Introduction
Desmoid tumour, also known as desmoid fibromatosis,
is a rare (3–4 cases/million individuals/year), deep-seated,
musculoaponeurotic tumour which accounts for 0.03% of all neoplasms
(1–2). Females are more susceptible to
developing this tumour than males, and the tumour may occur at any
age (3). The tumour usually
develops in the following three areas: i) extra-abdominal area of
the shoulder and pelvic girdle or chest and neck wall; ii)
abdominal area of wall muscles; iii) intra-abdominal area of the
pelvis, mesentery connective tissue and retroperitoneal space
(4).
The natural history of desmoid tumours remains
unknown. The tumours usually grow slowly, but in certain cases they
may enlarge rapidly. Some of these tumours may stop growing and
regress naturally (5,6). For this reason, desmoid tumours have
been referred to as enigmatic. The etiology of this disease is not
well-defined: trauma, genetic disposition and oestrogen imbalance
are considered to be factors responsible for this disease. Wide
local excision is the preferred method of treatment, but it often
causes serious damage to the limb function. In this study, we
investigate a rare case, wherein wide local excision and
reconstructive surgery were conducted in a single procedure.
The study was approved by the ethics committee of
the First Affiliated Hospital of Soochow University, China.
Case report
A 52-year-old female reported a slow-growing lump in
the right crus, which had been increasing in size for two years.
The patient complained of persistent pain, especially at night. The
patient was subjected to lump resection in another hospital,
wherein the postoperative histopathological examination showed
muscle fibroma. Following surgery, the patient demonstrated signs
of excellent recovery. Three months later, the lump recurred in the
same position. The persistent pain associated with the lump impeded
her ability to walk, and she did not report any other complaints.
Examination revealed an irregular tumour 10×8 cm in size with tough
texture, poor mobility, blurred border and moderate tenderness. The
results of other tests were negative.
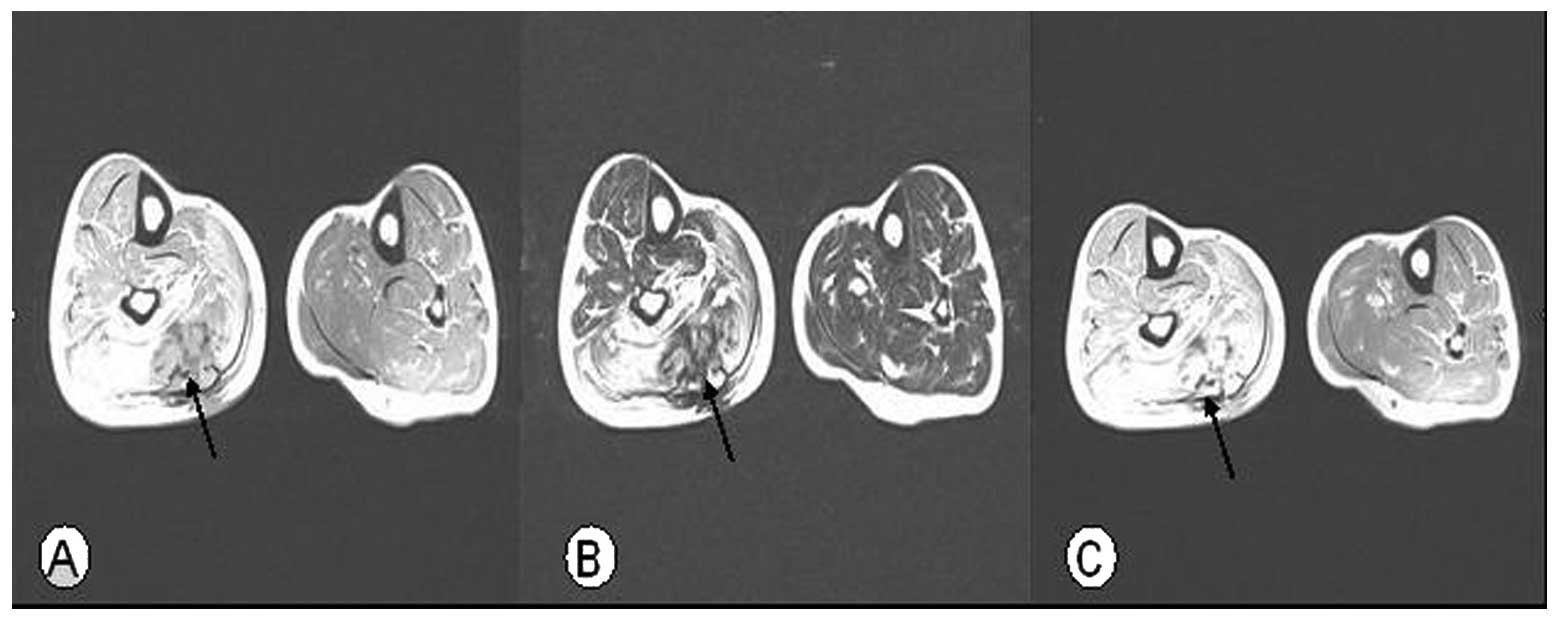
The MRI scan revealed a homogeneously iso-signal
intensity lesion on the T1-weighted image and a heterogeneous high
intensity signal was detected on the T2-weighted image. The
contrast-enhanced T1-weighted axial images showed mild enhancement
of the lesion through an irregular margin. The MRI scan also
revealed bands of low signal intensity within the lesion. In
addition, desmoid tumours did not reveal any central necrosis, even
in the largest lesions (Fig.
1).
Wide local excision through excision biopsy of the
tumour was planned. Under the spinal anaesthesia effect, with the
patient in a prone position, an arc incision of approximately 20 cm
was made along the long axis of the back side through the right
crus. The tumour was attached to the soleus and had infiltrated
into most of the gastrocnemius. The size of the tumour was
approximately 8×8 cm. The tumour was firm; however, it had an
irregular margin and lacked a capsule. We exposed the posterior
tibial nerve and posterior tibial blood vessel, which were not
affected by the tumour. We removed the medial and lateralis heads
of the gastrocnemius from the fringe. The major part of the soleus
muscle belly was resected. Then, the junction of the Achilles
tendon, gastrocnemius and soleus was removed. A small part of the
lateralis was left. The upper and lower ends of the residual
muscles were subjected to fast pathological examination. The fast
pathological examination confirmed that the resection margin was
negative. We made a longitudinal incision in the Achilles tendon,
wherein half of the Achilles tendon was included as an extension to
rebuild the Achilles tendon. Postoperatively, a cast immobilisation
was undertaken in the plantarflexion position for approximately 4
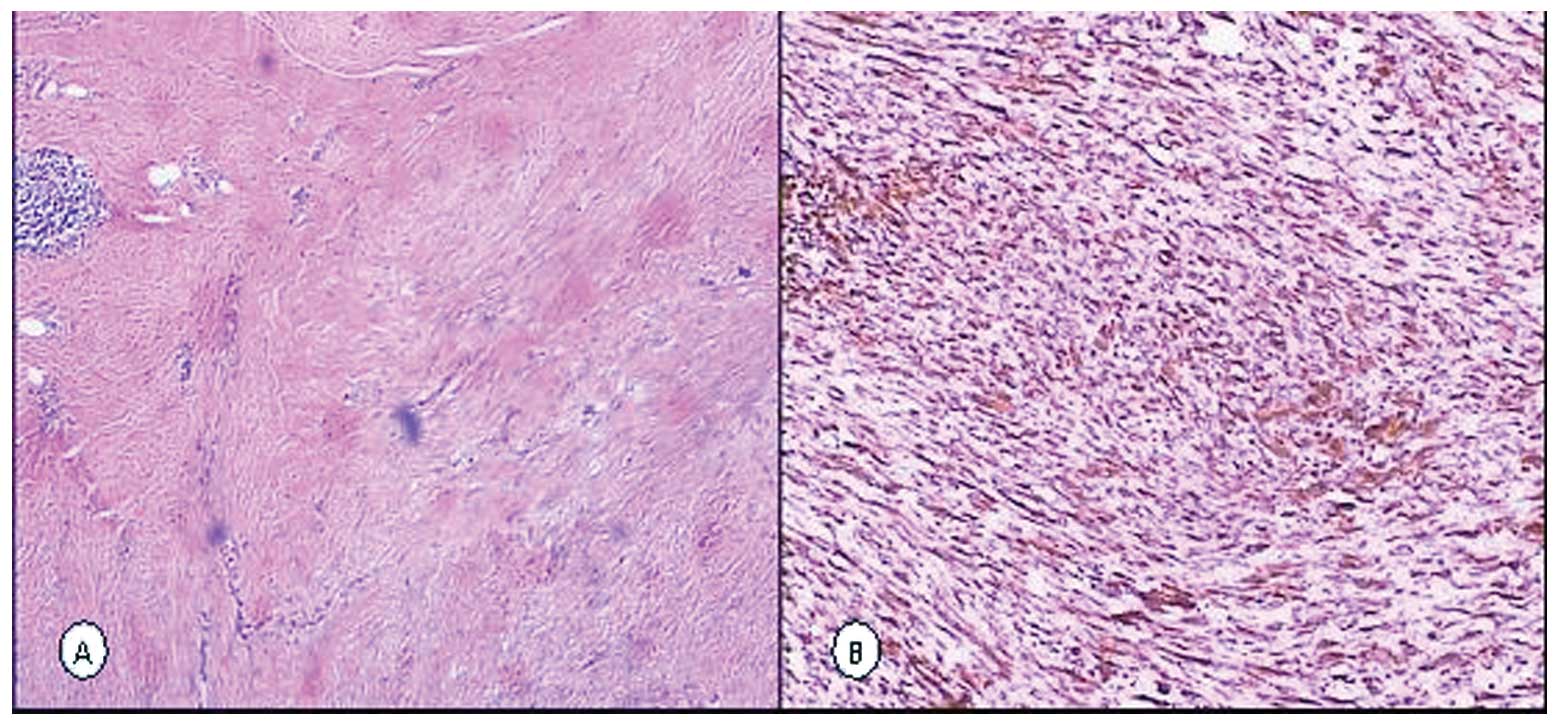
weeks. Postoperative histopathological examination of the right
crus revealed ligament sample fibroma. Immunohistochemical
examination revealed that staining for Vimentin was positive, while
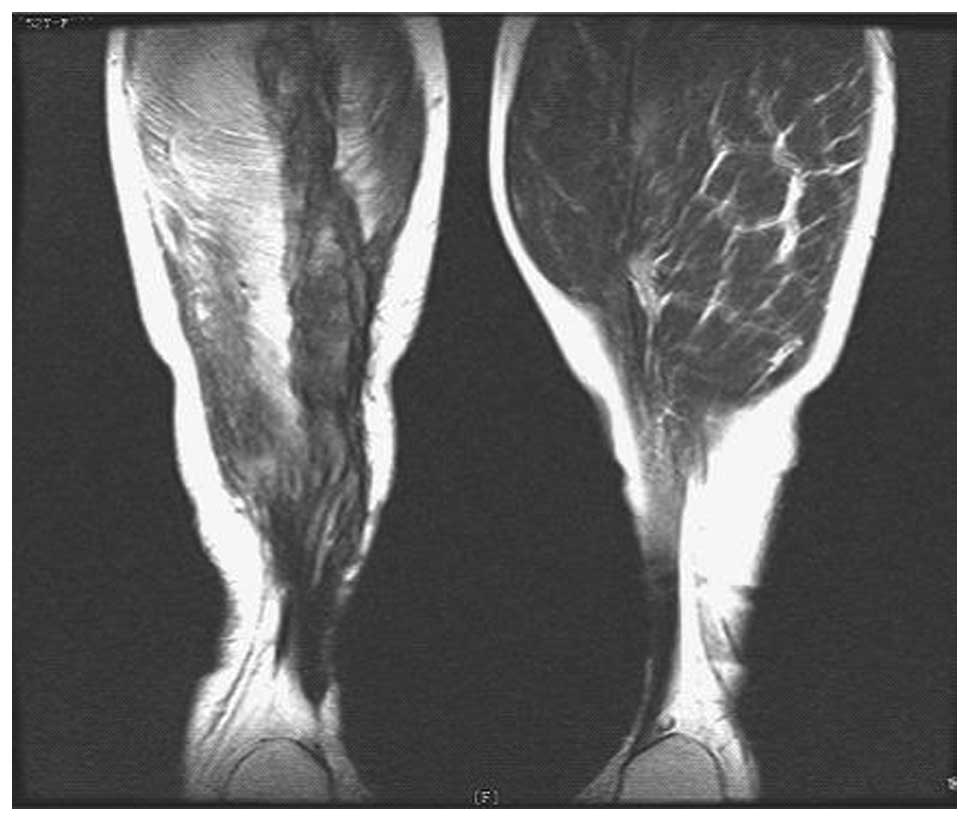
that for CD34 and SMA were negative (Fig. 2). Following the surgery, the
symptoms improved markedly and the patient partially recovered
plantarflexion function. After 4 months, the follow-up MRI
examination did not reveal any recurrence of the tumour (Fig. 3). In the follow-up period of six
years, the patient did not show any sign of recurrence.
Discussion
Extra-abdominal desmoid tumour is a fibroblastic
tumour which arises from the connective tissues of muscles, fascia,
aponeurosis or periosteum (7).
Despite their benign appearance, these are locally aggressive
tumours, which tend to invade the surrounding structures as they
lack a true capsule. Therefore, these tumours are often
misclassified as low-grade malignancies (low-grade malignant
tumours) (8). The tumour is not
known to metastasise, but it has a high recurrence rate after
surgery. A local recurrence rate of 24–77% has been reported at 10
years.
Current treatments include radiation therapy,
chemotherapy, drug therapy and hormone therapy. However, surgical
resection is the preferred method of treatment. As the disease has
the clinical characteristics of an aggressive growth and a high
recurrence rate, the tumour should be widely resected. Wide local
excision with a negative margin is considered to be a significant
factor that decreases the recurrence rate. Ballo et al
(9) performed a retrospective
review of 189 consecutive cases of desmoid tumour that were treated
only with surgical resection. Among the patients with negative
margins, the 10-year recurrence rate was 27%. However, 40 patients
with positive margins had a 10-year relapse rate of 54%. Leithner
et al (10) performed a
comparative analysis based on the data extrapolated from 412
retrospective studies: 152 patients with negative margins had a
recurrence rate of 27%, while 260 patients with positive margins
had a local recurrence rate of 72%. Therefore, the quality of the
resection boundary is considered to be the most significant factor
for predicting the recurrence of the tumour. If resection achieves
a negative margin, the postoperative recurrence rate is relatively
low. However, certain groups have reported that the recurrence rate
remains high following wide local excision with a negative margin.
We suggest two reasons for this observation. Firstly, desmoid
tumours lack a pseudocapsule and form a non-palpable mass that
infiltrates along the muscle bundles and fascia. Moreover, it is
difficult to detect the exact localisation and extension of
infiltration or dissemination of the lesion in the tumour.
Secondly, the negative margin is observed with the naked eye
instead of by pathological examination, which may not reflect the
true margin. In this case, we examined the upper and lower ends of
residual muscles for fast pathological examination. The
pathological examination confirmed that the resection margin was
negative.
However, wide local excision causes serious damage
to limb function. However, selecting the appropriate treatment
method remains a challenge. Ferraresi et al (11) described a case wherein the tumour
had selectively invaded the patient’s radial nerve. The tumour was
partially removed with the radial nerve and neurotransplantation
was performed. This procedure showed an excellent clinical recovery
and no recurrence was reported in the 6-year follow-up period.
Gallucci et al (12)
presented a case of aggressive fibromatosis in the proximal third
of the forearm that was treated with wide resection and
reconstructive surgery in a single procedure. An acceptable
functional result did not show any evidence of recurrence within
the 3-year follow-up period. Thus, wide local excision should be
undertaken to reduce the recurrence rate of tumours. Reconstructive
surgery proves to be of little significance if the tumour
relapses.
In this case, the tumour had a wide range. We
resected most of the gastrocnemius and soleus. After performing a
pathological examination, we conducted reconstructive surgery of
the Achilles tendon. We suggest that reconstructive surgery should
be performed to maintain the functioning of the lower limb. The
patient recovered part of the plantarflexion function after the
surgery and had no recurrence in the 6-year follow-up period.
In conclusion, we consider that wide local excision
with a negative margin by pathological examination reduces the
recurrence rate. As desmoid tumours are low-grade malignant
tumours, we need to maintain the optimum function of limbs as far
as possible. This reduces the recurrence rate of the tumours.
References
|
1
|
Berri RN, Baumann DP, Madewell JE, et al:
Desmoid tumor: current multidisciplinary approaches. Ann Plast
Surg. 67:551–564. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Shields CJ, Winter DC, Kirwan WO and
Redmond HP: Desmoid tumor. Eur J Surg Oncol. 27:701–706. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Meazza C, Bisogno G, Gronchi A, et al:
Aggressive fibromatosis in children and adolescents: the Italian
experience. Cancer. 116:233–240. 2010.PubMed/NCBI
|
|
4
|
Ferenc T, Sygut J, Kopczyński J, et al:
Aggressive fibromatosis (desmoid tumors): definition, occurrence,
pathology, diagnostic problems, clinical behavior, genetic
background. Pol J Pathol. 57:5–15. 2006.
|
|
5
|
Okuno S: The enigma of desmoid tumors.
Curr Treat Options Oncol. 7:438–443. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Dalén BP, Geijer M, Kvist H, et al:
Clinical and imaging observations of desmoid tumors left without
treatment. Acta Orthop. 77:932–937. 2006.PubMed/NCBI
|
|
7
|
Agrawal PS, Jagtap SM and Mitra SR:
Extra-abdominal desmoid tumour of the leg. Singapore Med J.
49:e6–e7. 2008.PubMed/NCBI
|
|
8
|
Merchant NB, Lewis JJ, Woodruff JM, et al:
Extremity and trunk desmoid tumors: a multifactorial analysis of
outcome. Cancer. 86:2045–2052. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ballo MT, Zagars GK, Pollack A, et al:
Desmoid tumor: prognostic factors and outcome after surgery,
radiation therapy, or combined surgery and radiation therapy. J
Clin Oncol. 17:158–167. 1999.PubMed/NCBI
|
|
10
|
Leithner A, Gapp M, Leithner K, et al:
Margins in extraabdominal desmoid tumors: A comparative analysis. J
Surg Oncol. 86:152–156. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ferraresi S, Garozzo D and Bianchini E:
Aggressive fibromatosis (desmoid tumor) of the radial nerve:
favorable resolution. Case report J Neurosurg. 95:332–333.
2001.PubMed/NCBI
|
|
12
|
Gallucci GL, Boretto JG and De Carli P:
Desmoid tumor of the forearm. Reconstructive surgery and functional
result. Chir Main. 28:326–329. 2009. View Article : Google Scholar : PubMed/NCBI
|