Introduction
Aggressive angiomyxoma (AAM) is a rare mesenchymal
tumor typically occurring in the pelvis and perineum of
reproductive females (1). AAM has
also been described in the male larynx, genital tract and
supraclavicular fossa (2–4). A notable case of AAM on the upper,
lateral aspect of the right thigh in a male patient has also been
reported (5). Due to the high
recurrence rate, tumor excision with wide tumor-free margins should
be performed for AAM. Studies suggest that hormonal manipulation
may also be of value (6,7). In this study, we present a case of AAM
of the thigh in a 43-year-old female patient. Informed consent was
obtained from the patient prior to the study.
Case report
A 43-year-old female patient presented with a solid
mass on the upper, lateral aspect of her right thigh. The mass had
been present for one month and had grown progressively during that
period. For the previous 2 months the patient had experienced
slight pain in the right thigh, which did not impact movement. She
had no history of surgical trauma or pain in the right thigh.
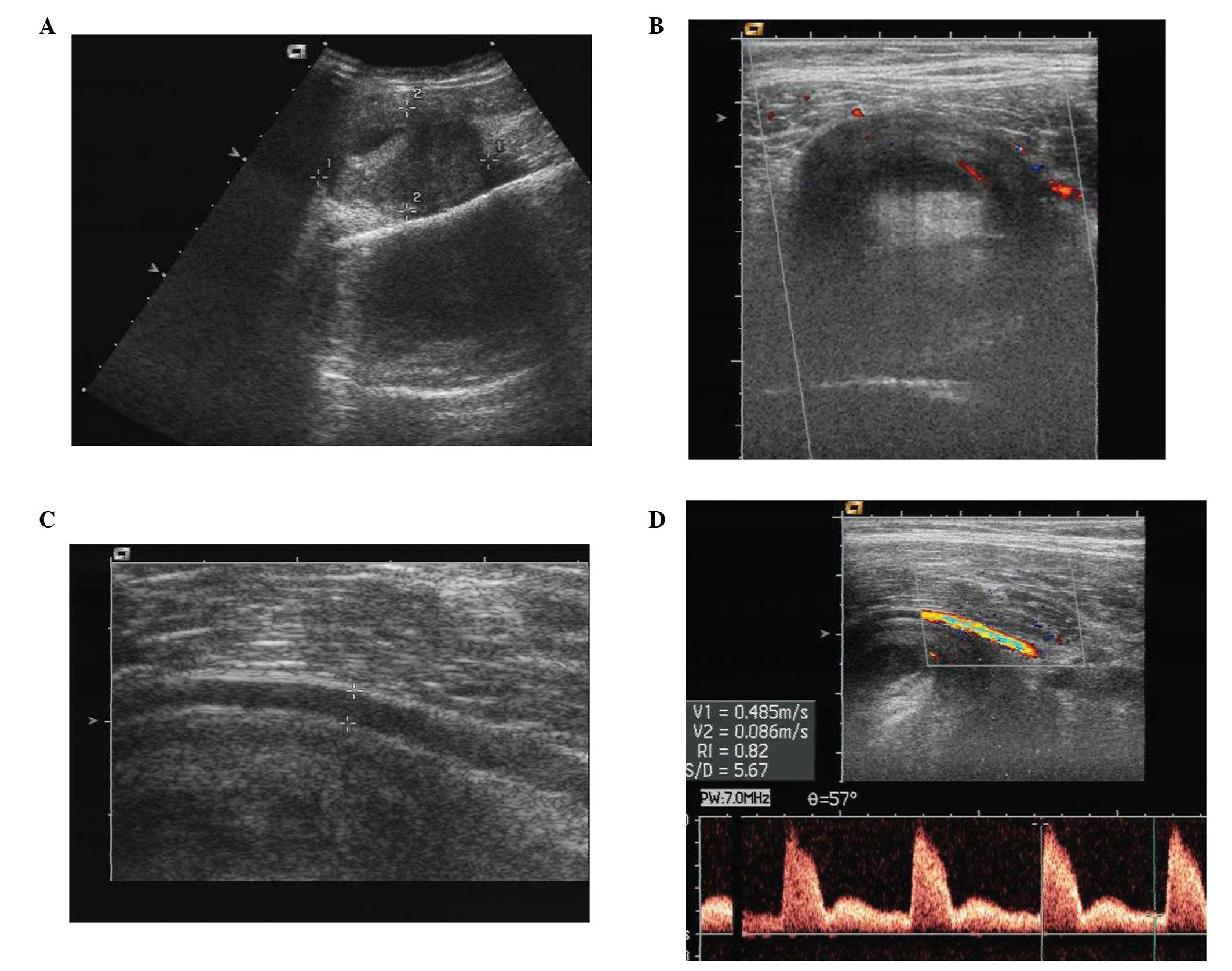
Sonography revealed a mass of approximately
6.1×3.7×5.3 cm overlying the upper part of the right thigh, close
to the inguinal region under the muscle. The mass was oval and
well-demarcated with a heterogeneous echotexture (Fig. 1A). Color Doppler ultrasonography
(CDUS) revealed weak blood flow in the mass with peripheral and
central avascularity (Fig. 1B). A
branch of the femoral artery passing alongside and attaching to the
surface of the mass was evident (Fig.
1C). The maximum peak systolic velocity (PSV) and resistive
index (RI) values of the artery around the mass were 48.5 cm/sec
and 0.82, respectively (Fig.
1D).
Computed tomography (CT) showed the mass to be
located on the right thigh under the spatium intermusculare of the
quadriceps femoris and demonstrated a well-defined margin of
hypodensity (Fig. 2). The
articulation bones of the hip had normal form and homogeneous
density. There was no evident destruction, absorption or
hyperplasia in the bones. The articular cavity of the hip was
visible and had no hydrops.
During surgery, a mass of approximately 6×7 cm was
revealed beneath the spatium intermusculare of the quadriceps
femoris on the upper part of the right thigh. The mass had a
moderate degree of hardness, complete adventitia and a rough
surface. A marginal surgical excision was performed around the
adventitia of the tumor.
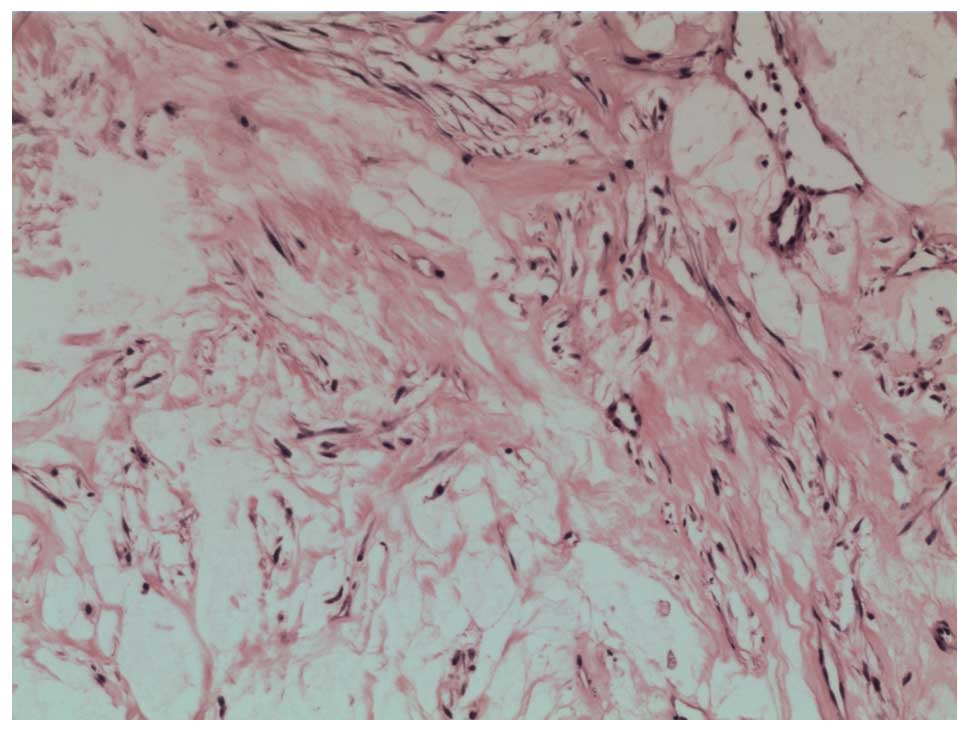
Histologically, the tumor consisted of a sparse
population of stellate and spindle-shaped tumor cells in the myxoid
stroma intermingled with an abundance of variably dilated blood
vessels (Fig. 3).
Immunohistochemically, the tumor cells were positive for vimentin,
CD-34 and α-smooth muscle actin, and negative for S-100 protein,
desmin and muscle-specific actin. At 18 months follow-up, there was
no recurrence.
Discussion
AAM is a rare benign mesenchymal tumor which, in
approximately 95% of cases, occurs in females of reproductive age
(8). As reported, the female to
male ratio is approximately 6.6:1 (9). AAM patients are usually asymptomatic
due to the slow and insidious growth pattern of the tumor (8). Steeper and Rosai (1) described the locally aggressive
behavior of the tumor and its tendency to recur locally. Surgery is
the most effective method for the treatment of AAM. In contrast to
other deep-seated soft tissue tumors, excision with wide tumor-free
margins should be performed for AAM, rather than local excision. In
addition, adjuvant therapy is necessary. Angiographic embolization
may shrink the tumor preoperatively, allowing the tumor to be
completely removed (10). Hormonal
manipulation may be used in recurrent cases or residual tumors
(11). Due to the specificity of
treatment in AAM, accurate diagnosis prior to surgery is
critical.
The characteristic sonographic appearance in the
present case was a mass with sharply demarcated borders and a
heterogeneous echotexture. In a review of the literature by
Jingping et al (11), the
characteristic appearance using B-ultrasound imaging for the
diagnosis of AAM was described as a hypoechoic, well-demarcated
mass with multiple thin, echogenic internal septa. The sonographic
findings in the current study were similar to those described by
Jingping et al. To the best of our knowledge, the issue of
blood supply in AAM presenting as a thigh tumor has never been
described in detail. Heffernan et al (5) reported a case in which some internal
blood flow was observed on CDUS. In our case, the tumor
demonstrated weak blood flow on CDUS. AAM is derived from
myofibroblasts as a phenotypic variant of the basic fibroblast
(12). Furthermore, there is no
evidence of an anastomosing and arborizing vascular pattern in AAM
(8,13). Therefore, the histological features
of AAM are responsible for the reduced blood supply observed on
CDUS. A branch of the femoral artery passing alongside and
attaching to the surface of the mass showed low velocity and high
resistance, which may be associated with the pressurization of the
tumor. However, it is important to preserve the blood vessels
during tumor excision due to the branch of the femoral artery
beside the mass.
A CT scan was also performed prior to surgery to
show the severity of the tumor. The appearance of AAM is often
hypodense on CT (14). In the
present study, the mass was hypodense with no invasion of the
skeletal structures and no hydrops in the articular cavity.
Enhanced CT demonstrated high vascularity in the AAM mass (5). The characteristic imaging of AAM on
MRI is isointense relative to muscle on T1-weighted images and
hyperintense on T2-weighted images (14).
The differential diagnosis was considered mainly to
exclude other myxoid-containing tumors such as intramuscular
myxoma, myxoid liposarcoma and malignant fibrous histocytoma of the
extremities. The definitive diagnosis is histological since the
non-specific imaging appearance of AAM did not distinguish it from
other myxoid neoplasms.
Histopathological examination revealed an AAM of the
thigh. Histologically, the tumor was characterized by spindle and
stellate cells in a loose myxoid stroma with a prominent vascular
component (2). Immunohistochemical
staining of the tumor, particularly the reactivity for desmin,
α-smooth muscle actin, muscle-specific actin, vimentin, CD-34,
S-100 protein, estrogen and progestin receptors, is essential for
diagnosis (12,15,16).
This study is the second reported case of femoral
AAM. Heffernan et al (5)
reported a mass without pain overlying the upper part of the right
thigh over the tensor fascia latae muscle. Ultrasonography revealed
a lobulated mass located in the subcutaneous fat of the right
thigh. Naturally, there are certain differences between the two
cases in terms of location, form and symptoms. A wide resection
taking the underlying fascia and subcutaneous fat as the
circumferential margin was successful and no recurrence occurred in
the 6 months after surgery in this case. Although the patient in
our case underwent marginal surgical excision, there was no
evidence of local recurrence in the 18 months following surgery.
The study showed no statistical difference in recurrences between
patients with negative margins and patients with positive margins
(9). Long-term follow-up is
essential to aid in the timely identification of AAM
recurrence.
In conclusion, we reported an uncommon case of AAM
of the thigh. When sonography reveals a mass of the thigh with
sharply demarcated borders and a heterogeneous echotexture, and
weak blood flow is observed on CDUS, AAM should be considered. The
mainstay of treatment for AAM of the thigh is surgical excison.
Abbreviations:
|
AAM
|
aggressive angiomyxoma
|
|
CDUS
|
color Doppler ultrasonography
|
|
CT
|
computed tomography
|
|
PSV
|
peak systolic velocity
|
|
RI
|
resistive index
|
References
|
1
|
Steeper TA and Rosai J: Aggressive
angiomyxoma of the female pelvis and perineum. Report of nine cases
of a distinctive type of gynaecologic soft-tissue neoplasm. Am J
Surg Pathol. 7:463–475. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sylvester DC, Kortequee S, Moor JW, et al:
Aggressive angiomyxoma of larynx: case report and literature
review. J Laryngol Otol. 124:793–795. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Idrees MT, Hoch BL, Wang BY and Unger PD:
Aggressive angiomyxoma of the male genital region. Report of 4
cases with immunohistochemical evaluation including hormone
receptor status. Ann Diagn Pathol. 10:197–204. 2006. View Article : Google Scholar
|
|
4
|
Pai CY, Nieh S, Lee JC, et al: Aggressive
angiomyxoma of supraclavicular fossa: a case report. Head Neck.
30:821–824. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Heffernan EJ, Hayes MM, Alkubaidan FO, et
al: Aggressive angiomyxoma of the thigh: case report. Skeletal
Radiol. 37:673–678. 2008. View Article : Google Scholar
|
|
6
|
Fine BA, Munoz AK, Litz CE, et al: Primary
medical management of recurrent aggressive angiomyxoma of the vulva
with a gonadotropin-releasing hormone agonist. Gynecol Oncol.
81:120–122. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chihara Y, Fujimoto K, Takada S, et al:
Aggressive angiomyxoma in the scrotum expressing androgen and
progesterone receptors. Int J Urol. 10:672–675. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Dahiya K, Jain S, Duhan N, et al:
Aggressive angiomyxoma of vulva and vagina: a series of three cases
and review of literature. Arch Gynecol Obstet. 283:1145–1148. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chan YM, Hon E, Ngai SW, et al: Aggressive
angiomyxoma in females: is radical resection the only option? Acta
Obstet Gynecol Scand. 79:216–220. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Nyan DCK and Pemberton J: Large aggressive
angiomyxoma of the perineum and perineum and pelvis: an alternative
approach. Diseases of the Colon and Rectum. 41:514–516. 1998.
View Article : Google Scholar
|
|
11
|
Jingping Z and Chunfu Z: Clinical
experiences on aggressive angiomyxoma in China (report of 93
cases). Int J Gynecol Cancer. 20:303–307. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hatano K, Tsujimoto Y, Ichimaru A, et al:
Rare case of aggressive angiomyxoma presenting as a retrovesical
tumor. Int J Urol. 13:1012–1014. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Nucci MR and Fletcher CD: Vulvovaginal
soft tissue tumors: update and review. Histopathology. 36:97–108.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wiser A, Korach J, Gotlieb W, et al:
Importance of accurate preoperative diagnosis in the management of
aggressive angiomyxoma: report of three cases and review of the
literature. Abdom Imaging. 31:383–386. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Fetsch JF, Laskin WB, Lefkowitz M, et al:
Aggressive angiomyxoma: a clinicopathological study of 29 female
patients. Cancer. 78:79–90. 1996. View Article : Google Scholar
|
|
16
|
Begin LR, Clement PB, Kirk ME, et al:
Aggressive angiomyxoma of pelvis soft parts: a clinicopathologic
study of nine cases. Hum Pathol. 16:621–628. 1985. View Article : Google Scholar : PubMed/NCBI
|