Introduction
Granular cell tumors (GCT), first described by
Abrikossoff in 1926, are an uncommon mesenchymal soft tissue
neoplasm of Schwann cell origin (1,2). These
tumors may occur throughout the body, usually in the head and neck,
skin or subcutaneous tissues of the trunk and upper extremities,
breasts and female genital region. They are usually benign and
solitary; however, approximately 2% occur as malignant tumors, and
5–10% as multiple lesions (3,4). The
common sites for distant metastases include bone, peripheral
nerves, the peritoneal cavity and the lung (5). In 1992, Uzoaru et al reported a
unique case of MGCT with breast cancer without adequate follow-up
(6). For MGCT, surgical excision is
the only treatment method proven to be effective. In the present
study, we report a case of MGCT with breast metastasis and discuss
the available treatment modalities. The study was approved by the
ethics committee of Sir Run Run Shaw Hospital, Zhejiang University,
China. Consent was obtained from the patient.
Case report
In October 2009, a 56-year-old Chinese woman was
referred to the Department of Surgical Oncology at Sir Run Run Shaw
Hospital due to multiple painless masses in the right lower
abdominal wall, right groin and right breast. A mass in the right
lower abdominal wall had first appeared 10 years earlier, and had
been excised in 2003. The tumor recurred in 2004 and was again
excised in 2006. The patient developed a mass in the same region of
the abdominal wall once again in 2007, followed by a mass in the
right groin and right breast in 2008. On physical examination,
masses were present in the upper outer quadrant of the right
breast, right lower abdominal wall and right groin, measuring 3×3,
5×8 and 6×7 cm in size, respectively (Fig. 1A). These masses were fixed,
non-tender and firm on palpation. The abdominal wall mass, whose
overlying skin was red and crusted, was located in the interior of
the incision scar. There was a swollen lymph node 2 cm in diameter
in the right axilla, which was freely mobile and slightly hard.
Ultrasound and X-ray revealed that the breast mass was a carcinoma.
Supraclavicular lymph nodes, pelvic lymph nodes, liver, lungs and
bones were evaluated preoperatively to exclude metastasis. Levels
of tumor markers, including CA153, CA125 and CEA, were normal. A
puncture biopsy of the right breast mass was performed and
confirmed the mass as a GCT. A right breast lumpectomy with right
axillary dissection, a right abdominal wall mass resection, and a
right inguinal mass resection with inguinal dissection were
performed. Twenty-seven months after surgery, the patient was in
good health with no sign of further tumor development.
Gross examination revealed that the mass in the
right breast, right lower abdominal wall and right groin measured
2.8×2.5, 6×3.3 and 5.2×4 cm in size, respectively (Fig. 1B-D). The masses were yellow-gray in
color and well-circumscribed. The previous two biopsy specimens
resected in 2003 and 2006 were reviewed. Having similar
histological performance, the specimens demonstrated a pattern
compatible with GCT. The lesion consisted of nests of polygonal
cells with generally round nuclei and abundant eosinophilic
granular cytoplasm. The mitotic count was 1 per 10 high-power
fields (magnification, ×200). No cytologic pleomorphism, vesicular
nuclei with prominent nucleoli or areas of necrosis were observed,
and no increase in nuclear to cytoplasmic ratio (N:C) was noted.
The tumor nests were surrounded by abundant reactive fibrous
stroma, plasma cells and scattered groups of lymphocytes (Fig. 2A). The findings concurred with the
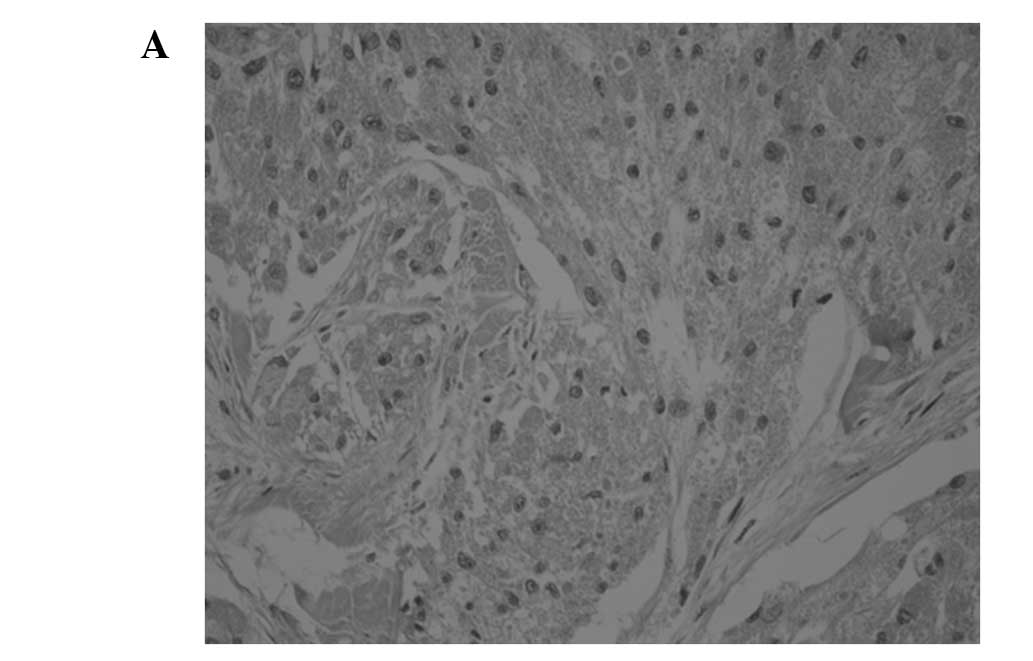
diagnosis of granular cell tumor. The pathological appearance of
the 2009 abdominal wall, right breast and right inguinal region
masses were similar (Fig. 2B-D).
The tumors were arrayed in nests and sheets composed of round to
irregular shaped cells with abundant eosinophilic granular
cytoplasm. The lesions were not completely encapsulated and focally
invaded adjacent connective tissue. The tumors demonstrated mild
cytologic pleomorphism, and round to oval-shaped vesicular nuclei
with prominent nucleoli were observed. The mitotic count was 3 per
10 high-power fields (magnification ×200). Four of the 14 right
axillary lymph nodes were found to be metastatic. The lymph nodes
in the right inguinal region demonstrated reactive hyperplasia.
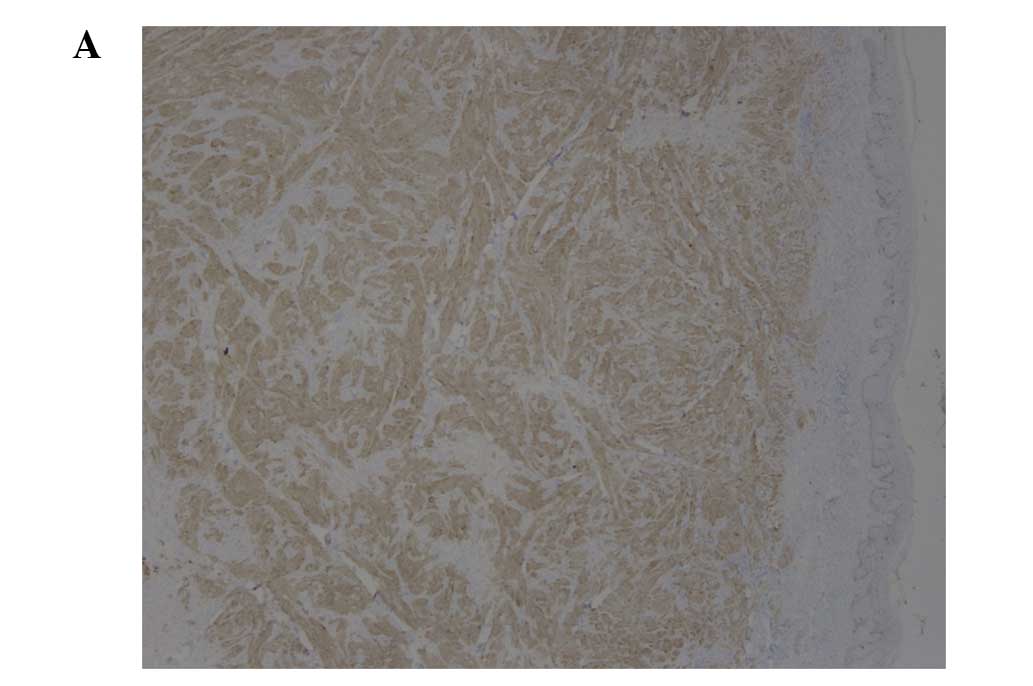
Immunohistochemical study of all tumors revealed
positivity for S100 protein, and p53 in <5% of cells. The Ki-67
proliferation index was 1% in the 2003 and 2006 biopsies and 10% in
the 2009 biopsy. CK and CD68 immunostains were negative in the
right breast tumor (Fig. 3A-C).
Discussion
Malignant granular cell tumors are similar in
epidemiology to their benign counterparts. Both are found twice as
often in females as in males and occur most commonly between the
age of 40 and 69 (2). Initially,
granular cell tumors were considered to arise from histiocytes,
fibroblasts, myocytes or intestinal mesenchymal cells. On the basis
of ultrastructural observations and histochemical evidence, the
tumors are now widely accepted to originate from Schwann cells
(7). Larger tumor size, advanced
age and local recurrence at presentation correlate with a worse
prognosis (8). MGCT is an extremely
rare type of cancer and at present no more than 100 cases have been
described in the English language literature. Among them, many
cases lack adequate follow-up. Consequently, diagnostic criteria
and management strategy for MGCTs remain controversial (9).
It is difficult to distinguish between malignant and
benign GCTs. Although metastasis remains one of the most important
criteria for defining malignancy, there is general recognition that
not all malignant tumors, even those of high grade, actually
metastasize. Clinically, it is of great significance to define
malignancy before metastasis occurs. Six histological criteria have
been established to predict malignant behavior according to the
retrospective analysis of previous case reports of malignant GCTs.
These are spindling of the tumor cells, the presence of vesicular
nuclei with large nucleoli, increased mitotic rate (2 mitoses per
10 high-power fields at ×200 magnification), a high nuclear to
cytoplasmic ratio, pleomorphism and necrosis (10). Neoplasms that meet three or more of
these criteria are classified as malignant, those that meet one or
two criteria are classified as atypical, and those that exhibit
only focal pleomorphism are classified as benign (11). In the reported case study, the two
initial lesions were consistent with benign histological
performance according to the stated criteria. The later lesions
were classified as malignant due to the observation of spindling of
the tumor cells, vesicular nuclei with large nucleoli and increased
mitotic rate. The benign lesion existed for several years and
recurred twice following local resection. Ultimately, multiple
subcutaneous and lymph node metastases occurred. Therefore, we
presume that MGCT results from the malignant transformation of
benign GCT. Although the possibility that there were multiple
primary GCTs (multifocality) cannot be excluded, metastasis is a
logical explanation for the simultaneous appearance of MGCT in the
right breast and right groin. In contrast to the common sites for
distant metastases, which include bone, peripheral nerves, the
peritoneal cavity and the lung (5),
the present case involved metastases in the breast. To the best of
our knowledge, this is the first case of MGCT with breast
metastasis that has adequate follow-up. The right breast GCT
closely resembled breast carcinoma in the ultrasound and X-ray
examination; however, microscopic examination revealed significant
differences between them. Since S100 is positive in one third of
breast carcinomas and cytokeratin is only positive in breast
carcinomas, cytokeratin immunohistochemical staining was performed
to differentiate GCT from common malignant breast tumors.
Although there is considerable overlap in the Ki-67
proliferative index between histologically benign, atypical and
malignant GCTs (11,12), statistical analysis reveals a
correlation between the Ki-67 proliferative index and malignant
classification. A score of >10% for the Ki-67 index was
significantly correlated with malignancy and unfavorable prognosis.
In the reported case, the previous two tumors of the abdominal wall
had a Ki-67 proliferative index of <1%, which increased to 10%
in the second recurrence and was associated with increased nuclear
pleomorphism, vesicular nuclei with prominent nucleoli and
increased mitotic rate. Similarly, Le et al reported that a
clinical recurrence exhibited progressively more marked nuclear
pleomorphism and vesicular nuclei with prominent nucleoli, as well
as an increased Ki-67 proliferative index (1–10%). Due to the
absence of demonstrable metastases, the tumor was classified as
atypical GCT of unknown malignancy (12). We believe that in GCT clinical
recurrences, an increased Ki-67 proliferative index predicts
clinical behavior and should be one of the criteria for defining
malignancy.
Wide local excision with regional lymph node
dissection is the first choice of treatment for MGCT. In metastatic
patients, there is no evidence that resection of the metastatic
lesions improves prognosis. In this case, considering the axillary
lymph node metastases of the right breast metastatic lesion,
regional lymph node dissection of the metastatic lesion was
advised. Whether regional lymph node dissection improves prognosis
may be determined by the follow-up. Although certain cases of
successful treatment have been reported, the effectiveness of
chemotherapy and radiotherapy remains controversial.
References
|
1
|
Abrikossoff A: Über Myome, ausgehend von
der quergestreiften willkürlichen Muskulatur. Virchows Arch Pathol
Anat Physiol. 260:215–233. 1926.
|
|
2
|
Mukai M: Immunohistochemical localization
of S-100 protein and peripheral nerve myelin proteins (P2 protein,
P0 protein) in granular cell tumors. Am J Pathol. 112:139–146.
1983.PubMed/NCBI
|
|
3
|
Gokaslan ST, Terzakis JA and Santagada EA:
Malignant granular cell tumor. J Cutan Pathol. 21:363–370. 1994.
View Article : Google Scholar
|
|
4
|
Lack EE, Worsham GF, Callihan MD, Crawford
BE, Klappenbach S, Rowden G and Chun B: Granular cell tumor: a
clinicopathological study of 110 patients. J Surg Oncol.
13:301–316. 1980. View Article : Google Scholar
|
|
5
|
Curtis BV, Calcaterra TC and Coulson WF:
Multiple granular cell tumor: a case report and review of the
literature. Head Neck. 19:634–637. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Uzoaru I, Filler B, Ray V, Hubbatd-Shepaid
M and Rhee H: Malignant granular cell tumor. Arch Pathol Lab Med.
116:2061992.
|
|
7
|
Fisher ER and Wechsler H: Granular cell
myoblastoma - a misnomer. Electron microscopic and histochemical
evidence concerning its Schwann cell derivation and nature
(granular cell schwannoma). Cancer. 15:936–954. 1962. View Article : Google Scholar
|
|
8
|
Enzinger RM and Weiss SW: Granular cell
tumor. Soft Tissue Tumors. 4th edition. Mosby; St. Louis: pp.
1178–1206. 2001
|
|
9
|
Mahoney A, Garg A, Wolpowitz D and
Mahalingam M: Atypical granular cell tumor - apropos of a case with
indeterminate malignant potential. Am J Dermatopathol. 32:370–373.
2010.PubMed/NCBI
|
|
10
|
Khansur T, Balducci L and Tavassoli M:
Granular cell tumor. Clinical spectrum of the benign and malignant
entity. Cancer. 60:220–222. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fanburg Smith JC, Meis Kindblom JM, Fante
R and Kindblom LG: Malignant granular cell tumor of soft tissue:
Diagnostic criteria and clinicopathologic correlation. Am J Surg
Pathol. 22:779–794. 1998.PubMed/NCBI
|
|
12
|
Le BH, Boyer PJ, Lewis JE and Kapadia SB:
Granular cell tumor immunohistochemical assessment of
inhibin-alpha, protein gene product 9.5, S100 protein, CD68, and
Ki-67 proliferative index with clinical correlation. Arch Pathol
Lab Med. 128:771–775. 2004.PubMed/NCBI
|