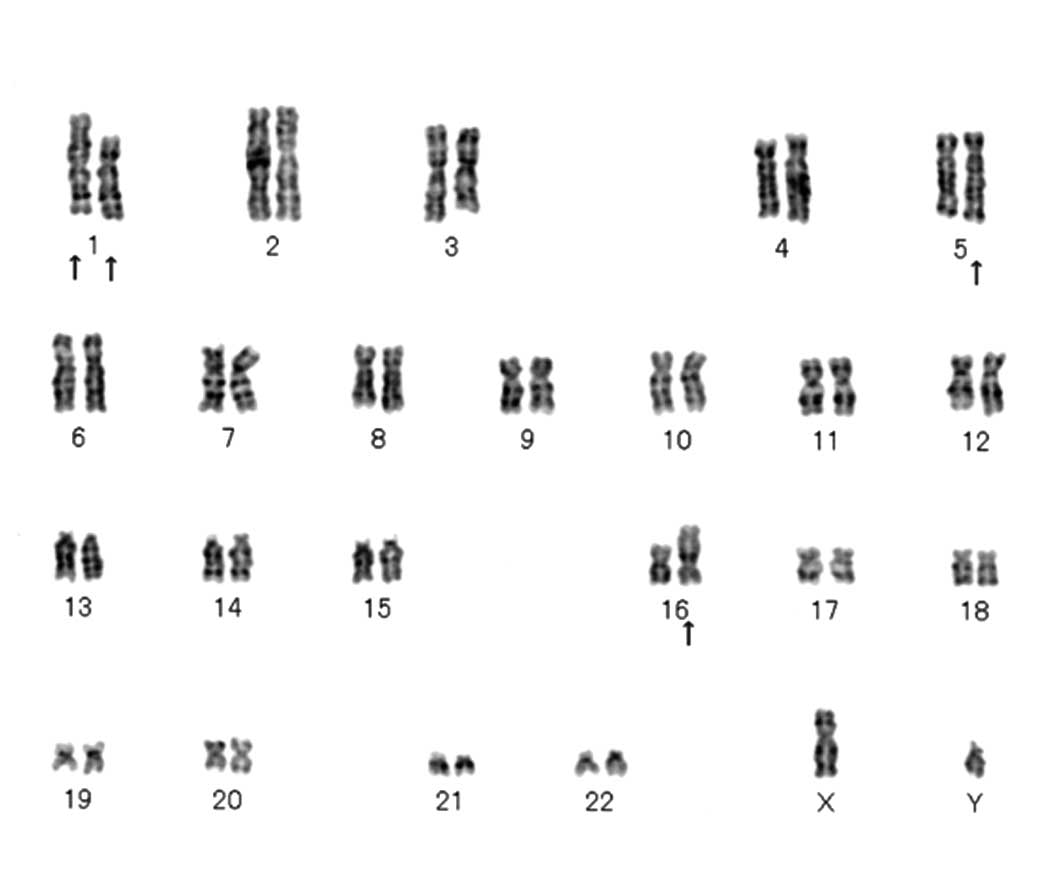
Cytogenetic findings
Cytogenetic analysis was performed on G-band by
trypsin and Giemsa (GTG) banding using surgical specimens. Standard
culture and harvesting procedures were utilized, as described
previously (5). The karyotypes were
expressed according to the International System for Human
Cytogenetic Nomenclature (6). Cells
(n=20) were analyzed. All 20 cells showed a clonal translocation
involving chromosome 1 and 16, and inversion 5 [46,XY, add(1)(q23), t(1;16)(p21;p11.2), inv(5)(q11.2;q15)] (Fig. 4).
Discussion
Histopathologically, whereas the expression of CD99
is high in EWS (2) and in certain
cases of SS, a low level of expression of CD99 is found in LGFMS,
rhabdomyosarcoma, lymphomas, mesenchymal chondrosarcoma,
osteosarcoma and neuroendocrine carcinoma (1,7,8). CD99
may act as a tumor suppressor. Some of these tumors are difficult
to diagnose differentially under microscopy, including
immunohistochemical staining. Therefore, cytogenetic analysis is
required for further tumor classification. For example, most EWS
contain a pathognomonic translocation of t(11;22)(q24;q12),
t(21;22)(q22.2;q12) or t(7;22)(p22;q12), fusing the EWS gene on
chromosome 22, which is a probable pivot event in the tumorigenesis
of this neoplasm (9). In addition,
most SS exhibit a well-known pathognomonic translocation of
t(18;X)(p11;q11), and most LGFMS exhibit t(11;16)(p11;p11).
Our case supports the possibility of a gene or genes
at chromosomes 1, 5 and 16. These genes may be important in
tumorigenesis. Three components of cytogenetic aberration were
observed in our case. The aberration add(1)(q23) has been non-specifically reported
thus far, but neither t(1;16)(p21;p11.2) nor inv(5)(q11.2;q15) were found in the NCBI
database (http://www.ncbi.nlm.njh.gov/sites/cancerchromosomes).
To the best of our knowledge, this is the first case of sarcoma
with t(1;16)(p21;p11.2) and inv(5)(q11.2;q15).
FUS gene (also known as TLS) is
encoded on chromosome band 16p11, and this location is specific for
LGFMS. FUS gene transcription may now be used as a
diagnostic marker for LGFMS. The FUS-CREB3L2 fusion gene
transcripts were observed in 95% of well-defined LGFMS. In
addition, the FUS-CREB3L1 variant resulting from
t(11;16)(p11;p11) was observed in 5%. The two chimeric genes encode
transcription activating proteins to form LGFMS (7). The immunohistochemical observations of
CD99 positivity and CD34 negativity in LGFMS are similar to our
case, but our case is high-grade, rather than low-grade sarcoma.
Although 16p11 in our case may be associated with FUS gene,
we were unable to clarify the specific event that affects the
tumorigenesis, as t(1;16)(p21;p11.2) has yet to be reported (NCBI
database). Moreover, inv(5) is also
a novel constitutional aberration in soft tissue tumors.
The reduction of CD99 expression in human EWS cell
lines results in neural differentiation, although its function in
the disease is unknown. EWS revealed an inverse correlation between
CD99 and neural markers, as well as an inverse correlation between
neural differentiation and oncogenic transformation (1). Therefore, CD99 expression may
correlate with tumorigenesis and malignant potential. Further
investigation is required to elucidate CD99-positive tumors.
Acknowledgements
The authors would like to thank Professor Tomoatsu
Kimura, of the Department of Orthopaedics, University of Toyama,
who provided clinical advice.
References
|
1
|
Rocci A, Manara MC, Sciandra M, et al:
CD99 inhibits neural differentiation of human Ewing sarcoma cells
and thereby contributes to oncogenesis. J Clin Invest. 120:668–680.
2010. View
Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sandverg AA and Bridge JA: The
Cytogenetics of Bone and Soft Tissue Tumors. RG Landes; Austin: pp.
288–312. 1994
|
|
3
|
Zucman J, Melot T, Desmaze C, et al:
Combinational generation of variable fusion proteins in the Ewing
family of tumors. EMBO J. 12:4481–4487. 1993.PubMed/NCBI
|
|
4
|
Elias A, Ryan L, Sulkes A, et al: Response
to mesna, doxorubicin, ifosfamide, and dacarbazine in 108 patients
with metastatic or unresectable sarcoma and no prior chemotherapy.
J Clin Oncol. 7:1208–1216. 1989.PubMed/NCBI
|
|
5
|
Bridge JA, Sreekantaiah C, Mouron B, et
al: Clonal chromosomal abnormalities in desmoid tumors:
implications for histopathogenesis. Cancer. 69:430–436. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
ISCN. An International System for Human
Cytogenetic Nomenclature. Mitelman F: Karger: Basel; 1995
|
|
7
|
Guillou L, Benhattar J, Gengler C, et al:
Translocation-positive low grade fibromyxoid sarcoma:
clinicopathological and molecular analysis of a series expanding
the morphologic spectrum and suggesting potential relationship to
sclerosing epithelioid fibrosarcoma: a study from the French
Sarcoma Group. Am J Surg Pathol. 31:1387–1402. 2007.
|
|
8
|
Malone VS, Dobin SM, Jones KA, et al:
CD99-positive large cell neuroendocrine carcinoma with rearranged
EWSR1 gene in an infant: a case of prognostically favorable tumor.
Virchows Arch. 457:389–395. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Desmaze C, Brizard F, Turc-Carel C, et al:
Multiple chromosomal mechanisms generate an EWS/FLI1 or an EWS/ERG
fusion gene in Ewing tumors. Cancer Genet Cytogenet. 97:12–19.
1997. View Article : Google Scholar : PubMed/NCBI
|