Introduction
Synchronous primary endometrial and ovarian cancer
(SPC) is frequently encountered in daily clinical settings. In
1985, Ulbright and Roth first reported the pathological criteria
for distinguishing metastatic disease from SPC (1). In 1995, Scully proposed more extensive
criteria (2), which are generally
used when cancers develop both in the endometrium and in the
ovary.
Zaino et al reported that SPC occurs in
approximately 10% of women with ovarian cancer and 5% of women with
endometrial cancer (3). Earlier
studies have suggested that there are other unique clinical
features in SPC. Soliman et al reported that SPC patients
are relatively young and nulliparous. The histology of SPC is
mostly well-differentiated endometrioid adenocarcinoma, and its
prognosis is better than that of primary uterine corpus cancer
(PCC) with ovarian metastasis or primary ovarian cancer (POC) with
uterus metastasis (4).
The prevalence of pelvic endometriosis is
approximately 6–10% in women (5).
It is estimated that the risk of ovarian cancer is considerably
higher in the presence of endometriosis, particularly endometrioid
adenocarcinoma and clear cell carcinoma of the ovary (6,7).
Furthermore, certain reports have suggested a correlation between
endometriosis and SPC (8).
In this study, we reviewed 13 cases of SPC treated
at our hospital, and compared their clinicopathological features
with those of PCC and POC patients in our department.
Patients and methods
Patients
This study included 186 patients with PCC, 136 with
POC and 13 with SPC. The patients were treated at Kyoto University
Hospital from 2005 to 2010. SPC was defined according to the
criteria of Scully et al (2). Written informed consent was obtained
from each patient.
Demographic data
The following demographic data were obtained from
medical records: age at diagnosis, presenting symptoms, body mass
index (BMI), parity, past medical history, menopausal status,
complication of thrombosis, recurrence of cancer, overall survival
rate and menstrual cycle (regular or irregular). Pathological
information, including histology, grade and presence of
endometriosis, were also obtained. Endometrial and ovarian cancer
stages were assigned based on the classification by the
International Federation for Gynecology and Obstetrics (FIGO).
Histological determination of the endometrial and ovarian cancer
was performed based on the World Health Organization (WHO)
committee classification of tumors. A comparison of SPC with PCC
and POC was performed for several clinical factors including age at
diagnosis, BMI, parity and thrombosis complication.
Statistical analysis
The GraphPad prism (MDF Co., Japan) was used for the
statistical analyses. Fisher's test was used to assess the
significance of differences in the categorical clinical and
pathological variables. Continuous variables were analyzed using
the Mann-Whitney test. P<0.05 was considered to indicate a
statistically significant difference.
Results
Patient characteristics
The characteristics of the SPC patients are listed
in Table I. The mean age at
diagnosis was 51.5 years, and the mean BMI was 22. Six of the 13
patients (46%) were nulliparous. Histologically, the lesion in the
endometrium was endometrioid adenocarcinoma (G1/G2) in all cases,
whereas the lesion in the ovary was well-differentiated
endometrioid adenocarcinoma in 12 of 13 cases, and clear cell
carcinoma in one case. The age at SPC diagnosis was significantly
lower than the age at PCC diagnosis (51.5 vs. 58.9 years; Table II). A greater number of SPC
patients were nulliparous (46.2%) compared with the PCC (28.5%) and
POC (33.8%) patients, although there was no significant difference.
In our department, complete cytoreductive surgery with adjuvant
chemotherapy is the standard treatment course for SPC. Recurrent
disease was observed in two SPC patients. All patients, including
those with disease recurrence, were alive as of January 2012.
Endometriosis was observed in all of the SPC cases.
 | Table ICharacteristics of synchronous primary
endometrial and ovarian cancer (SPC) patients. |
Table I
Characteristics of synchronous primary
endometrial and ovarian cancer (SPC) patients.
| No. | Age (years) | P | BMI | Symptom | Treatment | Menopause | Thrombosis | Corpus cancer
stage | Ovarian cancer
stage | Endometriosis | Recurrence | Overall survival
(M) |
|---|
| 1 | 48 | 2 | 24.6 | Ab bleeding | CCS+che | Post | − | EC,G1(1a) | EC,G1(1a) | + | − | 16 |
| 2 | 51 | 0 | 26.0 | Abd distention | CCS+che | Pre | + | EC,G1(1a) | EC,G1(1c) | + | − | 12 |
| 3 | 46 | 0 | 14.6 | Elevated marker | CCS+che | Pre | − | EC,G1(1b) | EC,G1(2c) | + | − | 18 |
| 4 | 43 | 2 | 19.2 | Ab bleeding | CCS+che | Pre | − | EC,G1(1b) | EC,G1(2c) | + | − | 14 |
| 5 | 46 | 0 | 24.7 | Abd distention | TAH+BSO
+pOM+chemo | Pre | + | EC,G1(1b) | EC,G1(2c) | + | − | 11 |
| 6 | 57 | 0 | 17.1 | Ab bleeding | CCS+che | Post | − | EC,G1(1a) | EC,G1(2a) | + | − | 12 |
| 7 | 57 | 1 | 25.3 | Residual urine | CCS+che | Post | − | EC,G1(2b) | EC,G1+CCC(2c) | + | + | 61 (AWD) |
| 8 | 50 | 2 | 21.2 | Ab bleeding | CCS+che | Pre | + | EC,G1(2b) | EC,G1(1c) | + | − | 57 |
| 9 | 61 | 2 | 24.6 | Abd distention | CCS+che | Post | − | EC,G1(2b) | EC,G1(1c) | + | − | 75 |
| 10 | 58 | 0 | 28.3 | Ab bleeding | TAH+BSO+che | Post | + | EC,G1(3a) | EC,G1(1c) | + | − | 45 |
| 11 | 52 | 2 | 19.5 | Ab bleeding | TAH+BSO+che | Post | + | EC,G1(1a) | EC,G1(1c) | + | − | 51 |
| 12 | 35 | 0 | 15.2 | Abd distention,
HNPCC | TAH+BSO+che | Pre | + | EC,G1(2a) | EC,G1(1c) | + | − | 26 |
| 13 | 67 | 1 | 27.5 | Ab bleeding | Che+CCS+che | Post | + | EC,G1(3) | CCC(2a) | + | + | 63 (AWD) |
| Table IIComparison of clinicopathological
features among SPC, POC and PCC patients. |
Table II
Comparison of clinicopathological
features among SPC, POC and PCC patients.
| SPC (n=13) | POC (n=136) | PCC (n=186) |
|---|
| Age (years) | 51.5 | 54.5 | 58.9a |
| Type of cancer |
| Endometrioid
adenocarcinoma G1/G2 (%) | 13 (100) | 11 (8.1) | 101 (54.5) |
| Endometrioid
adenocarcinoma G3 (%) | | 6 (4.4) | 34 (18.2) |
| Serous
adenocarcinoma (%) | | 53 (39.0) | 31 (16.6) |
| Clear cell
carcinoma (%) | 1 (7.8) | 37 (27.2) | 8 (4.3) |
| Mucinous
adenocarcinoma (%) | | 15 (11.0) | 1 (0.5) |
| Others (%) | | 24 (17.6) | 10 (5.3) |
| Stage |
| 1 | 1+1: 3 cases | 64 (47.1) | 111 (59.4) |
| 2 | 2+1: 3 cases, 1+2:
4 cases, 2+2: 1 cases | 5 (3.7) | 14 (7.5) |
| 3 | 3+1: 1 case, 3+2: 1
case | 47 (34.6) | 46 (24.6) |
| 4 | | 18 (13.2) | 16 (8.6) |
| BMI
(kg/m2) | 22.1 | 21.9 | 23.5 |
| Nulliparity
(%) | 6 (46.2) | 46 (33.8) | 54 (28.9) |
| Thromboembolism
(%) | 7
(53.8)* | 20 (14.7) | 10 (5.3) |
Comparison of young PCC and SPC
patients
As the age of the SPC patients was significantly
lower than that of PCC patients, we selected the young PCC patients
(those under 45 years old) with G1 and G2 endometrioid
adenocarcinoma, and compared them with the SPC patients in terms of
the clinicopathological factors. The POC patients whose
histological type was endometrioid adenocarcinoma or clear cell
carcinoma were also used for comparison (Table III). There was no significant
difference between each group in terms of age, BMI and nulliparity.
However, an irregular menstrual cycle was more frequently observed
among the PCC patients under 45 years old than among the SPC
patients (9 of 17, 52.9% vs. 2 of 13, 15.4%), although the
difference was not significant (p=0.05). In addition, endometriosis
complications were more frequent among the SPC patients than the
PCC patients under 45 years (17 of 17, 100% vs. 6 of 17, 35.3%).
Moreover, the incidence of thrombosis was significantly higher in
the SPC patients (7 of 13, 53.8% vs. none, 0%).
| Table IIIComparison among patients with SPC,
PCC with endometrial cancer (G1/G2 under 45 years old), POC with
ovarian endometrioid adenocarcinoma and POC with clear cell
carcinoma, which are recognized as endometriosis-related
cancer. |
Table III
Comparison among patients with SPC,
PCC with endometrial cancer (G1/G2 under 45 years old), POC with
ovarian endometrioid adenocarcinoma and POC with clear cell
carcinoma, which are recognized as endometriosis-related
cancer.
| SPC (n=13) | PCC (em cancer
G1/G2, under 45 years; n=17) | POC (endometrioid
cancer; n=17) | POC (clear cell
carcinoma; n=37) |
|---|
| Age (years) | 51.5 | | 55.1 | 53.1 |
| Stage (%) |
| 1 | 1+1: 3 cases | 15 (88.2) | 10 (58.8) | 28 (75.7) |
| 2 | 2+1: 3 cases, 1+2:
4 cases
2+1: 1 case | 1 (5.9) | 1 (5.9) | 1 (2.7) |
| 3 | 3+1: 1 cases, 3+2:
1 case | 1 (5.9) | 5 (29.4) | 4 (10.8) |
| 4 | | 0 (0) | 1 (5.9) | 4 (10.8) |
| BMI
(kg/m2) | 22.1 | 21.9 | 24.3 | 21.7 |
| Nulliparity
(%) | 6 (46.2) | 13 (76.5) | 6 (35.3) | 20 (54.1) |
| Thromboembolism
(%) | 7 (53.8)a | 0 (0) | 1 (5.9) | 6 (16.2) |
| Irregular mense
(%) | 2 (15.4)b | 9 (52.9) | | |
| Endometriosis
(%) | 13 (100)a | 6 (35.3) | | |
Incidence of thrombosis
Thrombosis complications were observed in SPC
patients at a significantly higher frequency (7 of 13, 53.8%) than
in PCC patients (10 of 186, 5.3%) and POC patients (20 of 146,
14.7%). We further investigated the clinical features of the
thrombosis cases (Tables IV and
V). Each group of cancer patients
was divided into a thrombosis (+) group and a thrombosis (−) group.
Among the PCC patients, patients with thrombosis were significantly
older and had a more advanced stage of disease (FIGO stage III+IV)
compared with those without thrombosis. POC patients with
thrombosis were also significantly older than those without
thrombosis. In contrast, there was no significant difference in age
and FIGO stage between the SPC patients with and without
thrombosis. In addition, when the incidence of thrombosis was
compared in advanced stage patients (FIGO stage II+III ovarian
cancer or FIGO stage III endometrial cancer), the SPC patients had
a significantly higher rate of thrombosis than the PCC (p<0.001)
or POC (p=0.004) patients.
| Table IVComparison among thrombosis(+)
patients in each group. |
Table IV
Comparison among thrombosis(+)
patients in each group.
| SPC (n=7) | POC (n=20) | PCC (n=10) |
|---|
| Age (years) | 51.1a | 62.8 | 66.1 |
| Type of cancer |
| Endometrioid
adenocarcinoma G1/G2 (%) | 7 (100) | | 3 (30) |
| Endometrioid
adenocarcinoma G3 (%) | | 1 (0.5) | 1 (10) |
| Serous
adenocarcinoma (%) | | 10 (50.0) | 4 (40) |
| Clear cell
carcinoma (%) | 1 (28.6) | 6 (30.0) | 1 (10) |
| Mucinous
adenocarcinoma (%) | | 2 (10.0) | |
| Others (%) | | 3 (15.0) | 1 (10) |
| Stage |
| 1 | 1+1: 2 cases | 6 (30.0) | 2 (20) |
| 2 | 2+1: 2 cases, 1+2:
1 case | 1 (0.5) | 1 (10) |
| 3 | 3+1: 1 cases, 3+2 1
case | 6 (30.0) | 3 (30) |
| 4 | | 7 (35.0) | 4 (40) |
| BMI
(kg/m2) | 23.2 | 22.5 | 22.8 |
| Nulliparity
(%) | 4 (66.2) | 3 (15.0) | 2 (20) |
| Table VComparison of clinical features of
thrombosis. |
Table V
Comparison of clinical features of
thrombosis.
| A, Comparison of
age between patients with positive and negative thrombosis status
in each group |
|---|
|
|---|
| Thrombosis(+) | Thrombosis(−) | p-value |
|---|
| SPC | 51.1 | 52.0 | 1.0 |
| POC | 62.8 | 53.0 | 0.002 |
| PCC | 66.1 | 58.0 | 0.03 |
|
| B, Comparison of
ratio of thrombosis(+) between patients with low-stage and
high-stage disease in each group |
|
| Thrombosis(+)/stage
1+2 | Thrombosis(+)/stage
3+4 | p-value |
|
| SPCa | 5/11 | 2/2 | 0.46 |
| POC | 7/69 | 13/65 | 0.15 |
| PCC | 3/125 | 7/60 | 0.015 |
|
| C, Comparison of
positive vs. negative thrombosis ratio among patients with SPC, POC
stage 2+3 and PCC stage 3 |
|
| Thrombosis(+) | Thrombosis(−) | |
|
| SPC | 7/13 | 6/13b,c | |
| POC stage 2+3 | 7/52 | 45/52 | |
| PCC stage 3 | 3/46 | 43/46 | |
Discussion
In this study, we compared several
clinicopathological features of SPC with those of PCC or POC.
First, we found a significant difference in the age at diagnosis
between patients with SPC and those with PCC. Patients with SPC
were significantly younger than those with PCC (51.5 vs. 58.9
years). Additionally, the mean age of patients with SPC was
relatively lower compared to POC, although the difference was not
statistically significant. In addition, patients with SPC exhibited
a relatively high rate of nulliparity compared to those with PCC.
There are several earlier reports that describe the
clinicopathological features of SPC. In their review of 84 cases of
SPC, Soliman et al reported that women with SPC were young,
obese and nulliparous (4). Sultan
et al also indicated that women with SPC were significantly
younger than women with PCC and POC (9). Herrinton et al reported that
high parity and long-term use of oral contraceptives reduced the
risk of SPC (10). Taken together,
younger age and nulliparity appear to be unique features of SPC.
Our next question was whether the difference between SPC and PCC is
due to the inclusion of older PCC patients, who might be
significantly different from younger patients in terms of tumor
biology as well as host condition. To address this issue, we
selected only the young PCC patients under the age of 45. When the
SPC patients were compared with this group of PCC patients, there
were still significant differences: the incidence of endometriosis
(100 vs. 35%) and thrombosis (54 vs. 0%) was significantly higher
in SPC patients. These data suggest that SPC has several unique
clinical features that are distinct from PCC in patients of a
similar age.
In all 13 SPC cases, the lesion in the endometrium
was well-differentiated endometrioid carcinoma, and in 11 of the 13
cases, the lesion in the ovary was also well-differentiated
endometrioid carcinoma. Of the other two SPC cases, one was clear
cell carcinoma, and the other involved both well-differentiated
endometrioid carcinoma and clear cell carcinoma in the ovary.
According to previous reports, the majority of SPC cases consist of
well-differentiated endometrioid carcinoma in both the endometrium
and the ovary (4,9,11),
which is consistent with the results of the present study. In a
relatively short follow-up period, only 2 (15.4%) cases of SPC
recurred, and both patients are currently alive, suggesting a
favorable outcome of SPC. Most of the previous reports refer to an
excellent overall survival rate in women with SPC, which is
reportedly due to the earlier stage at diagnosis of SPC compared
with POC. The first symptom in the majority of SPC cases is
abnormal bleeding (4). Accordingly,
in our study, 8 of the 13 SPC patients visited our hospital due to
abnormal bleeding. However, Williams et al revealed that SPC
still had a better prognosis that was independent of stage, even
after adjusting for other prognosis factors. In other words, SPC
itself might be directly associated with good prognosis (12).
Notably, in our study, the presence of endometriosis
was a factor in all the SPC patients. Endometriosis represents a
significant site of origin of ovarian cancer, particularly in the
case of endometrioid adenocarcinoma and clear cell carcinoma.
Several previous reports have suggested a correlation between
endometriosis and SPC. Kondi-Pafiti et al pathologically
confirmed endometriosis in all patients with SPC (13). Zaino et al reported the
presence of endometriosis in 31% of SPC patients (3). Two possibilities have been suggested
regarding the association between endometriosis and SPC. First,
endometriotic implants may undergo direct malignant transformation,
often through atypical endometriosis. Second, cancer and
endometriosis share various environmental, immunological, hormonal
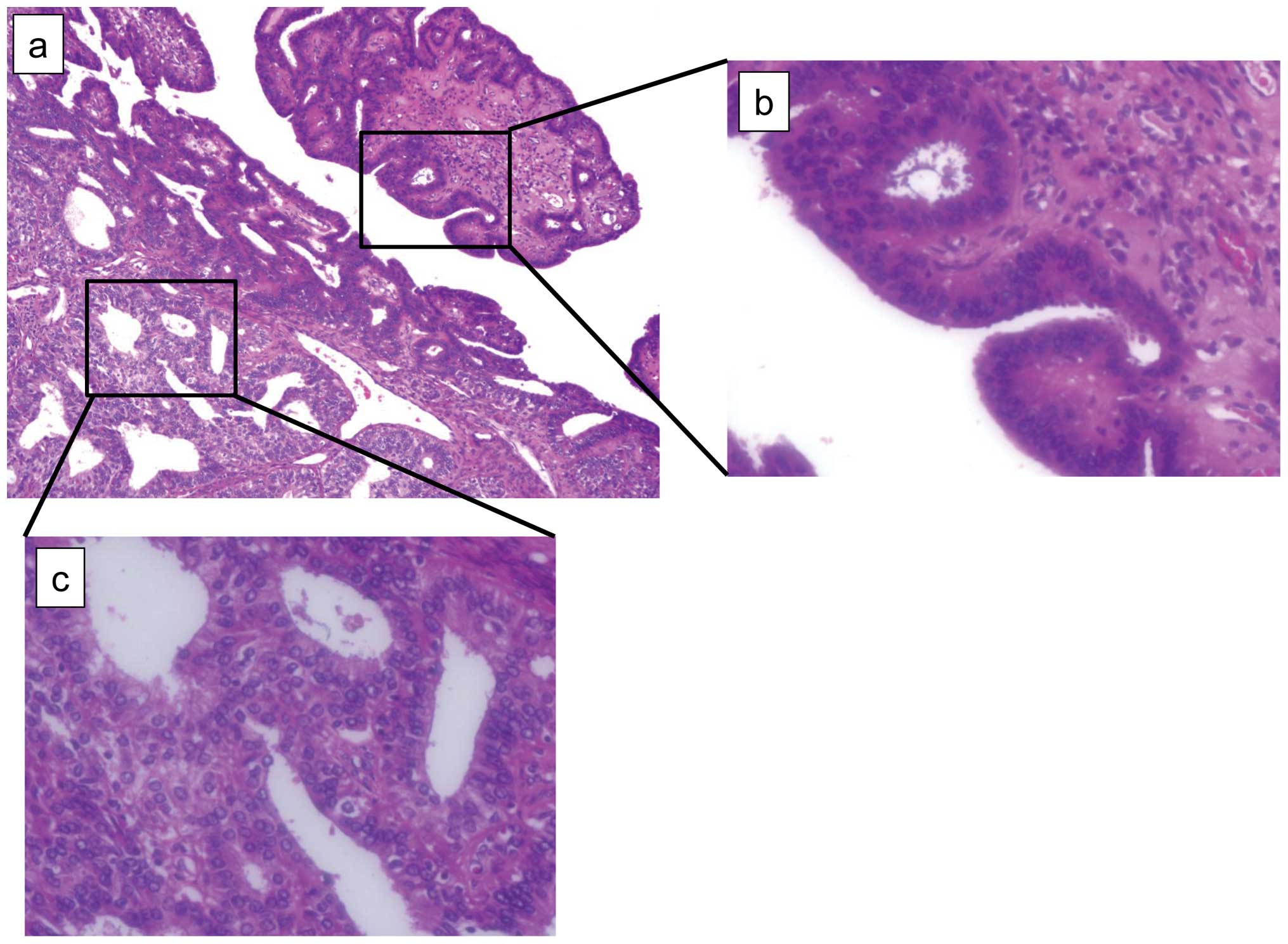
and genetic predisposing factors (14). In our study, the clinicopathological
features (irregular menstruation cycle and presence of
endometriosis) of SPC resemble those of endometriosis-associated
ovarian cancer rather than young-age PCC. In some of our SPC
patients, atypical endometriosis was observed (Fig. 1), which is reportedly found in
approximately 60–80% of endometriosis-associated ovarian cancer
(8,14).
Cancer-related thrombosis is also known as
Trousseau's syndrome, which was first reported in 1865 in
association with gastric cancer (15). Factors secreted by cancer cells
impair the coagulation and fibrinolytic system. One of these
factors is tissue factor (TF) (16). Conversion of factor VII to its
active form (factor VIIa) in complex with TF triggers the
production of other coagulation-related proteases, particularly
factor X and factor IXa. Elevated TF expression is observed in
carcinoma cells in Trousseau's syndrome as well as in associated
angiogenic endothelium. Activated oncogenes (K-ras, EGFR, PML-RARA
and MET) or inactivated tumor suppressors (p53 and PTEN) are known
to lead to an induction of TF and its activity (17). It is also suggested that tumor
hypoxia increases the expression of genes that facilitate
coagulation, including TF and plasminogen activator inhibitor type
1 (PAI-1) (18). In gynecological
malignancies, ovarian cancer, particularly clear cell carcinoma, is
known to increase the development of complicated thrombosis
(19,20). Uno et al studied TF activity
in ovarian cancer, and reported that TF expression in clear cell
carcinoma is significantly increased compared with that in
non-clear cell carcinoma (21). We
demonstrated that clear cell carcinoma of the ovary has aberrant
expression of coagulation-related genes, which is caused by the
microenvironment within the endometriotic cyst (22). Thus far, no study has addressed the
association between SPC and thrombosis. In the current study,
patients with SPC developed thromboses at a significantly higher
rate compared to PCC and POC patients; as many as 53.8% (7 of 13)
of the SPC patients developed complicated thrombosis prior to
starting therapy. In the PCC and POC patients, those who developed
thrombosis were significantly older than those who did not. In
patients with PCC, those who developed thrombosis had a
significantly higher FIGO stage than those who did not. However, in
SPC cases, there was no such tendency. Although there was only a
relatively small number of cases included in this study, SPC itself
may be an independent risk factor for thrombosis, similar to clear
cell carcinoma.
In conclusion, this study indicates that SPC has
several unique features, including young age, nulliparity and a
better prognosis. In addition, endometriosis was detected in all of
the SPC patients, which is consistent with several previous
studies. Clinically, SPC may be more similar to
endometriosis-related ovarian cancer than young-age corpus cancer.
Notably, thrombosis occurred in patients with SPC at a
significantly higher rate than in PCC and POC. There may be
specific carcinogenetic mechanisms in SPC that are related to its
own unique features, including the co-existence of endometriosis
and thrombogenic tendency. Further research is required to explore
these mechanisms.
References
|
1
|
Ulbright T and Roth L: Metastatic and
independent cancers of the endometrium and ovary: a
clinicopathologic study of 34 cases. Hum Pathol. 16:28–34. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Scully RE, Young RH and Clements PB:
Tumors of the ovary, maldeveloped gonads, fallopian tube, and broad
ligament. Atlas of Tumor Pathology. Series 3, Fascicle 23. Rosai J
and Sobin LH: Armed Forces Institute of Pathology; Washington DC:
pp. 125–126. 1998
|
|
3
|
Zaino R, Whitney C, Brady MF, et al:
Simultaneously detected endometrial and ovarian carcinomas- a
prospective clinicopathologic study of 74 cases: a Gynecologic
Oncology Group study. Gynecol Oncol. 83:355–362. 2001. View Article : Google Scholar
|
|
4
|
Soliman PT, Slomovitz BM, Broaddus RR, Sun
CC, Oh JC, Eifel PJ, Gershenson DM and Lu KH: Synchronous primary
cancers of the endometrium and ovary: a single institution review
of 84 cases. Gynecol Oncol. 94:456–462. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Giudice LC and Kao LC: Endometriosis.
Lancet. 364:1789–1799. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Komiyama S, Aoki D, Tominaga E, et al:
Prognosis of Japanese patients with ovarian clear cell carcinoma
associated with pelvic endometriosis: Clinicopathologic evalution.
Gynecol Oncol. 72:342–346. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
McMeekin DS, Burger RA, Manetta A, et al:
Endometrioid adenocarcinoma of the ovary and its relationship to
endometriosis. Gynecol Oncol. 59:81–86. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Stern RC, Dash R, Bentley RC, et al:
Malignancy in endometriosis: frequency and comparison of ovarian
and extraovarian types. Int J Gynecol Pathol. 20:133–139. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sultan E, Ibrahim G, Raziye O, et al:
Synchronous primary cancers of the female reproductive tract in
Turkish women. Asian Pac J Cancer Prev. 12:857–859. 2011.PubMed/NCBI
|
|
10
|
Herrinton LJ, Voigt LF and Weiss NS: Risk
factors for synchronous primary endometrial and ovarian cancers.
Annals of Epidemiology. 11:529–533. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lim YK, Padma R, Foo L, et al: Survival
outcome of women with synchronous cancers of endometrium and ovary:
a 10 year retrospective cohort study. J Gynecol Oncol. 22:239–243.
2011.PubMed/NCBI
|
|
12
|
Williams MG, Bandera EV, Demissie K, et
al: Synchronous primary ovarian and endometrial cancers. A
population-based assessment of survival. Obstet Gynecol.
113:783–789. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kondi-Pafiti A, Grapsa D, Liapsi K, et al:
Synchronous ovarian and endometrial carcinoma: a strong link to
endometriosis? Eur J Gynaecol Oncol. 29:256–259. 2008.PubMed/NCBI
|
|
14
|
Varma R, Rollason T, Gupta JK, et al:
Endometriosis and the neoplastic process. Reproduction.
127:293–304. 2004. View Article : Google Scholar
|
|
15
|
Donati MB: Thrombosis and cancer:
Trousseau syndrome revisited. Best Pract Res Clin Haematol. 22:3–8.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Varki A: Trousseau's syndrome: multiple
definitions and multiple mechanisms. Blood. 110:172–1729. 2007.
|
|
17
|
Rak J, Yu JL, Luyendyk J, et al:
Oncogenes, Trousseau syndrome, and cancer-related changes in the
coagulome of mice and humans. Cancer Res. 66:10643–10646. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Denko NC and Giaccia AJ: Tumor hypoxia,
the physiological link between Trousseau's syndrome
(carcinoma-induced coagulopathy) and metastasis. Cancer Res.
61:795–798. 2004.
|
|
19
|
Heit JA, Silverstein MD, Mohr DN, et al:
Risk factors for deep vein thrombosis and pulmonary embolism. Arch
Intern Med. 160:809–815. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Matsuura Y, Robertson G, Marsden DE, et
al: Thromboembolic complications in patients with clear cell
carcinoma of the ovary. Gynecol Oncol. 104:406–410. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Uno K, Homma S, Satoh T, et al: Tissue
factor expression as a possible determinant of thromboembolism in
ovarian cancer. Br J Cancer. 96:290–295. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Yamaguchi K, Mandai M, Oura T, et al:
Identification of ovarian clear cell carcinoma gene signature that
reflects inherent disease biology and carcinogenic processes.
Oncogene. 29:1741–1752. 2010. View Article : Google Scholar : PubMed/NCBI
|