Introduction
Diffusion-weighted magnetic resonance imaging
(DW-MRI) has increasingly been used for the detection of tumors and
their recurrence following surgical resection and/or chemoradiation
on follow-up examinations. The performance of DW-MRI in oncological
imaging has been investigated. Recent comparisons with positron
emission tomography (PET) indicate a similar or superior diagnostic
ability of DW-MRI in the detection and differentiation between
malignant and benign processes (1–3).
DW-MRI is particularly superior to PET in the distant staging of
prostate cancer and the detection of mucinous tumors (4,5). We
report a case of mucinous adenocarcinoma of the rectum with
PET-negative sacral bone metastasis and its recurrence, which was
demonstrated on DW-MRI following surgical and adjuvant treatment.
The study was approved by the ethics committee of the hospital and
the patient consented to the publication of his case.
Case report
A 56-year-old male patient was referred to the
Department of Medical Oncology with a four-month history of
perianal pain and fecal incontinence. He underwent colonoscopy and
a mass lesion in the rectum was detected that started 4 cm above
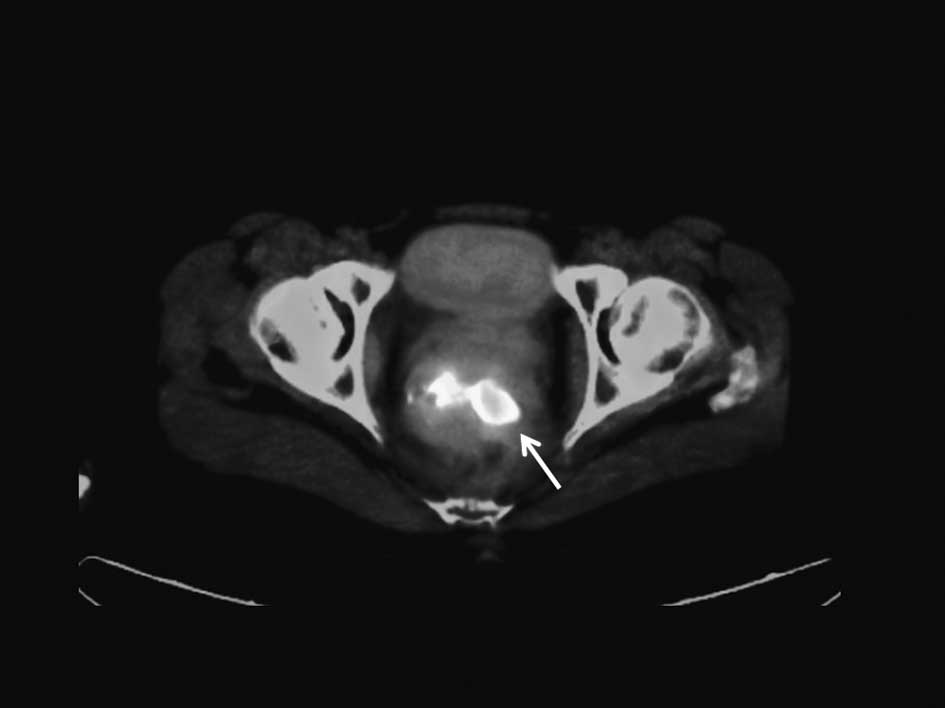
the anal verge and had a 10-cm cranial extension. Computed
tomography (CT) of the chest, abdomen and pelvis for the initial
staging revealed tumor invasion of the seminal vesicles and
prostate gland with enlarged iliac lymph nodes (Fig. 1). The chest CT was normal, revealing
a TNM stage of IIIB; cT4N1M0. The patient’s serum blood tumor
markers were 7.42 and 10.39 for carcinoembryonic antigen and cancer
antigen (CA) 19–9, respectively. ECOG (Eastern Cooperative Oncology
Group) performance was 1. The patient was scheduled for neoadjuvant
chemoradiotherapy with 5-fluorouracil 225 mgr/m2, 180
cGy/day, 5 days per week for five weeks to facilitate a
sphincter-sparing procedure and to decrease the locoregional
recurrence rate. Following completion of the chemoradiotherapy
regimen, the patient underwent pelvic MRI to determine the
locoregional staging and PET-CT for the distant staging. Pelvic MRI
was performed with DW-MRI using b values of 0, 400 and 800
sec/mm2. T1- and T2-weighted conventional imaging
sequences with and without intravenous contrast were also
obtained.
PET-CT revealed a localized tumor in the rectum with
increased standardized uptake values (SUV) (Fig. 2A). MRI showed a rectal mass adjacent
to the prostate capsule without seminal vesicle and/or prostatic
involvement (Fig. 2B). DW-MRI
revealed a sacral mass in the left half of the bone with diffusion
restriction (Fig. 2D). There was no
18F-fluorodeoxyglucose (FDG) uptake in the sacrum on PET-CT images
(Fig. 2C). No bone destruction was
appreciable on the PET-CT images. A CT-guided bone biopsy was
performed and material sampled from the sacrum was found to be
positive for mucinous adenocarcinoma. The patient underwent
abdominoperineal resection of the rectal tumor that also included
removal of the prostate and seminal vesicles with hemisacral
excision. The surgery ended with a mesh implantation to restrict
bowel motion into the pelvic cavity, to prevent intestinal side
effects in case of radiotherapy for locoregional recurrence.
Surgical material from the rectum was consistent with mucinous
adenocarcinoma and the same as the sacral bone material. The
surgical margins were all negative and there was no evidence of
contiguous tumor invasion of the sacrum. The patient received five
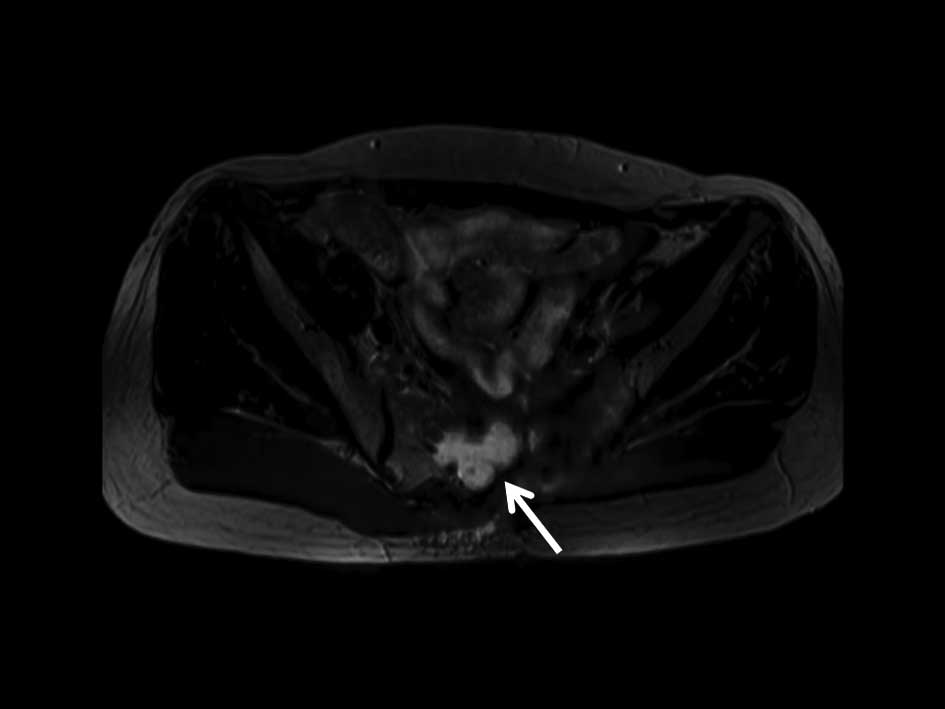
courses of FOLFOX-4 as adjuvant chemotherapy. Eight months
subsequent to the pelvic surgery, a follow-up MRI with DW-MRI was
performed, which showed a recurrent mass in the sacral bone
resection zone (Fig. 3). CT-guided
biopsy confirmed the MRI diagnosis. The patient was scheduled for
cyber-knife treatment of the sacral mass.
Discussion
Imaging is the most important diagnostic tool for
staging and monitoring therapy response in patients with colorectal
cancer. MRI has been used for the locoregional staging of the
tumor, whereas positron emission tomography (PET) with FDG has
become the modality of choice for the initial staging and
monitoring therapy response (6–9). The
majority of malignant tumors have a higher rate of glucose
metabolism than normal tissues. However, variations exist in the
glucose metabolic rate, depending on the histological type and the
aggressiveness of the tumor. Moderate and slow-growing malignant
lesions exhibit a lower glucose metabolic rate than aggressive
rapidly growing tumors (8,10). Awareness of the potential
limitations of FDG PET with particular histological subtypes is
essential for the proper application of this technique. Mucinous
adenocarcinoma is commonly localized in the gastrointestinal tract.
Mucins are high-molecular-weight glycoproteins and their presence
in colorectal tumors is associated with a poor prognosis, with the
exception of colorectal cancer, for which clinical studies have
shown that the presence of mucin is associated with a lower rate of
survival (11,12). FDG uptake has been correlated with
the number of viable tumor cells as well as the grade and the
differentiation of certain tumors. Findings of a recent report
showed that mucin exhibits a lower peak SUV of FDG than tumors
without mucin content (12). Lower
levels or absence of FDG uptake in mucinous tumors may be explained
by the reduced number of tumor cells, which are replaced by mucin
in the microenvironment, resulting in a decreased cellular density
of the tumor (12,13).
DW-MRI enables the visualization of Brownian
molecular motion, i.e, it reflects the motion of water molecules in
the extracellular, intracellular and intravascular spaces. DW-MRI
qualitatively and quantitatively assesses tissue cellularity and
the integrity of cell membranes, since the degree of restriction to
water diffusion in biological tissue inversely correlates with the
tissue cellularity and integrity of the cell membranes. Restricted
diffusion is observed in tissue with high cellular density such as
tumors, leading to tortuosity of the extracellular space and higher
density of hydrophobic cellular membranes, whereas in cystic or
necrotic tissues the apparent diffusion of water protons is
relatively less limited. Apparent diffusion coefficient (ADC)
values determine the ability of the water protons to diffuse.
Moreover, these values are expected to be lower in viable tumors
(1,4). Mucinous tumors reveal higher ADC
values than tumors without mucin content. However, the overall ADC
values and visual perception of the mucinous tumor are
distinguishable from cystic or necrotic tissues with high ADC
values (14). This may explain the
detection of the viable tumor in the sacrum by DW-MRI that had a
low SUV on PET.
The SUV values decrease from normal to imperceptible
values as early as three months following chemoradiotherapy in
colorectal cancer patients, although a certain degree of decrease
is expected earlier (9). In our
case, the PET imaging was performed five weeks after initiation of
chemoradiotherapy and was positive in the local tumor without
evidence of FDG uptake in sacrum. The absence of baseline PET prior
to chemoradiotherapy limited the evaluation of the treatment
response in our case. Histological variants of rectal
adenocarcinoma, including signet cell, mucinous, medullary,
adenosquamous, undifferentiated, spindle cell, clear cell, hepatoid
and oncocytic, have different clinical outcomes. These variants are
almost always associated with a poor prognosis compared to
adenocarcinoma of the same disease stage. Mucinous adenocarcinoma
is more aggressive than usual non-variant adenocarcinomas. It is
characterized as affecting younger patients and having a high
frequency of lymph node metastases, local recurrence and advanced
stage at presentation. Mucinous adenocarcinoma has been reported to
show poor downstaging following chemoradiotherapy in comparison
with that of rectal adenocarcinoma, thus surgical management is
always preferred in locally advanced disease (11,13).
In conclusion, we described a case of locally
advanced rectal mucinous adenocarcinoma with sacral bone
metastasis. PET-CT and DW-MRI revealed a rectal tumor, following
neoadjuvant chemoradiotherapy. DW-MRI demonstrated the presence of
sacral involvement despite physiological FDG uptake on PET in the
same location. The recurrent tumor in the excised sacrum was
detectable on the repeat DW-MRI eight months after surgery.
References
|
1
|
Koyama T, Tamai K and Togashi K: Current
status of body MR imaging: fast MR imaging and diffusion-weighted
imaging. Int J Clin Oncol. 11:278–285. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kwee TC, Takahara T, Ochiai R, et al:
Complementary roles of whole-body diffusion-weighted MRI and
18F-FDG PET: the state of the art and potential applications. J
Nucl Med. 51:1549–1558. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Watanabe T: Chemoradiotherapy and adjuvant
chemotherapy for rectal cancer. Int J Clin Oncol. 13:488–497. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Eschmann SM, Pfannenberg AC, Rieger A, et
al: Comparison of 11C choline- PET/CT and whole body-MRI for
staging of prostate cancer. Nuklearmedizin. 46:161–168.
2007.PubMed/NCBI
|
|
5
|
Kim SH, Lee JM, Hong SH, et al: Locally
advanced rectal cancer: added value of diffusion-weighted MR
imaging in the evaluation of tumor response to neoadjuvant chemo-
and radiation therapy. Radiology. 253:116–125. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Endo K, Oriuchi N, Higuchi T, et al: PET
and PET/CT using 18F-FDG in the diagnosis and management of cancer
patients. Int J Clin Oncol. 11:286–296. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Dresen RC, Beets GL, Rutten HJ, et al:
Locally advanced rectal cancer: MR imaging for restaging after
neoadjuvant radiation therapy with concomitant chemotherapy. Part I
Are we able to predict tumor confined to the rectal wall?
Radiology. 252:71–80. 2009. View Article : Google Scholar
|
|
8
|
Mainenti PP, Iodice D, Segreto S, et al:
Colorectal cancer and 18FDG-PET/CT: what about adding the T to the
N parameter in loco-regional staging? World J Gastroenterol.
17:1427–1433. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hur H, Kim NK, Yun M, et al:
18Fluoro-deoxy-glucose positron emission tomography in
assessing tumor response to preoperative chemoradiation therapy for
locally advanced rectal cancer. J Surg Oncol. 103:17–24. 2011.
View Article : Google Scholar
|
|
10
|
Zhu A, Lee D and Shim H: Metabolic
positron emission tomography imaging in cancer detection and
therapy response. Semin Oncol. 38:55–69. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Connelly JH, Robey-Cafferty SS and Cleary
KB: Mucinous carcinomas of the colon and rectum: analysis of 62
stage B and C lesions. Arch Pathol Lab Med. 115:1022–1025.
1991.PubMed/NCBI
|
|
12
|
Berger KL, Nicholson SA, Dehdashti F and
Siegel BA: FDG PET evaluation of mucinous neoplasms: correlation of
FDG uptake with histopathologic features. Am J Roentgenol.
174:1005–1008. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Green JB, Timmcke AE, Mitchell WT, Hicks
TC, Gathright JB Jr and Ray JE: Mucinous carcinoma-just another
colon cancer? Dis Colon Rectum. 36:49–54. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kim DJ, Kim JH, Lim JS, et al: Restaging
of rectal cancer with MR imaging after concurrent chemotherapy and
radiation therapy. Radiographics. 30:503–516. 2010. View Article : Google Scholar : PubMed/NCBI
|